
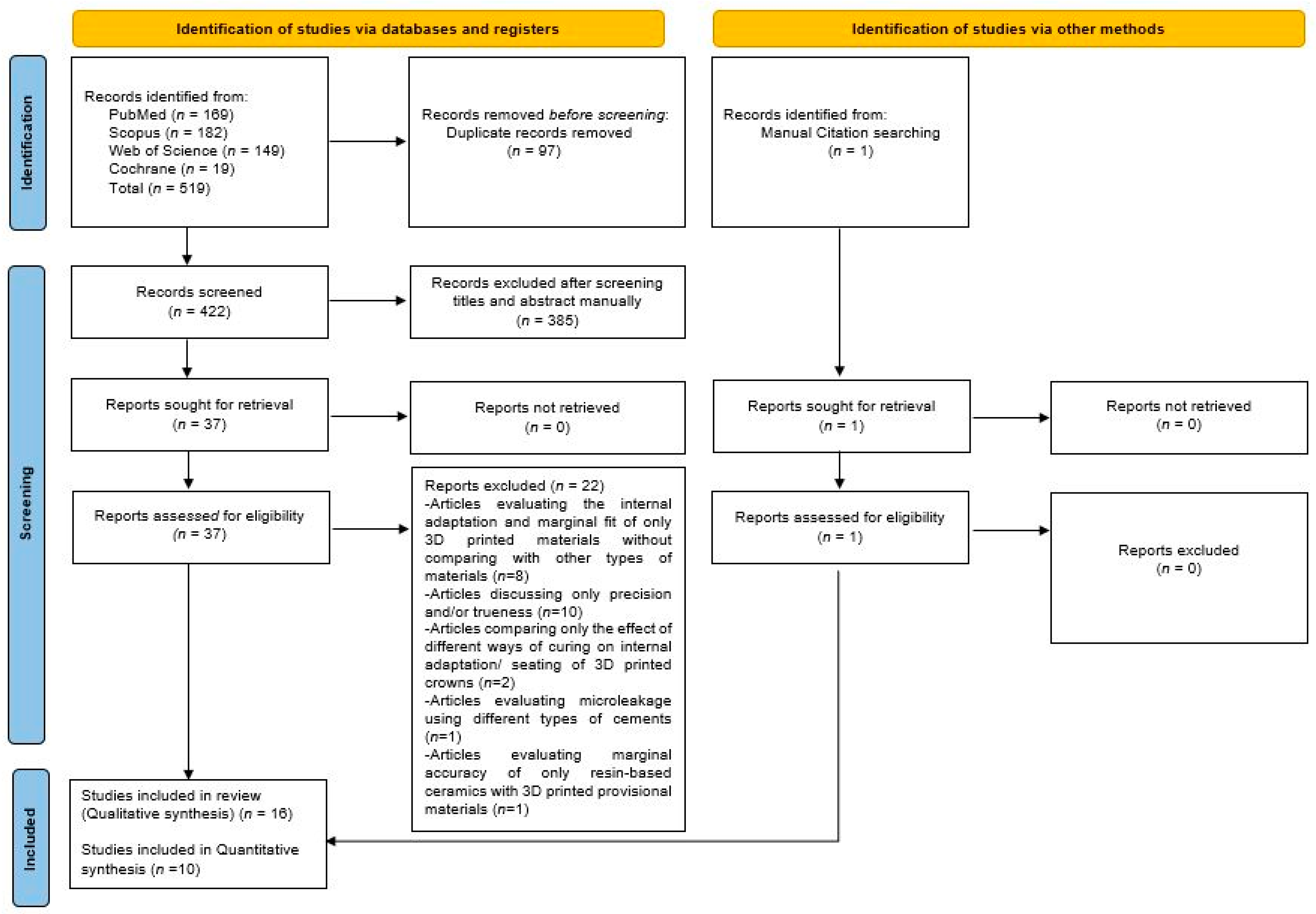
Marginal Adaptation and Internal Fit of 3D-Printed Provisional Crowns and Fixed Dental Prosthesis Resins Compared to CAD/CAM-Milled and Conventional Provisional Resins: A Systematic Review and Meta-Analysis


 , , , ,
, , , ,  , ,
, , {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
Share and Cite
Al Wadei, M.H.D.; Sayed, M.E.; Jain, S.; Aggarwal, A.; Alqarni, H.; Gupta, S.G.; Alqahtani, S.M.; Alahmari, N.M.; Alshehri, A.H.; Jain, M.; et al. Marginal Adaptation and Internal Fit of 3D-Printed Provisional Crowns and Fixed Dental Prosthesis Resins Compared to CAD/CAM-Milled and Conventional Provisional Resins: A Systematic Review and Meta-Analysis. Coatings 2022, 12, 1777. https://doi.org/10.3390/coatings12111777
Al Wadei MHD, Sayed ME, Jain S, Aggarwal A, Alqarni H, Gupta SG, Alqahtani SM, Alahmari NM, Alshehri AH, Jain M, et al. Marginal Adaptation and Internal Fit of 3D-Printed Provisional Crowns and Fixed Dental Prosthesis Resins Compared to CAD/CAM-Milled and Conventional Provisional Resins: A Systematic Review and Meta-Analysis. Coatings. 2022; 12(11):1777. https://doi.org/10.3390/coatings12111777
Chicago/Turabian StyleAl Wadei, Mohammed Hussain Dafer, Mohammed E. Sayed, Saurabh Jain, Aparna Aggarwal, Hatem Alqarni, Shilpi Gilra Gupta, Saeed M. Alqahtani, Nasser M. Alahmari, Abdullah Hasan Alshehri, Meena Jain, and et al. 2022. "Marginal Adaptation and Internal Fit of 3D-Printed Provisional Crowns and Fixed Dental Prosthesis Resins Compared to CAD/CAM-Milled and Conventional Provisional Resins: A Systematic Review and Meta-Analysis" Coatings 12, no. 11: 1777. https://doi.org/10.3390/coatings12111777
APA StyleAl Wadei, M. H. D., Sayed, M. E., Jain, S., Aggarwal, A., Alqarni, H., Gupta, S. G., Alqahtani, S. M., Alahmari, N. M., Alshehri, A. H., Jain, M., Ageeli, A. A., AlResayes, S. S., Alghamdi, S., Alnajdi, A. K., & Gharawi, M. M. (2022). Marginal Adaptation and Internal Fit of 3D-Printed Provisional Crowns and Fixed Dental Prosthesis Resins Compared to CAD/CAM-Milled and Conventional Provisional Resins: A Systematic Review and Meta-Analysis. Coatings, 12(11), 1777. https://doi.org/10.3390/coatings12111777