
Olfactory Impairment Correlates with Executive Functions Disorders and Other Specific Cognitive Dysfunctions in Parkinson’s Disease

 ,
,  ,
,  , , and
, , and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Procedures
2.3. Data Analysis
2.4. Ethical Considerations
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Fullard, M.E.; Morley, J.F.; Duda, J.E. Olfactory Dysfunction as an Early Biomarker in Parkinson’s Disease. Neurosci. Bull. 2017, 33, 515–525. [Google Scholar] [CrossRef] [PubMed]
- Ercoli, T.; Masala, C.; Cadeddu, G.; Mascia, M.M.; Orofino, G.; Gigante, A.F.; Solla, P.; Defazio, G.; Rocchi, L. Does Olfactory Dysfunction Correlate with Disease Progression in Parkinson’s Disease? A Systematic Review of the Current Literature. Brain Sci. 2022, 12, 513. [Google Scholar] [CrossRef] [PubMed]
- Doty, R. Olfactory dysfunction in Parkinson disease. Nat. Rev. Neurol. 2012, 8, 329–339. [Google Scholar] [CrossRef]
- Haehner, A.; Masala, C.; Walter, S.; Reichmann, H.; Hummel, T. Incidence of Parkinson’s disease in a large patient cohort with idiopathic smell and taste loss. J. Neurol. 2019, 266, 339–345. [Google Scholar] [CrossRef] [PubMed]
- Hanagasi, H.A.; Tufekcioglu, Z.; Emre, M. Dementia in Parkinson’s disease. J. Neurol. Sci. 2017, 374, 26–31. [Google Scholar] [CrossRef]
- Kwon, K.Y.; Kang, S.H.; Kim, M.; Lee, H.M.; Jang, J.W.; Kim, J.Y.; Lee, S.M.; Koh, S.B. Nonmotor Symptoms and Cognitive Decline in de novo Parkinson’s Disease. Can. J. Neurol. Sci. 2014, 41, 597–602. [Google Scholar] [CrossRef] [Green Version]
- Kang, S.H.; Lee, H.M.; Seo, W.K.; Kim, J.H.; Koh, S.B. The combined effect of REM sleep behavior disorder and hyposmia on cognition and motor phenotype in Parkinson’s disease. J. Neurol. Sci. 2016, 368, 374–378. [Google Scholar] [CrossRef]
- Kawasaki, I.; Baba, T.; Takeda, A.; Mori, E. Loss of awareness of hyposmia is associated with mild cognitive impairment in Parkinson’s disease. Parkinsonism Relat. Disord. 2016, 22, 74–79. [Google Scholar] [CrossRef]
- Pekel, N.B.; Yildiz, D.; Taymur, İ.; Budak, E.; Özmen, S.; Çapkur, Ç.; Seferoğlu, M.; Güneş, A.; Siğirli, D. Associations between Olfactory Impairment and Cognitive Functions in Patients with Parkinson Disease. Arch. Neuropsychiatry 2019, 57, 216–221. [Google Scholar]
- Baba, T.; Kikuchi, A.; Hirayama, K.; Nishio, Y.; Hosokai, Y.; Kanno, S.; Hasegawa, T.; Sugeno, N.; Konno, M.; Suzuki, K.; et al. Severe olfactory dysfunction is a prodromal symptom of dementia associated with Parkinson’s disease: A 3 year longitudinal study. Brain 2012, 135, 161–169. [Google Scholar] [CrossRef] [Green Version]
- Fang, T.C.; Chang, M.H.; Yang, C.P.; Chen, Y.H.; Lin, C.H. The Association of Olfactory Dysfunction with Depression, Cognition, and Disease Severity in Parkinson’s Disease. Front. Neurol. 2021, 12, 779712. [Google Scholar] [CrossRef]
- Sheng, M.Z.; Fang, T.C.; Chen, Y.H.; Chang, M.H.; Yang, C.P.; Lin, C.H. Is either anosmia or constipation associated with cognitive dysfunction in Parkinson’s disease? PLoS ONE 2021, 16, e0252451. [Google Scholar] [CrossRef] [PubMed]
- Masala, C.; Solla, P.; Liscia, A.; Defazio, G.; Saba, L.; Cannas, A.; Cavazzana, A.; Hummel, T.; Haehner, A. Correlation among olfactory function, motors’ symptoms, cognitive impairment, apathy, and fatigue in patients with Parkinson’s disease. J. Neurol. 2018, 265, 1764–1771. [Google Scholar] [CrossRef] [PubMed]
- Domellöf, M.E.; Lundin, K.F.; Edström, M.; Forsgren, L. Olfactory dysfunction and dementia in newly diagnosed patients with Parkinson’s disease. Park. Relat. Disord. 2017, 38, 41–47. [Google Scholar] [CrossRef] [PubMed]
- Cecchini, M.P.; Federico, A.; Zanini, A.; Mantovani, E.; Masala, C.; Tinazzi, M.; Tamburin, S. Olfaction and taste in Parkinson’s disease: The association with mild cognitive impairment and the single cognitive domain dysfunction. J. Neural. Transm. 2019, 126, 585–595. [Google Scholar] [CrossRef]
- Postuma, R.B.; Berg, D.; Stern, M.; Poewe, W.; Olanow, C.W.; Oertel, W.; Obeso, J.; Marek, K.; Litvan, I.; Lang, A.E.; et al. MDS clinical diagnostic criteria for Parkinson’s disease. Mov. Disord. 2015, 30, 1591–1601. [Google Scholar] [CrossRef]
- Fahn, S.; Elton, R. Members of the UPDRS Development Committee. The Unified Parkinson’s Disease Rating Scale. In Recent Developments in Parkinson’s Disease; Fahn, S., Marsde, C.D., Calne, D.B., Goldstein, M., Eds.; McMellam Health Care Information: Florham Park, NJ, USA, 1987; Volume 2, pp. 153–163. [Google Scholar]
- Hoehn, M.M.; Yahr, M.D. Parkinsonism: Onset, progression, and mortality. Neurology 1967, 17, 427–442. [Google Scholar] [CrossRef] [Green Version]
- Tomlinson, C.L.; Stowe, R.; Patel, S.; Rick, C.; Gray, R.; Clarke, C.E. Systematic review of levodopa dose equivalency re-porting in Parkinson’s disease. Mov. Disord. 2010, 25, 2649–2653. [Google Scholar] [CrossRef] [PubMed]
- Hummel, T.; Sekinger, B.; Wolf, S.; Pauli, E.; Kobal, G. ‘Sniffin’ Sticks’: Olfactory Performance Assessed by the Combined Testing of Odour Identification, Odor Discrimination and Olfactory Threshold. Chem. Senses. 1997, 22, 39–52. [Google Scholar] [CrossRef] [PubMed]
- Hummel, T.; Kobal, G.; Gudziol, H.; Mackay-Sim, A. Normative data for the “Sniffin’ Sticks” including tests of odor identification, odor discrimination, and olfactory thresholds: An upgrade based on a group of more than 3000 subjects. Eur. Arch. Otorhino-Laryngol. 2007, 264, 237–243. [Google Scholar] [CrossRef]
- Sanna, F.; Loy, F.; Piras, R.; Moat, A.; Masala, C. Age-Related Cognitive Decline and the Olfactory Identification Deficit Are Associated to Increased Level of Depression. Front. Neurosci. 2021, 15, 599593. [Google Scholar] [CrossRef] [PubMed]
- Masala, C.; Käehling, C.; Fall, F.; Hummel, T. Correlation between olfactory function, trigeminal sensitivity, and nasal anatomy in healthy subjects. Eur. Arch. Oto-Rhino-L. 2019, 276, 1649–1654. [Google Scholar] [CrossRef] [PubMed]
- Conti, S.; Bonazzi, S.; Laiacona, M.; Masina, M.; Coralli, M.V. Montreal Cognitive Assessment (MoCA)-Italian version: Regression based norms and equivalent scores. Neurol. Sci. 2015, 36, 209–214. [Google Scholar] [CrossRef] [PubMed]
- Nasreddine, Z.S.; Phillips, N.A.; Bédirian, V.; Charbonneau, S.; Whitehead, V.; Collin, I.; Cummings, J.L.; Chertkow, H. The Montreal Cognitive Assessment, MoCA: A Brief Screening Tool for Mild Cognitive Impairment. J. Am. Geriatr. Soc. 2005, 53, 695–699. [Google Scholar] [CrossRef] [PubMed]
- Julayanont, P.; Brousseau, M.; Chertkow, H.; Phillips, N.; Nasreddine, Z.S. Montreal Cognitive Assessment Memory Index Score (MoCA-MIS) as a predictor of conversion from mild cognitive impairment to Alzheimer’s disease. J. Am. Geriatr. Soc. 2014, 62, 679–684. [Google Scholar] [CrossRef]
- Stewart, S.A.; Pimer, L.; Fisk, J.D.; Rusak, B.; Leslie, R.A.; Eskes, G.; Schoffer, K.; McKelvey, J.R.; Rolheiser, T.; Khan, M.N.; et al. Olfactory Function and Diffusion Tensor Imaging as Markers of Mild Cognitive Impairment in Early Stages of Parkinson’s Disease. Clin. EEG Neurosci. 2023, 54, 91–97. [Google Scholar] [CrossRef]
- Yap, A.C.; Mahendran, R.; Kua, E.H.; Zhou, W.; Wang, Y. Olfactory dysfunction is associated with mild cognitive impairment in community-dwelling older adults. Front. Aging Neurosci. 2022, 14, 930686. [Google Scholar] [CrossRef]
- Schlintl, C.; Schienle, A. Reduced Olfactory Memory Performance Is Associated with Executive Function Deficits in Older Adults. Exp. Aging Res. 2022, 13, 1–13. [Google Scholar] [CrossRef]
- Chen, Z.; Xie, H.; Yao, L.; Wei, Y. Olfactory impairment and the risk of cognitive decline and dementia in older adults: A meta-analysis. Braz. J. Otorhinolaryngol. 2021, 87, 94–102. [Google Scholar] [CrossRef]
- Frasnelli, J.; Lundström, J.N.; Boyle, J.A.; Djordjevic, J.; Zatorre, R.J.; Jones-Gotman, M. Neuroanatomical correlates of olfactory performance. Exp. Brain Res. 2010, 201, 1–11. [Google Scholar] [CrossRef]
- Fjaeldstad, A.W.; Stiller-Stut, F.; Gleesborg, C.; Kringelbach, M.L.; Hummel, T.; Fernandes, H.M. Validation of Olfactory Network Based on Brain Structural Connectivity and Its Association with Olfactory Test Scores. Front. Syst. Neurosci. 2021, 15, 638053. [Google Scholar] [CrossRef] [PubMed]
- Wilson, R.S.; Arnold, S.E.; Tang, Y.; Bennett, D.A. Odor identification and decline in different cognitive domains in old age. Neuroepidemiology 2006, 26, 61–67. [Google Scholar] [CrossRef] [PubMed]
- Fagundo, A.B.; Jiménez-Murcia, S.; Giner-Bartolomé, C.; Islam, M.A.; de la Torre, R.; Pastor, A.; Casanueva, F.F.; Crujeiras, A.B.; Granero, R.; Baños, R.; et al. Modulation of Higher-Order Olfaction Components on Executive Functions in Humans. PLoS ONE 2015, 10, e0130319. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stuss, D.T.; Alexander, M.P. Executive functions and the frontal lobes: A conceptual view. Psychol. Res. 2000, 63, 289–298. [Google Scholar] [CrossRef]
- Challakere Ramaswamy, V.M.; Schofield, P.W. Olfaction and Executive Cognitive Performance: A Systematic Review. Front. Psychol. 2022, 13, 871391. [Google Scholar] [CrossRef] [PubMed]
- Chaudhary, S.; Kumaran, S.S.; Goyal, V.; Kalaivani, M.; Kaloiya, G.S.; Sagar, R.; Mehta, N.; Srivastava, A.K.; Jagannathan, N.R. Frontal lobe metabolic alterations characterizing Parkinson’s disease cognitive impairment. Neurol. Sci. 2021, 42, 1053–1064. [Google Scholar] [CrossRef]
- Berry, E.L.; Nicolson, R.I.; Foster, J.K.; Behrmann, M.; Sagar, H.J. Slowing of reaction time in Parkinson’s disease: The involvement of the frontal lobes. Neuropsychologia 1999, 37, 787–795. [Google Scholar] [CrossRef]
- Nordin, S.; Murphy, C. Odor memory in normal aging and Alzheimer’s disease. Ann. N. Y. Acad. Sci. 1998, 855, 686–693. [Google Scholar] [CrossRef]
- Solla, P.; Masala, C.; Liscia, A.; Piras, R.; Ercoli, T.; Fadda, L.; Hummel, T.; Haenher, A.; Defazio, G. Sex-related differences in olfactory function and evaluation of possible confounding factors among patients with Parkinson’s disease. J. Neurol. 2020, 267, 57–63. [Google Scholar] [CrossRef]
- Liu, R.; Umbach, D.M.; Peddada, S.D.; Xu, Z.; Tröster, A.I.; Huang, X.; Chen, H. Potential sex diferences in nonmotor symptoms in early drug-naive Parkinson disease. Neurology 2015, 84, 2107–2115. [Google Scholar] [CrossRef] [Green Version]
- Picillo, M.; Amboni, M.; Erro, R.; Longo, K.; Vitale, C.; Mocci, M.; Pierro, A.; Santangelo, G.; De Rosa, A.; De Michele, G.; et al. Gender diferences in non-motor symptoms in early, drug naïve Parkinson’s disease. J. Neurol. 2013, 260, 2849–2855. [Google Scholar] [CrossRef]
- San Luciano, M.; Wang, C.; Ortega, R.A.; Giladi, N.; Marder, K.; Bressman, S.; Saunders-Pullman, R.; Michael, J. Fox Foundation LRRK2 Consortium. Sex differences in LRRK2 G2019S and idiopathic Parkinson’s Disease. Ann. Clin. Transl. Neurol. 2017, 4, 801–810. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mertens, A.T.; Santo, J.B.; Markopoulou, K.; Chase, B.A. Cognitive processes that indirectly affect olfactory dysfunction in Parkinson’s disease. Clin. Park. Relat. Disord. 2019, 1, 13–20. [Google Scholar] [CrossRef] [PubMed]
- Gjerde, K.V.; Müller, B.; Skeie, G.O.; Assmus, J.; Alves, G.; Tysnes, O.B. Hyposmia in a simple smell test is associated with accelerated cognitive decline in early Parkinson’s disease. Acta Neurol. Scand. 2018, 138, 508–514. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.; Yu, K.H.; Lee, B.C.; Kim, B.C.; Kang, Y. Validity of the Montreal Cognitive Assessment (MoCA) Index Scores: A Comparison with the Cognitive Domain Scores of the Seoul Neuropsychological Screening Battery (SNSB). Dement. Neurocogn. Disord. 2021, 20, 28–37. [Google Scholar] [CrossRef]
- Kasten, M.; Bruggemann, N.; Schmidt, A.; Klein, C. Validity of the MoCA and MMSE in the detection of MCI and dementia in Parkinson disease. Neurologyz 2010, 75, 478. [Google Scholar] [CrossRef]


{kind=link}
| Demographics | PD | Control | p Value |
|---|---|---|---|
| N = 178 | N = 98 | ||
| Sex N (% female) | 75 (%42.1) | 52 (%53.1) | 0.081 |
| Age | 70.2 ± 9.3 | 68.4 ± 8.0 | 0.099 |
| Weight (kg) | 71.7 ± 15.9 | 70.1 ± 15.0 | 0.412 |
| Height (cm) | 164 ± 0.01 | 164 ± 0.1 | 0.999 |
| BMI | 26.6 ± 4.9 | 25.9 ± 4.1 | 0.344 |
| PD duration (years) | 4.2 ± 3.6 | NA | NA |
| UPDRS | 2.1 ± 0.8 | NA | NA |
| LEDD | 353 ± 293 | NA | NA |
| HY | 20.8 ± 12.5 | NA | NA |
| OT | 2.6 ± 2.2 | 5.7 ± 4.3 | 0.001 |
| OD | 7.5 ± 3.1 | 10.5 ± 2.7 | 0.001 |
| OI | 7.6 ± 3.3 | 11.7 ± 2.5 | 0.001 |
| TDI | 17.7 ± 6.9 | 28.0 ± 7.1 | 0.001 |
| MoCA | 21.1 ± 5.2 | 25.7 ± 3.2 | 0.001 |
| Groups | N | Mean ± SD | p Value | |
|---|---|---|---|---|
| OIS | PD | 178 | 5.7 ± 0.8 | 0.008 |
| Controls | 98 | 6.0 ± 0.2 | ||
| AIS | PD | 178 | 7.4 ± 2.4 | 0.001 |
| Controls | 98 | 9.3 ± 2.1 | ||
| LIS | PD | 178 | 4.3 ± 1.2 | 0.001 |
| Controls | 98 | 5.1 ± 0.9 | ||
| VIS | PD | 178 | 4.9 ± 1.7 | 0.001 |
| Controls | 98 | 6.4 ± 1.0 | ||
| MIS | PD | 178 | 1.6 ± 1.6 | 0.001 |
| Controls | 98 | 2.3 ± 1.6 | ||
| EIS | PD | 178 | 8.7 ± 3.2 | 0.001 |
| Controls | 98 | 11.5 ± 1.7 |
| OIS | AIS | LIS | VIS | MIS | EIS | ||
|---|---|---|---|---|---|---|---|
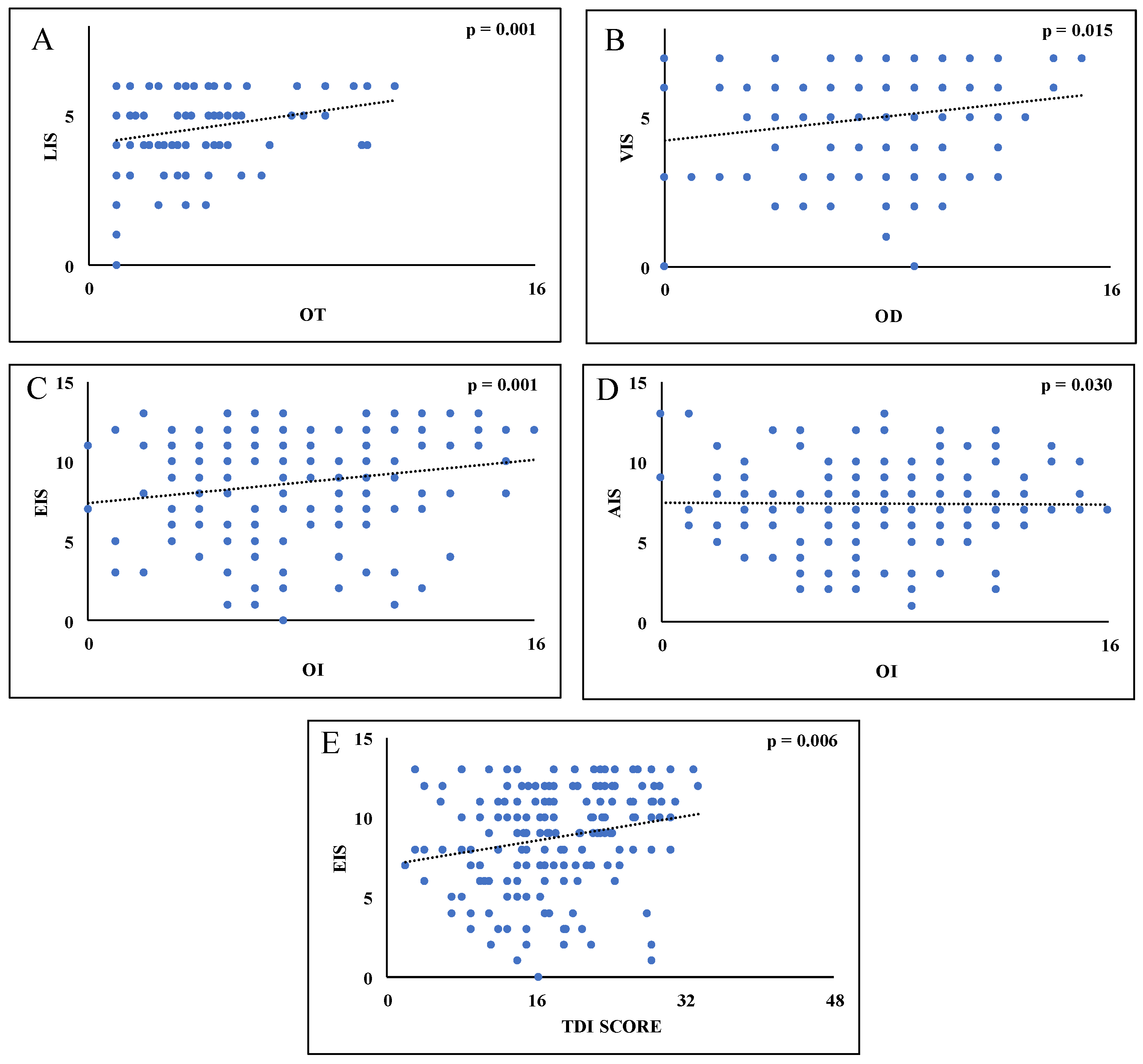
| OT | r | −0.009 | 0.193 | 0.245 | 0.181 | 0.099 | 0.161 |
| p | 0.097 | 0.010 | 0.001 | 0.016 | 0.188 | 0.031 | |
| OD | r | 0.103 | 0.002 | 0.153 | 0.183 | 0.112 | 0.152 |
| p | 0.171 | 0.978 | 0.041 | 0.015 | 0.136 | 0.043 | |
| OI | r | 0.130 | −0.009 | 0.086 | 0.114 | 0.113 | 0.176 |
| p | 0.084 | 0.906 | 0.254 | 0.128 | 0.134 | 0.019 | |
| TDI | r | 0.106 | 0.061 | 0.192 | 0.196 | 0.136 | 0.206 |
| p | 0.158 | 0.417 | 0.01 | 0.009 | 0.069 | 0.006 |
| Unstandardized Coefficients | Standardized Coefficients | ||||
|---|---|---|---|---|---|
| B | Std Error | β | t | p | |
| Model 1: OT as a dependent variable | |||||
| LIS | 0.454 | 0.135 | 0.245 | 3.358 | 0.001 |
| Age | −0.021 | 0.019 | −0.084 | −1.087 | 0.279 |
| Sex | 0.700 | 0.338 | 0.152 | 2.070 | 0.040 |
| Model 2: OD as a dependent variable | |||||
| VIS | 0.331 | 0.134 | 0.183 | 2.468 | 0.015 |
| Age | −0.059 | 0.026 | −0.174 | −2.259 | 0.025 |
| Sex | 1.222 | 0.463 | 0.193 | 2.637 | 0.009 |
| Model 3: OI as a dependent variable | |||||
| EIS | 0.323 | 0.100 | 0.311 | 3.238 | 0.001 |
| AIS | −0.286 | 0.131 | −0.210 | −2.182 | 0.030 |
| Age | −0.083 | 0.027 | −0.231 | −3.090 | 0.002 |
| Sex | 1.421 | 0.483 | 0.211 | 2.943 | 0.004 |
| Model 4: TDI Score as a dependent variable | |||||
| EIS | 0.444 | 0.159 | 0.206 | 2.790 | 0.006 |
| Age | −0.176 | 0.056 | −0.236 | −3.166 | 0.002 |
| Sex | 3.365 | 0.999 | 0.240 | 3.368 | 0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Solla, P.; Masala, C.; Ercoli, T.; Frau, C.; Bagella, C.; Pinna, I.; Loy, F.; Defazio, G. Olfactory Impairment Correlates with Executive Functions Disorders and Other Specific Cognitive Dysfunctions in Parkinson’s Disease. Biology 2023, 12, 112. https://doi.org/10.3390/biology12010112
Solla P, Masala C, Ercoli T, Frau C, Bagella C, Pinna I, Loy F, Defazio G. Olfactory Impairment Correlates with Executive Functions Disorders and Other Specific Cognitive Dysfunctions in Parkinson’s Disease. Biology. 2023; 12(1):112. https://doi.org/10.3390/biology12010112
Chicago/Turabian StyleSolla, Paolo, Carla Masala, Tommaso Ercoli, Claudia Frau, Caterina Bagella, Ilenia Pinna, Francesco Loy, and Giovanni Defazio. 2023. "Olfactory Impairment Correlates with Executive Functions Disorders and Other Specific Cognitive Dysfunctions in Parkinson’s Disease" Biology 12, no. 1: 112. https://doi.org/10.3390/biology12010112
APA StyleSolla, P., Masala, C., Ercoli, T., Frau, C., Bagella, C., Pinna, I., Loy, F., & Defazio, G. (2023). Olfactory Impairment Correlates with Executive Functions Disorders and Other Specific Cognitive Dysfunctions in Parkinson’s Disease. Biology, 12(1), 112. https://doi.org/10.3390/biology12010112