


Iodine Intake and Related Cognitive Function Impairments in Elementary Schoolchildren

 , , ,
, , ,  and
and 
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
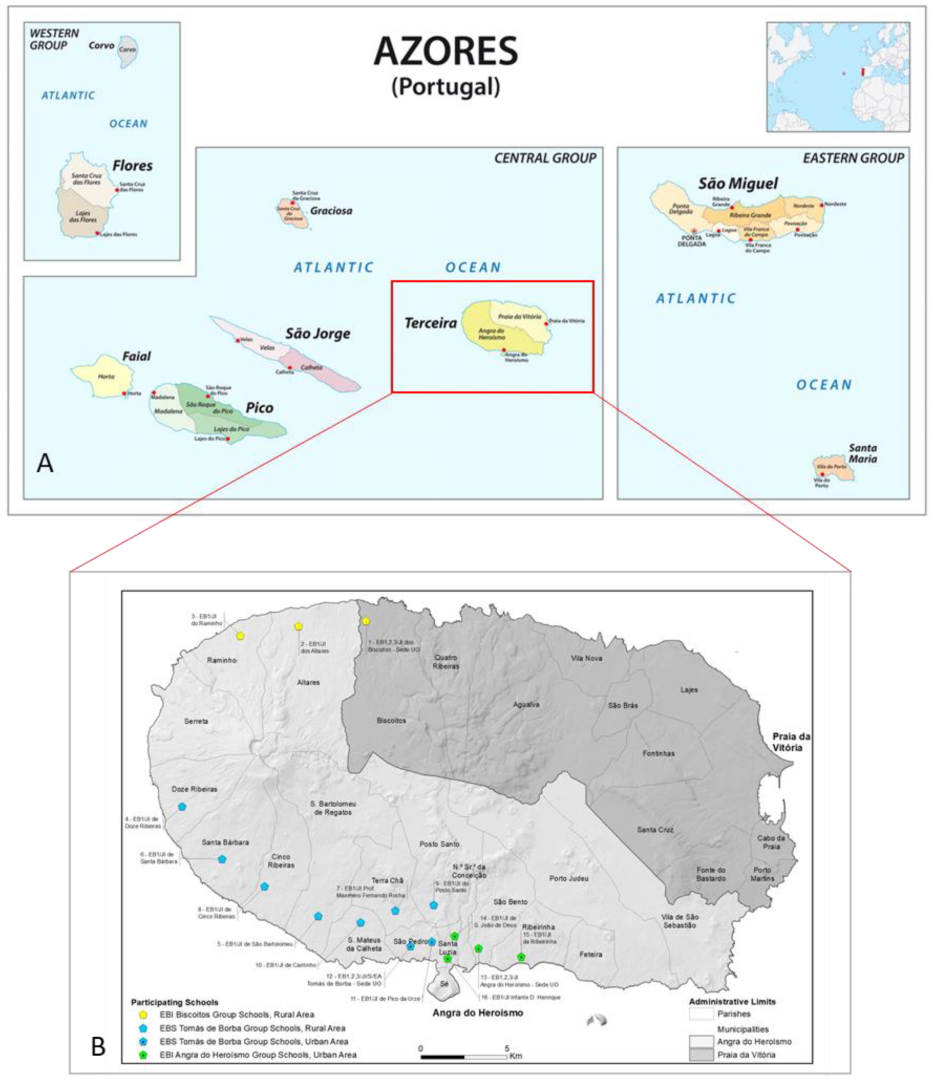
2.1. Study Area
2.2. Study Population and Assessment of Iodine Intake
2.3. Urinary Iodine Concentration Assessment
2.4. Cognitive Function Assessment
2.4.1. Raven´s Colored Progressive Matrices (CPM)—Sets A, AB, B
2.4.2. Wechsler Intelligence Scale for Children—3rd Edition (WISC-III)
2.5. Statistical Analyses
3. Results
3.1. Characteristics of the Study Population and Study Subgroups
3.2. Urinary Iodine Concentration (UIC)
3.3. Cognitive Function Assessment
3.3.1. Raven´s Colored Progressives Matrices (CPM)—A, AB, B
3.3.2. Wechsler Intelligence Scale for Children—3rd Edition (WISC-III)
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Andersson, M.; Karumbunathan, V.; Zimmermann, M.B. Global Iodine Status in 2011 and Trends over the Past Decade. J. Nutr. 2012, 142, 744–750. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Biban, B.G.; Lichiardopol, C. Iodine Deficiency, Still a Global Problem? Curr. Health Sci. J. 2017, 43, 103–111. [Google Scholar]
- Alloway, B.; Centeno, J.; Finkelman, R.; Fuge, R.; Lindh, U.; Smedley, P. Essentials of Medical Geology: Revised Edition; Selinus, O., Ed.; Springer Science & Business Media: Berlin/Heidelberg, Germany, 2013. [Google Scholar]
- Eastman, C.J.; Zimmermann, M.B. The Iodine Deficiency Disorders.; [Updated 6 February 2018]; Feingold, K.R., Anawalt, B., Boyce, A., Eds.; MDText.com, Inc.: South Dartmouth, MA, USA, 2000; PMID: 25905411. [Google Scholar]
- Laurberg, P.; Cerqueira, C.; Ovesen, L.; Rasmussen, L.B.; Perrild, H.; Andersen, S.; Carlé, A. Iodine intake as a determinant of thyroid disorders in populations. Best Pract. Res. Clin. Endocrinol. Metab. 2010, 24, 13–27. [Google Scholar] [CrossRef] [PubMed]
- Moog, N.K.; Entringer, C.; Heim, P.D.; Wadhwa, N.; Kathmann, N. Influence of maternal thyroid hormones during gestation on fetal brain development. Neuroscience 2017, 342, 68–100. [Google Scholar] [CrossRef] [Green Version]
- Caron, P. Neurocognitive outcomes of children secondary to mild iodine deficiency in pregnant women. Ann. Endocrinol. 2015, 76, 248–252. [Google Scholar] [CrossRef]
- Toloza, F.J.K.; Motahari, H.; Maraka, S. Consequences of Severe Iodine Deficiency in Pregnancy: Evidence in Humans. Front. Endocrinol. 2020, 11, 409. [Google Scholar] [CrossRef]
- Andersson, M.; De Benoist, B.; Rogers, L. Epidemiology of iodine deficiency: Salt iodisation and iodine status. Best Pract. Res. Clin. Endocrinol. Metab. 2010, 24, 1–11. [Google Scholar] [CrossRef]
- Zimmermann, M.B. Symposium on ‘Geographical and geological influences on nutrition’ Iodine deficiency in industrialised countries. Proc. Nutr. Soc. 2010, 69, 133–143. [Google Scholar] [CrossRef] [Green Version]
- Bleichrodt, N.; Born, M.P. A meta-analysis of research on iodine and its relationship to cognitive development. In The Damaged Brain of Iodine Deficiency; Cognizant Communication: New York, NY, USA, 1994; pp. 195–200. [Google Scholar]
- Bougma, K.; Aboud, F.E.; Harding, K.B.; Marquis, G.S. Iodine and mental development of children 5 years old and under: A systematic review and meta-analysis. Nutrients 2013, 5, 1384–1416. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zimmermann, M.B.; Connolly, K.; Bozo, M.; Bridson, J.; Rohner, F.; Grimci, L. Iodine supplementation improves cognition in iodine-deficient schoolchildren in Albania: A randomized, controlled, double-blind study. Am. J. Clin. Nutr. 2006, 83, 108–114. [Google Scholar] [CrossRef] [Green Version]
- Gordon, R.C.; Rose, M.C.; Skeaff, S.A.; Gray, A.R.; Morgan, K.M.; Ruffman, T. Iodine supplementation improves cognition in mildly iodine-deficient children. Am. J. Clin. Nutr. 2009, 90, 1264–1271. [Google Scholar] [CrossRef] [Green Version]
- Bath, S.C.; Steer, C.D.; Golding, J.; Emmett, P.; Rayman, M.P. Effect of inadequate iodine status in UK pregnant women on cognitive outcomes in their children: Results from the Avon Longitudinal Study of Parents and Children (ALSPAC). Lancet 2013, 382, 331–337. [Google Scholar] [CrossRef]
- Huda, S.N.; Grantham-McGregor, S.M.; Tomkins, A. Cognitive and motor functions of iodine-deficient but euthyroid children in Bangladesh do not benefit from iodized poppy seed oil (Lipiodol). J. Nutr. 2001, 131, 72–77. [Google Scholar] [CrossRef] [Green Version]
- Simões, M.; Rocha, A.M.; Ferreira, C. WISC-III, Escala de Inteligência de Wechsler para Crianças-3ª edição; Cegoc-TEA: Lisboa, Portugal, 2003. [Google Scholar]
- Simões, M.R. Investigações no Âmbito da Aferição Nacional do Teste das Matrizes Progressivas Coloridas de Raven (M.P.C.R.). Dissertação de Doutoramento em Psicologia, especialização em Avaliação Psicológica, apresentada à Faculdade de Psicologia e de Ciências da Educação da Universidade de Coimbra, Coimbra, Portugal, 1994. [Google Scholar]
- Simões, M.R. Investigações no Âmbito da Aferição Nacional do Teste das Matrizes Progressivas Coloridas de Raven (M.P.C.R.); Fundação Calouste Gulbenkian: Lisboa, Portugal, 2000. [Google Scholar]
- Benyamin, B.; Pourcain, B.; Davis, O.S.; Davies, G.; Hansell, N.K.; Brion, M.-J.; Kirkpatrick, R.M.; Cents, R.A.M.; Franić, S.; Miller, M.B.; et al. Childhood intelligence is heritable, highly polygenic and associated with FNBP1L. Mol. Psychiatry 2014, 19, 253–258. [Google Scholar] [CrossRef] [Green Version]
- Rinaldi, L.; Karmiloff-Smith, A. Intelligence as a Developing Function: A Neuroconstructivist Approach. J. Intell. 2017, 5, 18. [Google Scholar] [CrossRef] [Green Version]
- Limbert, E.; Prazeres, S.; Pedro, M.S.; Madureira, D.; Miranda, A.; Ribeiro, M.; Carrilho, F.; Jácome de Castro, J.; Santana Lopes, M.; Cardoso, J.; et al. Aporte do Iodo nas Crianças das Escolas em Portugal. Acta Med. Port. 2012, 25, 29–36. [Google Scholar]
- Combet, E.; Lean, M.E. Validation of a short food frequency questionnaire specific for iodine in UK females of childbearing age. J. Hum. Nutr. Diet. 2014, 27, 599–605. [Google Scholar] [CrossRef] [Green Version]
- Tan, L.M.; Charlton, K.E.; Tan, S.Y.; Ma, G.; Batterham, M. Validity and reproducibility of an iodine-specific food frequency questionnaire to estimate dietary iodine intake in older Australians. Nutr. Diet. 2013, 70, 71–78. [Google Scholar] [CrossRef]
- Rasmussen, L.B.; Ovesen, L.; Bulow, I.; Jorgensen, T.; Knudsen, N.; Laurberg, P.; Perrild, H. Evaluation of a semi-quantitative food frequency questionnaire to estimate iodine intake. Eur. J. Clin. Nutr. 2001, 55, 287–292. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gnat, D.; Dunn, A.D.; Chaker, S.; Delange, F.; Vertongen, F.; Dunn, J.T. Fast colorimetric method for measuring urinary iodine. Clin. Chem. 2003, 49, 186–188. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO. Urinary Iodine Concentrations for Determining Iodine Status Deficiency in Populations. Vitamin and Mineral Nutrition Information System; World Health Organization: Geneva, Switzerland, 2013. Available online: https://www.who.int/publications/i/item/WHO-NMH-NHD-EPG-13.1 (accessed on 11 July 2021).
- Raven, J. The Raven’s progressive matrices: Change and stability over culture and time. Cogn. Psychol. 2000, 41, 1–48. [Google Scholar] [CrossRef] [Green Version]
- Raven, J.; Raven, J.; Court, H. CPM-P, Matrizes Progressivas Coloridas; Cegoc-TEA: Lisboa, Portugal, 2009. [Google Scholar]
- Wechsler, D. Escala de Inteligência de Wechsler para Crianças—Terceira Edição (WISC-III): Manual [Wechsler Intelligence Scale for Children—Third Edition (WISC-III): Manual]; Cegoc: Lisboa, Portugal, 2003; [Adaptação portuguesa/Portuguese adaptation: Mário R. Simões, António Menezes Rocha e Carla Ferreira]. [novas edições/new editions, with most recent validity data: 2003, 2004, 2006, 2009]; Available online: https://www.edipsico.pt/files/WISC-III_daud312d.pdf (accessed on 12 August 2021).
- Wechsler, D. Wechsler Intelligence Scale for Children—Third Edition (WISC-III); The Psychological Corporation: San Antonio, TX, USA, 1991. [Google Scholar]
- Fenzi, G.F.; Giusti, L.F.; Aghini-Lombardi, F.; Bartalena, L.; Marcocci, C.; Santini, F.; Monteleone, M. Neuropsychological assessment in schoolchildren from an area of moderate iodine deficiency. J. Endocrinol. Investig. 1990, 13, 427–431. [Google Scholar] [CrossRef] [PubMed]
- Vitti, P.; Lombardi, F.A.; Antonangeli, L.; Rago, T.; Chiovato, L.; Pinchera, A.; Marcheschi, M.; Bargagna, S.; Bertuccelli, B.; Ferretti, G. Mild iodine deficiency in fetal/neonatal life and neuropsychological performances. Acta Medica Austriaca 1992, 19, 57–59. [Google Scholar]
- Lombardi, F.A.; Pinchera, A.; Antonangeli, L.; Rago, T.; Chiovato, L.; Bargagna, S.; Vitti, P. Mild iodine deficiency during fetal/neonatal life and neuropsychological impairment in Tuscany. J. Endocrinol. Investig. 1995, 18, 57–62. [Google Scholar] [CrossRef] [PubMed]
- IBM SPSS 20.0; IBM SPSS Statistics 20 Core System User´s Guide; Kirkpatrick, L.A.; Feeney, B.C. (Eds.) Wadsworth Publishing: Belmont, CA, USA, 2011; ISBN 978-1285086019. [Google Scholar]
- Cohen, J. A power primer. Psychol. Bull. 1992, 112, 155. [Google Scholar] [CrossRef] [PubMed]
- Hopkins, W.G. A Scale of Magnitudes for Effect Statistics. In A New View of Statistics. 2013. Available online: https://www.sportsci.org/resource/stats/effectmag.html (accessed on 12 August 2021).
- Schroeder, A.C.; Privalsky, M.L. Thyroid hormones, T3 and T4, in the brain. Front. Endocrinol. 2014, 5, 40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Niwattisaiwong, S.; Burman, K.D.; Li-Ng, M. Iodine deficiency: Clinical implications. Clevel. Clin. J. Med. 2017, 84, 236–244. [Google Scholar] [CrossRef] [PubMed]
- Redman, K.; Ruffman, T.; Fitzgerald, P.; Skeaff, S. Iodine Deficiency and the Brain: Effects and Mechanisms. Crit. Rev. Food Sci. Nutr. 2016, 56, 2695–2713. [Google Scholar] [CrossRef]
- Monahan, M.; Boelaert, K.; Jolly, K.; Chan, S.; Barton, P.; Roberts, T.E. Costs and benefits of iodine supplementation for pregnant women in a mildly to moderately iodine-deficient population: A modelling analysis. Lancet Diabetes Endocrinol. 2015, 3, 715–722. [Google Scholar] [CrossRef] [Green Version]
- Flanagan, D.P.; Harrison, P.L. (Eds.) Contemporary Intellectual Assessment: Theories, Tests, and Issues; Guilford Press: New York, NY, USA, 2012. [Google Scholar]
- Lezak, M.D. Neuropsychological Assessment; Oxford University Press: Oxford, UK, 1995. [Google Scholar]
- Raghubar, K.; Cirino, P.; Barnes, M.; Ewing-Cobbs, L.; Fletcher, J.; Fuchs, L. Errors in multi-digit arithmetic and behavioral inattention in children with math difficulties. J. Learn. Disabil. 2009, 42, 356–371. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Raghubar, K.P.; Barnes, M.A.; Hecht, S.A. Working memory and mathematics: A review of developmental, individual difference, and cognitive approaches. Learn. Individ. Differ. 2010, 20, 110–122. [Google Scholar] [CrossRef]
- Cirino, P.T.; Morris, M.K.; Morris, R.D. Semantic, executive, and visuospatial abilities in mathematical reasoning of referred college students. Assessment 2007, 14, 94–104. [Google Scholar] [CrossRef] [Green Version]
- Geary, D.C.; Hoard, M.K.; Byrd-Craven, J.; Nugent, L.; Numtee, C. Cognitive mechanisms underlying achievement deficits in children with mathematical learning disability. Child Dev. 2007, 78, 1343–1359. [Google Scholar] [CrossRef] [PubMed]
- Moncayo, R.; Ortner, K. Multifactorial determinants of cognition—Thyroid function is not the only one. BBA Clin. 2015, 3, 289–298. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Limbert, E.; Prazeres, S.; Madureira, D.; Miranda, A.; Ribeiro, M.; Abreu, F.S.; Lemos, L. Aporte do iodo nas Regiões Autónomas da Madeira e dos Açores. Rev. Port. Endocrinol. Diabetes Metab. 2012, 7, 2–7. [Google Scholar] [CrossRef] [Green Version]
- Álvarez-Pedrerol, M.; Ribas-Fitó, N.; Torrent, M.; Julvez, J.; Ferrer, C.; Sunyer, J. TSH concentration within the normal range is associated with cognitive function and ADHD symptoms in healthy preschoolers. Clin. Endocrinol. 2007, 66, 890–898. [Google Scholar] [CrossRef]
- Correia, N.; Mullally, S.; Cooke, G.; Tun, T.K.; Phelan, N.; Feeney, J.; Gibney, J. Evidence for a specific defect in hippocampal memory in overt and subclinical hypothyroidism. J. Clin. Endocrinol. Metab. 2009, 94, 3789–3797. Available online: https://www.ncbi.nlm.nih.gov/books/NBK285556/ (accessed on 12 August 2021). [CrossRef]
- Gazzaniga, M.S. Cerebral specialization and interhemispheric communication. Brain 2000, 123, 1293–1326. [Google Scholar] [CrossRef] [Green Version]
- Cassidy, C.M.; Van Snellenberg, J.X.; Benavides, C.; Slifstein, M.; Wang, Z.; Moore, H.; Horga, G. Dynamic Connectivity between Brain Networks Supports Working Memory: Relationships to Dopamine Release and Schizophrenia. J. Neurosci. 2016, 36, 4377–4388. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Moderate Iodine-Deficient (UIC 20–49 μg/L, n = 30) | Adequate Iodine Intake (UIC 100–199 μg/L, n = 30) | p-Value a |
|---|---|---|---|
| General characteristics | |||
| Age, y | 9.03 ± 1.066 | 8.90 ± 1.029 | 0.717 |
| Gender, male | 15 (50.0%) | 16 (53.3%) | 0.796 |
| Scholar Grade, 3rd | 22 (73.3%) | 14 (46.7%) | 0.035 |
| Study characteristics | |||
| Failure to pass year, no | 20 (66.7%) | 24 (80%) | 0.561 |
| Reading habits, no | 15 (50%) | 12 (40%) | 0.549 |
| Environmental tobacco smoke exposure, no | 22 (73.3%) | 17 (56.7%) | 0.139 |
| Parents | |||
| Employed | 21 (70%) | 20 (66.7%) | 0.500 |
| Difficulties at school, no | 8 (26.7%) | 14 (46.7%) | 0.390 |
| Scholar grade | 0.204 | ||
| ≤4 | 13 (43.3%) | 8 (26.7%) | |
| 5–9 | 8 (26.7%) | 12 (40%) | |
| 9–12 | 6 (20%) | 3 (10%) | |
| >12 | 3 (10%) | 7 (23.3%) | |
| Expectations for their children, scholar grade >12 | 20 (66.7%) | 21 (70%) | 0.540 |
| Iodine supplements in pregnancy, no | 28 (93.3%) | 26 (86.7%) | 0.335 |
| Iodine Status | |||||
|---|---|---|---|---|---|
| Measure | Moderate Iodine Deficiency (UIC 20–49 μg/L, n = 30) Score 1 | Adequate Iodine Intake (UIC 100–199 μg/L, n = 30) Score 1 | p 2 | Cohen´s d 5 | Cohen´s Standard 6 |
| IQ full scores | |||||
| Full Scale IQ | 86.67 ± 23.042 | 101.80 ± 22.605 | 0.013 | 0.7 (43%) | Very Large |
| Verbal IQ 3 | 44.50 ± 13.612 | 52.50 ± 13.216 | 0.024 | 0.6 (38.2%) | Large |
| Performance IQ 4 | 42.17 ± 13.447 | 49.30 ± 11.532 | 0.031 | 0.6 (33%) | Large |
| Age-standardized IQ percentiles scores | |||||
| Full Scale IQ | 29.66 ± 29.704 | 50.73 ± 31.796 | 0.010 | 0.7 (43%) | Very Large |
| Verbal IQ 3 | 36.29 ± 30.913 | 58.53 ± 30.937 | 0.007 | 0.7 (43%) | Very Large |
| Performance IQ 4 | 32.08 ± 32.104 | 47.07 ± 31.341 | 0.072 | 0.5 (33%) | Large |
| Measure | Iodine Status | ||||
|---|---|---|---|---|---|
| Moderate Iodine Deficiency (UIC 20–49 μg/L, n = 30) Score 1 | Adequate Iodine Intake (UIC 100–199 μg/L, n = 30) Score 1 | p2 | Cohen´s d 3 | Cohen´s Standard 4 | |
| Verbal IQ | |||||
| Information | 7.53 ± 2.80 | 9.23 ± 2.86 | 0.024 | 0.6 | Large |
| Similarities | 9.87 ± 3.33 | 12.20 ± 3.82 | 0.014 | 0.7 | Very Large |
| Arithmetic | 10.00 ± 2.96 | 10.73 ± 2.63 | 0.314 | ||
| Vocabulary | 8.80 ± 3.70 | 10.27 ± 3.90 | 0.141 | ||
| Comprehension | 8.30 ± 4.16 | 10.07 ± 3.27 | 0.073 | ||
| Digit Span | 8.20 ± 3.18 | 10.40 ± 2.84 | 0.006 | 0.7 | Very Large |
| Performance IQ | |||||
| Picture Completion | 8.57 ± 3.68 | 11.27 ± 3.81 | 0.007 | 0.7 | Very Large |
| Coding | 7.57 ± 3.42 | 7.63 ± 2.80 | 0.934 | ||
| Picture Arrangement | 9.13 ± 3.42 | 11.13 ± 3.40 | 0.027 | 0.6 | Large |
| Block Design | 8.40 ± 3.66 | 10.47 ± 3.35 | 0.026 | 0.6 | Large |
| Object Assembly | 8.50 ± 3.71 | 8.80 ± 3.27 | 0.741 | ||
| Symbol Search | 7.33 ± 3.28 | 8.20 ± 3.33 | 0.314 | ||
| Mazes | 8.40 ± 3.23 | 9.93 ± 4.06 | 0.111 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bailote, H.B.; Linhares, D.; Carvalho, C.; Prazeres, S.; Rodrigues, A.S.; Garcia, P. Iodine Intake and Related Cognitive Function Impairments in Elementary Schoolchildren. Biology 2022, 11, 1507. https://doi.org/10.3390/biology11101507
Bailote HB, Linhares D, Carvalho C, Prazeres S, Rodrigues AS, Garcia P. Iodine Intake and Related Cognitive Function Impairments in Elementary Schoolchildren. Biology. 2022; 11(10):1507. https://doi.org/10.3390/biology11101507
Chicago/Turabian StyleBailote, Helga B., Diana Linhares, Célia Carvalho, Susana Prazeres, Armindo S. Rodrigues, and Patrícia Garcia. 2022. "Iodine Intake and Related Cognitive Function Impairments in Elementary Schoolchildren" Biology 11, no. 10: 1507. https://doi.org/10.3390/biology11101507
APA StyleBailote, H. B., Linhares, D., Carvalho, C., Prazeres, S., Rodrigues, A. S., & Garcia, P. (2022). Iodine Intake and Related Cognitive Function Impairments in Elementary Schoolchildren. Biology, 11(10), 1507. https://doi.org/10.3390/biology11101507