
A Hunt for the Resistance of Haemophilus influnezae to Beta-Lactams

Abstract
:1. Introduction
2. Results
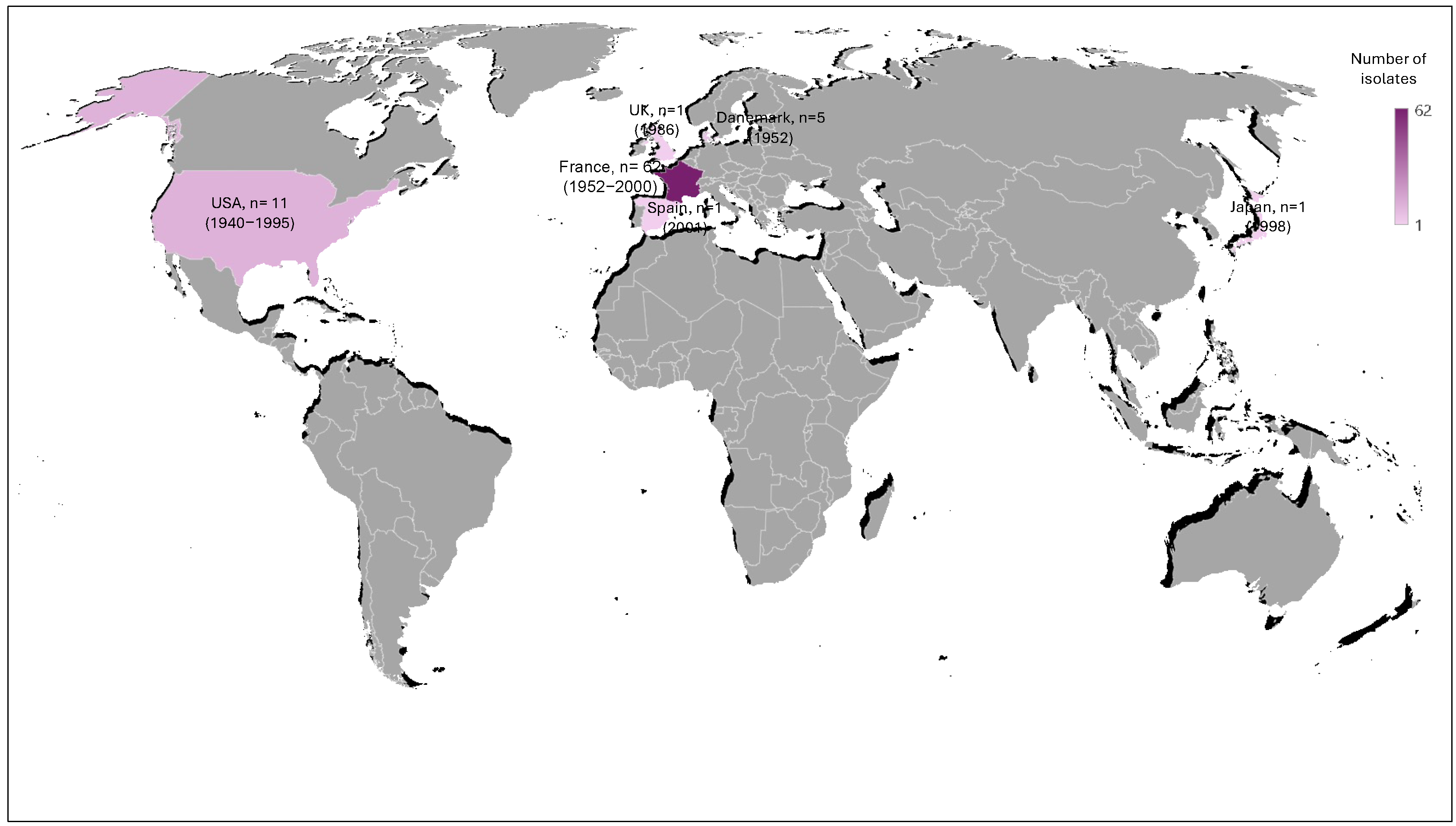
2.1. Characteristics of the Historic Collection of H. influenzae Isolates
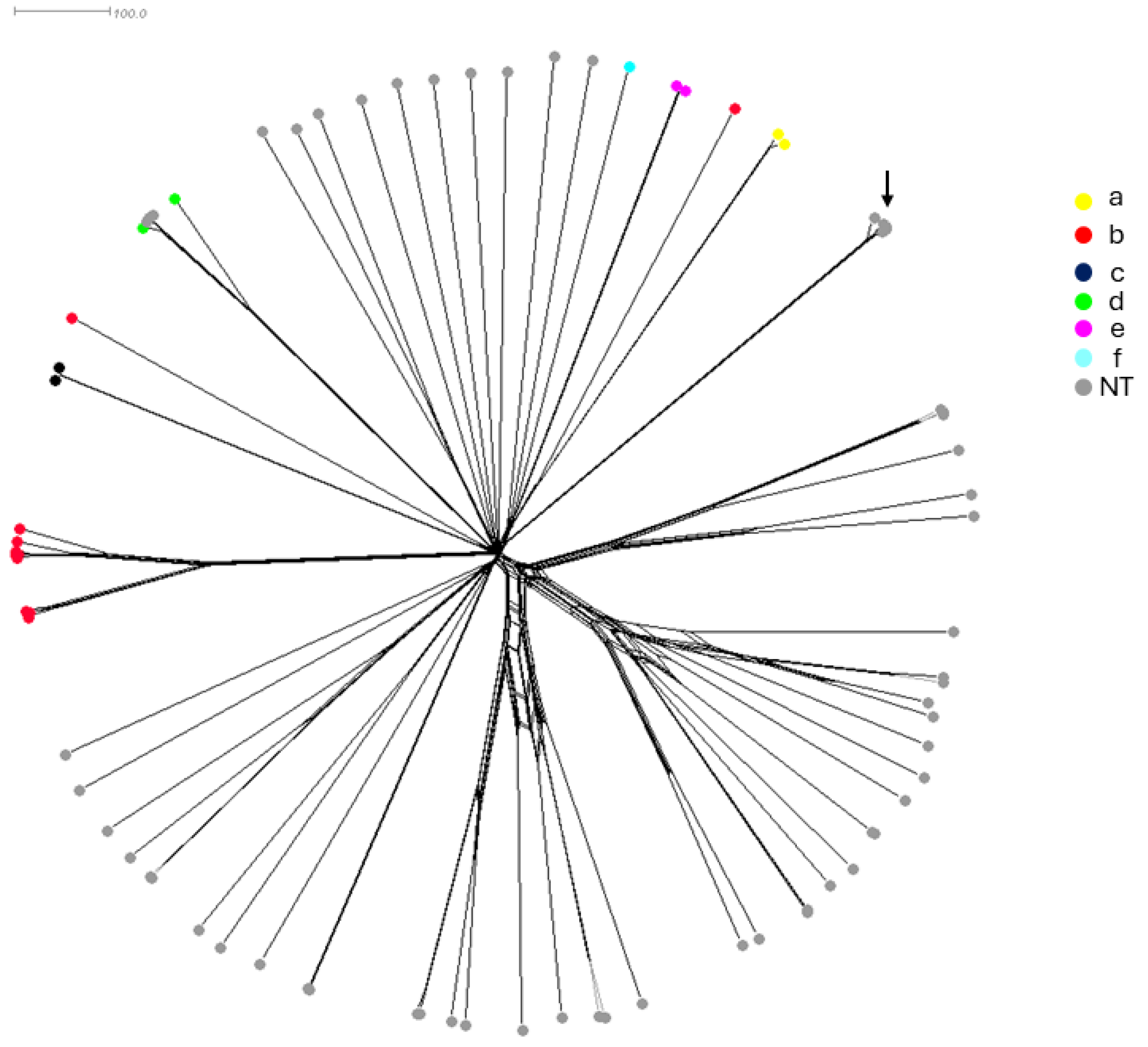
2.2. Genetic Characteristics of the Historic Collection of H. influenzae Isolates
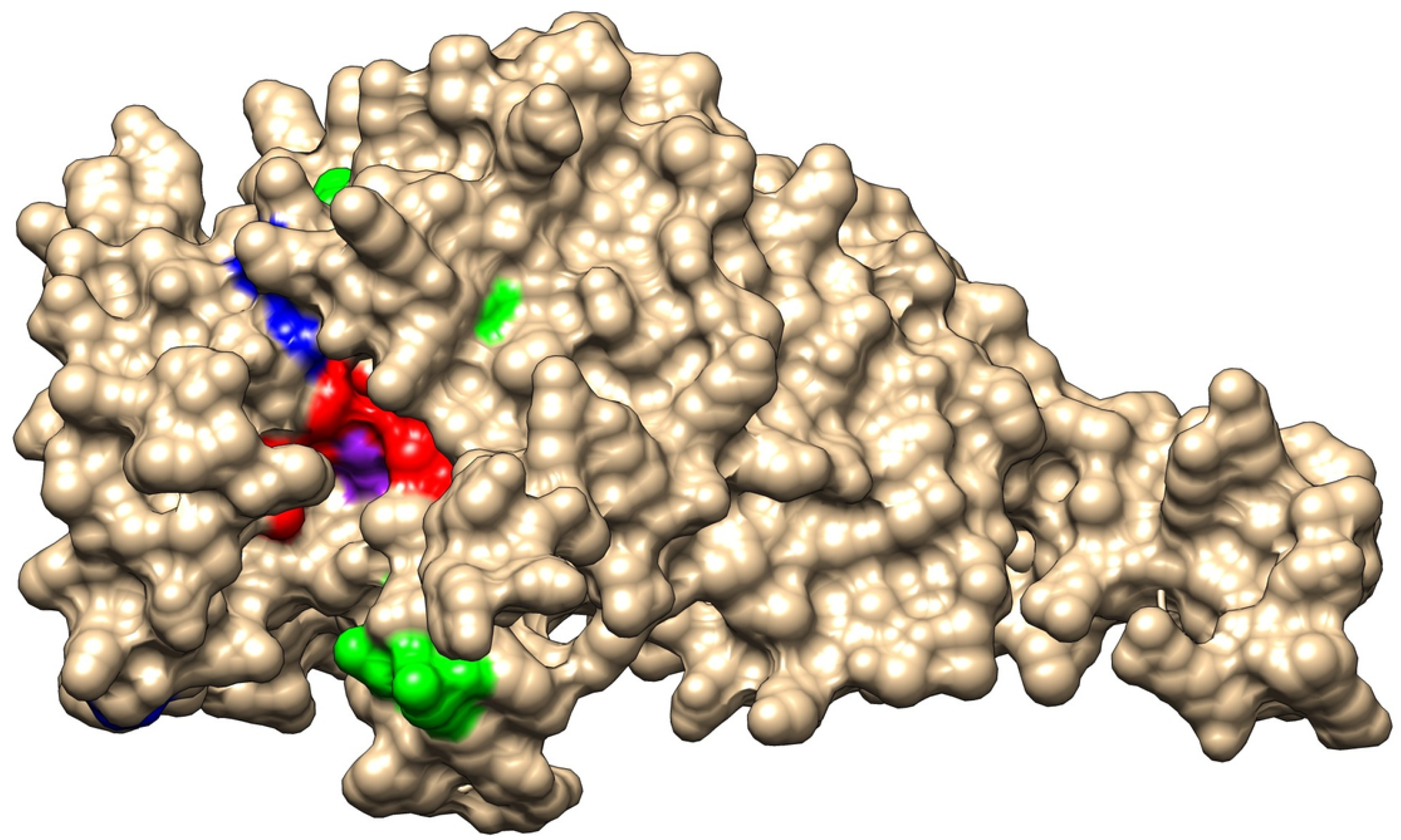
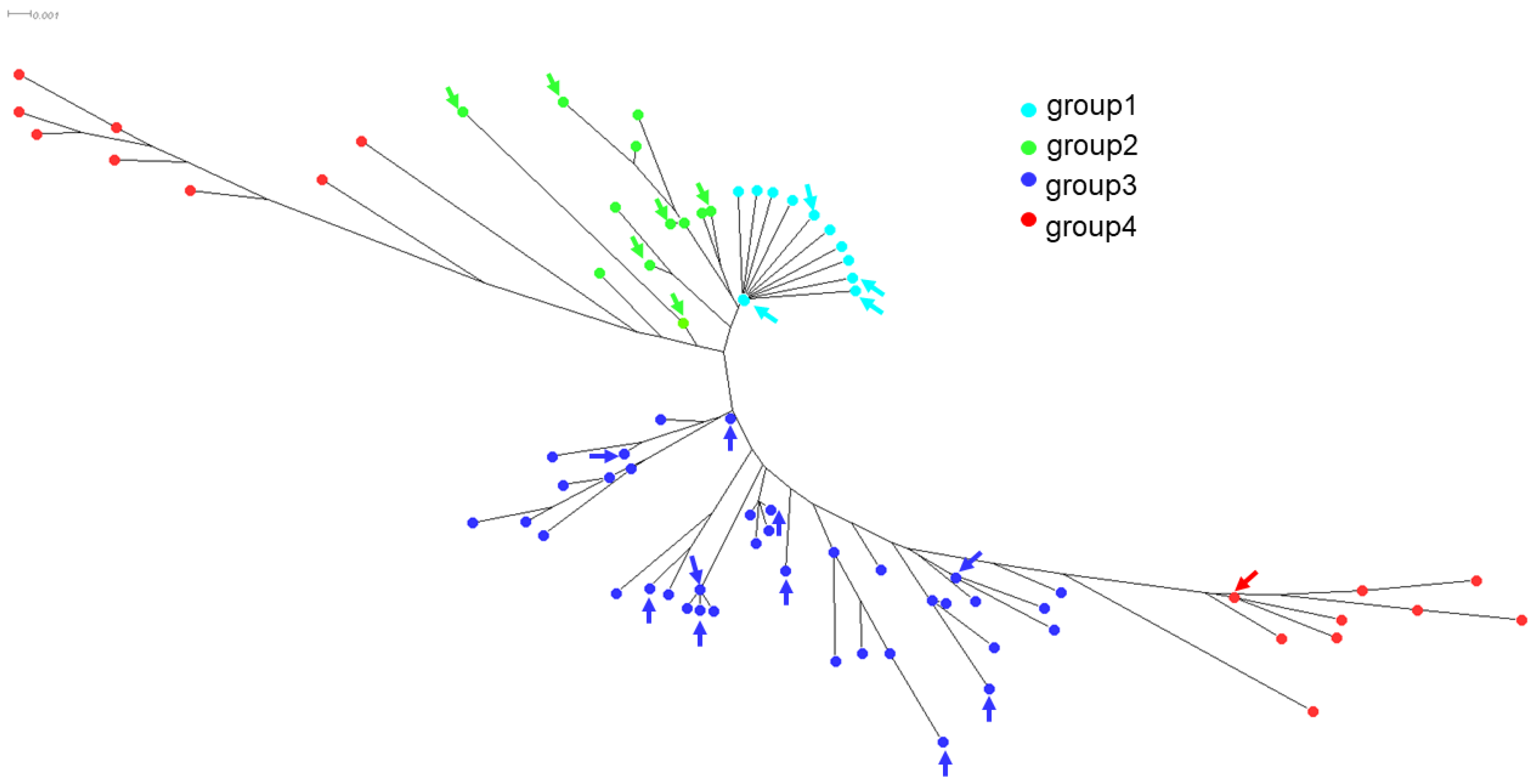
2.3. Characteristics of Genes Involved in Antibiotic Resistance
3. Discussion
4. Materials and Methods
4.1. Isolates and Analysis
4.2. Molecular Analysis
4.3. Structure–Function Analysis
4.4. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Aminov, R.I. The role of antibiotics and antibiotic resistance in nature. Environ. Microbiol. 2009, 11, 2970–2988. [Google Scholar] [CrossRef] [PubMed]
- Mucsi, Z.; Chass, G.A.; Csizmadia, I.G. Reply to the ‘Comment on “Penicillin’s catalytic mechanism revealed by inelastic neutrons and quantum chemical theory”’ by S. A. Glover Phys. Chem. Chem. Phys. 2019, 21, 18012. Phys. Chem. Chem. Phys. 2019, 21, 25513–25517. [Google Scholar] [CrossRef]
- Rao, V.K.; Krasan, G.P.; Hendrixson, D.R.; Dawid, S.; St. Geme, J.W., III. Molecular determinants of the pathogenesis of disease due to non-typable Haemophilus influenzae. FEMS Microbiol. Rev. 1999, 23, 99–129. [Google Scholar] [CrossRef] [PubMed]
- Wenger, J.D.; Pierce, R.; Deaver, K.; Franklin, R.; Bosley, G.; Pigott, N.; Broome, C.V.; Haemophilus Influenzae Study Group. Haemophilus influenzae Study Group Invasive Haemophilus influenzae disease: A population-based evaluation of the role of capsular polysaccharide serotype. J. Infect. Dis. 1992, 165, S34–S35. [Google Scholar] [CrossRef] [PubMed]
- Musser, J.M.; Kroll, J.S.; Granoff, D.M.; Moxon, E.R.; Brodeur, B.R.; Campos, J.; Dabernat, H.; Frederiksen, W.; Hamel, J.; Hammond, G.; et al. Global genetic structure and molecular epidemiology of encapsulated Haemophilus influenzae. Rev. Infect. Dis. 1990, 12, 75–111. [Google Scholar] [CrossRef] [PubMed]
- Rosenstein, N.E.; Perkins, B.A. Update on Haemophilus influenzae serotype b and meningococcal vaccines. Pediatr. Clin. North. Am. 2000, 47, 337–352. [Google Scholar] [CrossRef] [PubMed]
- Collins, S.; Ramsay, M.; Campbell, H.; Slack, M.P.; Ladhani, S.N. Invasive Haemophilus influenzae type b disease in England and Wales: Who is at risk after 2 decades of routine childhood vaccination? Clin. Infect. Dis. 2013, 57, 1715–1721. [Google Scholar] [CrossRef] [PubMed]
- Giufrè, M.; Fabiani, M.; Cardines, R.; Riccardo, F.; Caporali, M.G.; D'Ancona, F.; Pezzotti, P.; Cerquetti, M. Increasing trend in invasive non-typeable Haemophilus influenzae disease and molecular characterization of the isolates, Italy, 2012–2016. Vaccine 2018, 36, 6615–6622. [Google Scholar] [CrossRef] [PubMed]
- Cho, H.; Uehara, T.; Bernhardt, T.G. Beta-lactam antibiotics induce a lethal malfunctioning of the bacterial cell wall synthesis machinery. Cell 2014, 159, 1300–1311. [Google Scholar] [CrossRef]
- Park, J.T.; Strominger, J.L. Strominger, Mode of action of penicillin. Science 1957, 125, 99–101. [Google Scholar] [CrossRef]
- Deghmane, A.-E.; Hong, E.; Chehboub, S.; Terrade, A.; Falguières, M.; Sort, M.; Harrison, O.; Jolley, K.A.; Taha, M.-K. High diversity of invasive Haemophilus influenzae isolates in France and the emergence of resistance to third generation cephalosporins by alteration of ftsI gene. J. Infect. 2019, 79, 7–14. [Google Scholar] [CrossRef] [PubMed]
- Tsang, R.S.; Shuel, M.; Whyte, K.; Hoang, L.; Tyrrell, G.; Horsman, G.; Wylie, J.; Jamieson, F.; Lefebvre, B.; Haldane, D.; et al. Antibiotic susceptibility and molecular analysis of invasive Haemophilus influenzae in Canada, 2007 to 2014. J. Antimicrob. Chemother. 2017, 72, 1314–1319. [Google Scholar] [PubMed]
- Xiao, J.; Su, L.; Huang, S.; Liu, L.; Ali, K.; Chen, Z. Epidemic Trends and Biofilm Formation Mechanisms of Haemophilus influenzae: Insights into Clinical Implications and Prevention Strategies. Infect. Drug Resist. 2023, 16, 5359–5373. [Google Scholar] [CrossRef] [PubMed]
- Bajanca-Lavado, M.P.; Casin, I.; Pato, M.V.V. Antimicrobial resistance and epidemiological study of Haemophilus influenzae strains isolated in Portugal. The Multicentre Study Group. J. Antimicrob. Chemother. 1996, 38, 615–625. [Google Scholar] [CrossRef] [PubMed]
- Giufrè, M.; Daprai, L.; Cardines, R.; Bernaschi, P.; Ravà, L.; Accogli, M.; Raponi, M.; Garlaschi, M.L.; degli Atti, M.L.C.; Cerquetti, M. Carriage of Haemophilus influenzae in the oropharynx of young children and molecular epidemiology of the isolates after fifteen years of H. influenzae type b vaccination in Italy. Vaccine 2015, 33, 6227–6234. [Google Scholar] [CrossRef] [PubMed]
- Tchatchouang, S.; Nzouankeu, A.; Hong, E.; Terrade, A.; Denizon, M.; Deghmane, A.-E.; Ndiang, S.M.T.; Pefura-Yone, E.-W.; Beng, V.P.; Njouom, R.; et al. Analysis of Haemophilus species in patients with respiratory tract infections in Yaounde, Cameroon. Int. J. Infect. Dis. 2020, 100, 12–20. [Google Scholar] [CrossRef] [PubMed]
- Sondergaard, A.; Norskov-Lauritsen, N. Contribution of PBP3 Substitutions and TEM-1, TEM-15, and ROB-1 Beta-Lactamases to Cefotaxime Resistance in Haemophilus influenzae and Haemophilus parainfluenzae. Microb. Drug Resist. 2016, 22, 247–252. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. World Health Organization WHO Bacterial Priority Pathogens List, 2024: Bacterial Pathogens of Public Health Importance to Guide Research, Development and Strategies to Prevent and Control Antimicrobial Resistance; WHO: Geneva, Switzerland, 2024. [Google Scholar]
- Dabernat, H.; Delmas, C.; Seguy, M.; Pelissier, R.; Faucon, G.; Bennamani, S.; Pasquier, C. Diversity of beta-lactam resistance-conferring amino acid substitutions in penicillin-binding protein 3 of Haemophilus influenzae. Antimicrob. Agents Chemother. 2002, 46, 2208–2218. [Google Scholar] [CrossRef] [PubMed]
- Ubukata, K.; Shibasaki, Y.; Yamamoto, K.; Chiba, N.; Hasegawa, K.; Takeuchi, Y.; Sunakawa, K.; Inoue, M.; Konno, M. Association of amino acid substitutions in penicillin-binding protein 3 with beta-lactam resistance in beta-lactamase-negative ampicillin-resistant Haemophilus influenzae. Antimicrob. Agents Chemother. 2001, 45, 1693–1699. [Google Scholar] [CrossRef]
- Qin, L.; Watanabe, H.; Zhou, Z.; Hu, B.; Yamamoto, T. Antimicrobial susceptibility and genetic characteristics of Haemophilus influenzae isolated from community-acquired respiratory tract infection patients in Shanghai City, China. J. Infect. Chemother. 2012, 18, 508–514. [Google Scholar] [CrossRef]
- Schotte, L.; Wautier, M.; Martiny, D.; Piérard, D.; Depypere, M. Detection of beta-lactamase-negative ampicillin resistance in Haemophilus influenzae in Belgium. Diagn. Microbiol. Infect. Dis. 2019, 93, 243–249. [Google Scholar] [CrossRef] [PubMed]
- Jolley, K.A.; Maiden, M.C. BIGSdb: Scalable analysis of bacterial genome variation at the population level. BMC Bioinform. 2010, 11, 595. [Google Scholar] [CrossRef] [PubMed]
- Enne, V.I.; King, A.; Livermore, D.M.; Hall, L.M.C. Sulfonamide resistance in Haemophilus influenzae mediated by acquisition of sul2 or a short insertion in chromosomal folP. Antimicrob. Agents Chemother. 2002, 46, 1934–1939. [Google Scholar] [CrossRef] [PubMed]
- European Committee on Antimicrobial Susceptibility Testing. Breakpoint Tables for Interpretation of MICs and Zone Diameters. Version 14.0. 2024. Available online: http://www.eucast.org (accessed on 15 April 2024).
- Quentin, R.; Goudeau, A.; Wallace, R.J.; Smith, A.L.; Selander, R.K.; Musser, J.M. Urogenital, maternal and neonatal isolates of Haemophilus influenzae: Identification of unusually virulent serologically non-typable clone families and evidence for a new Haemophilus species. J. Gen. Microbiol. 1990, 136, 1203–1209. [Google Scholar] [CrossRef] [PubMed]
- Andrzejczuk, S.; Kosikowska, U.; Chwiejczak, E.; Stępień-Pyśniak, D.; Malm, A. Prevalence of Resistance to beta-Lactam Antibiotics and bla Genes. Among Commensal Haemophilus parainfluenzae Isolates from Respiratory Microbiota in Poland. Microorganisms 2019, 7, 427. [Google Scholar] [CrossRef] [PubMed]
- Taha, A.; Adeline, F.; Taha, M.-K.; Deghmane, A.-E. Haemophilus influenzae drug resistance in France from 2017 to 2021: Consideration for treatment of otitis media. J. Glob. Antimicrob. Resist. 2022, 31, 222–227. [Google Scholar] [CrossRef] [PubMed]
- Sauvage, E.; Kerff, F.; Terrak, M.; Ayala, J.A.; Charlier, P. The penicillin-binding proteins: Structure and role in peptidoglycan biosynthesis. FEMS Microbiol. Rev. 2008, 32, 234–258. [Google Scholar] [CrossRef] [PubMed]
- Bellini, D.; Koekemoer, L.; Newman, H.; Dowson, C.G. Novel and Improved Crystal Structures of H. influenzae, E. coli and P. aeruginosa Penicillin-Binding Protein 3 (PBP3) and N. gonorrhoeae PBP2: Toward a Better. Understanding of beta-Lactam Target-Mediated Resistance. J. Mol. Biol. 2019, 431, 3501–3519. [Google Scholar] [CrossRef]
- Lee, M.; Hesek, D.; Suvorov, M.; Lee, W.; Vakulenko, S.; Mobashery, S. A mechanism-based inhibitor targeting the DD-transpeptidase activity of bacterial penicillin-binding proteins. J. Am. Chem. Soc. 2003, 125, 16322–16326. [Google Scholar] [CrossRef]
- Kumar, K.M.; Anitha, P.; Sivasakthi, V.; Bag, S.; Lavanya, P.; Anbarasu, A.; Ramaiah, S. In silico study on Penicillin derivatives and Cephalosporins for upper respiratory tract bacterial pathogens. 3 Biotech 2014, 4, 241–251. [Google Scholar] [CrossRef]
- Zapun, A.; Morlot, C.; Taha, M.K. Resistance to beta-Lactams in Neisseria ssp Due to Chromosomally Encoded Penicillin-Binding Proteins. Antibiotics 2016, 5, 35. [Google Scholar] [CrossRef] [PubMed]
- Golparian, D.; Bazzo, M.L.; Golfetto, L.; Gaspar, P.C.; Schörner, M.A.; Benzaken, A.S.; Ramos, M.C.; Ferreira, W.A.; Neto, J.B.A.; Pereira, G.F.M.; et al. Genomic epidemiology of Neisseria gonorrhoeae elucidating the gonococcal antimicrobial resistance and lineages/sublineages across Brazil, 2015–2016. J. Antimicrob. Chemother. 2020, 75, 3163–3172. [Google Scholar] [CrossRef] [PubMed]
- Falla, T.J.; Crook, D.W.; Brophy, L.N.; Maskell, D.; Kroll, J.S.; Moxon, E.R. PCR for capsular typing of Haemophilus influenzae. J. Clin. Microbiol. 1994, 32, 2382–2386. [Google Scholar] [CrossRef] [PubMed]
- Huson, D.H.; Bryant, D. Application of phylogenetic networks in evolutionary studies. Mol. Biol. Evol. 2006, 23, 254–267. [Google Scholar] [CrossRef] [PubMed]
- Pettersen, E.F.; Goddard, T.D.; Huang, C.C.; Couch, G.S.; Greenblatt, D.M.; Meng, E.C.; Ferrin, T.E. UCSF Chimera--a visualization system for exploratory research and analysis. J. Comput. Chem. 2004, 25, 1605–1612. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| N° | Beta-Lactamase | Amoxicillin: Phenotype * (Range MIC mg/L) | Amoxicillin/Clavulanic Acid: Phenotype (Range MIC mg/L) | Cefotaxime: Phenotype (Range MIC mg/L) |
|---|---|---|---|---|
| 56 | Negative | S (0.25–1) | S (0.25–1) | S (0.004–0.125) |
| 10 | Negative | R (3–256) | R (3–256) | S (0.032–0.125) |
| 1 | Negative | R (256) | R (256) | R (4) |
| 10 | Positive | R (3–256) | S (0.125–1) | S (0.008–0.023) |
| 4 | Positive | R (64–256) | R (3) | S (0.032–0.064) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Denizon, M.; Hong, E.; Terrade, A.; Taha, M.-K.; Deghmane, A.-E. A Hunt for the Resistance of Haemophilus influnezae to Beta-Lactams. Antibiotics 2024, 13, 761. https://doi.org/10.3390/antibiotics13080761
Denizon M, Hong E, Terrade A, Taha M-K, Deghmane A-E. A Hunt for the Resistance of Haemophilus influnezae to Beta-Lactams. Antibiotics. 2024; 13(8):761. https://doi.org/10.3390/antibiotics13080761
Chicago/Turabian StyleDenizon, Mélanie, Eva Hong, Aude Terrade, Muhamed-Kheir Taha, and Ala-Eddine Deghmane. 2024. "A Hunt for the Resistance of Haemophilus influnezae to Beta-Lactams" Antibiotics 13, no. 8: 761. https://doi.org/10.3390/antibiotics13080761