The Prevalence of Multidrug Resistance of Helicobacter pylori and Its Impact on Eradication in Korea from 2017 to 2019: A Single-Center Study

 and
and
Abstract
:1. Introduction
2. Results
2.1. Patient Demographics and the Culture Success Rate of H. pylori
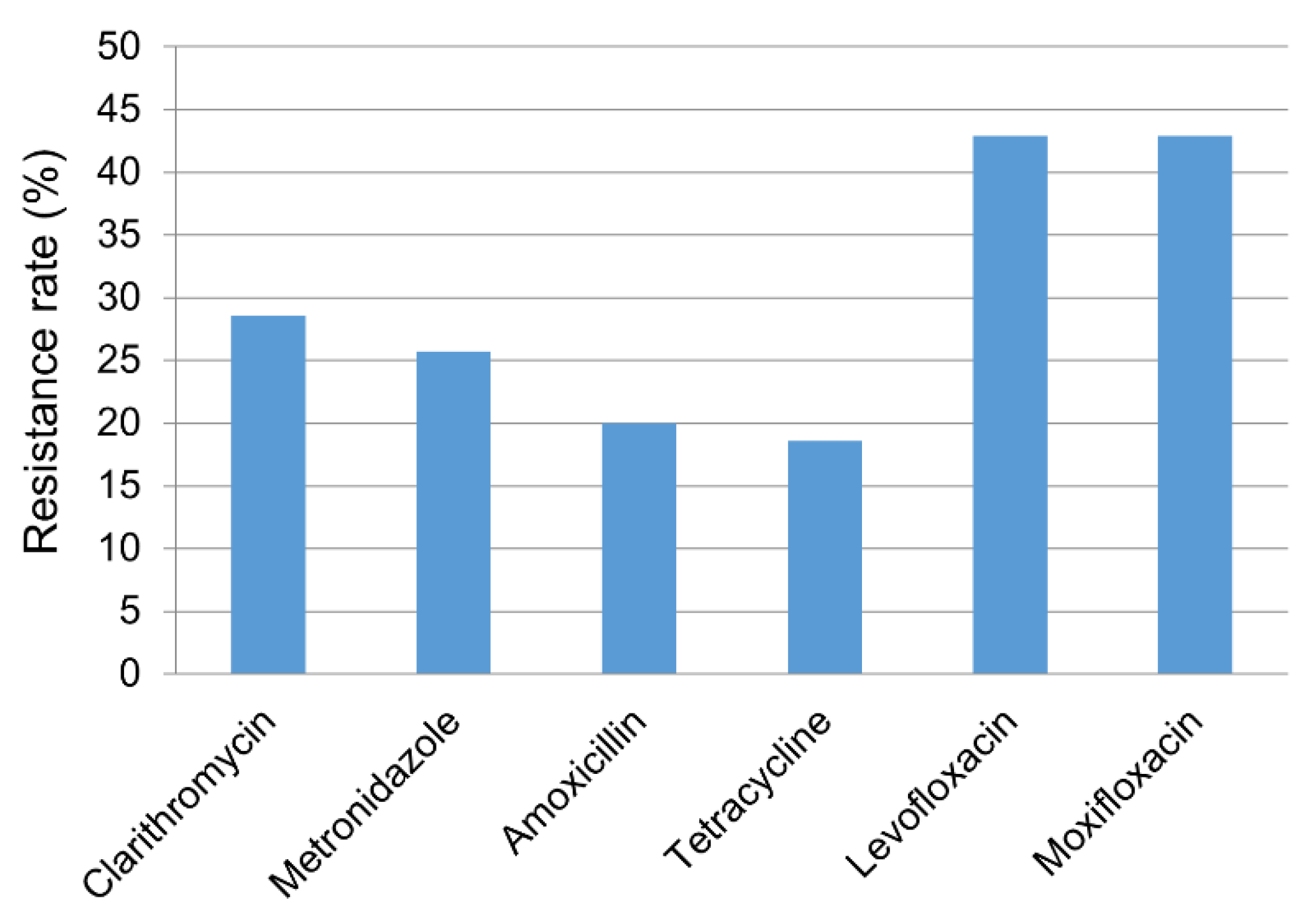
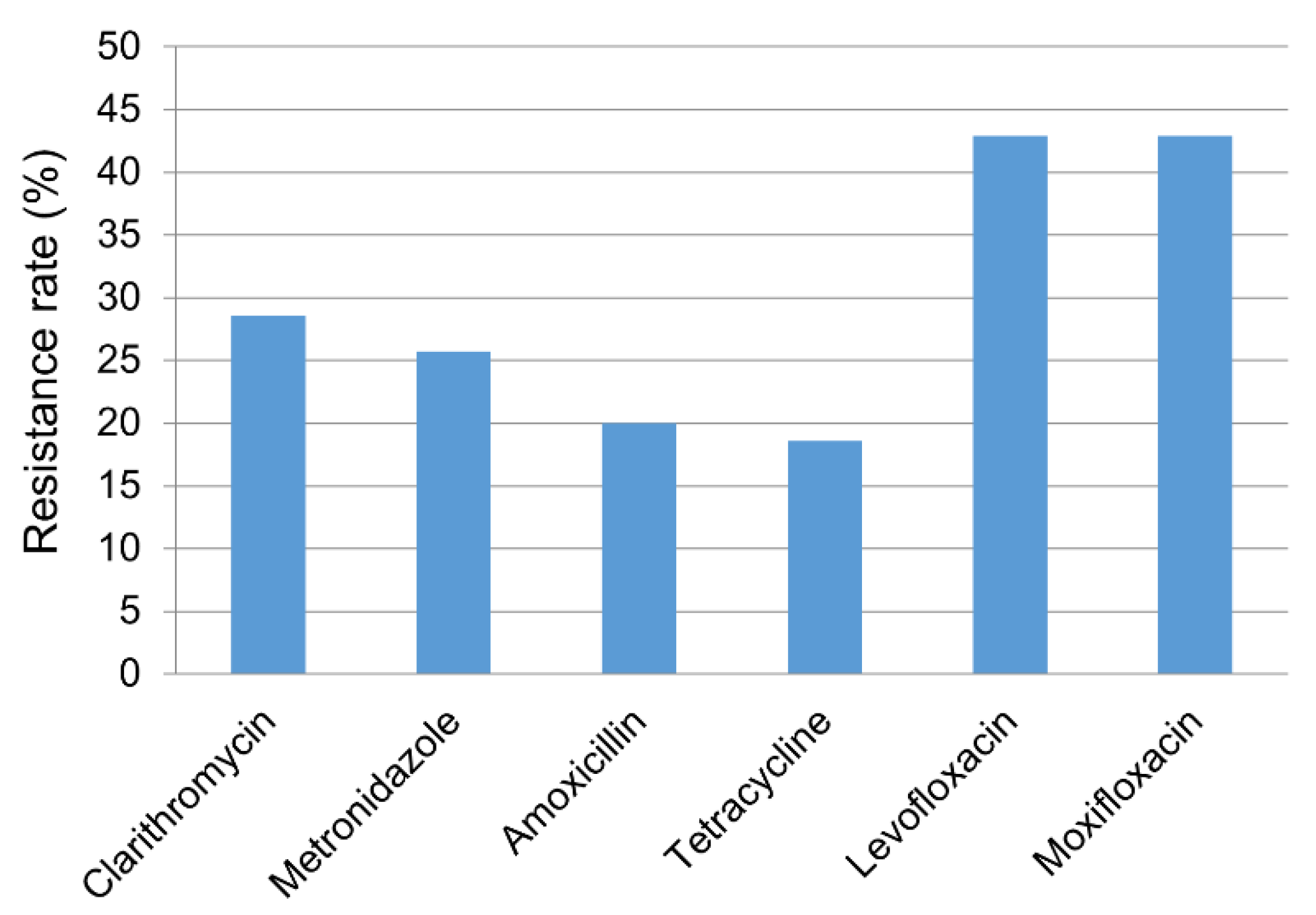
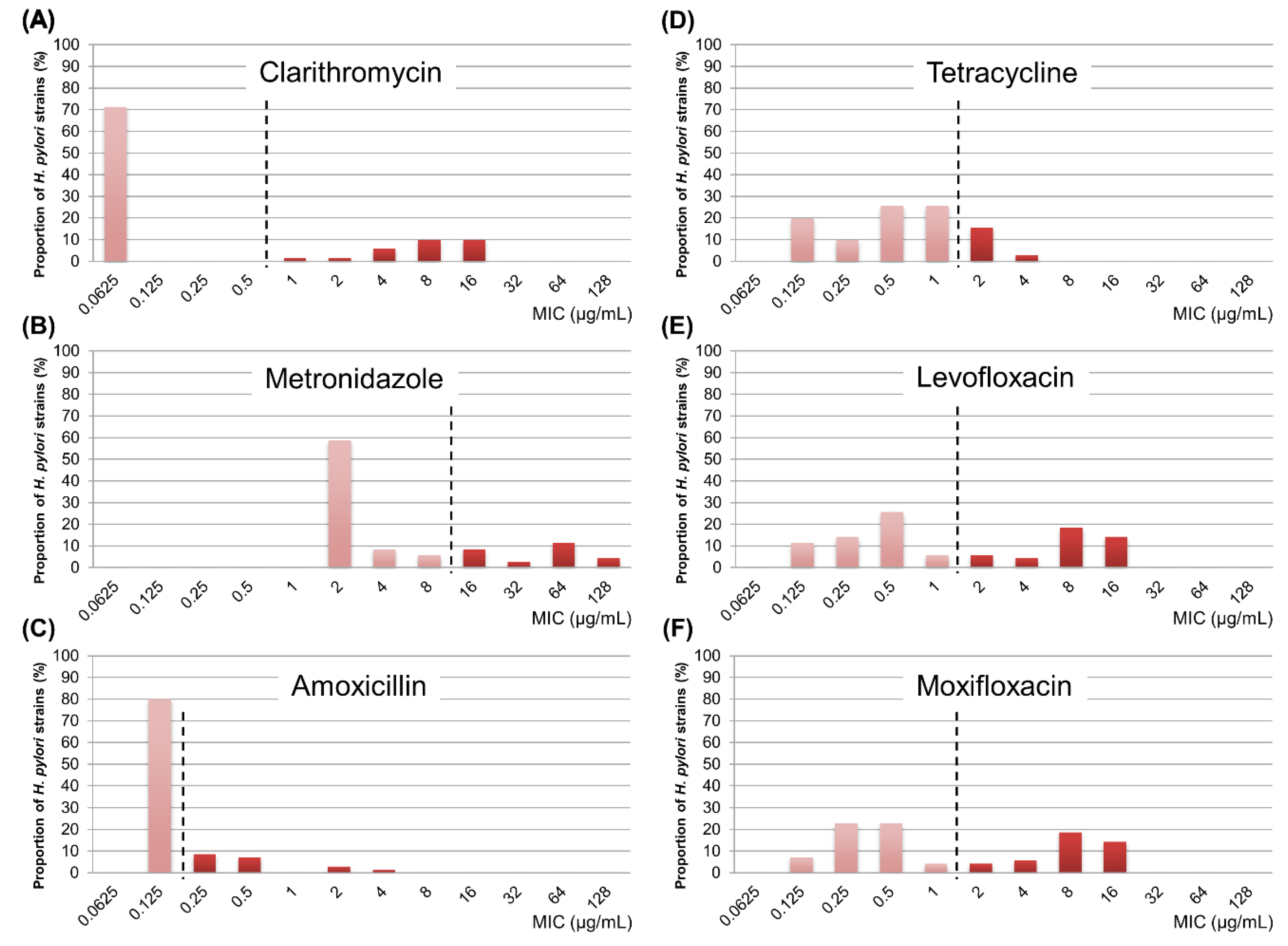
2.2. The Antibiotic Resistance Rates and MIC Profiles of H. pylori
2.3. Differences of Antibiotic Resistance According to the Site of Isolation
2.4. Profile of Multidrug Resistance among H. pylori Strains
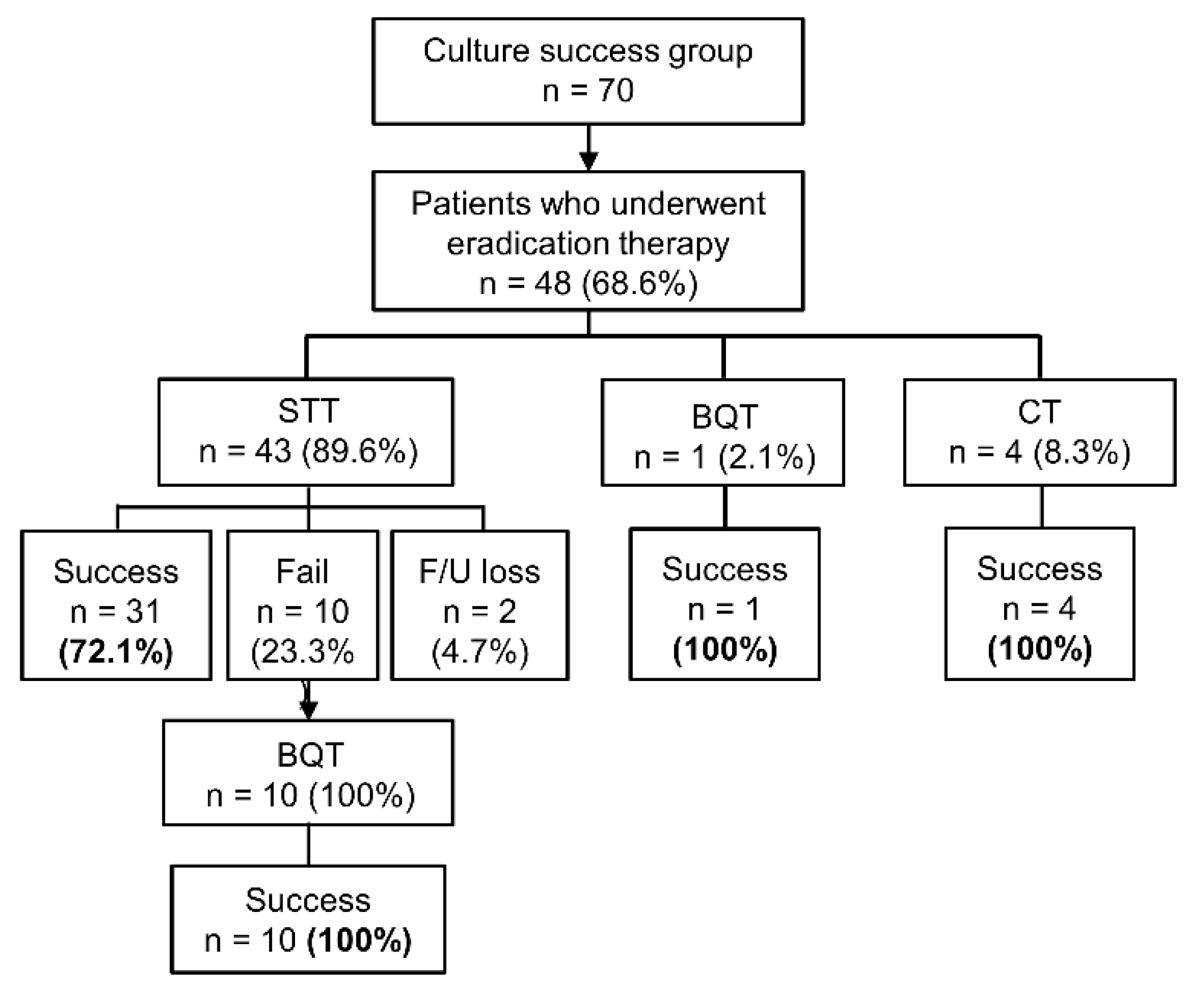
2.5. The Effect of Antibiotic Resistance on the Clinical Eradication Results
3. Discussion
4. Materials and Methods
4.1. Study Population
4.2. H. pylori Culture and Isolation
4.3. Determination of MICs of Antibiotics
4.4. Data Collection of Eradication Results
4.5. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Schistosomes, Liver Flukes and Helicobacter pylori. IARC Working Group on the Evaluation of Carcinogenic Risks to Humans. Lyon, 7–14 June 1994; IARC Publicatins: Lyon, France, 1994; Volume 61, pp. 1–241. [Google Scholar]
- Graham, D.Y.; Lew, G.M.; Klein, P.D.; Evans, D.G.; Evans, D.J., Jr.; Saeed, Z.A.; Malaty, H.M. Effect of treatment of Helicobacter pylori infection on the long-term recurrence of gastric or duodenal ulcer. A randomized, controlled study. Ann. Intern. Med. 1992, 116, 705–708. [Google Scholar] [CrossRef] [PubMed]
- Sung, J.J.; Chung, S.C.; Ling, T.K.; Yung, M.Y.; Leung, V.K.; Ng, E.K.; Li, M.K.; Cheng, A.F.; Li, A.K. Antibacterial treatment of gastric ulcers associated with Helicobacter pylori. N. Engl. J. Med. 1995, 332, 139–142. [Google Scholar] [CrossRef] [PubMed]
- Choi, I.J.; Kook, M.C.; Kim, Y.I.; Cho, S.J.; Lee, J.Y.; Kim, C.G.; Park, B.; Nam, B.H. Helicobacter pylori Therapy for the Prevention of Metachronous Gastric Cancer. N. Engl. J. Med. 2018, 378, 1085–1095. [Google Scholar] [CrossRef] [PubMed]
- Malfertheiner, P.; Megraud, F.; O’Morain, C.A.; Gisbert, J.P. Management of Helicobacter pylori infection-the Maastricht V/Florence Consensus Report. Gut 2017, 66, 6–30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chey, W.D.; Leontiadis, G.I.; Howden, C.W.; Moss, S.F. ACG Clinical Guideline: Treatment of Helicobacter pylori Infection. Am. J. Gastroenterol. 2017, 112, 212–239. [Google Scholar] [CrossRef]
- Savoldi, A.; Carrara, E.; Graham, D.Y.; Conti, M.; Tacconelli, E. Prevalence of Antibiotic Resistance in Helicobacter pylori: A Systematic Review and Meta-analysis in World Health Organization Regions. Gastroenterology 2018, 155, 1372–1382.e17. [Google Scholar] [CrossRef] [Green Version]
- Graham, D.Y.; Fischbach, L. Helicobacter pylori treatment in the era of increasing antibiotic resistance. Gut 2010, 59, 1143–1153. [Google Scholar] [CrossRef]
- Kim, B.J.; Kim, H.S. Online Registry for Nationwide Database of Current Trend of Helicobacter pylori Eradication in Korea: Interim Analysis. J. Korean Med. Sci. 2016, 31, 1246–1253. [Google Scholar] [CrossRef]
- Kim, T.H.; Park, J.M. Comparison of 7- and 14-Day Eradication Therapy for Helicobacter pylori with First- and Second-Line Regimen: Randomized Clinical Trial. J. Korean Med. Sci. 2020, 35, e33. [Google Scholar] [CrossRef]
- Mégraud, F. H pylori antibiotic resistance: Prevalence, importance, and advances in testing. Gut 2004, 53, 1374–1384. [Google Scholar] [CrossRef] [Green Version]
- Tai, W.C.; Lee, C.H.; Chiou, S.S.; Kuo, C.M.; Kuo, C.H.; Liang, C.M.; Lu, L.S.; Chiu, C.H.; Wu, K.L.; Chiu, Y.C.; et al. The clinical and bacteriological factors for optimal levofloxacin-containing triple therapy in second-line Helicobacter pylori eradication. PLoS ONE 2014, 9, e105822. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, S.Y. Time Trends in the Prevalence of Helicobacter pylori Infection and Future Directions in Korea. Korean J. Helicobacter Up Gastrointest. Res. 2016, 16, 123–128. [Google Scholar] [CrossRef]
- Lee, J.H.; Choi, K.D. Seroprevalence of Helicobacter pylori in Korea: A multicenter, nationwide study conducted in 2015 and 2016. Helicobacter 2018, 23, e12463. [Google Scholar] [CrossRef] [Green Version]
- Kim, S.E.; Park, M.I.; Park, S.J.; Moon, W.; Choi, Y.J.; Cheon, J.H.; Kwon, H.J.; Ku, K.H.; Yoo, C.H.; Kim, J.H.; et al. Trends in Helicobacter pylori eradication rates by first-line triple therapy and related factors in eradication therapy. Korean J. Intern. Med. 2015, 30, 801–807. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.H.; Ahn, J.Y.; Choi, K.D. Nationwide antibiotic resistance mapping of Helicobacter pylori in Korea: A prospective multicenter study. Helicobacter 2019, 24, e12592. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.Y.; Kim, N. Primary and secondary antibiotic resistance of Helicobacter pylori in Korea from 2003 to 2018. Helicobacter 2019, 24, e12660. [Google Scholar] [CrossRef]
- Jung, Y.S.; Park, C.H. Efficacy of Helicobacter pylori eradication therapies in Korea: A systematic review and network meta-analysis. Helicobacter 2017, 22. [Google Scholar] [CrossRef]
- Kim, B.J.; Lee, H. Ten-Day Concomitant, 10-Day Sequential, and 7-Day Triple Therapy as First-Line Treatment for Helicobacter pylori Infection: A Nationwide Randomized Trial in Korea. Gut Liver 2019, 13, 531–540. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.M.; Kim, J.S.; Jung, H.C.; Kim, N.; Song, I.S. Antibiotic resistance of Helicobacter pylori isolated from Korean patients in 2003. Korean J. Gastroenterol. 2004, 44, 126–135. [Google Scholar]
- Ghotaslou, R.; Leylabadlo, H.E.; Asl, Y.M. Prevalence of antibiotic resistance in Helicobacter pylori: A recent literature review. World J. Methodol. 2015, 5, 164–174. [Google Scholar] [CrossRef]
- Kim, J.M. Antibiotic resistance of Helicobacter pylori isolated from Korean patients. Korean J. Gastroenterol. 2006, 47, 337–349. [Google Scholar] [PubMed]
- Kim, J.J.; Reddy, R.; Lee, M.; Kim, J.G.; El-Zaatari, F.A.; Osato, M.S.; Graham, D.Y.; Kwon, D.H. Analysis of metronidazole, clarithromycin and tetracycline resistance of Helicobacter pylori isolates from Korea. J. Antimicrob. Chemother. 2001, 47, 459–461. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Choi, W.J.; Do, G.W.; Lee, G.H. Changes in the Antibiotic Resistance Rates of Helicobacter pylori Strains Isolated in Tertiary Medical Institutions in Seoul. Korean J. Med. 2014, 86, 308–313. [Google Scholar] [CrossRef]
- Hwang, T.J.; Kim, N.; Kim, H.B.; Lee, B.H.; Nam, R.H.; Park, J.H.; Lee, M.K.; Park, Y.S.; Lee, D.H.; Jung, H.C.; et al. Change in antibiotic resistance of Helicobacter pylori strains and the effect of A2143G point mutation of 23S rRNA on the eradication of H. pylori in a single center of Korea. J. Clin. Gastroenterol. 2010, 44, 536–543. [Google Scholar] [CrossRef] [PubMed]
- Graham, D.Y.; Lee, Y.C.; Wu, M.S. Rational Helicobacter pylori therapy: Evidence-based medicine rather than medicine-based evidence. Clin. Gastroenterol. Hepatol. 2014, 12, 177–186.e3; Discussion e112–e173. [Google Scholar] [CrossRef] [Green Version]
- Cuadrado-Lavín, A.; Salcines-Caviedes, J.R.; Diaz-Perez, A.; Carrascosa, M.F.; Ochagavía, M.; Fernandez-Forcelledo, J.L.; Cobo, M.; Fernández-Gil, P.; Ayestarán, B.; Sánchez, B.; et al. First-line eradication rates comparing two shortened non-bismuth quadruple regimens against Helicobacter pylori: An open-label, randomized, multicentre clinical trial. J. Antimicrob. Chemother. 2015, 70, 2376–2381. [Google Scholar] [CrossRef] [Green Version]
- Zullo, A.; Scaccianoce, G.; De Francesco, V.; Ruggiero, V.; D’Ambrosio, P.; Castorani, L.; Bonfrate, L.; Vannella, L.; Hassan, C.; Portincasa, P. Concomitant, sequential, and hybrid therapy for H. pylori eradication: A pilot study. Clin. Res. Hepatol. Gastroenterol. 2013, 37, 647–650. [Google Scholar] [CrossRef]
- The European Committee on Antimicrobial Susceptibility Testing. Breakpoint Tables for Interpretation of MICs and Zone Diameters, Version 6.0. Available online: http://www.eucast.org/clinical_breakpoints/ (accessed on 20 December 2016).
- Wu, J.Y.; Kim, J.J.; Reddy, R.; Wang, W.M.; Graham, D.Y.; Kwon, D.H. Tetracycline-resistant clinical Helicobacter pylori isolates with and without mutations in 16S rRNA-encoding genes. Antimicrob. Agents Chemother. 2005, 49, 578–583. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.W.; Kim, N.; Kim, J.M.; Nam, R.H.; Chang, H.; Kim, J.Y.; Shin, C.M.; Park, Y.S.; Lee, D.H.; Jung, H.C. Prevalence of primary and secondary antimicrobial resistance of Helicobacter pylori in Korea from 2003 through 2012. Helicobacter 2013, 18, 206–214. [Google Scholar] [CrossRef]
- Boyanova, L.; Hadzhiyski, P.; Kandilarov, N.; Markovska, R.; Mitov, I. Multidrug resistance in Helicobacter pylori: Current state and future directions. Expert Rev. Clin. Pharmacol. 2019, 12, 909–915. [Google Scholar] [CrossRef]
- Seo, J.W.; Park, J.Y.; Shin, T.S.; Kim, J.G. The analysis of virulence factors and antibiotic resistance between Helicobacter pylori strains isolated from gastric antrum and body. BMC Gastroenterol. 2019, 19, 140. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
{kind=link}
| Variables | Total Enrolled Patients | Patients with Successful H. pylori Culture (n = 70) |
|---|---|---|
| (n = 174) | ||
| Number of patients | 174 (100%) | 70 (100%) |
| Mean age ± SD (years) | 60.5 ± 13.1 | 61.2 ± 9.2 |
| Sex (male/female) | 100/74 (57.5%/42.5%) | 44/36 (62.9%/37.1%) |
| Endoscopic diagnosis | ||
| Peptic ulcer disease | 34 (19.5%) | 20 (28.6%) |
| Gastric cancer | 34 (19.5%) | 13 (18.6%) |
| Gastric adenoma | 17 (9.8%) | 5 (7.1%) |
| MALT lymphoma | 1 (0.6%) | 1 (1.4%) |
| Gastritis | 88 (50.6%) | 31 (44.3%) |
| Drug Resistance Profile | Subjects with Successful H. pylori Culture (n = 70) | Subjects with Resistant H. pylori Strains (n = 49) | ||||
|---|---|---|---|---|---|---|
| Resistant to 5 drugs | 1 (1.4%) | 1 (2.0%) | ||||
| C | M | A | T | Q | 1 (1.4%) | 1 (2.0%) |
| Resistant to 4 drugs | 2 (2.9%) | 2 (4.1%) | ||||
| C | M | A | Q | 1 (1.4%) | 1 (2.0%) | |
| M | A | T | Q | 1 (1.4%) | 1 (2.0%) | |
| Resistant to 3 drugs | 10 (14.3%) | 10 (20.4%) | ||||
| C | M | T | 1 (1.4%) | 1 (2.0%) | ||
| C | A | T | 1 (1.4%) | 1 (2.0%) | ||
| C | A | Q | 4 (5.7%) | 4 (8.2%) | ||
| M | A | Q | 2 (2.9%) | 2 (4.1%) | ||
| M | T | Q | 2 (2.9%) | 2 (4.1%) | ||
| Resistant to 2 drugs | 17 (24.3%) | 17 (34.7%) | ||||
| C | M | 3 (4.3%) | 3 (6.1%) | |||
| C | Q | 4 (5.7%) | 4 (8.2%) | |||
| M | Q | 4 (5.7%) | 4 (8.2%) | |||
| A | Q | 2 (2.9%) | 2 (4.1%) | |||
| T | Q | 4 (5.7%) | 4 (8.2%) | |||
| Resistant to 1 drug | 19 (27.1%) | 19 (38.8%) | ||||
| C | 5 (7.1%) | 5 (10.2%) | ||||
| M | 4 (5.7%) | 4 (8.2%) | ||||
| A | 2 (2.9%) | 2 (4.1%) | ||||
| T | 3 (4.3%) | 3 (6.1%) | ||||
| Q | 5 (7.1%) | 5 (10.2%) | ||||
| Drug Resistance Profile | Subjects with Successful H. pylori Culture (n = 70) | Subjects with Resistant H. pylori Strains (n = 44) | |||
|---|---|---|---|---|---|
| Resistant to 4 drugs | 1 (1.4%) | 1 (2.3%) | |||
| C | M | A | T | 1 (1.4%) | 1 (2.3%) |
| Resistant to 3 drugs | 4 (5.7%) | 4 (9.1%) | |||
| C | M | A | 1 (1.4%) | 1 (2.3%) | |
| C | M | T | 1 (1.4%) | 1 (2.3%) | |
| C | A | T | 1 (1.4%) | 1 (2.3%) | |
| M | A | T | 1 (1.4%) | 1 (2.3%) | |
| Resistant to 2 drugs | 11 (15.7%) | 11 (25.0%) | |||
| C | M | 3 (4.3%) | 3 (6.8%) | ||
| C | A | 4 (5.7%) | 4 (9.1%) | ||
| M | A | 2 (2.9%) | 2 (4.5%) | ||
| M | T | 2 (2.9%) | 2 (4.5%) | ||
| Resistant to 1 drug | 28 (40.0%) | 28 (63.6%) | |||
| C | 9 (12.9%) | 9 (20.5%) | |||
| M | 8 (11.4%) | 8 (18.2%) | |||
| A | 4 (5.7%) | 4 (9.1%) | |||
| T | 7 (10.0%) | 7 (15.9%) | |||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, J.Y.; Shin, T.-S.; Kim, J.H.; Yoon, H.J.; Kim, B.J.; Kim, J.G. The Prevalence of Multidrug Resistance of Helicobacter pylori and Its Impact on Eradication in Korea from 2017 to 2019: A Single-Center Study. Antibiotics 2020, 9, 646. https://doi.org/10.3390/antibiotics9100646
Park JY, Shin T-S, Kim JH, Yoon HJ, Kim BJ, Kim JG. The Prevalence of Multidrug Resistance of Helicobacter pylori and Its Impact on Eradication in Korea from 2017 to 2019: A Single-Center Study. Antibiotics. 2020; 9(10):646. https://doi.org/10.3390/antibiotics9100646
Chicago/Turabian StylePark, Jae Yong, Tae-Seop Shin, Ji Hyun Kim, Hong Jip Yoon, Beom Jin Kim, and Jae Gyu Kim. 2020. "The Prevalence of Multidrug Resistance of Helicobacter pylori and Its Impact on Eradication in Korea from 2017 to 2019: A Single-Center Study" Antibiotics 9, no. 10: 646. https://doi.org/10.3390/antibiotics9100646
APA StylePark, J. Y., Shin, T. -S., Kim, J. H., Yoon, H. J., Kim, B. J., & Kim, J. G. (2020). The Prevalence of Multidrug Resistance of Helicobacter pylori and Its Impact on Eradication in Korea from 2017 to 2019: A Single-Center Study. Antibiotics, 9(10), 646. https://doi.org/10.3390/antibiotics9100646