
Alteration of Platelet Count in Patients with Severe Non-Plasmodium falciparum Malaria: A Systematic Review and Meta-Analysis

 ,
,  and
and {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:Simple Summary
Abstract
1. Introduction
2. Methods
2.1. Study Registration
2.2. Types of Studies and Inclusion and Exclusion Criteria
2.3. Search Strategy and Data Extraction
2.4. Assessment of Risk of Bias
2.5. Data Synthesis and Analysis
3. Results
3.1. Characteristics of the Included Studies
3.2. Risk of Bias of Individual Studies
3.3. Prevalence of Severe Thrombocytopenia in Severe Non-P. falciparum Malaria
3.4. Prevalence of Profound Thrombocytopenia in Severe Non-P. falciparum Malaria
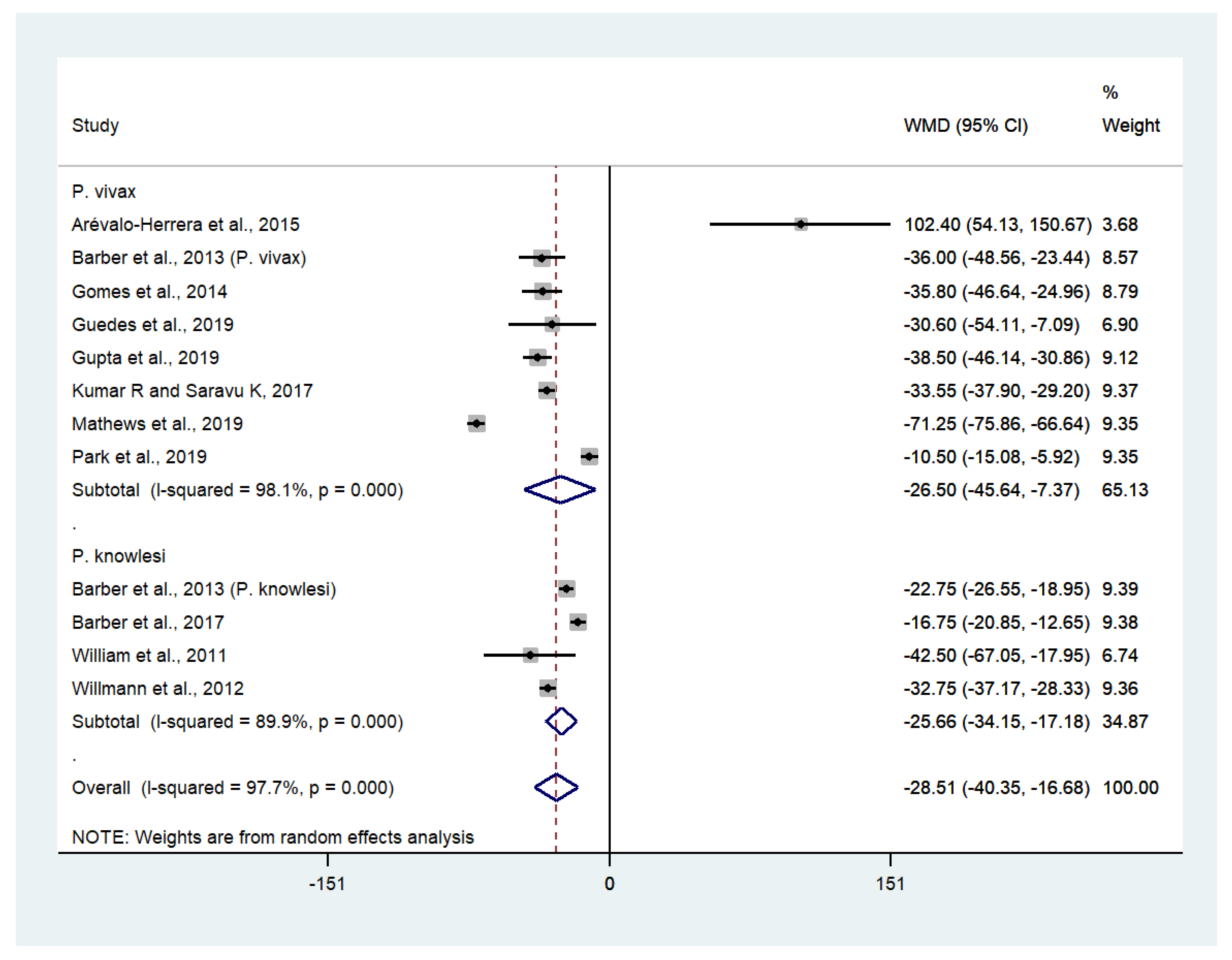
3.5. Difference in Platelet Counts between Patients with Severe and Uncomplicated Non-P. falciparum Malaria
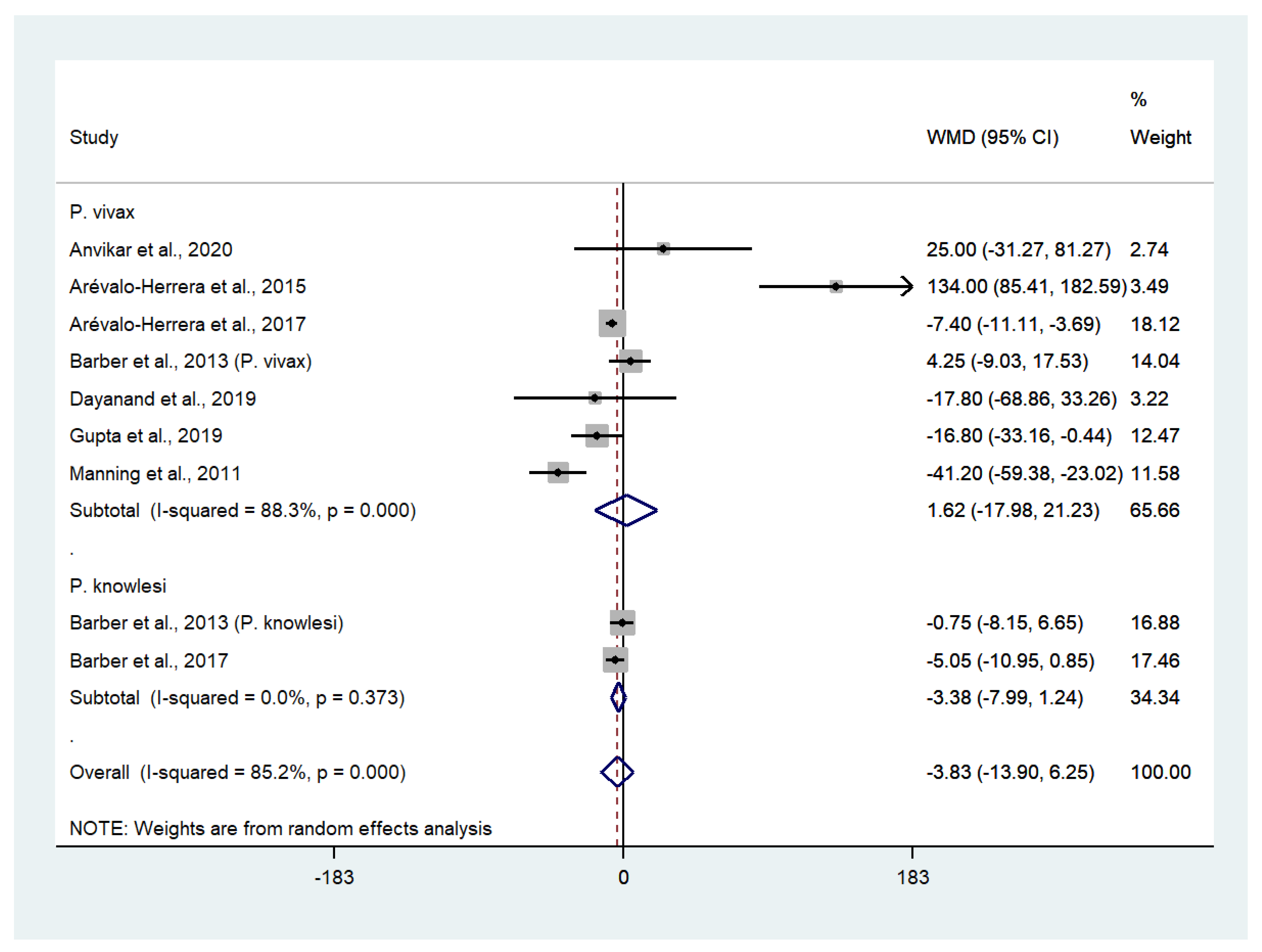
3.6. Differences in Platelet Counts between Patients with Severe Non-P. falciparum and Severe P. falciparum Malaria
3.7. Meta-Regression Analysis
3.8. Risk of Severe or Profound Thrombocytopenia in Patients with Severe Non-P. falciparum Malaria Compared with Uncomplicated Non-P. falciparum Malaria
3.9. Risk of Severe or Profound Thrombocytopenia in Patients with Severe Non-P. falciparum Malaria Compared with Severe P. falciparum Malaria
3.10. Deaths Related to Severe or Profound Thrombocytopenia
3.11. Publication Bias
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- van der Meijden, P.E.J.; Heemskerk, J.W.M. Platelet biology and functions: New concepts and clinical perspectives. Nat. Rev. Cardiol. 2019, 16, 166–179. [Google Scholar] [CrossRef]
- Das, S.; Rajkumari, N.; Chinnakali, P. A comparative study assessing the effect of haematological and biochemical parameters on the pathogenesis of malaria. J. Parasit. Dis. 2019, 43, 633–637. [Google Scholar] [CrossRef]
- Sari, N.D.; Yoruk, G. Retrospective evaluation of 31 malaria cases hospitalized in our clinic between 2012–2018. Turk. Parazitol. Derg. 2019, 43, 170–174. [Google Scholar] [CrossRef] [PubMed]
- Nwaneri, D.; Oladipo, O.; Ifebi, E.; Oviawe, O.; Asemota, O.; Ogboghodo, B.; Israel-Aina, Y.; Sadoh, A. Haematological parameters and spleen rate of asymptomatic and malaria negative children in Edo south district, Nigeria. Ann. Glob. Health 2020, 86, 62. [Google Scholar] [CrossRef]
- Kochar, D.K.; Das, A.; Kochar, A.; Middha, S.; Acharya, J.; Tanwar, G.S.; Gupta, A.; Pakalapati, D.; Garg, S.; Saxena, V.; et al. Thrombocytopenia in Plasmodium falciparum, Plasmodium vivax and mixed infection malaria: A study from Bikaner (Northwestern India). Platelets 2010, 21, 623–6277. [Google Scholar] [CrossRef]
- Leal-Santos, F.A.; Silva, S.B.; Crepaldi, N.P.; Nery, A.F.; Martin, T.O.; Alves-Junior, E.R.; Fontes, C.J. Altered platelet indices as potential markers of severe and complicated malaria caused by Plasmodium vivax: A cross-sectional descriptive study. Malar. J. 2013, 12, 462. [Google Scholar] [CrossRef] [Green Version]
- Supanaranond, W.; Davis, T.M.; Dawes, J.; Silamut, K.; Vilaiwanna, N.; White, N.J. In-vivo platelet activation and anomalous thrombospondin levels in severe falciparum malaria. Platelets 1992, 3, 195–200. [Google Scholar] [CrossRef]
- Kochar, D.K.; Das, A.; Kochar, A.; Middha, S.; Acharya, J.; Tanwar, G.S.; Gupta, A.; Pakalapati, D.; Garg, S.; Saxena, V.; et al. Platelet accumulation in brain microvessels in fatal pediatric cerebral malaria. J. Infect. Dis. 2003, 187, 461–466. [Google Scholar]
- Lacerda, M.V.; Mourao, M.P.; Coelho, H.C.; Santos, J.B. Thrombocytopenia in malaria: Who cares? Mem. Inst. Oswaldo Cruz. 2011, 106 (Suppl. 1), 52–63. [Google Scholar] [CrossRef] [Green Version]
- Tanwar, G.S.; Khatri, P.C.; Chahar, C.K.; Sengar, G.S.; Kochar, A.; Tanwar, G.; Chahar, S.; Khatri, N.; Middha, S.; Acharya, J.; et al. Thrombocytopenia in childhood malaria with special reference to P. vivax monoinfection: A study from Bikaner (Northwestern India). Platelets 2012, 23, 211–216. [Google Scholar] [CrossRef] [PubMed]
- Thapa, R.; Biswas, B.; Mallick, D.; Sardar, S.; Modak, S. Childhood Plasmodium vivax malaria with severe thrombocytopenia and bleeding manifestations. J. Pediatr. Hematol. Oncol. 2009, 31, 758–759. [Google Scholar] [CrossRef]
- Punyagupta, S.; Srichaikul, T.; Nitiyanant, P.; Petchclai, B. Acute pulmonary insufficiency in falciparum malaria: Summary of 12 cases with evidence of disseminated intravascular coagulation. Am. J. Trop. Med. Hyg. 1974, 23, 551–559. [Google Scholar] [CrossRef]
- WHO. Guidelines for the Treatment of Malaria 2015. Available online: https://www.who.int/docs/default-source/documents/publications/gmp/guidelines-for-the-treatment-of-malaria-eng.pdf?sfvrsn=a0138b77_2 (accessed on 25 July 2020).
- Hanson, J.; Phu, N.H.; Hasan, M.U.; Charunwatthana, P.; Plewes, K.; Maude, R.J.; Prapansilp, P.; Kingston, H.W.; Mishra, S.K.; Mohanty, S.; et al. The clinical implications of thrombocytopenia in adults with severe falciparum malaria: A retrospective analysis. BMC Med. 2015, 13, 97. [Google Scholar] [CrossRef] [Green Version]
- Naing, C.; Whittaker, M.A. Severe thrombocytopaenia in patients with vivax malaria compared to falciparum malaria: A systematic review and meta-analysis. Infect. Dis. Poverty 2018, 7, 10. [Google Scholar] [CrossRef] [Green Version]
- Wells, G.A.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses 2019. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 25 July 2020).
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control. Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Kotepui, M.; Kotepui, K.U.; De Jesus Milanez, G.; Masangkay, F.R. Plasmodium spp. mixed infection leading to severe malaria: A systematic review and meta-analysis. Sci. Rep. 2020, 10, 11068. [Google Scholar] [CrossRef]
- Kotepui, M.; Kotepui, K.U.; Milanez, G.D.; Masangkay, F.R. Severity and mortality of severe Plasmodium ovale infection: A systematic review and meta-analysis. PLoS ONE 2020, 15, e0235014. [Google Scholar] [CrossRef]
- Kotepui, M.; Kotepui, K.U.; Milanez, G.D.; Masangkay, F.R. Prevalence of severe Plasmodium knowlesi infection and risk factors related to severe complications compared with non-severe P. knowlesi and severe P. falciparum malaria: A systematic review and meta-analysis. Infect. Dis. Poverty 2020, 9, 106. [Google Scholar] [CrossRef]
- Kotepui, M.; Kotepui, K.U.; Milanez, G.J.; Masangkay, F.R. Prevalence and risk factors related to poor outcome of patients with severe Plasmodium vivax infection: A systematic review, meta-analysis, and analysis of case reports. BMC Infect. Dis. 2020, 20, 363. [Google Scholar] [CrossRef]
- Kotepui, M.K.K.; Milanez, G.D.; Masangkay, F.R. Global prevalence and mortality of severe Plasmodium malariae infection: A systematic review and meta-analysis. Malar. J. 2020, 10, 11068. [Google Scholar] [CrossRef]
- Ahmad, S.; Shirazi, N.; Bhat, N.K.; Dhar, M.; Mittal, G.; Mittal, M.; Kaeley, N.; Kumar, M. A hospital-based retrospective comparative study of complications, outcomes, clinical and laboratory parameters of malaria with and without neurological involvement. Mediterr. J. Hematol. Infect. Dis. 2017, 9, e2017006. [Google Scholar] [CrossRef] [Green Version]
- Alexandre, M.A.; Ferreira, C.O.; Siqueira, A.M.; Magalhães, B.L.; Mourão, M.P.G.; Lacerda, M.V.; Alecrim, M.D.G.C. Severe Plasmodium vivax malaria, Brazilian Amazon. Emerg. Infect. Dis. 2010, 16, 1611–1614. [Google Scholar] [CrossRef]
- Anvikar, A.R.; van Eijk, A.M.; Shah, A.; Upadhyay, K.J.; Sullivan, S.A.; Patel, A.J.; Joshi, J.M.; Tyagi, S.; Singh, R.; Carlton, J.M.; et al. Clinical and epidemiological characterization of severe Plasmodium vivax malaria in Gujarat, India. Virulence 2020, 11, 730–738. [Google Scholar] [CrossRef]
- Arboleda, M.; Perez, M.F.; Fernandez, D.; Usuga, L.Y.; Meza, M. Clinical and laboratory profile of Plasmodium vivax malaria patients hospitalized in Apartado, Colombia. Biomedica 2012, 32 (Suppl. 1), 58–67. [Google Scholar] [CrossRef] [Green Version]
- Arevalo-Herrera, M.; Lopez-Perez, M.; Medina, L.; Moreno, A.; Gutierrez, J.B.; Herrera, S. Clinical profile of Plasmodium falciparum and Plasmodium vivax infections in low and unstable malaria transmission settings of Colombia. Malar. J. 2015, 14, 154. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arévalo-Herrera, M.; Rengifo, L.; Lopez-Perez, M.; Arce-Plata, M.I.; García, J.; Herrera, S. Complicated malaria in children and adults from three settings of the Colombian Pacific Coast: A prospective study. PLoS ONE 2017, 12, e0185435. [Google Scholar] [CrossRef] [Green Version]
- Barber, B.E.; William, T.; Grigg, M.J.; Parameswaran, U.; Piera, K.A.; Price, R.N.; Yeo, T.W.; Anstey, N.M. Effects of aging on parasite biomass, inflammation, endothelial activation, microvascular dysfunction and disease severity in Plasmodium knowlesi and Plasmodium falciparum malaria. J. Infect. Dis. 2017, 215, 1908–1917. [Google Scholar] [CrossRef] [Green Version]
- Barber, B.E.; William, T.; Grigg, M.J.; Menon, J.; Auburn, S.; Marfurt, J.; Anstey, N.M.; Yeo, T.W. A prospective comparative study of knowlesi, falciparum, and vivax malaria in Sabah, Malaysia: High proportion with severe disease from Plasmodium knowlesi and Plasmodium vivax but no mortality with early referral and artesunate therapy. Clin. Infect. Dis. 2013, 56, 383–397. [Google Scholar] [CrossRef]
- Dayanand, K.K.; Kishore, P.; Chandrashekar, V.; Achur, R.N.; Ghosh, S.K.; Kakkilaya, S.B.; Kumari, S.N.; Tiwari, S.; Boloor, A.; Devi, R.; et al. Malaria severity in Mangaluru city in the southwestern coastal region of India. Am. J. Trop. Med. Hyg. 2019, 100, 275–279. [Google Scholar] [CrossRef] [Green Version]
- Douglas, N.M.; Pontororing, G.J.; Lampah, D.A.; Yeo, T.W.; Kenangalem, E.; Poespoprodjo, J.R.; Ralph, A.P.; Bangs, M.J.; Sugiarto, P.; Anstey, N.M.; et al. Mortality attributable to Plasmodium vivax malaria: A clinical audit from Papua, Indonesia. BMC Med. 2014, 12, 217. [Google Scholar] [CrossRef]
- Gomes, L.T.; Alves-Junior, E.R.; Rodrigues-Jesus, C.; Nery, A.F.; Gasquez-Martin, T.O.; Fontes, C.J. Angiopoietin-2 and angiopoietin-2/angiopoietin-1 ratio as indicators of potential severity of Plasmodium vivax malaria in patients with thrombocytopenia. PLoS ONE 2014, 9, e109246. [Google Scholar]
- Guedes, K.S.; Sanchez, B.A.M.; Gomes, L.T.; Fontes, C.J.F. Aspartate aminotransferase-to-platelet ratio index (APRI): A potential marker for diagnosis in patients at risk of severe malaria caused by Plasmodium vivax. PLoS ONE 2019, 14, e0224877. [Google Scholar] [CrossRef]
- Gupta, P.; Guddattu, V.; Saravu, K. Characterization of platelet count and platelet indices and their potential role to predict severity in malaria. Pathog. Glob. Health 2019, 113, 86–93. [Google Scholar] [CrossRef]
- Gupta, P.; Sharma, R.; Chandra, J.; Kumar, V.; Singh, R.; Pande, V.; Singh, V. Clinical manifestations and molecular mechanisms in the changing paradigm of vivax malaria in India. Infect. Genet. Evol. 2016, 39, 317–324. [Google Scholar] [CrossRef] [PubMed]
- Jain, V.; Agrawal, A.; Singh, N. Malaria in a tertiary health care facility of Central India with special reference to severe vivax: Implications for malaria control. Pathog. Glob. Health 2013, 107, 299–304. [Google Scholar] [CrossRef] [Green Version]
- Kumar, R.; Saravu, K. Severe vivax malaria: A prospective exploration at a tertiary healthcare centre in Southwestern India. Pathog. Glob. Health 2017, 111, 148–160. [Google Scholar] [CrossRef]
- Kumari, M.; Ghildiyal, R. Clinical profile of Plasmodium vivax malaria in children and study of severity parameters in relation to mortality: A tertiary care centre perspective in Mumbai, India. Malar. Res. Treat. 2014, 2014, 765657. [Google Scholar] [CrossRef] [Green Version]
- Kute, V.B.; Trivedi, H.L.; Vanikar, A.V.; Shah, P.R.; Gumber, M.R.; Patel, H.V.; Goswami, J.G.; Kanodia, K.V. Plasmodium vivax malaria-associated acute kidney injury, India, 2010–2011. Emerg. Infect. Dis. 2012, 18, 842–845. [Google Scholar] [CrossRef]
- Lança, E.F.C.; Magalhães, B.M.L.; Vitor-Silva, S.; Siqueira, A.M.; Benzecry, S.G.; Alexandre, M.A.A.; O’Brien, C.; Bassat, Q.; Lacerda, M.V.G. Risk factors and characterization of Plasmodium vivax-associated admissions to pediatric intensive care units in the Brazilian Amazon. PLoS ONE 2012, 7, e35406. [Google Scholar] [CrossRef]
- Manning, L.; Laman, M.; Law, I.; Bona, C.; Aipit, S.; Teine, D.; Warrell, J.; Rosanas-Urgell, A.; Lin, E.; Kiniboro, B.; et al. Features and prognosis of severe malaria caused by Plasmodium falciparum, plasmodium vivax and mixed plasmodium species in Papua New Guinean children. PLoS ONE 2011, 6, e29203. [Google Scholar] [CrossRef] [Green Version]
- Mathews, S.E.; Bhagwati, M.M.; Agnihotri, V. Clinical spectrum of Plasmodium vivax infection, from benign to severe malaria: A tertiary care prospective study in adults from Delhi, India. Trop. Parasitol. 2019, 9, 88–92. [Google Scholar] [CrossRef]
- O’Brien, A.T.; Ramirez, J.F.; Martinez, S.P. A descriptive study of 16 severe Plasmodium vivax cases from three municipalities of Colombia between 2009 and 2013. Malar. J. 2014, 13, 404. [Google Scholar] [CrossRef] [Green Version]
- Park, S.Y.; Park, Y.S.; Park, Y.; Kwak, Y.G.; Song, J.E.; Lee, K.S.; Cho, S.H.; Lee, S.E.; Shin, H.I.; Yeom, J.S. Severe vivax malaria in the Republic of Korea during the period 2000 to 2016. Travel Med. Infect. Dis. 2019, 30, 108–113. [Google Scholar] [CrossRef]
- Punnath, K.; Dayanand, K.K.; Chandrashekar, V.N.; Achur, R.N.; Kakkilaya, S.B.; Ghosh, S.K.; Mukhi, B.; Midya, V.; Kumari, S.N.; Gowda, D.C. Clinical features and haematological parameters among malaria patients in Mangaluru city area in the southwestern coastal region of India. Parasitol. Res. 2020, 119, 1043–1056. [Google Scholar] [CrossRef]
- Rajeshwar, K.K.B. Clinical profile of severe Plasmodium vivax malaria in a tertiary centre in J.J.M. Medical College, Davangere. Indian J. Basic Appl. Med. Res. 2015, 4, 133–139. [Google Scholar]
- Raposo, C.C.; Santos, J.B.; Santos, G.M.; Goncalves Eda, G.; Silva, A.R. Plasmodium vivax malaria: Related factors to severity in the State of Maranhao, Brazil. Rev. Da Soc. Bras. De Med. Trop. 2013, 46, 67–72. [Google Scholar] [CrossRef] [Green Version]
- Sharma, R.; Gohain, S.; Chandra, J.; Kumar, V.; Chopra, A.; Chatterjee, S.; Aneja, S.; Kumar Dutta, A. Plasmodium vivax malaria admissions and risk of mortality in a tertiary-care children’s hospital in North India. Paediatr. Int. Child Health 2012, 32, 152–157. [Google Scholar] [CrossRef]
- Singh, H.; Parakh, A.; Basu, S.; Rath, B. Plasmodium vivax malaria: Is it actually benign? J. Infect. Public Health 2011, 4, 91–95. [Google Scholar] [CrossRef] [Green Version]
- Sud, R.; Singh, H.; Aggarwal, A.; Bhatnagar, M.K. Resurgence of complicated malaria associated with severe thrombocytopenia in a tertiary care hospital in Delhi. J. Assoc. Physicians India 2012, 60, 68. [Google Scholar]
- Val, F.; Avalos, S.; Gomes, A.A.; Zerpa, J.E.A.; Fontecha, G.; Siqueira, A.M.; Bassat, Q.; Alecrim, M.G.C.; Monteiro, W.M.; Lacerda, M.V.G. Are respiratory complications of Plasmodium vivax malaria an underestimated problem? Malar. J. 2017, 16, 495. [Google Scholar] [CrossRef] [Green Version]
- William, T.; Menon, J.; Rajahram, G.; Chan, L.; Ma, G.; Donaldson, S.; Khoo, S.; Fredrick, C.; Jelip, J.; Anstey, N.M.; et al. Severe Plasmodium knowlesi malaria in a tertiary care hospital, Sabah, Malaysia. Emerg. Infect. Dis. 2011, 17, 1248–1255. [Google Scholar] [CrossRef]
- Willmann, M.; Ahmed, A.; Siner, A.; Wong, T.; Woon, L.C.; Singh, B.; Krishna, S.; Cox-Singh, J. Laboratory markers of disease severity in Plasmodium knowlesi infection: A case control study. Malar. J. 2012, 11, 363. [Google Scholar] [CrossRef] [Green Version]
- Kotepui, M.; Phunphuech, B.; Phiwklam, N.; Chupeerach, C.; Duangmano, S. Effect of malarial infection on haematological parameters in population near Thailand-Myanmar border. Malar. J. 2014, 13, 218. [Google Scholar] [CrossRef] [Green Version]
- Erhart, L.M.; Yingyuen, K.; Chuanak, N.; Buathong, N.; Laoboonchai, A.; Miller, R.S.; Meshnick, S.R.; Gasser, R.A.; Wongsrichanalai, C. Hematologic and clinical indices of malaria in a semi-immune population of western Thailand. Am. J. Trop. Med. Hyg. 2004, 70, 8–14. [Google Scholar] [CrossRef]
- Lampah, D.A.; Yeo, T.W.; Malloy, M.; Kenangalem, E.; Douglas, N.M.; Ronaldo, D.; Sugiarto, P.; Simpson, J.A.; Poespoprodjo, J.R.; Anstey, N.M.; et al. Severe malarial thrombocytopenia: A risk factor for mortality in Papua, Indonesia. J. Infect. Dis. 2015, 211, 623–634. [Google Scholar] [CrossRef] [Green Version]
- Gerardin, P.; Rogier, C.; Ka, A.S.; Jouvencel, P.; Brousse, V.; Imbert, P. Prognostic value of thrombocytopenia in African children with falciparum malaria. Am. J. Trop. Med. Hyg. 2002, 66, 686–691. [Google Scholar] [CrossRef] [Green Version]
- Pain, A.; Ferguson, D.J.; Kai, O.; Urban, B.C.; Lowe, B.; Marsh, K.; Roberts, D.J. Platelet-mediated clumping of Plasmodium falciparum-infected erythrocytes is a common adhesive phenotype and is associated with severe malaria. Proc. Natl. Acad. Sci. USA 2001, 98, 1805–1810. [Google Scholar] [CrossRef] [Green Version]
- WHO. Severe malaria. Trop. Med. Int. Health 2014, 19, 7–131. [Google Scholar] [CrossRef]
- Kotepui, M.; Piwkham, D.; PhunPhuech, B.; Phiwklam, N.; Chupeerach, C.; Duangmano, S. Effects of malaria parasite density on blood cell parameters. PLoS ONE 2015, 10, e0121057. [Google Scholar] [CrossRef]
- Tagny, C.T.; Mbanya, D.; Tapko, J.B.; Lefrere, J.J. Blood safety in Sub-Saharan Africa: A multi-factorial problem. Transfusion 2008, 48, 1256–1261. [Google Scholar] [CrossRef]
- Looareesuwan, S.; Davis, J.G.; Allen, D.L.; Lee, S.H.; Bunnag, D.; White, N.J. Thrombocytopenia in malaria. Southeast Asian J. Trop. Med. Public Health 1992, 23, 44–50. [Google Scholar] [PubMed]
- Bottieau, E.; Clerinx, J.; Van Den Enden, E.; Van Esbroeck, M.; Colebunders, R.; Van Gompel, A.; Van Den Ende, J. Imported non-Plasmodium falciparum malaria: A five-year prospective study in a European referral center. Am. J. Trop. Med. Hyg. 2006, 75, 133–138. [Google Scholar] [CrossRef] [PubMed]
- Langford, S.; Douglas, N.M.; Lampah, D.A.; Simpson, J.A.; Kenangalem, E.; Sugiarto, P.; Anstey, N.M.; Poespoprodjo, J.R.; Price, R.N. Plasmodium malariae Infection Associated with a High Burden of Anemia: A hospital-based surveillance study. PLoS Negl. Trop. Dis. 2015, 9, e0004195. [Google Scholar] [CrossRef]
- Rojo-Marcos, G.; Rubio-Muñoz, J.M.; Ramírez-Olivencia, G.; García-Bujalance, S.; Elcuaz-Romano, R.; Díaz-Menéndez, M.; Calderón, M.; García-Bermejo, I.; Ruiz-Giardín, J.M.; Merino-Fernández, F.J.; et al. Comparison of imported Plasmodium ovale curtisi and P. ovale wallikeri infections among patients in Spain, 2005–2011. Emerg. Infect. Dis. 2014, 20, 409–416. [Google Scholar] [CrossRef] [PubMed]
- Turner, G.D.; Morrison, H.; Jones, M.; Davis, T.M.; Looareesuwan, S.; Buley, I.D.; Gatter, K.C.; Newbold, C.I.; Pukritayakamee, S.; Nagachinta, B.; et al. An immunohistochemical study of the pathology of fatal malaria. Evidence for widespread endothelial activation and a potential role for intercellular adhesion molecule-1 in cerebral sequestration. Am. J. Pathol. 1994, 145, 1057–1069. [Google Scholar]
- Sadler, J.E. Biochemistry and genetics of von Willebrand factor. Ann. Rev. Biochem. 1998, 67, 395–424. [Google Scholar] [CrossRef] [PubMed]
- Löwenberg, E.C.; Charunwatthana, P.; Cohen, S.; van den Born, B.J.; Meijers, J.C.; Yunus, E.B.; Hassan, M.B.; Hoque, G.; Maude, R.J.; Nuchsongsin, F.; et al. Severe malaria is associated with a deficiency of von Willebrand factor cleaving protease, ADAMTS13. Thromb. Haemost. 2010, 103, 181–187. [Google Scholar] [CrossRef] [PubMed]
- Morrell, C.N.; Aggrey, A.A.; Chapman, L.M.; Modjeski, K.L. Emerging roles for platelets as immune and inflammatory cells. Blood 2014, 123, 2759–2767. [Google Scholar] [CrossRef] [Green Version]
- Boutlis, C.S.; Yeo, T.W.; Anstey, N.M. Malaria tolerance--for whom the cell tolls? Trends Parasitol. 2006, 22, 371–377. [Google Scholar] [CrossRef] [Green Version]
- Yeo, T.W.; Lampah, D.A.; Gitawati, R.; Tjitra, E.; Kenangalem, E.; McNeil, Y.R.; Darcy, C.J.; Granger, D.L.; Weinberg, J.B.; Lopansri, B.K.; et al. Impaired nitric oxide bioavailability and L-arginine reversible endothelial dysfunction in adults with falciparum malaria. J. Exp. Med. 2007, 204, 2693–2704. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kong, T.F.; Ye, W.; Peng, W.K.; Hou, H.W.; Preiser, P.R.; Nguyen, N.T.; Han, J. Enhancing malaria diagnosis through microfluidic cell enrichment and magnetic resonance relaxometry detection. Sci. Rep. 2015, 5, 11425. [Google Scholar] [CrossRef] [Green Version]
- Di Gregorio, E.; Ferrauto, G.; Schwarzer, E.; Gianolio, E.; Valente, E.; Ulliers, D.; Aime, S.; Skorokhod, O. Relaxometric studies of erythrocyte suspensions infected by Plasmodium falciparum: A tool for staging infection and testing anti-malarial drugs. Magn. Reson. Med. 2020, 84, 3366–3378. [Google Scholar] [CrossRef]
- Peng, W.K.; Kong, T.F.; Ng, C.S.; Chen, L.; Huang, Y.; Bhagat, A.A.S.; Nguyen, N.T.; Preiser, P.R.; Han, J. Micromagnetic resonance relaxometry for rapid label-free malaria diagnosis. Nat. Med. 2014, 20, 1069–1073. [Google Scholar] [CrossRef]
- Gupta, M.; Singh, K.; Lobiyal, D.K.; Safvan, C.P.; Sahu, B.K.; Yadav, P.; Singh, S. A sensitive on-chip probe–based portable nuclear magnetic resonance for detecting low parasitaemia Plasmodium falciparum in human blood. Devices Sens. 2020, 3, e10098. [Google Scholar] [CrossRef]
- Arndt, L.; Koleala, T.; Orbán, Á.; Ibam, C.; Lufele, E.; Timinao, L.; Lorry, L.; Butykai, Á.; Kaman, P.; Molnár, A.P.; et al. Magneto-optical diagnosis of symptomatic malaria in Papua New Guinea. Nat. Commun. 2021, 12, 969. [Google Scholar] [CrossRef]
- Yamamoto, T.; Hashimoto, M.; Nagatomi, K.; Nogami, T.; Sofue, Y.; Hayashi, T.; Ido, Y.; Yatsushiro, S.; Abe, K.; Kajimoto, K. Field Evaluation of a Quantitative, and Rapid Malaria Diagnostic System Using a Fluorescent Blue-Ray Optical Device. 2019. Available online: https://www.biorxiv.org/content/10.1101/721076v1 (accessed on 23 October 2021).







Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mahittikorn, A.; Masangkay, F.R.; Kotepui, K.U.; Mala, W.; Milanez, G.D.J.; Wilairatana, P.; Kotepui, M. Alteration of Platelet Count in Patients with Severe Non-Plasmodium falciparum Malaria: A Systematic Review and Meta-Analysis. Biology 2021, 10, 1275. https://doi.org/10.3390/biology10121275
Mahittikorn A, Masangkay FR, Kotepui KU, Mala W, Milanez GDJ, Wilairatana P, Kotepui M. Alteration of Platelet Count in Patients with Severe Non-Plasmodium falciparum Malaria: A Systematic Review and Meta-Analysis. Biology. 2021; 10(12):1275. https://doi.org/10.3390/biology10121275
Chicago/Turabian StyleMahittikorn, Aongart, Frederick Ramirez Masangkay, Kwuntida Uthaisar Kotepui, Wanida Mala, Giovanni De Jesus Milanez, Polrat Wilairatana, and Manas Kotepui. 2021. "Alteration of Platelet Count in Patients with Severe Non-Plasmodium falciparum Malaria: A Systematic Review and Meta-Analysis" Biology 10, no. 12: 1275. https://doi.org/10.3390/biology10121275
APA StyleMahittikorn, A., Masangkay, F. R., Kotepui, K. U., Mala, W., Milanez, G. D. J., Wilairatana, P., & Kotepui, M. (2021). Alteration of Platelet Count in Patients with Severe Non-Plasmodium falciparum Malaria: A Systematic Review and Meta-Analysis. Biology, 10(12), 1275. https://doi.org/10.3390/biology10121275