
Recent Advances in Image-Guided Locoregional Therapies for Primary Liver Tumors

Abstract
:Simple Summary
Abstract

1. Introduction
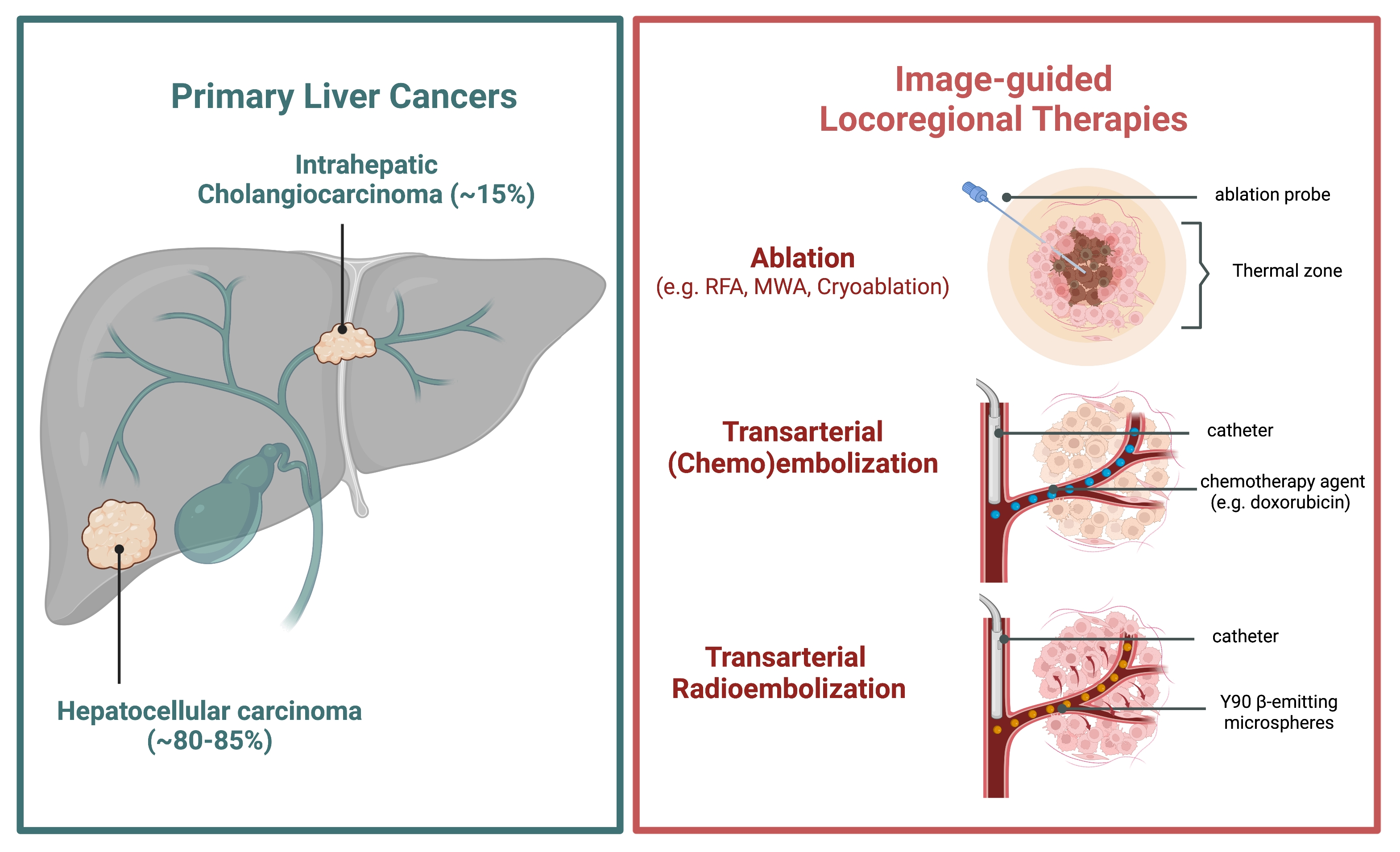
2. Primary Liver Cancers
2.1. Hepatocellular Carcinoma
2.2. Intrahepatic Cholangiocarcinoma
3. Image-Guided, Tumor-Directed Locoregional Therapies
3.1. Rationale for Liver Cancer Treatment
3.2. Ablation Techniques
3.3. Transarterial Chemoembolization Techniques
3.4. Transarterial Radioembolization Techniques
3.5. Combining Image-Guided Locoregional Modalities
4. Locoregional and Immunological Therapies
4.1. Immunological Basis of Image-Guided Tumor-Directed Therapies
4.2. Combining Image-Guided Therapies with Immunotherapy
5. Discussion and Future Directions
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Augustine, M.M.; Fong, Y. Epidemiology and Risk Factors of Biliary Tract and Primary Liver Tumors. Surg. Oncol. Clin. 2014, 23, 171–188. [Google Scholar] [CrossRef] [PubMed]
- Makary, M.S.; Khandpur, U.; Cloyd, J.M.; Mumtaz, K.; Dowell, J.D. Locoregional Therapy Approaches for Hepatocellular Carcinoma: Recent Advances and Management Strategies. Cancers 2020, 12, 1914. [Google Scholar] [CrossRef]
- Labib, P.L.; Davidson, B.R.; Sharma, R.A.; Pereira, S.P. Locoregional Therapies in Cholangiocarcinoma. Hepatic Oncol. 2017, 4, 99–109. [Google Scholar] [CrossRef] [PubMed]
- Bosch, F.X.; Ribes, J.; Díaz, M.; Cléries, R. Primary Liver Cancer: Worldwide Incidence and Trends. Gastroenterology 2004, 127, S5–S16. [Google Scholar] [CrossRef] [PubMed]
- Owen, M.; Makary, M.S.; Beal, E.W. Locoregional Therapy for Intrahepatic Cholangiocarcinoma. Cancers 2023, 15, 2384. [Google Scholar] [CrossRef]
- Llovet, J.M.; Lencioni, R. MRECIST for HCC: Performance and Novel Refinements. J. Hepatol. 2020, 72, 288–306. [Google Scholar] [CrossRef] [Green Version]
- Ko, C.-C.; Yeh, L.-R.; Kuo, Y.-T.; Chen, J.-H. Imaging Biomarkers for Evaluating Tumor Response: RECIST and Beyond. Biomark. Res. 2021, 9, 52. [Google Scholar] [CrossRef]
- Center, M.M.; Jemal, A. International Trends in Liver Cancer Incidence Rates. Cancer Epidemiol Biomark. Prev 2011, 20, 2362–2368. [Google Scholar] [CrossRef] [Green Version]
- McGlynn, K.A.; Petrick, J.L.; El-Serag, H.B. Epidemiology of Hepatocellular Carcinoma. Hepatology 2021, 73 (Suppl. S1), 4–13. [Google Scholar] [CrossRef]
- Janevska, D.; Chaloska-Ivanova, V.; Janevski, V. Hepatocellular Carcinoma: Risk Factors, Diagnosis and Treatment. Open Access Maced. J. Med. Sci. 2015, 3, 732–736. [Google Scholar] [CrossRef] [Green Version]
- Younossi, Z.M.; Henry, L. Epidemiology of Non-Alcoholic Fatty Liver Disease and Hepatocellular Carcinoma. JHEP Rep. 2021, 3, 100305. [Google Scholar] [CrossRef]
- Flores, Y.N.; Datta, G.D.; Yang, L.; Corona, E.; Devineni, D.; Glenn, B.A.; Bastani, R.; May, F.P. Disparities in Hepatocellular Carcinoma Incidence, Stage, and Survival: A Large Population-Based Study. Cancer Epidemiol. Biomark. Prev. 2021, 30, 1193–1199. [Google Scholar] [CrossRef]
- Balogh, J.; Victor, D.; Asham, E.H.; Burroughs, S.G.; Boktour, M.; Saharia, A.; Li, X.; Ghobrial, R.M.; Monsour, H.P. Hepatocellular Carcinoma: A Review. J. Hepatocell. Carcinoma 2016, 3, 41–53. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chidambaranathan-Reghupaty, S.; Fisher, P.B.; Sarkar, D. Hepatocellular Carcinoma (HCC): Epidemiology, Etiology and Molecular Classification. Adv. Cancer Res. 2021, 149, 1–61. [Google Scholar] [CrossRef] [PubMed]
- Schlageter, M.; Terracciano, L.M.; D’Angelo, S.; Sorrentino, P. Histopathology of Hepatocellular Carcinoma. World J. Gastroenterol. 2014, 20, 15955–15964. [Google Scholar] [CrossRef]
- Wu, Y.; Liu, Z.; Xu, X. Molecular Subtyping of Hepatocellular Carcinoma: A Step toward Precision Medicine. Cancer Commun. 2020, 40, 681–693. [Google Scholar] [CrossRef] [PubMed]
- Brar, G.; Greten, T.F.; Graubard, B.I.; McNeel, T.S.; Petrick, J.L.; McGlynn, K.A.; Altekruse, S.F. Hepatocellular Carcinoma Survival by Etiology: A SEER-Medicare Database Analysis. Hepatol. Commun. 2020, 4, 1541–1551. [Google Scholar] [CrossRef]
- Reig, M.; Forner, A.; Rimola, J.; Ferrer-Fàbrega, J.; Burrel, M.; Garcia-Criado, Á.; Kelley, R.K.; Galle, P.R.; Mazzaferro, V.; Salem, R.; et al. BCLC Strategy for Prognosis Prediction and Treatment Recommendation: The 2022 Update. J. Hepatol. 2022, 76, 681–693. [Google Scholar] [CrossRef]
- Brindley, P.J.; Bachini, M.; Ilyas, S.I.; Khan, S.A.; Loukas, A.; Sirica, A.E.; Teh, B.T.; Wongkham, S.; Gores, G.J. Cholangiocarcinoma. Nat. Rev. Dis. Primers 2021, 7, 65. [Google Scholar] [CrossRef]
- Halder, R.; Amaraneni, A.; Shroff, R.T. Cholangiocarcinoma: A Review of the Literature and Future Directions in Therapy. Hepatobiliary Surg. Nutr. 2022, 11, 555–566. [Google Scholar] [CrossRef]
- Ustundag, Y.; Bayraktar, Y. Cholangiocarcinoma: A Compact Review of the Literature. World J. Gastroenterol. 2008, 14, 6458–6466. [Google Scholar] [CrossRef] [PubMed]
- Massarweh, N.N.; El-Serag, H.B. Epidemiology of Hepatocellular Carcinoma and Intrahepatic Cholangiocarcinoma. Cancer Control 2017, 24, 1073274817729245. [Google Scholar] [CrossRef]
- Patel, T. Worldwide Trends in Mortality from Biliary Tract Malignancies. BMC Cancer 2002, 2, 10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taylor-Robinson, S.; Toledano, M.; Arora, S.; Keegan, T.; Hargreaves, S.; Beck, A.; Khan, S.; Elliott, P.; Thomas, H. Increase in Mortality Rates from Intrahepatic Cholangiocarcinoma in England and Wales 1968–1998. Gut 2001, 48, 816–820. [Google Scholar] [CrossRef] [Green Version]
- Van Dyke, A.L.; Shiels, M.S.; Jones, G.S.; Pfeiffer, R.M.; Petrick, J.L.; Beebe-Dimmer, J.L.; Koshiol, J. Biliary Tract Cancer Incidence and Trends in the United States by Demographic Group, 1999–2013. Cancer 2019, 125, 1489–1498. [Google Scholar] [CrossRef] [PubMed]
- Saha, S.K.; Zhu, A.X.; Fuchs, C.S.; Brooks, G.A. Forty-Year Trends in Cholangiocarcinoma Incidence in the U.S.: Intrahepatic Disease on the Rise. Oncologist 2016, 21, 594–599. [Google Scholar] [CrossRef] [Green Version]
- Tyson, G.L.; El-Serag, H.B. Risk Factors of Cholangiocarcinoma. Hepatology 2011, 54, 173–184. [Google Scholar] [CrossRef] [Green Version]
- Banales, J.M.; Marin, J.J.G.; Lamarca, A.; Rodrigues, P.M.; Khan, S.A.; Roberts, L.R.; Cardinale, V.; Carpino, G.; Andersen, J.B.; Braconi, C.; et al. Cholangiocarcinoma 2020: The next Horizon in Mechanisms and Management. Nat. Rev. Gastroenterol. Hepatol. 2020, 17, 557–588. [Google Scholar] [CrossRef]
- Shirono, T.; Niizeki, T.; Iwamoto, H.; Shimose, S.; Suzuki, H.; Kawaguchi, T.; Kamachi, N.; Noda, Y.; Okamura, S.; Nakano, M.; et al. Therapeutic Outcomes and Prognostic Factors of Unresectable Intrahepatic Cholangiocarcinoma: A Data Mining Analysis. J. Clin. Med. 2021, 10, 987. [Google Scholar] [CrossRef]
- Mavros, M.N.; Economopoulos, K.P.; Alexiou, V.G.; Pawlik, T.M. Treatment and Prognosis for Patients with Intrahepatic Cholangiocarcinoma: Systematic Review and Meta-Analysis. JAMA Surg. 2014, 149, 565–574. [Google Scholar] [CrossRef] [Green Version]
- Sumiyoshi, T.; Shima, Y.; Okabayashi, T.; Negoro, Y.; Shimada, Y.; Iwata, J.; Matsumoto, M.; Hata, Y.; Noda, Y.; Sui, K.; et al. Chemoradiotherapy for Initially Unresectable Locally Advanced Cholangiocarcinoma. World J. Surg. 2018, 42, 2910–2918. [Google Scholar] [CrossRef]
- Alvaro, D.; Gores, G.J.; Walicki, J.; Hassan, C.; Sapisochin, G.; Komuta, M.; Forner, A.; Valle, J.W.; Laghi, A.; Rizvi, S.I.; et al. EASL-ILCA Clinical Practice Guidelines on the Management of Intrahepatic Cholangiocarcinoma. J. Hepatol. 2023, 79, 181–208. [Google Scholar] [CrossRef]
- Breedis, C.; Young, G. The Blood Supply of Neoplasms in the Liver. Am. J. Pathol. 1954, 30, 969–977. [Google Scholar]
- Yoshida, K.; Matsui, O.; Miyayama, S.; Ibukuro, K.; Yoneda, N.; Inoue, D.; Kozaka, K.; Minami, T.; Koda, W.; Gabata, T. Isolated Arteries Originating from the Intrahepatic Arteries: Anatomy, Function, and Importance in Intervention. J. Vasc. Interv. Radiol. 2018, 29, 531–537.e1. [Google Scholar] [CrossRef] [PubMed]
- Hare, A.E.; Makary, M.S. Locoregional Approaches in Cholangiocarcinoma Treatment. Cancers 2022, 14, 5853. [Google Scholar] [CrossRef]
- Bridgewater, J.; Galle, P.R.; Khan, S.A.; Llovet, J.M.; Park, J.-W.; Patel, T.; Pawlik, T.M.; Gores, G.J. Guidelines for the Diagnosis and Management of Intrahepatic Cholangiocarcinoma. J. Hepatol. 2014, 60, 1268–1289. [Google Scholar] [CrossRef] [Green Version]
- Ryan, M.J.; Willatt, J.; Majdalany, B.S.; Kielar, A.Z.; Chong, S.; Ruma, J.A.; Pandya, A. Ablation Techniques for Primary and Metastatic Liver Tumors. World J. Hepatol. 2016, 8, 191–199. [Google Scholar] [CrossRef] [PubMed]
- Deng, Q.; He, M.; Fu, C.; Feng, K.; Ma, K.; Zhang, L. Radiofrequency Ablation in the Treatment of Hepatocellular Carcinoma. Int. J. Hyperth. 2022, 39, 1052–1063. [Google Scholar] [CrossRef] [PubMed]
- Izzo, F.; Granata, V.; Grassi, R.; Fusco, R.; Palaia, R.; Delrio, P.; Carrafiello, G.; Azoulay, D.; Petrillo, A.; Curley, S.A. Radiofrequency Ablation and Microwave Ablation in Liver Tumors: An Update. Oncologist 2019, 24, e990–e1005. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Poulou, L.S.; Botsa, E.; Thanou, I.; Ziakas, P.D.; Thanos, L. Percutaneous Microwave Ablation vs Radiofrequency Ablation in the Treatment of Hepatocellular Carcinoma. World J. Hepatol. 2015, 7, 1054–1063. [Google Scholar] [CrossRef]
- Kalra, N.; Gupta, P.; Chawla, Y.; Khandelwal, N. Locoregional Treatment for Hepatocellular Carcinoma: The Best Is yet to Come. World J. Radiol. 2015, 7, 306–318. [Google Scholar] [CrossRef]
- Criss, C.R.; Makary, M.S. Salvage Locoregional Therapies for Recurrent Hepatocellular Carcinoma. World J. Gastroenterol. 2023, 29, 413–424. [Google Scholar] [CrossRef]
- Majumdar, A.; Roccarina, D.; Thorburn, D.; Davidson, B.R.; Tsochatzis, E.; Gurusamy, K.S. Management of People with Early- or Very Early-stage Hepatocellular Carcinoma. Cochrane Database Syst. Rev. 2017, 2017, CD011650. [Google Scholar] [CrossRef]
- Sommer, C.M.; Kauczor, H.U.; Pereira, P.L. Locoregional Therapies of Cholangiocarcinoma. Visc. Med. 2016, 32, 414–420. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lencioni, R. Loco-Regional Treatment of Hepatocellular Carcinoma. Hepatology 2010, 52, 762–773. [Google Scholar] [CrossRef] [PubMed]
- Guan, Y.-S.; He, Q.; Wang, M.-Q. Transcatheter Arterial Chemoembolization: History for More than 30 Years. Int. Sch. Res. Not. 2012, 2012, 480650. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Melchiorre, F.; Patella, F.; Pescatori, L.; Pesapane, F.; Fumarola, E.; Biondetti, P.; Brambillasca, P.; Monaco, C.; Ierardi, A.M.; Franceschelli, G.; et al. DEB-TACE: A Standard Review. Future Oncol. 2018, 14, 2969–2984. [Google Scholar] [CrossRef] [PubMed]
- Song, J.E.; Kim, D.Y. Conventional vs Drug-Eluting Beads Transarterial Chemoembolization for Hepatocellular Carcinoma. World J. Hepatol. 2017, 9, 808–814. [Google Scholar] [CrossRef]
- Li, H.; Wu, F.; Duan, M.; Zhang, G. Drug-Eluting Bead Transarterial Chemoembolization (TACE) vs. Conventional TACE in Treating Hepatocellular Carcinoma Patients with Multiple Conventional TACE Treatments History: A Comparison of Efficacy and Safety. Medicine 2019, 98, e15314. [Google Scholar] [CrossRef]
- Ikeda, M.; Arai, Y.; Inaba, Y.; Tanaka, T.; Sugawara, S.; Kodama, Y.; Aramaki, T.; Anai, H.; Morita, S.; Tsukahara, Y.; et al. Conventional or Drug-Eluting Beads? Randomized Controlled Study of Chemoembolization for Hepatocellular Carcinoma: JIVROSG-1302. Liver Cancer 2022, 11, 440–450. [Google Scholar] [CrossRef]
- Llovet, J.M.; Real, M.I.; Montaña, X.; Planas, R.; Coll, S.; Aponte, J.; Ayuso, C.; Sala, M.; Muchart, J.; Solà, R.; et al. Arterial Embolisation or Chemoembolisation versus Symptomatic Treatment in Patients with Unresectable Hepatocellular Carcinoma: A Randomised Controlled Trial. Lancet 2002, 359, 1734–1739. [Google Scholar] [CrossRef] [PubMed]
- Lo, C.-M.; Ngan, H.; Tso, W.-K.; Liu, C.-L.; Lam, C.-M.; Poon, R.T.-P.; Fan, S.-T.; Wong, J. Randomized Controlled Trial of Transarterial Lipiodol Chemoembolization for Unresectable Hepatocellular Carcinoma. Hepatology 2002, 35, 1164–1171. [Google Scholar] [CrossRef] [Green Version]
- Llovet, J.M.; Bruix, J. Systematic Review of Randomized Trials for Unresectable Hepatocellular Carcinoma: Chemoembolization Improves Survival. Hepatology 2003, 37, 429–442. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kong, J.-Y.; Li, S.-M.; Fan, H.-Y.; Zhang, L.; Zhao, H.-J.; Li, S.-M. Transarterial Chemoembolization Extends Long-Term Survival in Patients with Unresectable Hepatocellular Carcinoma. Medicine 2018, 97, e11872. [Google Scholar] [CrossRef]
- Park, S.-Y.; Kim, J.H.; Yoon, H.-J.; Lee, I.-S.; Yoon, H.-K.; Kim, K.-P. Transarterial Chemoembolization versus Supportive Therapy in the Palliative Treatment of Unresectable Intrahepatic Cholangiocarcinoma. Clin. Radiol. 2011, 66, 322–328. [Google Scholar] [CrossRef] [PubMed]
- Lv, T.-R.; Hu, H.-J.; Liu, F.; Regmi, P.; Jin, Y.-W.; Li, F.-Y. The Effect of Trans Arterial Chemoembolization in the Management of Intrahepatic Cholangiocarcinoma. A Systematic Review and Meta-Analysis. Eur. J. Surg. Oncol. 2022, 48, 956–966. [Google Scholar] [CrossRef]
- Salem, R.; Lewandowski, R.J.; Sato, K.T.; Atassi, B.; Ryu, R.K.; Ibrahim, S.; Nemcek, A.A.; Omary, R.A.; Madoff, D.C.; Murthy, R. Technical Aspects of Radioembolization with 90Y Microspheres. Tech. Vasc. Interv. Radiol. 2007, 10, 12–29. [Google Scholar] [CrossRef]
- Tohme, S.; Bou Samra, P.; Kaltenmeier, C.; Chidi, A.P.; Varley, P.R.; Tsung, A. Radioembolization for Hepatocellular Carcinoma: A Nationwide 10-Year Experience. J. Vasc. Interv. Radiol. 2018, 29, 912–919.e2. [Google Scholar] [CrossRef]
- Choi, J.W.; Kim, H.-C. Radioembolization for Hepatocellular Carcinoma: What Clinicians Need to Know. J. Liver Cancer 2022, 22, 4–13. [Google Scholar] [CrossRef]
- Sangro, B.; Iñarrairaegui, M.; Bilbao, J.I. Radioembolization for Hepatocellular Carcinoma. J. Hepatol. 2012, 56, 464–473. [Google Scholar] [CrossRef]
- Mosconi, C.; Cappelli, A.; Pettinato, C.; Golfieri, R. Radioembolization with Yttrium-90 Microspheres in Hepatocellular Carcinoma: Role and Perspectives. World J. Hepatol. 2015, 7, 738–752. [Google Scholar] [CrossRef] [PubMed]
- d’Abadie, P.; Hesse, M.; Louppe, A.; Lhommel, R.; Walrand, S.; Jamar, F. Microspheres Used in Liver Radioembolization: From Conception to Clinical Effects. Molecules 2021, 26, 3966. [Google Scholar] [CrossRef]
- Golfieri, R. SIR-Spheres Yttrium-90 Radioembolization for the Treatment of Unresectable Liver Cancers. Hepat. Oncol. 2014, 1, 265–283. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salem, R.; Johnson, G.E.; Kim, E.; Riaz, A.; Bishay, V.; Boucher, E.; Fowers, K.; Lewandowski, R.; Padia, S.A. Yttrium-90 Radioembolization for the Treatment of Solitary, Unresectable HCC: The LEGACY Study. Hepatology 2021, 74, 2342–2352. [Google Scholar] [CrossRef] [PubMed]
- Salem, R.; Gordon, A.C.; Mouli, S.; Hickey, R.; Kallini, J.; Gabr, A.; Mulcahy, M.F.; Baker, T.; Abecassis, M.; Miller, F.H.; et al. Y90 Radioembolization Significantly Prolongs Time to Progression Compared with Chemoembolization in Patients with Hepatocellular Carcinoma. Gastroenterology 2016, 151, 1155–1163.e2. [Google Scholar] [CrossRef] [Green Version]
- Mosconi, C.; Solaini, L.; Vara, G.; Brandi, N.; Cappelli, A.; Modestino, F.; Cucchetti, A.; Golfieri, R. Transarterial Chemoembolization and Radioembolization for Unresectable Intrahepatic Cholangiocarcinoma—A Systemic Review and Meta-Analysis. Cardiovasc. Interv. Radiol. 2021, 44, 728–738. [Google Scholar] [CrossRef]
- Higgins, M.C.S.S.; Soulen, M.C. Combining Locoregional Therapies in the Treatment of Hepatocellular Carcinoma. Semin. Interv. Radiol. 2013, 30, 74–81. [Google Scholar] [CrossRef] [Green Version]
- Rossi, S.; Garbagnati, F.; Lencioni, R.; Allgaier, H.P.; Marchianò, A.; Fornari, F.; Quaretti, P.; Tolla, G.D.; Ambrosi, C.; Mazzaferro, V.; et al. Percutaneous Radio-Frequency Thermal Ablation of Nonresectable Hepatocellular Carcinoma after Occlusion of Tumor Blood Supply. Radiology 2000, 217, 119–126. [Google Scholar] [CrossRef]
- Galanakis, N.; Kehagias, E.; Matthaiou, N.; Samonakis, D.; Tsetis, D. Transcatheter Arterial Chemoembolization Combined with Radiofrequency or Microwave Ablation for Hepatocellular Carcinoma: A Review. Hepat. Oncol. 2018, 5, HEP07. [Google Scholar] [CrossRef] [Green Version]
- Kung, J.W.C.; Ng, K.K.C. Role of Locoregional Therapies in the Management of Patients with Hepatocellular Carcinoma. Hepatoma Res. 2022, 8, 17. [Google Scholar] [CrossRef]
- Jiang, C.; Cheng, G.; Liao, M.; Huang, J. Individual or Combined Transcatheter Arterial Chemoembolization and Radiofrequency Ablation for Hepatocellular Carcinoma: A Time-to-Event Meta-Analysis. World J. Surg. Oncol. 2021, 19, 81. [Google Scholar] [CrossRef] [PubMed]
- Dong, W.; Zhang, T.; Wang, Z.-G.; Liu, H. Clinical Outcome of Small Hepatocellular Carcinoma after Different Treatments: A Meta-Analysis. World J. Gastroenterol. 2014, 20, 10174–10182. [Google Scholar] [CrossRef] [PubMed]
- Hoechst, B.; Voigtlaender, T.; Ormandy, L.; Gamrekelashvili, J.; Zhao, F.; Wedemeyer, H.; Lehner, F.; Manns, M.P.; Greten, T.F.; Korangy, F. Myeloid Derived Suppressor Cells Inhibit Natural Killer Cells in Patients with Hepatocellular Carcinoma via the NKp30 Receptor. Hepatology 2009, 50, 799–807. [Google Scholar] [CrossRef]
- Ringelhan, M.; Pfister, D.; O’Connor, T.; Pikarsky, E.; Heikenwalder, M. The Immunology of Hepatocellular Carcinoma. Nat. Immunol. 2018, 19, 222–232. [Google Scholar] [CrossRef]
- DeNardo, D.G.; Ruffell, B. Macrophages as Regulators of Tumor Immunity and Immunotherapy. Nat. Rev. Immunol. 2019, 19, 369–382. [Google Scholar] [CrossRef] [PubMed]
- Singh, P.; Toom, S.; Avula, A.; Kumar, V.; Rahma, O.E. The Immune Modulation Effect of Locoregional Therapies and Its Potential Synergy with Immunotherapy in Hepatocellular Carcinoma. J. Hepatocell. Carcinoma 2020, 7, 11–17. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Q.; He, Y.; Luo, N.; Patel, S.J.; Han, Y.; Gao, R.; Modak, M.; Carotta, S.; Haslinger, C.; Kind, D.; et al. Landscape and Dynamics of Single Immune Cells in Hepatocellular Carcinoma. Cell 2019, 179, 829–845.e20. [Google Scholar] [CrossRef]
- Llovet, J.M.; De Baere, T.; Kulik, L.; Haber, P.K.; Greten, T.F.; Meyer, T.; Lencioni, R. Locoregional Therapies in the Era of Molecular and Immune Treatments for Hepatocellular Carcinoma. Nat. Rev. Gastroenterol. Hepatol. 2021, 18, 293–313. [Google Scholar] [CrossRef]
- Dromi, S.A.; Walsh, M.P.; Herby, S.; Traughber, B.; Xie, J.; Sharma, K.V.; Sekhar, K.P.; Luk, A.; Liewehr, D.J.; Dreher, M.R.; et al. Radiofrequency Ablation Induces Antigen-Presenting Cell Infiltration and Amplification of Weak Tumor-Induced Immunity. Radiology 2009, 251, 58–66. [Google Scholar] [CrossRef] [Green Version]
- Widenmeyer, M.; Shebzukhov, Y.; Haen, S.P.; Schmidt, D.; Clasen, S.; Boss, A.; Kuprash, D.V.; Nedospasov, S.A.; Stenzl, A.; Aebert, H.; et al. Analysis of Tumor Antigen-Specific T Cells and Antibodies in Cancer Patients Treated with Radiofrequency Ablation. Int. J. Cancer 2011, 128, 2653–2662. [Google Scholar] [CrossRef]
- Schueller, G.; Paolini, P.; Friedl, J.; Stift, A.; Dubsky, P.; Bachleitner-Hofmann, T.; Jakesz, R.; Gnant, M. Heat Treatment of Hepatocellular Carcinoma Cells: Increased Levels of Heat Shock Proteins 70 and 90 Correlate with Cellular Necrosis. Anticancer Res. 2001, 21, 295–300. [Google Scholar] [PubMed]
- Zhang, H.; Hou, X.; Cai, H.; Zhuang, X. Effects of Microwave Ablation on T-Cell Subsets and Cytokines of Patients with Hepatocellular Carcinoma. Minim. Invasive Ther. Allied Technol. 2017, 26, 207–211. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Fu, X.; Li, T.; Yan, H. The Prognostic Value of Myeloid Derived Suppressor Cell Level in Hepatocellular Carcinoma: A Systematic Review and Meta-Analysis. PLoS ONE 2019, 14, e0225327. [Google Scholar] [CrossRef] [Green Version]
- Iwata, T.; Kondo, Y.; Kimura, O.; Morosawa, T.; Fujisaka, Y.; Umetsu, T.; Kogure, T.; Inoue, J.; Nakagome, Y.; Shimosegawa, T. PD-L1+MDSCs Are Increased in HCC Patients and Induced by Soluble Factor in the Tumor Microenvironment. Sci. Rep. 2016, 6, 39296. [Google Scholar] [CrossRef] [Green Version]
- Pinato, D.J.; Murray, S.M.; Forner, A.; Kaneko, T.; Fessas, P.; Toniutto, P.; Mínguez, B.; Cacciato, V.; Avellini, C.; Diaz, A.; et al. Trans-Arterial Chemoembolization as a Loco-Regional Inducer of Immunogenic Cell Death in Hepatocellular Carcinoma: Implications for Immunotherapy. J. Immunother. Cancer 2021, 9, e003311. [Google Scholar] [CrossRef]
- Liao, Y.; Wang, B.; Huang, Z.-L.; Shi, M.; Yu, X.-J.; Zheng, L.; Li, S.; Li, L. Increased Circulating Th17 Cells after Transarterial Chemoembolization Correlate with Improved Survival in Stage III Hepatocellular Carcinoma: A Prospective Study. PLoS ONE 2013, 8, e60444. [Google Scholar] [CrossRef] [Green Version]
- Guo, J.; Wang, S.; Han, Y.; Jia, Z.; Wang, R. Effects of Transarterial Chemoembolization on the Immunological Function of Patients with Hepatocellular Carcinoma. Oncol. Lett. 2021, 22, 554. [Google Scholar] [CrossRef]
- Greten, T.F.; Mauda-Havakuk, M.; Heinrich, B.; Korangy, F.; Wood, B.J. Combined Locoregional-Immunotherapy for Liver Cancer. J. Hepatol. 2019, 70, 999–1007. [Google Scholar] [CrossRef] [Green Version]
- Chew, V.; Lee, Y.H.; Pan, L.; Nasir, N.J.M.; Lim, C.J.; Chua, C.; Lai, L.; Hazirah, S.N.; Lim, T.K.H.; Goh, B.K.P.; et al. Immune Activation Underlies a Sustained Clinical Response to Yttrium-90 Radioembolisation in Hepatocellular Carcinoma. Gut 2019, 68, 335–346. [Google Scholar] [CrossRef]
- Haag, F.; Manikkam, A.; Kraft, D.; Bär, C.; Wilke, V.; Nowak, A.J.; Bertrand, J.; Omari, J.; Pech, M.; Gylstorff, S.; et al. Selective Internal Radiotherapy Changes the Immune Profiles of Extracellular Vesicles and Their Immune Origin in Patients with Inoperable Cholangiocarcinoma. Cells 2022, 11, 2309. [Google Scholar] [CrossRef] [PubMed]
- Kudo, M.; Ueshima, K.; Ikeda, M.; Torimura, T.; Tanabe, N.; Aikata, H.; Izumi, N.; Yamasaki, T.; Nojiri, S.; Hino, K.; et al. Randomised, Multicentre Prospective Trial of Transarterial Chemoembolisation (TACE) plus Sorafenib as Compared with TACE Alone in Patients with Hepatocellular Carcinoma: TACTICS Trial. Gut 2020, 69, 1492–1501. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Zhao, W.; Wang, M.; Hu, J.; Wang, E.; Zhao, Y.; Liu, L. Transarterial Chemoembolization plus Sorafenib for the Management of Unresectable Hepatocellular Carcinoma: A Systematic Review and Meta-Analysis. BMC Gastroenterol. 2018, 18, 138. [Google Scholar] [CrossRef] [PubMed]
- Duffy, A.G.; Ulahannan, S.V.; Makorova-Rusher, O.; Rahma, O.; Wedemeyer, H.; Pratt, D.; Davis, J.L.; Hughes, M.S.; Heller, T.; ElGindi, M.; et al. Tremelimumab in Combination with Ablation in Patients with Advanced Hepatocellular Carcinoma. J. Hepatol. 2017, 66, 545–551. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cadamuro, M.; Fabris, L.; Zhang, X.; Strazzabosco, M. Tumor Microenvironment and Immunology of Cholangiocarcinoma. Hepatoma Res. 2022, 8, 11. [Google Scholar] [CrossRef]
- Qu, S.; Zhang, X.; Wu, Y.; Meng, Y.; Pan, H.; Fang, Q.; Hu, L.; Zhang, J.; Wang, R.; Wei, L.; et al. Efficacy and Safety of TACE Combined with Lenvatinib Plus PD-1 Inhibitors Compared with TACE Alone for Unresectable Hepatocellular Carcinoma Patients: A Prospective Cohort Study. Front. Oncol. 2022, 12, 874473. [Google Scholar] [CrossRef]
- Muscari, F.; Maulat, C. Preoperative Alpha-Fetoprotein (AFP) in Hepatocellular Carcinoma (HCC): Is This 50-Year Biomarker Still up-to-Date? Transl. Gastroenterol. Hepatol. 2020, 5, 46. [Google Scholar] [CrossRef]
- Lee, J.S.; Chon, Y.E.; Kim, B.K.; Park, J.Y.; Kim, D.Y.; Ahn, S.H.; Han, K.-H.; Kang, W.; Choi, M.S.; Gwak, G.-Y.; et al. Prognostic Value of Alpha-Fetoprotein in Patients Who Achieve a Complete Response to Transarterial Chemoembolization for Hepatocellular Carcinoma. Yonsei Med. J. 2021, 62, 12. [Google Scholar] [CrossRef]
- Liu, L.; Zhao, Y.; Jia, J.; Chen, H.; Bai, W.; Yang, M.; Yin, Z.; He, C.; Zhang, L.; Guo, W.; et al. The Prognostic Value of Alpha-Fetoprotein Response for Advanced-Stage Hepatocellular Carcinoma Treated with Sorafenib Combined with Transarterial Chemoembolization. Sci. Rep. 2016, 6, 19851. [Google Scholar] [CrossRef] [Green Version]
- Chen, I.-H.; Hsu, C.-C.; Yong, C.-C.; Cheng, Y.-F.; Wang, C.-C.; Lin, C.-C.; Chen, C.-L. AFP Response to Locoregional Therapy Can Stratify the Risk of Tumor Recurrence in HCC Patients after Living Donor Liver Transplantation. Cancers 2023, 15, 1551. [Google Scholar] [CrossRef]
- Pavicevic, S.; Reichelt, S.; Uluk, D.; Lurje, I.; Engelmann, C.; Modest, D.P.; Pelzer, U.; Krenzien, F.; Raschzok, N.; Benzing, C.; et al. Prognostic and Predictive Molecular Markers in Cholangiocarcinoma. Cancers 2022, 14, 1026. [Google Scholar] [CrossRef]
- Tampaki, M.; Doumba, P.P.; Deutsch, M.; Koskinas, J. Circulating Biomarkers of Hepatocellular Carcinoma Response after Locoregional Treatments: New Insights. World J. Hepatol. 2015, 7, 1834–1842. [Google Scholar] [CrossRef] [PubMed]
- Criss, C.; Nagar, A.M.; Makary, M.S. Hepatocellular Carcinoma: State of the Art Diagnostic Imaging. World J. Radiol. 2023, 15, 56–68. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| iLRT Modality | Procedure Technique | Image Modality Utilized | HCC Clinical Indications | ICCA Clinical Indications |
|---|---|---|---|---|
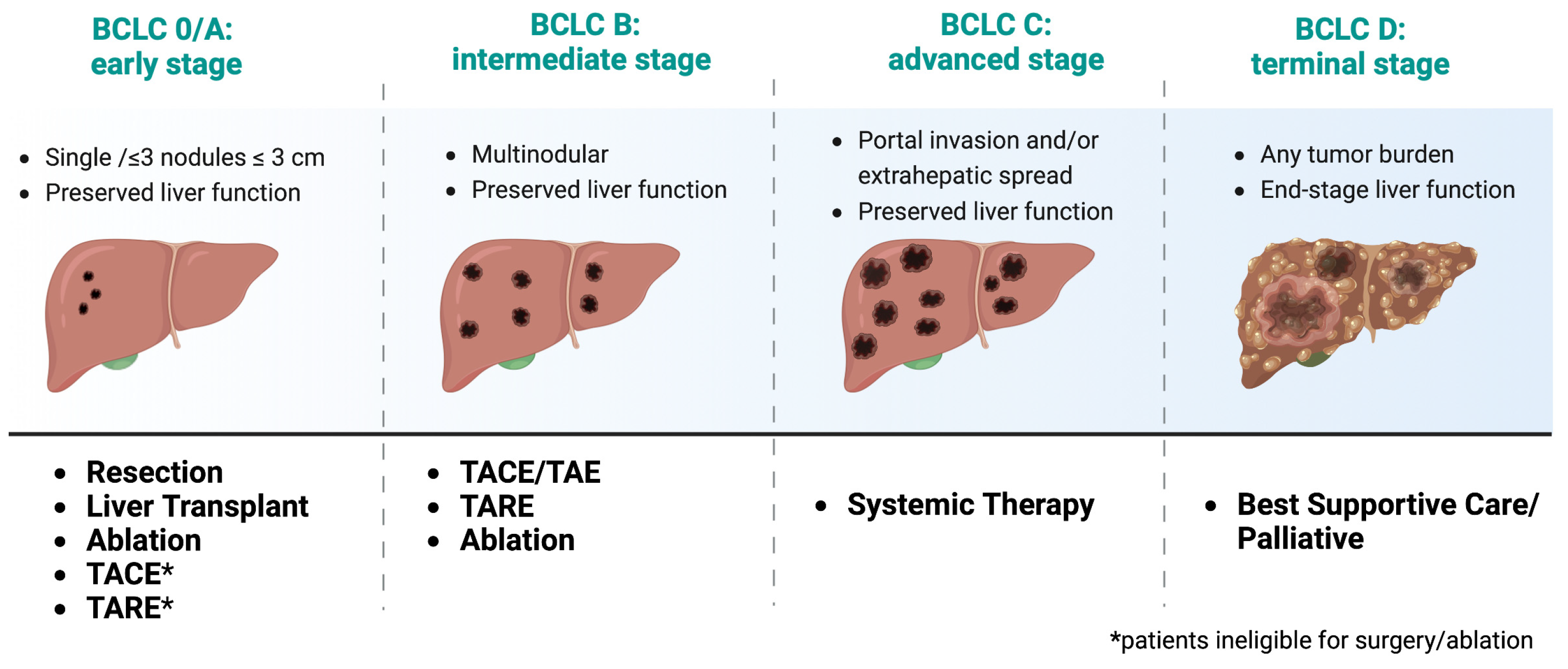
| Ablation | Percutaneous probe delivering high-frequency (RFA), microwave (MVA), cooling (Cryoablation), or chemical injection (PEI) directly to tumor cells. | Ultrasound or CT | Curative for non-surgical candidates with very early (BCLC-0) and early (BCLC-A) stage [18] | Bridging/downgrading and palliative for unresectable ICCA (stage III-IV) [35,36] |
| TACE | Catheter-driven chemotherapy (e.g., doxorubicin), embolic agent and, contrast directly to tumor-feeding vessels. | Angiography | Bridging/downgrading and disease control for early (BCLC-A) and Intermediate (BCLC-B) stage [18] | Bridging/downgrading and palliative for unresectable ICCA (stage III-IV) [35,36] |
| TARE | Catheter-driven microspheres loaded with Yttrium-90 labeled isotopes that emit β-radiation to tumor-feeding vessels | Angiography | Early (BCLC-A) and Intermediate (BCLC-B) stage [18] | Disease control, Bridging/downgrading and palliative for unresectable ICCA (stage III-IV) [35,36] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Criss, C.R.; Makary, M.S. Recent Advances in Image-Guided Locoregional Therapies for Primary Liver Tumors. Biology 2023, 12, 999. https://doi.org/10.3390/biology12070999
Criss CR, Makary MS. Recent Advances in Image-Guided Locoregional Therapies for Primary Liver Tumors. Biology. 2023; 12(7):999. https://doi.org/10.3390/biology12070999
Chicago/Turabian StyleCriss, Cody R., and Mina S. Makary. 2023. "Recent Advances in Image-Guided Locoregional Therapies for Primary Liver Tumors" Biology 12, no. 7: 999. https://doi.org/10.3390/biology12070999
APA StyleCriss, C. R., & Makary, M. S. (2023). Recent Advances in Image-Guided Locoregional Therapies for Primary Liver Tumors. Biology, 12(7), 999. https://doi.org/10.3390/biology12070999