3. Results
3.1. Characteristic of Examined and Control Groups
In the study group with the etiological record of erosion, 7 patients reported (currently or in the past) anorexia, 14 bulimia and 1 gastroesophageal reflux disease (GERD). In addition, 5 patients reported both anorexia and bulimia disorders, and 2 more anorexia, bulimia and GERD. One patient reported the combined incidence of anorexia and GERD. Based on the questionnaire study, 21 patients experienced vomiting, occurring at a frequency ranging from several episodes a month to 7 times a day. In 25 patients, a record of co-existence was also associated with erosiogenic factors associated with a frequent consumption of food with a low pH index. Some of the patients reported taking medications that could affect the formation of erosive changes (anti-depressants, 21; calming drugs, 10; medication that irritates the mucous membrane of the gastrointestinal tract, 1). Twenty five patients scored higher than 20 points in the Eating Attitude Test-26, which corresponds to the probability of eating disorders, and the range of scores in the study group ranged from 2 points to 72 points. In 18 patients in the study group, symptoms of temporomandibular joint dysfunction were recorded (according to the Hellkimo index).
All patients in the control group had a record of frequent acidic food intake, and some patients reported taking drugs that could have an erosive activity. In this group, 5 people reported taking antidepressant drugs and 2 people reported taking sedatives. All control patients in the EAT-26 scored less than 20 points. In 13 people, symptoms of temporomandibular joint dysfunction were reported (according to the Hellkimo index).
3.2. Results Regarding Examination Times in the Assessment of Particular Indices
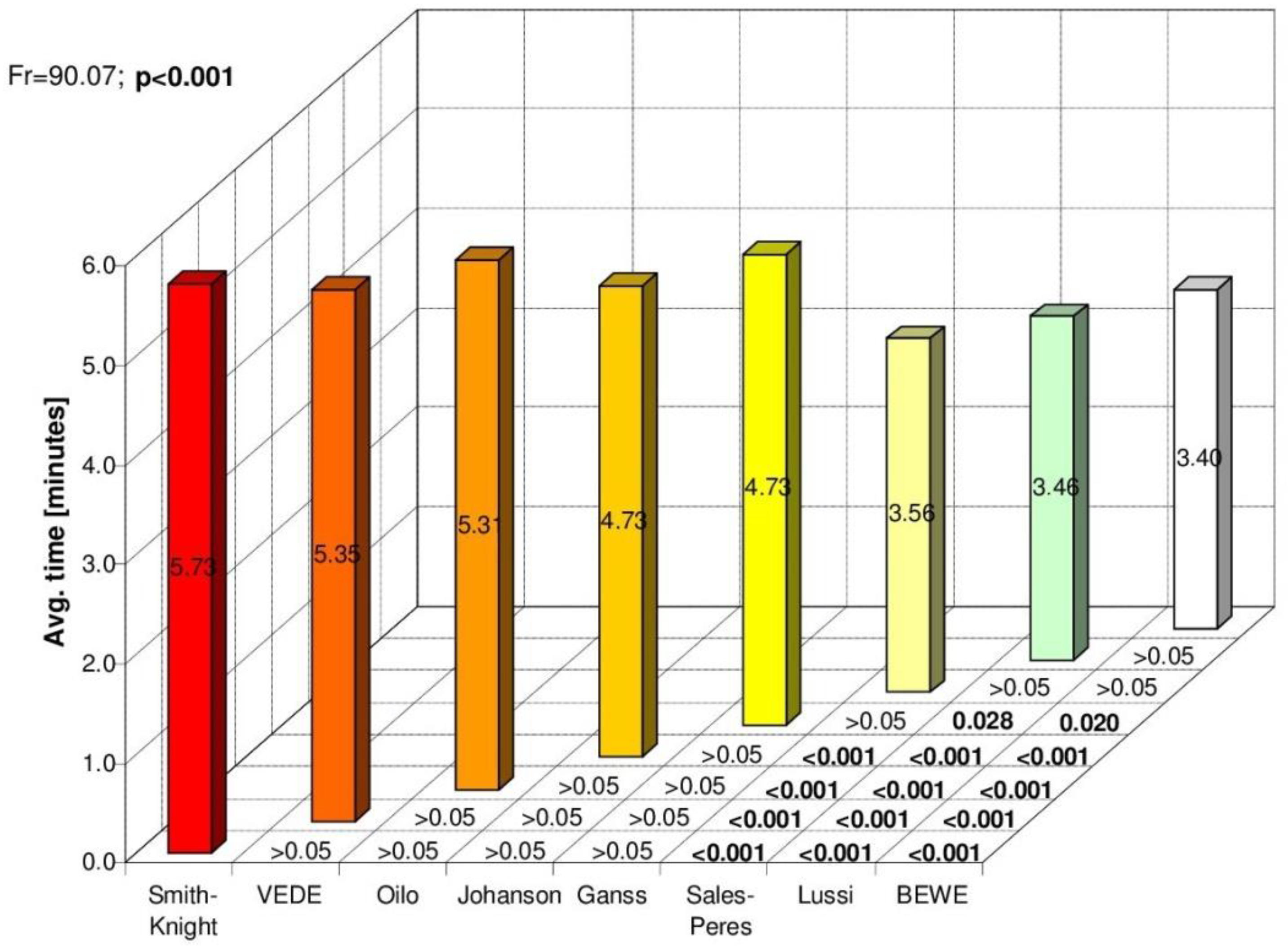
There were statistically significant differences between the test and control groups in the duration of the test using individual indices of tooth wear/erosion with respect to the following indexes: BEWE, TWI with the de Carvahlo Sales-Peres et al. modification, Oilo et al. and Johansson et al. In all of the above cases, longer examination times were obtained in the study group (
Table 4).
The largest differences in the study group occurred between the average examination time (minutes) using the Tooth Wear Index according to Smith and Knight (VEDE) and the following indexes: BEWE, Lussi’s and TWI modified by de Carvahlo Sales-Peres et al. Differences were observed within the control group in the same way as above (
Figure 1 and
Figure 2).
Based on the questionnaire study in the subjective assessment of patients in both the study and control groups, it was shown that the examination time for the following indexes: Lussi’s, TWI modified by de Carvahlo Sales-Peres et al., BEWE, VEDE and Oilo et al., was most often described as ‘short’, while Smith and Knight’s Tooth Wear Index was described as ‘average’.
Patients in the study group most often determined the examination times of Johansson’s and Linkosalo and Markkanen’s modified by Ganss et al. indices as ‘average’, whereas the control group described those examinations as ‘short’.
3.3. Subjective Assessment of Indices by Patients
While analyzing the patients’ answers to the questionnaire, which concerned the subjective perception of the least bothersome assessment of the patient’s tooth wear/erosion index, no statistically significant differences were found in the frequency of selecting ‘the least bothersome’ answer when comparing the examined group and the control group. In the answers to the question, it being an attempt to compare the indexes and the visits (indexes: TWI according to Smith and Knight, Lussi, Johansson et al.), there were statistically significant differences among the patients in the study group (χ2 = 22.28; p < 0.001). The Lussi’s index was assessed by the patients of this group to be significantly higher than the TWI and Johansson’s indexes.
In the control group, the Lussi’s index was also chosen as not too bothersome. Likewise, in this group, the worst assessments from the first visit were obtained by the Johansson et al.’s index. Between Lussi’s, Smith and Knight’s TWI and Johansson et al.’s indexes there were statistically significant differences (χ2 = 23.25; p < 0.001).
Answers to the questions regarding the evaluation of indexes during the second visit (TWI modified by de Carvahlo Sales-Peres et al., BEWE, Linkosalo and Markkanen’s modified by Ganss et al.) proved that the patients of the test group significantly more advantageously (χ2 = 14.32; p < 0.001) assessed the TWI by de Carvahlo Sales-Peres et al., and the BEWE index than the Linkosallo and Markkanen’s index modified by Ganss et al. The evaluation of these indexes by the control group was similar (χ2 = 28.37; p < 0.001).
The analysis of the responses to questions from the patient questionnaire in the aspect of an evaluation of indexes during the third visit (VEDE, Oilo et al.,) showed that both groups were more favorably assessed by the Oilo et al. index, with statistically significant differences between the indexes only observed within the control group (χ2 = 4.435; p = 0.035).
Subsequently, the most frequently selected indexes during the first, second and third visit within each group were compared. The indexes of Lussi, BEWE and Oilo et al., were best evaluated by the patients of the study group, while patients from the control group chose the following indexes as the least bothersome: Lussi, BEWE, TWI modified by de Carvahlo Sales-Peres et al., and the Oilo et al. index. In the control group, the BEWE and TWI modified by de Carvahlo Sales-Peres et al. indexes were selected at a similar frequency for being the least bothersome. When comparing the sets of indexes chosen by patients as optimal within the studied group (χ
2 = 2.06,
p = 0.357) and within the control group (χ
2 = 2.61,
p = 0.455), there were no statistically significant differences in the frequency of their selection (
Table 5).
The statistical analysis showed that there were no statistically significant differences in the frequency of selection of non-etiological indexes as compared to etiological indices chosen as the optimal set in the case of the two groups (χ2 = 0.333, p = 0.564).
When asked about the possible feeling of anxiety and embarrassment during the VEDE and Oilo et al.,’s tests, most patients of both groups denied such an occurrence during this procedure. As for the assessment of possible discomfort in posing for digital photographs of the oral cavity, the prevailing opinion was its absence, with fewer answers confirming some discomfort felt but only to a small extent, both in the control group and in the study group.
Patients of both groups did not feel anxiety or self-restraint while carrying out tests using individual assessment of tooth wear/erosion indices, with the exception of indices related to the making of impressions. During the test using the Johansson’s index, 30% of patients in the study group did not feel anxiety or embarrassment during the whole examination; however, another 30% indicated that they were anxious and slightly embarrassed. In the assessment of the study by the indices according to Linkosalo and Markkanen as modified by Ganss et al., a similar relationship occurred among the control group of patients. Patients of the study group slightly more frequently chose the answer ‘occurrence of anxiety and embarrassment, but only slight’. The impressions themselves were assessed by the majority of patients in both groups as ‘discomfort to a small extent’ in the case of both indices. It should be noted, however, that 6 patients from the study group and 4 patients from the control group used the option to refuse to take part in the making of impressions during the second visit (index modified by Ganss et al.). All respondents explained their decision in writing as being due to unpleasant sensations while taking impressions during the first visit (Johansson et al.’s index).
3.4. Subjective Assessment of the Indices by the Operator
The analysis of the response to the questionnaire of the operator’s questionnaire showed that in the operator’s subjective assessment of the time needed to examine the patient with the use of individual tooth wear/erosion indexes, there were statistically significant differences (χ
2 = 258.9;
p < 0.001) between all indexes selected in the study. The time of testing using Smith and Knight’s TWI and VEDE indices was most often referred to by the operator as ‘too long’. In the case of Johansson’s, Linkosalo and Markkanen’s modified by Ganss et al. and Oilo et al., it was described as ‘average’. The research using the indexes by
Lussi, de Carvahlo Sales-Peres et al. (TWI) and BEWE was described as ‘short’ (
Table 6).
Both in the case of the set of non-etiological and etiological indices, the subjective operator’s assessment of the degree of scale development and the degree of difficulty in assimilating the evaluation criteria and the index application algorithm were usually referred to as ‘average’. There were statistically significant differences between the selected indices in the aspect of the extension of scales and the degree of difficulty in assimilating their assessment criteria.
Based on the answer to the question regarding the degree of difficulty in the preparation of diagnostic aids accompanying the study, there were no statistically significant differences (χ2 = 0.742; p = 0.690) between the difficulty of preparing impressions according to Johansson et al. or Linkosalo and Markkanen modified by Ganss et al. Such differences (χ2 = 41.91; p < 0.001) occurred for the level of difficulty in preparing digital photography in the suggested projections accompanying the VEDE and Oilo et al. indexes. In that case, preparation of photos was assessed as less troublesome and laborious during the course of study as recommended by Oilo et al.’s index.
The operator’s opinion about the length of time needed to prepare diagnostic help was similar. In the case of models, there were no statistically significant differences (χ2 = 5.483; p = 0.064) between the indexes of Johansson et al. and Linkosalo and Markkanen modified by Ganss et al. However, they occurred (χ2 = 23.07; p < 0.001) in assessing the length of time needed to prepare digital photographs. In the case of the Oilo et al.’s index, this time was more often subjectively assessed by the operator as short or average, while in the case of the VEDE index, as average or long. In the subjective assessment of the operator regarding the usefulness of models in the assessment of changes, statistically significant differences were found (χ2 = 35.31; p < 0.001) in the case of indexes using models. That usefulness was usually assessed as small or average in the case of the Johansson et al.’s index, while in the case of the index modified by Ganss et al., the answers small, average and significant were more evenly distributed.
While considering subjective opinions of the operator in the aspect of the usefulness of digital photographs of the oral cavity in an assessment of tooth wear/erosion changes, it was found that, in the case of the VEDE index, this usefulness was most often assessed as significant, while in the case of Oilo et al., it was average. However, there were no statistically significant differences between these indexes (χ2 = 2.267; p = 0.322). In the case of indices which use diagnostic models, the convenience of archiving these diagnostic aids was most often assessed by the operator as small, and in the case of indices which use digital photographs, as significant.
4. Discussion
The evaluation of the different research tools/indices selected for this study also required account to be taken of the limitations of this project. The main one, in the author’s opinion, was the lack of gender diversity within the study group compared to the control group. In the control group, nearly 67% were women, while in the study group it was 100%. At the center for the treatment of neuroses and eating disorders, after the preliminary information about the planned studies, a desire to participate in them was expressed by several men; however, they did not meet the criteria for inclusion in the study (they were treated for neurosis, not eating disorders). In developing the project’s initial assumptions, the authors decided to randomly qualify the patients who met the inclusion criteria for tooth wear/erosion and who are not disqualified by gender.
When taking a summary of the results, it should be noted that the specificity of the study group could have a potential impact on the preference results in relation to the used indices. In the scientific literature concentrated on the analysis of the condition of this group of patients, specific characteristics affecting the quality of contact and the way in which the proposed medical procedures are performed are highlighted. Increased levels of anxiety can be expected during the selected dental procedures, mainly due to the presence of foreign matter in the mouth during the examination (mirror). Of great importance for these patients is the necessity to meticulously inform them about the course of individual procedures accompanying the planned oral examinations. It is also necessary to take into account the association of the occurrence of eating disorders with the increased vegetative reactions of the body. The influence of the environmental conditions and organoleptic properties of materials and tools to obtain diagnostic models on the subjective reception of the course of the study in patients with eating disorders must not be overlooked. In addition, some authors highlight the gender preferences of patients with eating disorders with regards to the doctors and medical staff [
1,
11,
17].
In the case of the Smith and Knight’s TWI index, the literature draws attention to its usefulness both for individual research and in epidemiological studies. This index is considered to be closest to the ‘golden standard’ in studies of losses of non-carries origin. Its non-etiological formula allows for the evaluation of multifactor wear. The high reliability and validity of this research tool is often emphasized. The only doubts concerning this index arise from the inclusion of the criterion of ‘exposed dentin’, which is not considered very reliable. However, it is used in a large number of research works, which has a positive effect on the possibility of comparing their results [
18,
19,
20,
21,
22,
23,
24,
25,
26]. Smith and Knight emphasized that the average TWI test time does not exceed 5 min, including the time needed to clean the tooth surface. However, in the present study, the mean time of examination with this index was 5.60 min for patients in the study group and 5.45 min for patients in the control group. Bardsley, Taylor and Milosevic developed a simplified version of this index in order to limit the time of the examination, due to the fact that their research was epidemiological, taking into account a large sample group of patients [
22,
27].
In our own studies, no statistically significant differences were found between the control group and the study group as regards the length of the examination times using Smith and Knight’s TWI index. In the assessment of examination time, the most common term among patients in both groups was ‘average’. In the subjective opinion of the operator, it was usually perceived as too long. The advantages of the TWI index described in the literature were not reflected in the evaluations of the participants in this research in terms of simplicity of its application/submission to the study using it. In this aspect, within the indexes of the first visit, the research group assessed that index as significantly more difficult/more embarrassing than the Lussi’s index. Similarly, in the set of the most-chosen as the best, easy-to-use indexes of all three visits, Smith and Knight’s Tooth Wear Index was not mentioned by any of the groups.
The operator’s opinion on the subject of the examination using this index seems to be similar to the patients’ opinions. The most frequent answers were: “difficult, extended assessment criteria”, followed by “too long examination time”, “difficult assessment of the neck and buccal surfaces of the upper third molars included in the index”. Taking into account the difficulty to use complicated and extensive criteria, attention was also paid to the importance of good cooperation and the positive attitude of patients during the examination. The advantages of the index mentioned by the operator include those easy to remember and only one group of teeth was rejected from the assessment, which were “teeth with extensive restorations filled tightly”.
However, Donachie and Walls, in their article demonstrating the need to modify the TWI for the elderly population, criticized the issue of exclusion from teeth with extensive fillings assessment. According to them, fillings in the Black’s class V Black may mask a significant degree of wear [
28]. The operator primarily emphasized accuracy as an advantage of using this index. When analyzing the results of our own research, the conclusion is that this index seems to be more useful for studying the wear of an individual patient than a large group of them.
The Lussi’s index is regarded almost as the ‘golden standard’ among those indexes that take into account the etiology of changes. Studies highlight high results in both components of reliability, simplicity of use, and ease of comparison of results obtained from independent research [
18,
29,
30]. In our own research, the patients of both groups evaluated the examination time using this index as ‘favorable/short’. Mean examination times were only 3.43 min for the study group and 3.32 min for the control group. The short duration of the examination is also raised by the operator as the main advantage of this index. In the opinion of the patients of the study group, the Lussi’s index turned out to be statistically significantly simpler/less embarrassing than the remaining indexes of the first visit. In the free, subjective opinions of patients in the course of the examination, the following opinions prevailed: short, non-invasive, comfortable examination. When assessing the indexes for examinations carried out without using diagnostic aids, resembling a standard dental review, the significance of obtaining earlier accurate information and predictability of applied procedures was reported only by patients from the study group.
As one of the disadvantages of using the index, the operator reported the presence of two separate scales to assess the labial/cheek, occlusal surfaces and incisal edges. Despite this, the evaluation criteria were still assessed as easy and understandable. The Lussi’s index takes into account the criterion of exposed dentine, but its creator emphasizes a much easier use of this criterion when it is not considered = in relation to 1/3 of the test area (as is the case for TWI and VEDE indices), but up to 1/2 of the tested area [
29]. The opinion of the operator conducting the Lussi’s index examination was similar in this respect.
The TWI modification created by de Carvahlo Sales-Peres et al. for epidemiological purposes was distinguished in our research by the short time needed to conduct the examination [
16]. Time values were similar to those obtained during the Lussi’s index, but in the case of de Carvahlo Sales-Peres et al.’s modification, the examinations of the control group were statistically significantly shorter than in the study group. According to our own observations, patients with eating disorders (which in their free written statements emphasized the importance of obtaining accurate information) were already slightly encouraged after the first visit. During de Carvahlo Sales-Peres et al.’s TWI examination, which was the first index during the second visit, they used the course of the study to ask a lot of questions about their state of teeth and methods of prevention and treatment of non-carious lesions. The same regularity was applied to the BEWE index. The third visit was dominated by the acquisition of oral photographs and generally a large amount of equipment was used for those procedures; questions about the state of teeth were almost never asked by the patients. Thus, it seems that the statistically significant difference in the length of the examination time with these indices (TWI modified by de Carvahlo Sales-Peres et al. BEWE) between the study group and the control group may have some psychological explanation.
Among the indexes of the second visit, the TWI modification was assessed by both groups as an easier/more favorable examination than the Linkosalo and Markkanen’s index modified by Ganss et al. There were statistically significant differences in the assessment of these indices. In the list of the most optimal metrics out of all three visits, the TWI by de Carvahlo Sales-Peres et al. received recognition among patients in the control group, where it was selected as optimal with a similar frequency as the BEWE index. In any written statements of patients about the course of the examination, frequent descriptions of these two indexes are similar and ‘almost indistinguishable’. It seems, therefore, that due to the similarity of the examination times and algorithms used by these indexes from the point of view of the examined person, the main differences in their assessment may come almost exclusively from the operator conducting the study. It draws the most attention to simplicity, transparency and ease of remembering the assessment criteria, short examination time, and index universalism. In 16 cases, the operator drew attention to their feelings of an easier, more comfortable carrying out of the TWI procedure in the modified version. It should be noted that the de Carvahlo Sales-Peres et al. TWI version, which, unlike the original, does not take into account the degree of exposed dentin, obtained higher results in reliability tests [
16]. As a drawback, the operator listed a large number of groups of teeth classified in category 9, which means teeth rejected from the assessment. This may seem difficult to remember and may lead to a lack of therapeutic indexes (in comparison with the BEWE). These few flaws, however, do not change the fact that from the viewpoint of the operator, this index appears to be a tool covering the largest number of issues/advantages among all the indexes selected for this study.
The average duration of the examination while using the BEWE index differed in a statistically significant way in the study group from the mean duration of the examination in the control group. The control group was tested for a shorter period, similarly to the case of the TWI index modified by de Carvahlo Sales-Peres et al. Both the patient groups and the operator perceived the examination time as short. The prevailing opinion among all participating patients was that in comparison with the algorithm of other selected indexes, the BEWE index test method was one of the least troublesome procedures for them. It has been evaluated as being more advantageous in a statistically significant manner, e.g., from the method of the Linkosalo and Markkanen’s index modified by Ganss et al. These assessments are in line with Lussi’s opinion that the index is a modern, simplified and easily applicable research tool in all conditions [
31]. A similar opinion was reported by the operator conducting the examination. In the comments section, which is an element of the operator’s questionnaire, the most frequent opinions were related to the short examination time (23.6% of all operator’s comments on the research method with this index), clarity and transparency of the evaluation criteria used (21.7%) and the easy-to-remember system of sextants (17.9%). The operator also emphasized the advantages of the presence of therapeutic indices, assigned to the appropriate ‘BEWE score sum’ thresholds, which, according to Bartlett, Ganss and Lussi’s intention while creating this tool, was to significantly contribute to facilitating the doctor’s future decisions regarding solving the problem of erosion in a given patient [
32]. As an advantage of the BEWE system, the literature cites no need to distinguish the degree of exposed dentin, which translates into the ease of distinguishing between types 2 and 3 of the index. This fact was recognized in the operator’s opinions, but was mentioned infrequently (3.8% of opinions). According to the operator, the disadvantage of the BEWE index was its etiological character, which may seem a little less universal. Analogical considerations were expressed by Young et al. in an article that analyzes the validity of the erosion assessment criteria [
33]. Summing up, in own research, the BEWE index, together with the Lussi’s and TWI modified by de Carvahlo Sales-Peres et al., achieves the status of one of the leading choices for the study of tooth wear/erosion rates in terms of optimality of use, from the point of view of the physician and both groups of patients.
In the case of the examination conducted according to the Johansson et al.’s index, the time needed to test the control group was on average 47 s shorter, which was a statistically significant difference. Similarly, patients in the study group perceived the examination as subjectively longer than those in the control group. Considering the aspect of ‘optimum use based on the feelings of being subjected to a patient’s examination’, this rate was assessed by patients of both groups as the worst among the indexes of the first visit was statistically significantly worse than the Lussi’s index.
Even though the majority of the members of both groups marked the level of anxiety, embarrassment or discomfort as “present but low” while completing the patient questionnaire, somewhat different conclusions arose in the analysis of subjective, written opinions of patients on the topic of taking impressions, especially in relation to patients with eating disorders. During the assessment of this procedure, psychological aspects of the examination such as the predictability of the examination and trust in the dentist (three times more often than in the control group), anxiety caused by the occurrence of negative dental experiences from the past were expressed in the examined group more often than issues of somatic feelings (possible pain, discomfort, too many items in the mouth). Both groups reported the occurrence of the gag reflex with a similar frequency, but greater difficulty in breathing was reported by as much as 25% of patients in the test group and was reported more than in the control group. In contrast, the issue of the occurrence of retching in patients of both groups was differently expressed by the operator. The analysis of their remarks shows that the occurrence of the gag reflex during the taking of impressions was twice as frequent in the patients of the test group than in the control group. In addition, the feeling of an anxious attitude or poor cooperation on the part of the patient during the procedure was reported 24% more often in patients with eating disorders.
On the basis of the feelings accompanying the taking of impressions using Johansson et al.’s algorithm, some patients refused to take part in that procedure during the next visit. Patients in the study group accounted for as much as 60% of this group. Larsen et al. state that the use of plaster models based on alginate impressions to assess early erosive lesions does not actually fulfill its role due to the poorly reflected small details of the surface patterns. These authors, however, emphasize the general advantages of impressions accompanying the clinical examination, ensuring that the use of materials recommended by them (silicone masses, models of epoxy resins) for the assessment of the models sometimes allows to capture subtle changes in the surface, which cannot be found in a clinical study [
34]. In our own research, the usefulness of models in assessing changes according to the Johansson et al.’s index was assessed by the operator as “little” or “average”. The opinion of the operator does not coincide with the opinion of Ganss et al., who mention the numerous advantages of using models for assessing changes, such as: the possibility of evaluating repeatedly, in convenient lighting conditions, the freedom to choose the time of the implementation [
20]. A similar opinion is expressed by Hooper et al. [
14] In our own research, from the operator’s point of view, the prevalence of an examination combined with a clinical trial was emphasized, in comparison with the index use scheme, where the assessment of the tooth surface was carried out only on the basis of an analysis of diagnostic models. The lack of an ability to evaluate the optical properties of the enamel, such as gloss or color, made it difficult to assess the early changes in the model, especially those according to the index use scheme: alginate impressions were used and the models were cast from gypsum. This confirms the opinion of Larsen et al. on the limitations of those materials in the assessment of the described changes [
34]. Another limitation of this study was the omission of an assessment of progression changes while using indexes that include an assessment of plaster models. The Johansson et al. index, in its original version, also contained a separate scale to assess the progression of changes over time, with the evaluation being based on models cast from impressions taken 18 months apart [
23]. Despite the high reliability of the results obtained by this research tool, its assessment from the point of view of the participants in this study was less favorable than it was the case with other tooth wear/erosion indexes.
There were many analogies between the evaluation of examination using the following indexes: Johansson et al.’s as well as Linkosalo and Markkanen’s modified by Ganss et al. Similar to the case of Johansson et al.’s index, the objective average time of the examination while using the index modified by Ganss et al. was statistically significantly longer than the analogous time for the control group. Certainly, a significant limitation of the assessment of the examination time with these indexes was that only the time of taking diagnostic aids in the surgery was measured. It did not take into account the time needed to prepare plaster models in the technician’s workshop and their evaluation by the operator. However, this issue was reflected in the subjective opinions of the operator on the research using these indexes and the results of the assessment in terms of the convenience of archiving and storage of diagnostic models, which they assessed as ‘little’. From the operator’s point of view, the degree of difficulty and the time of preparation of impressions was similar to that of Johansson et al. In the subjective perception of the control group of patients, the time of the examination following Ganss et al.’s modification seemed ‘short’, whereas the group with eating disorders and the operator conducting the test reported it as ‘average’. Similarly, as in the case of the indexes of the first visit, also among the tools selected for research during the second visit, the index associated with taking impressions was assessed as the most troublesome/least optimal for the patients of both groups. The differences between the indexes presented here were statistically significant for both groups of patients.
Subjective written comments of the patients over the course of the examination conducted with the Ganss et al.’s index were analogous with the comments regarding the previous index, and some patients refused to participate in the study, explaining in writing their fear and unpleasant sensations while taking previous impressions. A surprising conclusion is that as many as 53% of the study group and 26% of the control group reported the organoleptic properties of the impression material, such as its taste, appearance, smell or temperature, as being important issues. The main disadvantages of this index, from the operator’s point of view, included the lack of an accompanying clinical trial, as already described in the case of Johansson et al. It was difficult to distinguish the tooth tissues from the solid fillings present in it without the possibility of assessing the color or level of translucence. The issue of the quality of the impression and the model was of key importance here. In the case of this index, the operator also clearly emphasized the importance of the degree of cooperation on the part of the patient.
In the case of difficult cooperation, the ability of a more accurate analysis of the possible erosion occurring in the area of the last teeth of the arch, which would be impossible during a clinical trial, was a certain advantage of the models. For the physician conducting the examination, it was also easier to apply the indexes that used one unified scale to assess all the present tooth surfaces, than those in which the assessment included two separate scales with different criteria. In its original version, the index was used for epidemiological and long-term assessment of the degree of erosion in children and adolescents on the basis of models taken for orthodontic purposes within an interval of 5 years [
20]. The ability to assess the progression of changes over time is an indisputable advantage of this method. The results of our own research, however, suggest that the use of research tools in which the analysis of plaster models serve as the basis for tooth assessment is more justified when we already have ready models previously made for other therapeutic and diagnostic purposes [
14,
20]. This is indicated by more favorable assessments of other indexes for tooth wear/erosion tests for both groups of patients, as well as for the operator conducting the examination. The index, in which the performance of impressions and models was strictly planned to assess the wear/erosion, was, for example, Larsen et al.’s index. However, it did not gain widespread approval due to its time-consuming and complex quantitative and qualitative criteria [
18,
34].
Average study times with the Visual Erosive Wear Examination Index (VEDE) did not show statistically significant differences between the groups and fluctuated around 5.5 min. Therefore, that time was only slightly shorter than the examination using the most time-consuming of the indexes selected for the study, which was the TWI. Despite the fact that, objectively, they achieved similar values in terms of minutes, the VEDE examination seemed shorter in the subjective perception of the patients. The operator described the examination time as “too long” in the case of both indices. Most patients in both groups indicated in the survey that they did not feel fear or embarrassment while taking digital photographs of their oral cavities. On the other hand, the negative feelings associated with the presence of expanders in the mouth appeared three times more often among patients in the study group than in the control group. The opinion of the operator shows that lip stretching with the expander was more often perceived as oppressive and caused an unattractive facial appearance in the study group, which may be explained by the elevated level of anxiety and narcissism in these patients, which was proven in scientific publications [
11,
35]. Of all the patients who, in their examination descriptions, complained about too many objects being in their mouth during the examination, patients with eating disorders constituted a group 14% greater than the control group. At the same time, the same percentage distribution occurred when describing the study as ‘an interesting, new experience’.
According to the answers given in the operator’s questionnaire, the time devoted to the preparation of diagnostic aids was usually referred to as ‘average’ or ‘too long’. However, they perceived the convenience of archiving images and their considerable usefulness to evaluate erosive changes as the undoubted advantages of the VEDE index. The presence of a very good, accurate and helpful photo index, accompanied by an algorithm describing its use, is a crucial advantage, as it significantly facilitates assigning the stage of development of changes to the appropriate category. This opinion coincides with the results of research carried out by Mulic et al., which are a comparative analysis of reliability of the VEDE index, compared to the BEWE index [
26]. In line with the guidelines for the standardization process of research tools, these studies were preceded by the training of researchers. Their results proved that in the tests of compatibility between researchers, while using the ‘test–retest’ patterns during the evaluation of photos, higher reliability results were achieved by the VEDE index. It should be noted that the VEDE index takes into account the criterion of the degree of exposed dentine, which is considered to be of debatable reliability, due to the differentiated distribution of enamel thickness on the tooth surface [
21].
Based on the analysis of subjective written comments on the use of the VEDE index, it is clear from the operator’s point of view that the greatest drawbacks are: the difficulty in performing digital projections and mapping of the tooth surfaces in such a way that they correspond to the photo guide included in the index. The operator expressed this opinion 55% more frequently after conducting the test within the examined group than in the control group. Another issue, raised most frequently by the operator, was the large amount of specialized equipment needed for the examination (camera with a ‘macro’ lens function, expanders, a set of intraoral mirrors). It is difficult to describe this index as a simple research tool that enables a quick, routine erosion test in all conditions. It is actually necessary to have help from a dental assistant for the perfect quality of the photos taken for this index. Despite the use of indexed teeth, which aims at shortening the examination time, in our own research it seemed relatively long compared with other selected indexes. Considering the above data, the opinion expressed in the studies of Mulic et al. seems to be true, claiming that the VEDE index better serves research at the individual level than for epidemiological purposes, as it allows a further assessment of the progression of erosive changes over time [
26]. This last feature would seem particularly important during the diagnosis and planning of erosion treatment, especially in the group of patients with eating disorders. However, this index is a time-consuming, complicated procedure for preparing digital photo projections from the operator’s point of view. Moreover, it was also less often described as ‘optimal’ by patients in other indexes, receiving worse assessments in comparison with other research tools selected for this research.
The examination with the Oilo et al.’s index was statistically significantly longer in the group of patients with eating disorders, but was subjectively perceived by these patients as being ‘short’. The control group assessed it similarly. From the point of view of the operator conducting the examination, this time was perceived as ‘average’. Examinations with this index were less difficult in both groups than was the case with the VEDE index, although in the control group there were statistically significant differences in this respect. This index was among the most frequently selected among all three visits in both groups of patients. The research scheme of Oilo et al.’s index did not generally entail negative feelings of anxiety, embarrassment or discomfort. Unlike the indexes taking into account the necessity of taking impressions, after the patients got acquainted with the procedure of taking digital photos of the inside of the mouth during the VEDE test, there was not a single refusal to participate in the next examination involving taking pictures. In the operator’s opinion, the projections assigned to Oilo et al.’s index proved to be significantly simpler in preparation when compared to the previous index. Oilo et al.’s index is intended for assessing the occlusive wear, regardless of its etiology, and is based rather on the assessment of the overall contour of the tooth than on the depth of individual defects [
14,
24]. Extremely original categories created by its authors are a characteristic feature of this research tool. Unlike most indexes, these are no numerical thresholds but categories in the form of proper names or male names. This difference contributed to the opinion of the operator conducting the examination, that it was easy to memorize the main categories of the index and the evaluation criteria assigned to them, as well as the fact that the last two categories describe the wear as unacceptable, indicating the necessity to undertake therapeutic intervention.
Oilo et al.’s index uses qualitative assessment criteria such as, for example, hardness of tissues, their color or hypersensitivity [
18,
24]. However, since the maximum degree of wear in the majority of patients in both groups was SDF (small areas of exposed dentine unrelated to hypersensitivity of tissues or changes in their hardness) or even less severe: SOF (wear spots within the incisal edge of enamel and occlusal surfaces of teeth), qualifying patients to the initial wear category: Sierra, the overwhelming need to use only the first few subcategories did not pose difficulties during the examination. The designation of the concept of ‘individual level of wear’ is another innovative solution used in this index, which covers 90% of the results found in a given patient and also depends on the number of teeth preserved in the patient’s mouth [
21]. The introduction of this concept seems to be of particular importance when comparing results. The patients of both groups, examined for the purpose of this study, in their written reports commented on the increase of the comfort level in the procedures conducted according to Oilo et al.’s index, as compared to the VEDE, due to the lack of the necessity to use intraoral mirrors. When using the previous index, they were perceived as problematic by 26.6% of patients in each group. According to the operator’s own observations, the positive opinions of patients regarding the examination following Oilo et al.’s index could be influenced by the fact that it was already the last index, ending the entire series of examinations. Patients had a higher level of trust and experience in cooperation with the operator, which was reflected in their opinions. While testing according to Oilo et al.’s index, its authors preceded the research with a training and calibration of researchers and an attempt to assess its reliability, obtaining the results of compatibility between researchers at a level of 85%. They also emphasize the good level of sensitivity of this research tool, reflecting on the degree of detection of changes, as they were actually present on the examined surfaces [
13,
24].
It is widely discussed that a multidisciplinary approach to the patients is crucial [
36]. More and more patients are having eating disorders and the possibility of meeting patients suffering from this problem is higher. It seems to be very important to implement the tooth wear indexes into the medical history, which would make more dentists pay attention to the characteristic symptoms of bulimia and anorexia. As a result, dentists could be a part of an interdisciplinary group of experts who can diagnose and treat the patient due to the latest standards.





{kind=link}
{kind=link}