Abstract
As pioneers in this field, our role in shaping the future of serious games in healthcare logistics is crucial. Digital media design significantly influences the quality of gaming simulation studies in healthcare. The leading challenge scholars face is introducing innovative and valuable features to university students. The data–simulation–gaming pyramid could serve as a blueprint for outlining how interactive simulations could be conducted. A participatory design process is important in serious game development. More recently, the literature has illustrated the contribution of extended reality. However, researchers have not explored this research framework in detail. This paper traces the participatory design process of serious games using an emergency logistics case study in Stockholm, Sweden. It underscores the importance of choosing the correct narratives and game mechanics to support the implementation of serious games using extended reality for the demonstration of non-technical skills. The research findings are threefold. (1) The participatory design process helps to place focus on the implementing philosophy that values health equality in networked hospitals. (2) Further analysis reveals that gamification could turn everyday tasks in the emergency department, which represents a stressful workplace in a hospital, into a spectrum of learning experiences for in-demand skills, including situational awareness, leadership, communication, and ethical thinking. (3) A closer inspection of the reality-changing methods shows new requirements to shorten patient queues before and after the (implementation of the) strengthened waiting time guarantee proposal in 2024. There is abundant room for principals in healthcare institutions to implement reality-changing methods to foster collaboration at the departmental, cross-departmental, and cross-institutional levels.
1. Introduction
Emergency care awareness emerges from the interplay among health equity, policies, and technological adoption within resource allocation systems used to allocate patients between areas of the facility in settings with limited material assets, and this awareness needs to be strengthened using campaign strategies to increase the accessibility and utilization of medical services [1]. Emergency departments are evolving into a socio-technical system characterized by interconnected components catering to the diverse needs of patients. Resource planning and management for problematic situations to realize improved teamwork performance based on cognition and interpersonal behaviors was pursued based on the introduction of crisis resource management principles in the aviation industry [2] and was implemented using various technologies, such as computer-based programs [3], in situ simulation [4], and serious games among university students [5].
Emergency department planning and management have been the subject of extensive research efforts in systems science. In the first two decades of the 21st century, an increasing number of studies have examined system-level design issues within hospitals using analytical methods. Previous studies have presented a thorough summary of application-oriented studies of models, using scenarios to describe resource parameters in the context of public health preparedness [6]. Although these studies contribute to a better understanding of the modeling and simulation techniques for emergency departments, there is a lack of experience regarding how in-depth participatory design tools, e.g., serious games, could prepare university students with an integrative body of knowledge and expertise. For a long time, non-technical skills training has been central to managers’ efforts to prevent the majority of accidents in educational research development [7]. The constellation empirically identifies communication, teamwork, challenging seniority, and decision making as the most common individual attributes in emergency management [8].
In recent years, emergency department administrators have encountered more and more service delivery requirements [9,10]. This calls for managers to not only stay informed about the human dimension of the institution but also to pay attention to the performance indicators related to waiting time [11], ‘left without being seen’ rates [12], resource utilization, and patient satisfaction [13]. In order to highlight the ability of emergency care professionals to control new situations and productivity issues they might face when continuously exposed to significant levels of stress and uncertainty, this article defines intangible skills as the personal quality of recognizing the broader societal and cultural aspects of the interaction between patients and the medical system in a low-resource setting; these skills are becoming increasingly critical to acknowledge the broader societal and cultural aspects of product development due to customer demands [14]. Understanding how games and their mechanics have been effectively structured can be useful in prioritizing the efficient delivery of care and assessing whether user engagement helps to achieve the intended learning outcomes.
From a practical viewpoint, serious games do not only rely on the quality of the extended reality devices given that the architecture, visualization, and reward system also require integrating utilitarian and hedonic elements given the limited effort and resources stakeholders may dispose. Nevertheless, gaming analytics are based on the outcome of interactions among a large number of learners who pursue their experience in the virtual environment. A diverse group of actors specializing in complementary knowledge domains, digital narratives, and scenarios that influence university student behavior over time, and the scale representation of the reference system, all play a crucial role in how extended reality devices for medical applications translate knowledge into reality.
The management and planning of resources, along with the exchange of information among university students to support patient handover, can also be facilitated through learning tasks in extended reality technology, either by co-creating the prototype or offering ready-to-use design features. In recent years, co-creating serious games has emerged as a viable alternative for healthcare institutions, particularly when the core gameplay mechanics evolves from a collaborative design process. Therefore, participatory design is deployed in this study; however, this does not necessarily indicate exclusive reliance on the involvement of multiple stakeholders in perspective-taking workshops.
Serious games in the extended reality enable stakeholders to interact with digital and physical objects simultaneously. They are intuitive and context-aware, with effective design features facilitating collective innovation. However, researchers have not explored their research frameworks in detail. To address this knowledge gap, this study aims to provide methodological insights into the design process and evaluation outcomes of serious games, drawing on the lessons from an emergency logistics case study in Stockholm, Sweden. The objective of this study is to qualitatively analyze the outcome of serious gaming as a reality-changing method for improving emergency logistics in networked hospitals, reflecting the unique characteristics of patient flow, particularly for handling the critically ill during a full working day as well as university students’ acquisition of intangible skills based on user feedback. The key contributions of the study include the following:
- Revealing the process of gamifying a module-based emergency department driven by interactions with personnel during the staff shifts of a typical working day;
- Investigating how design considerations and participatory engagement based on user feedback change across sessions and according to modalities;
- Using design features to establish connections among the layers of data, simulation, and gaming in the previous research framework to translate the complex details of a healthcare institution into a demonstrative space of intangible skills;
- Discussing the updated research framework, which includes new layers of patient flow data, extended reality simulation, contextual serious gaming, the strengths and pitfalls in the design process, and their relationship for further implementation of gameplay mechanics, such as areas of influence and deck-building strategies.
The synthesis of the case study provides, for the first time, to the best of the authors’ knowledge, a first-hand account of the use of a reality-changing method for improving emergency logistics while upholding top-notch standards of quality and safety. The remainder of this paper is structured as follows. The next section examines the literature on the principles of emergency care provision and the backbones of healthcare systems. Section 3 describes the methodology and the Stockholm study. The research findings are presented in Section 4, and a discussion is provided in Section 5. Section 6 concludes with the study’s ramifications and future research avenues.
2. Literature Review
Managers and researchers have shown a longstanding interest in the quality and safety of emergency logistics, with a special focus on the performance of emergency departments. Although interactive approaches such as reality-changing methods have been employed to recognize the central position of workers, recent studies have started to explore the internal processes within departments in addition to the medical and mental conditions of patients. This is largely driven by advancements in game sciences [15], which have offered researchers a springboard with strong theoretical foundations in design science for testing new artifacts. This section describes the literature on the principles of emergency care provision, healthcare system design, and gaming.
Healthcare system engineers refer to a wide range of models to describe institutions regarding the efficiency and effectiveness of resource allocations. These models are developed from computer simulation packages with no direct human involvement during the runtime [16]. Such techniques help investigate the capacity bottlenecks of a hospital facility rather than the complexity amongst design aspects, and they usually undergo verification and validation procedures based on explicit numerical values to predict performance [17]. Another area of research for healthcare stakeholders is to explore serious games with medical benefits and to perform a discourse analysis on a chosen topic at the institutional level. Although these research findings shed light on the digitalization of complex details and inspire meaningful discussions on how collective innovation are deemed important, the tentative presentation of data and rules and the visual appearance of many computerized programs barely describe the multi-faced segment of emergency logistic systems.
The emergence of game science theory points to a brand-new field of study that aims to advance domain-specific knowledge using extended reality games as the basis for experimental investigations. The success of game science research relies on iteratively executing a constellation of activities, including media development, implementation, evaluation, and debriefing. There is an expanding body of scholarly research that extends the paradigm to radically change the methods used to address capacity-building issues in sectors such as manufacturing [18], transport [19], business [20], occupational health [21], and higher education [22]. To experimentally navigate the adoption of reality-changing methods, real-world systems are usually digitalized with gamification elements, and sessions should target a better understanding of the role of immersive technology.
Based on research into the design process of serious games, there are several commonly used proposals emphasizing the design aspect of production or service delivery. The process uses norms required for various concerns across sectors, but the final presentation is always mediated by the user experience. According to the literature, serious games used to raise awareness of local issues are commonly co-designed. These examples include ‘Energy Safari’ for the innovative governance paradigm toward sustainable societies [23] and ‘Dynamix’ for livestock integration among farms [24]. The co-creation of serious games refers to a wider range of collaborative activities to enable value production alongside stakeholders. Although co-design has been frequently used for the presentation of scenarios when planning spatial systems (i.e., the game could be transferred into a decision support system with the exchange between university students reaching a level of self-efficacy that cannot be achieved in real-world systems), co-creation has been proven to transform innovative ideas from outside actors into the manifestation of built-in materials (i.e., with the help of an involvement matrix to establish the degree of participation) [25].
Several studies have been conducted to compare the novel designs of serious games in the wake of behavioral analysis. Researchers provide immersive environments based on delivery room situations to simulate the dialog and activities found in obstetric situations [26]. University student behaviors during escalating circumstances were elicited based on a first-person shooter game [27] and open-world game concepts [28]. The former study analyzed gameplay actions stemming from the triadic interaction of scenarios, signage, and level design.
Within the scope of hospital emergency departments, serious games have been less frequently employed to explore innovative forms of teamwork in the face of challenges such as demand surges, time limitations, or resource constraints. The utility of these games was evident in several contexts, including the Friday Night at the Emergency Room tabletop suite at multiple American academic centers [29], operating room simulations [30], the improvement of cognitive screening abilities in Canadian institutions [31], and the integration of high-fidelity graphics and advanced user interface designs to represent the well-functioning workflows in the German medical context [32]. In their research, Zhang et al. enhanced the design study of serious games by comparing the impact of modality on effectiveness using board and digital games [33]. The results demonstrated that better performance in absorbing demand uncertainty in emergency logistics depends on the acquisition of skills and the development of a systems thinking mindset over time. Addressing real-world ‘wicked problems’, which are often difficult to solve using analytical approaches [34], always requires creative efforts. This will help lift an innovation culture in emergency care to pursue resilience in an ever-changing landscape among networked service providers.
2.1. Tabletop Exercises and Extended Reality Devices in Managing Hospitals
Managing hospitals is becoming an increasingly interesting subject of systems research, especially regarding participatory methods. It is, therefore, worthwhile to examine the literature from an application-oriented perspective, describe the games, and analyze their characteristics to determine the generalizability of research findings. This study performed a literature search to identify top-tier articles indexed by the Web of Science Core Collection. A comprehensive query consisting of all research terms was defined as ‘(TS = (hospital) OR (TI = (emergency) OR TS = (ER))) AND (TS = (game) OR TI = (serious game) OR TI = (gaming) OR TI = (table SAME top))’ for the search engine. This search was applied to the Science Citation Index, Social Science Citation Index, and Arts & Humanities Citation Index databases from 1990 until the present. Following this, abstracts, book reviews, and items without full access were excluded. The procedure ultimately identified twelve representative articles bridging both perspectives on management and learning.
As can be seen from the collection of studies, Kraus et al.’s literature review was the only report summarizing the best practices in the last decade of the 20th century [35]. According to the authors, a handful of studies have addressed emergency planning issues based on standalone computerized simulations with interfaces. Apart from performing these drill exercises, there was a lack of collaborative learning processes to execute department-wide management elements, support complex decision making, and, in particular, form interdependencies across the institution. In light of this, research into important capability building has presented findings from discussion-based game activities, i.e., tabletop exercises or extended reality devices. Fusco et al. utilized Friday Night at the ER as the prototype toolbox for students in health profession programs to learn emergency management principles with formal evaluations of performance indicators, i.e., systems thinking scores and self-perceived proficiency [36]. Its popularity is evidenced by the inculcation of interprofessional collaborative practice competencies consisting of an educational game [37], the gamified scenario of managing a busy hospital on a daily basis, the user-friendly design, and the configuration based on a universally applicable triage system. All of the aforementioned characteristics were found in this popular gaming suite, which not only serves as a metaphor for the complexity of industrial systems, in general, but also provides new possibilities for new health profession students to optimize healthcare outcomes in a multi-choice environment.
Past work on extended reality has approached the context of the capacity-building process by managing emergency cases. Based on user–system interaction data obtained from working with the serious game, Chon et al. reported enhanced procedural knowledge of medical students and the general control of the emergency department by visualizing the patient inflow from the physician, the dispatching process, the patient’s medical history, and the establishment of diagnosis and treatment [38]. The research findings led to discussions on the perceived usability of digitalized medical content as an important precursor for motivated learning and the knowledge gain attributable to the game itself. Nicolaidou et al. proposed Virtual Emergency TeleMedicine for training doctors, nurses, and medical students during encounters in clinical scenarios, bridging the knowledge gap regarding the effects of including virtual patients in medical education [39]. Tong et al. created and implemented a serious game to evaluate self-administered tools during routine assessments [40]. This game was designed to expedite patient information flow in busy environments, i.e., emergency rooms. In summary, previous studies on extended reality applications have focused on the presentation of patient tasks and their progress toward the decision points. These efforts utilized statistical models to analyze behavioral pattern changes before and after the intervention; however, little is known about the impact of media design as experienced by university students.
2.2. Hospital Management in Sweden: Overview and Local Incident Control
In Stockholm, a total of six key initiatives have been identified for pediatric care. At the regional level, there is a proposal to extend opening hours at the Solna outpatient clinic to avoid a large flow of patients to medical centers in the evening. In addition, the council called for a uniform triage manual with clear criteria as a decision support tool for referral to the correct level of care. Missions in surgery and orthopedics are expected to expand so that recipients can prepare investment, training, implementation plan, etc. For Karolinska University Hospital, increased search clarity is required for the Solna area, where, currently, many individuals make mistakes that lead to a high proportion of referrals. The Information and Technology department further developed data systems that enable the follow-up of flows from referral via emergency visits to inpatient care to control the correct way forward. Finally, hospital employees have expanded the use of advanced care for children in their homes both in terms of geographical coverage and new patient groups. By building on its existing strengths, ranging from coordinating patient flows to systems design considerations with inclusivity, the city of Stockholm can model scalable solutions for global healthcare systems.
Hospital management in Sweden features patient flow optimization across several arrival types. Patient arrival types include walk-ins, healthcare center visitors, neighborhood clinic users, individuals seeking medical counseling, and those not referred. Karolinska University Hospital, as the top medical center in Stockholm County, is responsible for highly specialized healthcare covering the most complex disorders and critically ill patients [41]. Many providers assign a high proportion of formal referrals, and this organization of care experiences large seasonal changes in emergency visits, driving variations in inpatient needs, capacity, and utilization at the head of the structure. In addition, almost half of the extensive hospital stays occur between 20:00 and 24:00, when the neighborhood clinic begins to prepare for closure. Nevertheless, a record number of patients waited longer than promised in 2024. Addressing overcrowding issues calls for stronger local control, clearer communication, and a thinking process based on core system concepts developed by the Systems in Evaluation Topical Interest Group of the American Evaluation Association without compromising the accessibility of emergency care in line with the patient’s expectations.
There has been an increase in patient inflow during the past few years. According to the official registry, the number of arrivals in pediatric emergency departments is expected to increase by greater than 10%. Crowding introduces operational challenges ranging from productivity drops due to work-related chronic stress [42] to excessive length of stays [43]. In recent years, bed shortages have been observed in certain seasons [44]. In order to reduce the bottlenecks at the hospitals, the regional county council and the institution work together to propose key initiatives as outlined in the ‘Future Medical Plans’. The county council worked on extending the opening hours of the neighborhood clinic to avoid a large flow of patients in the evening, standardizing decision support tools for recommendations to the correct level of care, and expanding surgical operations. On the other hand, hospitals aim for increased search clarity in the catchment area and the expanded use of the ‘advanced care of children in their homes’ package, both in terms of geographical coverage and new patient groups.
The acuity assignment applies the five-level triage framework uniformly implemented in the Swedish medical services [45]. An overall coordination structure is in place for moving sick infants elsewhere so that the most advanced facility can receive the smallest children that are most sick at Karolinska University Hospital (ALB-S). However, from the manager’s perspective, these units, which are located in different sites in the Solna, Danderyd, and Huddinge communities, exhibit a networked infrastructure with micro-systems that are capable of meeting specialized care demands, whereas most professionals are currently optimizing the patient flow using a bottom-up administrative approach rather than an approach based on an overview of the functional areas. The neonatal patients are held as long as needed in the specialized ward, and the birth clinic is responsible for these patients during the first week. Moreover, during that first week, the normal course of action is to visit the emergency department if an infection, a contagious disease, or a similar event occurs.
Awareness that the headquarters is no longer the sole provider of orthopedic and surgical care, with patients increasingly seeking closer proximity in the future, broadens pathways for meeting the need for all levels of government, nongovernmental organizations, and the private sector to work together to prevent, protect against, mitigate, respond to, and recover from incidents, as pointed out by the Federal Emergency Management Agency, Washington, D.C., USA [46]. Incorporating this dynamic is considered an important aspect of creating a game for resource allocation, helping staff members connect their everyday work and effectively balance patient inflow demands with individual competence.
2.3. Synthesis
Although game science theory is increasingly applied to case studies where critical appraisals are given by stakeholders, many of these attempts are made without considering the nuanced complexities of how university students engage with context-based information. As such, serious games from other fields make limited connections to the dynamics of the healthcare system and, therefore, lack the immediacy and spontaneity for a thought-provoking perspective. Interestingly, almost no studies have investigated co-created possibilities with experts and stakeholders (e.g., game designers, doctors, or system engineers) to describe an emergency department as a demonstrative theater promoting the acquisition of intangible skills. An investigation based on the heuristic evaluation of serious games thus falls more in line with routine practices exercised in particular domains, calling into question the usefulness and generalizability of reported outcomes, such as behavioral endurance (the ability to persist in activities despite fatigue, discomfort, or other barriers), procedural adherence (the execution of activities against defined standards), and expert–novice performance differences (the examination of advanced metrics focusing on changes in trials). Rezvani and Khabiri [47], for the first time, reviewed the social computing methods of gamers to identify behavioral deviations. The synthesis of articles categorized previous studies into five broad classes, suggesting future lines of research in behavioral science. In another article, Rahimabad and Rezvani investigated all the underlying factors affecting immersion and concentration in serious gameplay [48]. Structural analysis revealed that the reality-changing method and the incorporation of unexpended challenges were the most important aspects.
According to the literature, the challenge in generalizing the relevant research findings from game-based studies might be linked to the limited use of collaborative, adaptive, and rigorous research frameworks in the design process for achieving targeted objectives [49]. The adaptation of and potential further developments on the existing structure present an opportunity to address the design complexity problem in serious games [50]. Detailed procedures for documenting the spread of complexity across different phases of the design process are available. The documentation of project meetings, including the verbal and written exchange of ideas throughout each phase, could be reviewed for consistency, and this method was used to enhance knowledge of the emergency logistics system in Stockholm, Sweden.
3. Methodology
As communication and cultural study scholars have concluded, “the co-design process of the storytelling game is carried out to establish the grounds for the narrative and game experience” [51]. A method to facilitate the comprehension of multiple skills and respond to the surroundings appropriately involves the use of emergency department simulations [52]. In their studies, the simulation as part of the collaborative program between the medicine and strategy domains offered hyper-realistic scenarios for the development of competencies. Furthermore, participation necessitated a strong sense of interdisciplinarity and a pluralistic outlook from the players for the system’s beneficiaries [53], in this case, the patients. This led to the introduction of a reality-changing method to specify the resources that were necessary for the relevance of the game. A crucial aspect of the game was adhering to the institutional standards linked with emergency logistics. It is prioritized to demonstrate to students that healthcare workplaces aim to create an ideal patient journey, with shared responsibility for preventing inflow bottlenecks. For example, in Sweden, half of the patients at the hospital in 2016 waited for almost two hours before seeing a doctor.
The game was created to immerse university students in live action and to demonstrate how the emergency department could operate in the face of substantial uncertainty regarding patient inflow. To achieve this, the design process started with traditional board game elements. Previous applications included the creation of board games for research [54] or modified versions of well-established games, like Monopoly. These games became a sustained metaphor for socially conscious participation. Its appeal originated from the opportunity to be creative [55], and it subsequently became one of the most famous cultural products of this century [56]. In light of this similar thread to depict randomness in healthcare and encourage players to exercise resource allocation to significantly impact the ever-changing dynamics of the healthcare system, the author compressed the spatial system using low-poly items to enable resource deployment, binding text to the patient profiles to assemble the overall narrative, and polishing event cards to describe the situational challenges.
To take care of the critically ill, the emergency department implements a triage and distribution framework from a need-based perspective. Following this, patients will be conveyed to various modules supervised by teamwork-oriented, leading nurses. Rider et al. summarized that marshaling the skills and intangible assets possessed by the institution is fundamental to high-quality healthcare [57]. Through the behaviors and attitudes of the leading nurses, university students in serious games were exposed to the attributes of the quality of care necessary to work and interact within the accountability framework. Such a form of interactivity, together with university students’ physical presence, replicated the ontology of the social–technical system, highlighting the parallels between role-play and those of the theater [58] and, in the case of this research, offering real-time insight into the nature of the intangible skills. By immersing themselves in imaginary situations, as presented in Figure 1, university students were expected to comprehend what interprofessional capacity building consisted of and to anticipate a broader vision of the leading nurse.
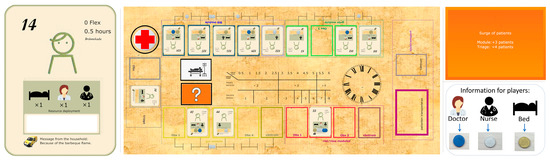
Figure 1.
An illustration of the toolkit. (Left): one of 127 patient cards with different profiles; (Middle): the board; (Right-top): one of 16 event cards; (Right-bottom): the information card.
The authors customized game elements to symbolize the ever-changing dynamics of emergency care provision. These visual and written accounts facilitate affective engagement through a sense of curiosity, content richness, and the willingness to explore. By virtue of the flexibility given to the actors with a fairly thorough representation of the technical system, the toolkit as a whole serves as a gaming instrument rather than a pure simulation of the healthcare system. As Donovan summarized, “wherever the future takes us, board games will be there, mirroring our choices and our attitudes on paper and cardboard” [56]. The analog materials boosted engagement by visualizing the impact of negotiated gameplay on the reduction in department-wide overcrowding, in general, and queue lengths for each module in particular; university students’ feedback indicated that the switch from a fast-paced working environment into a therapeutic atmosphere made it easy for them to stay focused on their bodies and minds. It is important for the game to involve stakeholders from multiple domains with diverse insights. Prior to the release of build materials, the reality-changing method sought, through perspective-taking activities, concrete advice from experts in residence in the fields of sociology, extended reality, systems engineering, and emergency medicine. Such an integration of research knowledge and design experience provided another possibility to situate oneself in the position of the recipients, as pointed out by the literature [59]. In addition, the principal consulted previous design outcomes of gaming simulations in urban systems. This helped to develop a media style that would allow university students to explore multiple contextual layers, i.e., layouts, scenes, and maps. These features inspired the development of the digital version and the subsequent comparison of modality impacts, as presented in Figure 2.
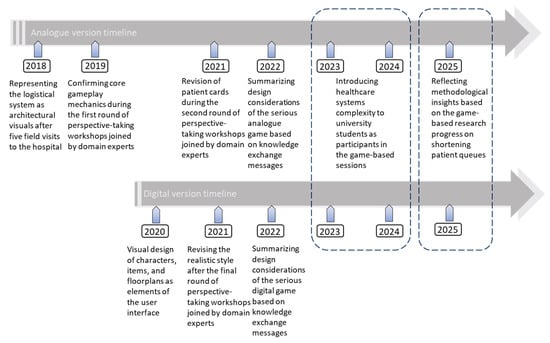
Figure 2.
The research progress of deploying serious games as the catalyst to address complexity issues in the healthcare logistics system. (Dot line): the implementation of game-based sessions.
The game was realized through prototyping. Instead of progressing through the variations in the pursuit of the final form of the instrument, the author documented the different versions in detail to understand how to meaningfully choose gameplay mechanics and design features. The first version was reviewed by experts in residence during perspective-taking workshops and by university students new to emergency logistics. As an example, the university students found that more textual elaborations on the patient inflow would assist the resource allocations and staff rotations under various constraints without interrupting the practice of intangible skills; they preferred intertwining factual information on the card deck to facilitate ‘production in pawl’ rather than relying on the constellation of event cards to experience the unexpected. After this, card decks and certain rules were updated based on the feedback, evaluation outcomes, and observations of the principal.
Figure 3 presents a data flow chart for the case study. University students found it interesting to make a series of meaningful decisions when undergoing patient tasks; therefore, additional spaces were added to the cards to keep track of the arrival and completion times separately. The game was initially developed to illustrate the consequences of delays in monetary values. Later on, the bill’s appearance was criticized by the experts since it encouraged cash chasing and subsequently distorted the climate of the leading nurses; therefore, it was replaced by tokens. Another important factor was genre selection for the digital version. The game objects initially utilized older-looking models from isometric camera views that are popular in video games such as Theme Hospital, SimCity [60], and the Sims series [61]. Such top-down simulation games allow the implementation of changes for city-wide prosperity. This was found too broad, as their gameplay was encountered at the macro-scale and barely illustrated the coordination between service providers. The digital version of the serious game evolved into an open-world style with a smooth blend of realism and retro-inspired items, decorations, and furniture in hospitals to recreate the environment inside the emergency department.
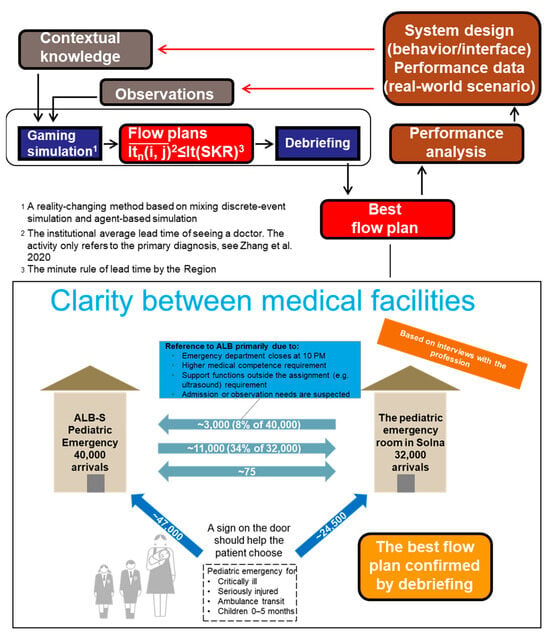
Figure 3.
Data flow chart for the case study steered by the emergency care organization in Stockholm, Sweden [62].
The prototyping efforts helped elucidate the flow experiences caused by the modalities. This evaluation was based on participant feedback. Remarkably, analog materials were associated with a high level of engagement, with everybody’s high recognition of peer contributions; however, university students were not eager to share extra possibilities during the night shifts. In contrast, as the game progressed, the dynamics in the digital version of the serious game prompted more conversations. The university students could apply their newfound understanding of the working environment to reality. The freedom of open-world exploration is therefore considered a much-needed venue for connecting people rather than a distraction from achieving the intended gaming outcomes.
4. Research Findings
4.1. Design Considerations
For university students who seek to effectively plan and manage the emergency department, the game needs to feature the underlying proponents of the reference system. Previously, this knowledge gap was addressed through the lens of systems modeling, realistic simulation, and additional experimentation to resolve capacity issues within healthcare institutions. Meanwhile, in terms of acquiring intangible skills, there is a need to strengthen bonds between university students and the extended reality; this is currently possible through a more prevalent adoption and integration of design features to increase situational awareness. This was made possible by two games, one using AnyLogic and the other using the Unity game engine.
The single-player game was built to galvanize user input on whether it is appropriate to visualize patient flows, built environments, items, and performance indicators with instant feedback. Such integrated development tools have already been used to develop management simulations with user interfaces [63]. Therefore, the technical implementation should not distort the design process and evaluation outcome of a serious game.
Using the Unity game engine, a first-person multiplayer capability was added to stimulate communications and decision making among university students. The game designers incorporated lessons from previous iterations to push the boundaries of what is possible to gamify. As a result, the designers incorporated the patient duties and background information as a digital narrative, representing a new design idea attempted by the multiplayer online game to illustrate the realistic yet ethical aspects of the working environment. By conversing with non-player characters, the university students were given the opportunity to virtually experience the emergency room during the sessions, determining additional information about the patient’s circumstances. This game was considered open-form since the university students took on the role of senior nurses in charge of the logistical aspects of emergency care.
Utilizing the script component associated with each non-player character, the patient arrival time, task durations, and necessary resources to complete their journeys were integrated to instantiate Unity objects. The game switched into a freely traversable world on top of a quest system, adhering to a rigid structure. This allowed university students to stride toward the completion of clinical pathways rather than generally exploring the places of the hospital. The university students can monitor the availability of resources and distribute them properly to ensure the best performance of the emergency department. These processes provide opportunities to exercise communications in a short amount of time, leading to a better understanding of the patient mix as well as an overview of the resource utilization levels for each module. Since the university students selected the role of a floor manager with the aim of efficiently organizing patient flows amidst high-stake situations, they were aware of the responsibilities but were also given the chance to approach the broader structure of a healthcare institution. This part of the game is considered free-form.
The behaviors occurring throughout the gameplay sessions were recorded using the input–output system as one interacted with objects and made decisions related to the delivery of care, producing log data with disclosures of planning, management, and the occurrence of learning activities. A constructive debriefing session was organized between personnel shifts to address system-level issues and highlight performance gaps encountered during teamwork. The entire gameplay session was followed using already established questionnaires to gather university students’ feedback pertaining to the experience, usability, and confidence of playing. The remarks by university students served as the foundation for the ad hoc evaluation of outcomes using analytical methods. Previous studies deployed structural equation modeling to explore the relationships among gameplay factors [64]. To better understand the persuasive impact of design practices, the deployment of analytical methods can also include the formulation and testing of multivariate regression models, behavioral transition matrixes, or cross-session hypotheses.
To acquire intangible skills from playing the game, the game sessions showcased university students’ preferences for the manifestation of reality in the context, service delivery, and institutional structure of emergency care. In addition, when navigating the configuration of spaces and locations in full detail, they would rather interact with the ready-made objects in a visually appealing format to adhere to the intended outcomes drafted by the designers. The additional symbolic level imposed on the everyday items in healthcare enhanced the environment’s authenticity. One contribution of serious games involves providing a learning experience that prepares individuals for scenarios and translates innovations along with knowledge pertaining to emergency medicine.
To portray the social dynamics between agencies, it is important to recognize that the game, which occurs in the multidisciplinary field of emergency medicine and typically focuses on resource planning and management, needs to enhance the university students’ willingness to collaborate in the workplace. We observe that digital games like Theme Hospital and others prioritize ludicrous aspects. In contrast, first-person games are commonly used for surgical training [65]. As opposed to these applications, research shows that games for patient handover should not be built beyond the norms, and the institutional conventions should remain largely unchanged, serving as building blocks for future-proof teamwork that will be applicable to patient inflow fluctuations, uncertainty, and complexity.
4.2. Digital Serious Game with an Analog Version or Vise Versa?
The level of engagement, flexibility, and user experiences during playtime are taken into account while determining the form of gaming the participant will participate in. This is made possible by the empirical study of developing and evaluating the digital and board game based on the modeling of the same system, with results suggesting that the latter modality facilitated more in-depth discussions. To keep the university students well informed through a simplified version of the reference system, the analog materials need to adopt design features with front-loaded remarks, leading to noticeable differences in visual presentation compared to their digital counterparts. The board game showed flexibility and capabilities in executing subsequent tasks:
- The nurse or the doctor would go to the room and complete the tasks. If the patient required minor care, the nurse or doctor would stay there.
- The patients would be taken to the emergency room, where the facility deployed resources accordingly. This occurred if the patients were thought to be unstable based on unstable vital parameters.
- The patients would go directly to the emergency room, where a nurse would register the patients into the system if they were really sick.
Serious games have been designed with an educational purpose and are increasingly applied for the generation of user profiles. However, to integrate knowledge with design solutions, the digital media should define the reference system using epistemology. A strong case can be made for the growing application of board games in formal settings. In fact, in many cases, the act of strategically moving pieces around a table has evolved into a standalone design practice.
At present, there are no so-called ‘one-size-fits-all’ design solutions for healthcare systems because the creation of gaming materials should always take user preferences into account. Professionals on the front lines anticipated more in-depth discussions on quality and safety concerns in emergency treatment. As was noted throughout the game assessment process, university students better received this message while playing with analog materials. This is due to the fact that board games make it easy to identify capacity bottlenecks from the array of details. University students were offered clear paths to explore various resource management and planning strategies, understand the enduring impact of decision making, and collectively provide novel ideas through much more imaginative use of artifacts. Although the principal might find university students preoccupied when they delved into the mechanics, they navigated such a gamified environment while having fewer direct conflicts with one other. This again helps to elicit intangible skills from the ever-changing dynamics of the working environment. Rather than being standalone applications, the modalities contemplate each other and become a research tool for better design of serious games, in general, and the reference system in particular.
4.3. Engagement
When new thoughts or solutions are formed during gameplay, the documentation of the user-generated content is necessary for evaluation purposes as well as to inform the university students, particularly at debriefing sessions. Game analytics are used in this encounter to visualize data and characterize user profiles. To understand the experience and learning effects of games, it is common practice to combine questionnaires, interviews and formal assessments as a means of data collection. These techniques are still lacking, with the exception of validations based on multiplayer board games; therefore, this research direction may be explored in the future. In addition to quantitative methods, discourse analysis and ethnography studies could be performed to uncover naturally occurring communications that build on each participant’s agency. If correctly recorded, the transition of their game-related behaviors might reveal underlying cognitive and emotional processes. For interpreting the results, however, knowledge mapping and information visualizations are used as keywords. A rigorous methodology of evaluating the game’s effects is required, both during gameplay and at debriefing sessions.
This study found that design features openly and appropriately showcasing the reference system would trigger the university students’ navigation of the virtual environment. To realize this, the serious game has to develop from a player-centered perspective together with a greater depth of content, a broader variety of gameplay elements, and built-in heuristics. Previous games that featured emerging design principles were successful in such endeavors [66]. This holds true for the creation of serious games based on complex systems. However, it is still impossible to completely digitize the complexity of socio-technical systems because doing so would not simulate the roles and agencies of stakeholders. In fact, it disregards access to meaningful choices made by the participant and excludes the playable aspect. It is interesting to learn about other design strategies, including the distinction between moments of high activity and time-outs [67], to involve the player in the cross-domain knowledge production space.
The game is expected to effectively characterize the reference system so that university students can identify with and interpret the dynamics of the working environment. Historically, this requirement was approached through the lens of medical simulations, whereby high-fidelity and methodologically sound models were developed. Recent studies have shown that incorporating game design elements, such as narrative and visual esthetics, can also amplify participant engagement and help realize digital assets. From the perspective of the model acting as a facilitator in the creation of a design artifact, there are additional constraints arising from the context of usage. When building models for educational or training purposes, it is crucial to take into account both design features and realistic scenarios. This can ensure that the viewpoint of the serious game is effectively communicated to and received by the target audience.
4.4. Summary
As shown in the intersection area in Figure 4, the research findings from the serious game study could be organized around specified themes through the lens of systems engineering and disciplinary interaction integration. It is demonstrated that structured decomposition, participatory engagement, and purpose-driven digital media are critical to administering complex systems like networked hospitals. The findings underscore the methodological framework’s enduring relevance in addressing modern socio-technical challenges, provided this framework is augmented with iterative, human-centric instruments.
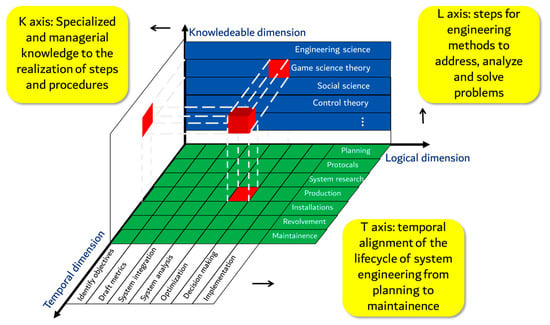
Figure 4.
Main research findings based on Hall’s Hard System Structure [68].
The serious game revealed that modular design (e.g., separating triage, bed allocation, and discharge processes) reduced bottlenecks. By simulating workflows as discrete subsystems, hospitals could independently optimize components, such as emergency triage algorithms, while maintaining interoperability. Real-time feedback mechanisms (e.g., dynamic bed-tracking dashboards) improved responsiveness to surges in patient demand. The game demonstrated that closed-loop systems based on predictive analytics adjusting bed allocations hourly reduced waiting times to around 30 min in gaming simulations. It is worthwhile to note that the game highlighted the need for standardized channels to synchronize patient records across institutions, reducing redundant tests and miscommunication.
The serious game, serving as a participatory instrument, advocates stakeholder involvement in problem definition and validation. Clinicians and administrators co-designed game scenarios, ensuring alignment with real-world constraints (e.g., staffing limits). This reduced resistance to implementation compared to top-down mandates. Players adopting roles, including leading nurses or bed managers, developed cross-functional empathy, leading to consensus regarding resource-sharing protocols (e.g., inter-hospital transfers during resource shortages). Finally, 3D serious games provided immersive, experiential learning, whereas discrete-event simulation platforms, e.g., Arena, were optimal for modeling patient flow as a sequence of admissions and discharges.
5. Discussion
The perspective-taking workshops revealed a change in focus amongst the participatory design process by highlighting rich descriptions of experience to strengthen bonds between the player and the avatar; in particular, the degree to which university students identified with avatars required customizations based on the frequently sought design features. Avatars have to support the embodiment manifestation with a gaming environment and, therefore, allow a higher-level conceptual appraisal of one’s agency. During the game-based scenarios, it never occurred to the teachers and educators that they would not contest each other’s expertise, as they were inexperienced in the relevant areas, as reported in previous studies [69]. Rather, the examination and criticism of certain gameplay mechanics judged inappropriate for use in healthcare finally resolved the challenge of designing serious games. This calls for a shift from the simulation of mundane tasks toward simulation-driven scenarios that must come with a procedural narrative and compelling characters, as outlined in the next paragraphs.
Simulation-driven scenarios imply the abstraction of as many nuanced complexities as possible from the reference system. In emergency care provision, the interplay of resource planning, management, and competency requirements affecting service delivery profoundly influences any treatment process. These requirements consist of a situational awareness of factual information (vital signs, diagnoses, and progress notes), the timely handling of a variety of patient feelings (relief, satisfaction, and depression), and workload adjustments in teamwork (keeping an eye open on the well-being of workers). Although speculating on the above-mentioned directions is not barred from activities in previous serious games, their contents are seldom delineated in a genuine and coherent manner. The proposed serious game allowed each participant to make their own choices for the sake of patients, leading to the formulation of a positive procedural narrative as an efficient catalyst for the acquisition of intangible skills. In either modality, the university students quickly discovered that, as is the case in reality, they had to remain consistent to be successful when planning and managing the emergency department.
In addition to a procedural narrative, a shift to simulation-driven scenarios is supported by a ubiquitous visual style. The standard display of characters in serious games was found to involve bodies, costumes, and ornamentations with respect to their real-world archetypes. These components should enable a wider range of expressions that broaden university students’ perceptions of personal traits such as commitment, humanity, and conscientiousness. These also represent areas for brand-new design features. The appreciation of game esthetics needs to be integrated into the subject matter, and it should be left to the university students to decide how long they will engage with ludic pleasures at their own discretion. The extended reality simulation supported a verisimilitude as the novel feature, which elevated agency to role-play.
The workshops revealed that manual placement and legacy were the most effective mechanics for maintaining ethics, situational awareness, leadership, and communication skills. Legacy needed multiple shifts to establish the overall plot of a serious game. As the game proceeded, a combination of new events, items, and profiles was brought in to displace their antecedent counterparts. The strategic and random potentials of the game offered university students a refreshing sense of growth. In addition, manual placement was a frequently observed but not a primarily used board game mechanic. However, its intuitiveness, operability, and simplicity contributed to the interaction between university students in the serious game. Typically, this interaction was contingent on the cardinal system, in which only a limited number of tokens could be placed at a given location at any one moment. As a result, university students must be aware of their choices to avoid resources from being unavailable or fully occupied. The perspective-taking workshops revealed that both versions of the serious game required designated objects, i.e., tokens and workstations, to represent the personal and the locations for placement, respectively. The standard process of manual placement involved the following steps:
- Participants take turns placing one or more tokens.
- Location effects, which might include the further accumulation of resources or points, are activated as part of the response.
- At the conclusion of a patient’s journey, tokens are reclaimed by their corresponding players to restart the manual placement process.
Incorporating design features into the integrated research framework is important to synthesize the general lessons to better design serious games as part of extended reality. It is worthwhile to note that the updates to the pyramid are not intended to be prescriptive but rather a flexible plug-in that may be tailored to the circumstances. The integrated research framework has to build upon a mapping approach that includes many different aspects, i.e., mechanics, art, and storytelling, and addresses them in an iterative manner. To the best of the authors’ knowledge, there is only one triadic scheme that illustrates specific features of the serious game positioned toward the development of professional competencies [70]. However, the practices emphasizing the fundamental elements of a layered approach are rarely presented like those presented in this project. This has been identified as a shortcoming for the application of gaming methods in healthcare institutions.
Research findings show that the proportion of inter-hospital transfer increases by 7.2% as long as the resource utilization increases by 10% at the module level. This means that prioritizing ambulance transport capacity could be considered the most impactful intervention to reduce employee strain and mitigate systemic overcrowding. The managerial implication highlights the stratification of care delivery by integrating mobile units into operational frameworks to reduce reliance on traditional medical transport for low-acuity cases and the revision of performance indicators to prioritize response time equity and employee workload balance. To spread the management implications to other industries, the transferability of the research findings requires abstracting the core principles of serious game design, including modularity, participation, and adaptive tool selection, and contextualizing them within the operational realities of target industries. By leveraging the methodological framework alongside advanced digital tools, industries can underscore the operational viability of this approach in domains as diverse as manufacturing, logistics, and public services. Operations managers must act as systems integrators, fostering collaboration between technical teams and frontline stakeholders while advocating for scalable, resilient system designs.
A critical challenge lies in balancing structured phases with agile adaptation. Organizations must institutionalize iterative feedback mechanisms, such as cross-functional task forces or digital twin platforms, to test modular interventions without disrupting core operations. Furthermore, aligning incentives using policy frameworks or industry consortia can accelerate sector-wide adoption. By codifying lessons from one domain into reusable frameworks, such as adapting healthcare administration logic to emergency response coordination in disaster management, industries not only cultivate a shared language of resilience but also transform isolated improvements into cross-sector best practices, advancing systemic efficiency and innovation.
5.1. Reflections on Conducting Serious Games and Tabletop Exercises in Hospital Systems
In this study, the use of design features as building blocks parallels the approach developed by Renger et al. for the Homeland Security Exercise and Evaluation Program (HSEEP) [71]. However, a substantial amount of time and resources have been invested to model and simulate the work environment, considering the advantages of the interactive media format in relocating the skillsets needed to address ground-level issues inside an emergency department [72]. The author believes that the focus of programming the scenarios could help frame the gaming type of discussion-based exercises in similar studies related to disaster preparedness. At the current stage, the participatory design process of the serious game as an extended reality must proceed through further refinement procedures before rising to the level of a program. As long as a program is ascertained, the Balanced Scorecard approach that has been demonstrated to be viable in the fields of healthcare evaluation [73] and emergency management [74,75] could serve as the reference benchmark to indicate high-level contrasts in performance.
It is beneficial to explore the role of the top-level medical center as the critical infrastructure for disease control. Singleton et al. examined the detailed corrective actions and continuous improvement associated with the HSEEP After Action Report/Improvement Plan template, a promising toolbox for strengthening the functionalities of public health institutions during a pandemic or outbreak response [76]. Previous scholars reported effective procedures for handling chemical crisis situations from the European perspective [77]. The European medical response exercise demonstrated not only the rapid consumption of critical resources in the catchment area but also surge capacity bottlenecks inside triage, the intensive care unit, patient transport, and communication as components of the pediatric emergency department. To extend the sector’s coverage of children’s health, documentation and reporting methods for adverse events need refinement in the serious game. These methods should allow the successful identification of deficiencies for a knowledge-intensive organization that has been positioned to specialize in translating innovation into practice.
The efforts to assemble forms of media are overall prioritizing the deployment of skillsets in exposure to patient flow challenges compared to previous studies primarily addressing common issues such as vaccines, school closures, and death rates [78]. Mirzaei et al. utilized conventional lecturing and practical training by reviewing an earthquake scenario, suggesting more significant effects of the practical education method than lecturing education [79]. The authors have already implemented a debriefing component for university students to ensure that they learn new information. Further studies could feature variations based on the lecturing–gaming–debriefing method to align with the level of the healthcare professional’s readiness for natural disasters [80]. To foster a teamwork atmosphere, the steering group confirmed the narrative, scenario, and dominant design strategy through collective bargaining at the early stage of the project. However, it is important to refer to well-known cooperative games, i.e., the Healthy Heart Hospital, which familiarizes players with creativity and expresses a discourse to reclaim its former prestige [81]. This has to be recognized using fine art design, opening new opportunities for customers to appreciate the intellectual content.
5.2. Reflections on the Integrated Research Framework of the Reality-Changing Method
The integrated research framework is a breakdown supporting the adoption of the reality-changing method from idea generation to the finalization of build materials toward a demonstrative space based on the interplay among dynamics, scenarios, and role-play, as presented in Figure 5. The layered approach can be extended to principals who wish to bring in additional features and motivate university students through visual communications. It is therefore mapped out in a way that is easy to follow from cross-domain perspectives to make sure that the final appearance of the serious game as an extended reality corresponds to the achievement of intended outcomes. The proposal could be easily practiced because it does not require additional factual information or delay due to extensive details; it could be relished and discussed at spatial resolutions, including single-departmental, cross-departmental, and cross-institutional levels. The clarity of the proposal is considered meritorious by virtue of the straightforward process of focusing on the design philosophies, applications of techniques, and pluralism to cultivate innovations. Furthermore, it filters out inappropriate and counter-intuitive mechanics as it only involves selective features. The framework does not require an analytical dimension, which is often subject to quantitative measurements of performance. In order to operationalize the framework, perspective-taking workshops should be arranged, followed by debriefings.
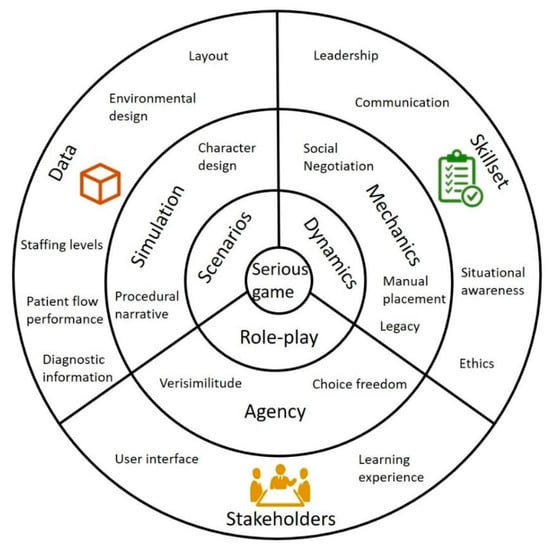
Figure 5.
The integrated research framework summarized from implementing the serious game as an extended reality among university students.
6. Conclusions
This study discovered that the reality-changing method encompassed diverse insights from stakeholders and increased the level of engagement in deliberate practice. The reality-changing method affected the outcomes of serious gaming in the context of skillset development. The outcomes from the emergency logistics case study updated the data–simulation–gaming pyramid with several novel features that further established the correspondences between the multiple layers of the integrated research framework. In addition, the average waiting time during the serious game decreased to 32 min, a considerable improvement given that more than half of the patients at the hospital in 2024 waited longer than the strengthened duration guarantee before seeing a doctor in Sweden. The reality-changing method, which better integrates scenarios, dynamics, and role-play, could be extended to future projects of hospital administrations.
The scheme could be tailored by principals based on the intersection area between serious gaming and healthcare. This refinement is subject to contextual ramifications founded in stakeholder engagement. Further updates are expected to include scripted and non-scripted activities. It is worthwhile to mention that the principals need to explore immersive technologies when establishing a ‘safe space’ for the expression of agency. The procedural narrative could fit into the extended reality together with other design improvement strategies, such as enveloping objectives and assignments [82]. Intuitive, rewarding systems could be adopted to enhance the experience of new interactions between people and services [83]. Further revisions of the gameplay mechanics could feature deck building and area influence genres. Finally, the display of advanced metrics for emergency department performance through the user interface should facilitate an intensive, high-frequency decision-making process that expedites the acquisition of intangible skills.
Author Contributions
Conceptualization, Y.S. and C.Z.; data curation, Y.S. and C.Z.; formal analysis, Y.S. and C.Z.; funding acquisition, Y.S.; investigation, Y.S. and C.Z.; methodology, Y.S. and C.Z.; resources, Y.S. and C.Z.; software, C.Z.; supervision, C.Z.; validation, C.Z.; writing—original draft, Y.S. and C.Z.; writing—review and editing, Y.S. and C.Z. All authors have read and agreed to the published version of the manuscript.
Funding
This study was funded by the University-Level Teaching Reform Project of Shandong University of Finance and Economics of China under Grant No. jy202310, the Shandong Provincial Natural Science Foundation of China under Grant No. ZR2023MG020, and the Program for Scientific Research Innovation Team in Colleges and Universities of Shandong Province of China under Grant No. 2022RW084.
Data Availability Statement
Data used to support the findings of this study are available from the authors upon request.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Nto, S.E.; Oluwatola, T.; Samuel, O.; Okagbue, H.; Atobatele, S.; Ibanga, A.; Adegoke, A.; Emuren, D.; Dumbulwa, S.A.; Sampson, S.; et al. Strengthening care for emergencies: What is the level of awareness and utilization of Emergency Medical Services (EMS) in FCT, Nigeria? BMC Emerg. Med. 2024, 24, 73. [Google Scholar] [CrossRef] [PubMed]
- Musson, D.M. Crew Resource Management (CRM) in the Aviation Industry. In Improving Healthcare Team Communication; CRC Press: Boca Raton, FL, USA, 2008. [Google Scholar]
- Sonesson, L.; Boffard, K.D.; Örtenwall, P.; Vekzsler, P. Determining the educational impact of virtual patients on trauma team training during a multinational, large-scale civil military simulation exercise. J. Trauma Acute Care Surg. 2023, 95 (Suppl. S1), S99–S105. [Google Scholar] [CrossRef] [PubMed]
- Rider, A.C.; Williams, S.R.; Jones, V.; Rebagliati, D.; Schertzer, K.; Gisondi, M.A.; Sebok-Syer, S.S. Assessing Team Performance: A Mixed-Methods Analysis Using Interprofessional in situ Simulation. West. J. Emerg. Med. 2024, 25, 557–564. [Google Scholar] [CrossRef] [PubMed]
- Rojas López, M.D.; Jerez Jiménez, Y.A.; Morales Barbosa, R.E. Strengthening administrative knowledge through a serious game. Cuad. Adm. 2023, 39, 5. [Google Scholar]
- Beishuizen, B.H.; Stein, M.L.; Buis, J.S.; Tostmann, A.; Green, C.; Duggan, J.; Connolly, M.A.; Rovers, C.P.; Timen, A. A systematic literature review on public health and healthcare resources for pandemic preparedness planning. BMC Public Health 2024, 24, 3114. [Google Scholar] [CrossRef]
- Flin, R.; O’Connor, P. Safety at the Sharp End: A Guide to Non-Technical Skills; CRC Press: London, UK, 2017. [Google Scholar] [CrossRef]
- Tan, Y.X.; Jalal, A.H.B.; Ngai, V.; Manobharath, N.; Soh, T.C.F. What are the non-technical skills required by junior doctors in the NHS to manage medical emergencies? A scoping review. Postgrad. Med. J. 2021, 97, 813–818. [Google Scholar] [CrossRef]
- Tenso, K.; Pizer, S.; Palani, S. Delivery system emergency department capacity and its effect on nonsystem service utilization. Acad. Emerg. Med. 2023, 30, 359–367. [Google Scholar] [CrossRef]
- Howard, M.; Pflaum-Carlson, J.; Hurst, G.; Gardner-Gray, J.; Kinni, H.; Coba, V.; Rivers, E.; Jayaprakash, N. A roadmap for developing an emergency department based critical care consultation service: Building the early intervention team (EIT). Am. J. Emerg. Med. 2023, 66, 81–84. [Google Scholar] [CrossRef]
- Puissant, M.M.; Agarwal, I.; Scharnetzki, E.; Cutler, A.; Gunnell, H.; Strout, T.D. Racial differences in triage assessment at rural vs urban Maine emergency departments. Intern. Emerg. Med. 2024, 19, 1733–1743. [Google Scholar] [CrossRef]
- Muir, K.J.; McHugh, M.D.; Merchant, R.M.; Lasater, K.B. Left Without Being Seen: Nurse Work Environment and Timely Outcomes in New York and Illinois Emergency Departments. J. Emerg. Nurs. 2024, 50, 660–669. [Google Scholar] [CrossRef]
- Natan, M.B.; Maman, D.; Avramov, M.; Shamilov, G.; Berkovich, Y. Exploring Factors Influencing Orthopedic Patients’ Willingness to Recommend a Hospital: Insights From a Cross-Sectional Survey. J. Patient Exp. 2024, 11, 23743735241282706. [Google Scholar] [CrossRef] [PubMed]
- Ali, S.; Li, G.; Yang, P.; Hussain, K.; Latif, Y. Unpacking the importance of intangible skills in new product development and sustainable business performance; strategies for marketing managers. PLoS ONE 2020, 15, e0238743. [Google Scholar] [CrossRef] [PubMed]
- Lukosch, H.K. Richard D. Duke: Systems Thinker, Game Science Founder & Beloved Mentor. Simul Gaming 2023, 54, 221–234. [Google Scholar] [CrossRef]
- Mustafee, N.; Katsaliaki, K.; Taylor, S.J.E. Profiling Literature in Healthcare Simulation. Simulation 2010, 86, 543–558. [Google Scholar] [CrossRef]
- Perera, T.S.; Uslu, B.Ç. Simulation analysis of a neonatal unit with complex patient flow patterns—An enhanced model for capacity planning. S. Afr. J. Ind. Eng. 2022, 33, 94–108. [Google Scholar] [CrossRef]
- Omidvarkarjan, D.; Hofelich, M.; Conrad, J.; Klahn, C.; Meboldt, M. Teaching agile hardware development with an open-source engineering simulator: An evaluation with industry participants. Comput. Appl. Eng. Educ. 2023, 31, 946–962. [Google Scholar] [CrossRef]
- Peñafiel-Mera, A.; Santos, G. Differences in perceptions of fuel duties and emissions trading in road transport. Transp. Policy 2024, 153, 24–38. [Google Scholar] [CrossRef]
- Tanner, C.; Schmocker, D.; Katsarov, J.; Christen, M. Educating moral sensitivity in business: An experimental study to evaluate the effectiveness of a serious moral game. Comput. Educ. 2022, 178, 104381. [Google Scholar] [CrossRef]
- Rodrigues, V.; Rocha, R. Participatory ergonomics approaches to design and intervention in workspaces: A literature review. Theor. Issues Ergon. Sci. 2022, 24, 413–428. [Google Scholar] [CrossRef]
- Waite, I.A.; Kavakoglu, A.A.; Robescu, L.D.; Cocarta, D.M.; Vuta, L.I. Game-based learning about the circular economy in building sustainable communities: A case of international and interdisciplinary university collaboration. Int. J. Sustain. High. Educ. 2024, 25, 378–396. [Google Scholar] [CrossRef]
- Gugerell, K.; Zuidema, C. Gaming for the energy transition. Experimenting and learning in co-designing a serious game prototype. J. Clean. Prod. 2017, 169, 105–116. [Google Scholar] [CrossRef]
- Ryschawy, J.; Grillot, M.; Charmeau, A.; Pelletier, A.; Moraine, M.; Martin, G. A participatory approach based on the serious game Dynamix to co-design scenarios of crop-livestock integration among farms. Agric. Syst. 2022, 201, 103414. [Google Scholar] [CrossRef]
- Derks, S.; Willemen, A.M.; Wouda, M.; Meekel, M.; Sterkenburg, P.S. The co-creation design process of ‘You & I’: A serious game to support mentalizing and stress-regulating abilities in adults with mild to borderline intellectual disabilities. Behav. Inf. Technol. 2022, 41, 2988–3000. [Google Scholar] [CrossRef]
- Timm, A.; Maindal, H.T.; Hillersdal, L. Co-creating with families and healthcare professionals: Shaping a context-sensitive health promotion intervention ‘Face-it’. Health Promot. Int. 2022, 37, ii60–ii72. [Google Scholar] [CrossRef]
- bin Kamruddin, A.; Sandison, H.; Patil, G.; Musolesi, M.; di Bernardo, M.; Richardson, M.J. Modelling human navigation and decision dynamics in a first-person herding task. R. Soc. Open Sci. 2024, 11, 231919. [Google Scholar] [CrossRef]
- El-Maissi, A.M.; Kassem, M.M.; Mohamed Nazri, F. Resilient critical infrastructures: An innovative methodological perspective for critical infrastructure (CI) integrated assessment models by inducing digital technologies during multi-hazard incidents. MethodsX 2024, 12, 102561. [Google Scholar] [CrossRef]
- Sanko, J.S.; Gattamorta, K.; Young, J.; Durham, C.F.; Sherwood, G.; Dolansky, M. A Multisite Study Demonstrates Positive Impacts to Systems Thinking Using a Table-top Simulation Experience. Nurse Educ. 2021, 46, 29. [Google Scholar] [CrossRef]
- Broski, J.; Tarver, S.; Krase, K.; Petersen, S.; Wolverton, A.; Winchester, M.; Berbel, G.; Zabel, T.; Warren, H.; Lineberry, M. Integrating simulation and interpretive description to explore operating room leadership: Critical event continuing education. Adv. Health Sci. Educ. Theory Pract. 2023, 28, 1211–1244. [Google Scholar] [CrossRef]
- Tong, T.; Chignell, M.; Tierney, M.C.; Lee, J. A Serious Game for Clinical Assessment of Cognitive Status: Validation Study. JMIR Serious Games 2016, 4, e7. [Google Scholar] [CrossRef]
- Mand, N.; Hoffmann, M.; Schwalb, A.; Leonhardt, A.; Sassen, M.; Stibane, T.; Maier, R.F.; Donath, C. Management of Paediatric Cardiac Arrest due to Shockable Rhythm-A Simulation-Based Study at Children’s Hospitals in a German Federal State. Children 2024, 11, 776. [Google Scholar] [CrossRef]
- Zhang, C.; Hauge, J.B.; Härenstam, K.P.; Meijer, S. Game Experience and Learning Effects of a Scoring-Based Mechanic for Logistical Aspects of Pediatric Emergency Medicine: Development and Feasibility Study. JMIR Serious Games 2021, 9, e21988. [Google Scholar] [CrossRef] [PubMed]
- Rittel, H.W.J.; Webber, M.M. Dilemmas in a general theory of planning. Policy Sci. 1973, 4, 155–169. [Google Scholar] [CrossRef]
- Kraus, M.; Rauner, M.S.; Schwarz, S. Hospital management games: A taxonomy and extensive review. Cent. Eur. J. Oper. Res. 2010, 18, 567–591. [Google Scholar] [CrossRef]
- Fusco, N.M.; Foltz-Ramos, K.; Ohtake, P.J.; Mann, C. Interprofessional Simulation Learning Game Increases Socialization and Teamwork Among Students of Health Professions Programs. Nurse Educ. 2024, 49, E32–E35. [Google Scholar] [CrossRef] [PubMed]
- Fusco, N.M.; Foltz-Ramos, K.; Jacobsen, L.J.; Gambacorta, J. Educational game improves systems thinking, socialization, and teamwork among students of 13 health professions programs. J. Interprof. Care 2024, 38, 176–181. [Google Scholar] [CrossRef] [PubMed]
- Chon, S.H.; Timmermann, F.; Dratsch, T.; Schuelper, N.; Plum, P.; Berlth, F.; Datta, R.R.; Schramm, C.; Haneder, S.; Späth, M.R.; et al. Serious Games in Surgical Medical Education: A Virtual Emergency Department as a Tool for Teaching Clinical Reasoning to Medical Students. JMIR Serious Games 2019, 7, e13028. [Google Scholar] [CrossRef]
- Nicolaidou, I.; Antoniades, A.; Constantinou, R.; Marangos, C.; Kyriacou, E.; Bamidis, P.; Dafli, E.; Pattichis, C.S. A Virtual Emergency Telemedicine Serious Game in Medical Training: A Quantitative, Professional Feedback-Informed Evaluation Study. J. Med. Internet Res. 2015, 17, e150. [Google Scholar] [CrossRef]
- Tong, T.; Chignell, M.; Tierney, M.C.; Lee, J.S. Test-Retest Reliability of a Serious Game for Delirium Screening in the Emergency Department. Front. Aging Neurosci. 2016, 8, 258. [Google Scholar] [CrossRef]
- Care at Karolinska University Hospital. Available online: https://www.karolinskahospital.com/care-at-karolinska/ (accessed on 23 January 2024).
- Hobgood, C.D.; Jarman, A.F. Resilience Building Practices for Women Physicians. J. Womens Health 2024, 33, 532–541. [Google Scholar] [CrossRef]
- Belardinelli, M.; Ricci, M.; Frassini, S.; Ventura, D.; Rasori, S. Process nurse: The experience of the Emergency Department of Fano. Assist. Inferm. E Ric. AIR 2024, 43, 54–60. [Google Scholar] [CrossRef]
- Rylander, C.; Sternley, J.; Petzold, M.; Oras, J. Unit-to-unit transfer due to shortage of intensive care beds in Sweden 2015–2019 was associated with a lower risk of death but a longer intensive care stay compared to no transfer: A registry study. J. Intensive Care 2024, 12, 10. [Google Scholar] [CrossRef] [PubMed]
- Olsson, M.; Svensson, A.; Andersson, H.; Dehre, A.; Elmqvist, C.; Rask, M.; Wireklint, S.; Boysen, G.N. Educational intervention in triage with the Swedish triage scale RETTS©, with focus on specialist nurse students in ambulance and emergency care—A cross-sectional study. Int. Emerg. Nurs. 2022, 63, 101194. [Google Scholar] [CrossRef] [PubMed]
- National Incident Management System (NIMS), 3rd ed.; [Online]. Available online: https://www.fema.gov/media-library-data/1508151197225-ced8c60378c3936adb92c1a3ee6f6564/FINAL_NIMS_2017.pdf (accessed on 5 January 2024).
- Rezvani, M.H.; Khabiri, D. Gamers’ Behaviour and Communication Analysis in Massively Multiplayer Online Games: A Survey. In Proceedings of the 2018 2nd National and 1st International Digital Games Research Conference: Trends, Technologies, and Applications (DGRC), Tehran, Iran, 29–30 November 2018; IEEE: Piscataway, NJ, USA, 2018; pp. 61–69. [Google Scholar] [CrossRef]
- Rahimabad, R.M.; Rezvani, M.H. Identifying Factors Affecting the Immersion and Concentration of Players in Serious Games. In Proceedings of the 2020 International Serious Games Symposium (ISGS), Tehran, Iran, 23–24 December 2020; IEEE: Piscataway, NJ, USA, 2020; pp. 61–67. [Google Scholar] [CrossRef]
- Jaccard, D.; Suppan, L.; Sanchez, E.; Huguenin, A.; Laurent, M. The co.LAB Generic Framework for Collaborative Design of Serious Games: Development Study. JMIR Serious Games 2021, 9, e28674. [Google Scholar] [CrossRef] [PubMed]
- Westera, W.; Nadolski, R.J.; Hummel, H.G.K.; Wopereis, I.G.J.H. Serious games for higher education: A framework for reducing design complexity. J. Comput. Assist. Learn. 2008, 24, 420–432. [Google Scholar] [CrossRef]
- Roig, A.; De Sá, F.P.; Cornelio, G.S. Future Story Chasers: An experience with co-creation of fiction in the classroom through a collaborative storytelling game. Catalan J. Commun. Cult. Stud. 2018, 10, 279–289. [Google Scholar] [CrossRef]
- Shirazi, F.B.; Moslehi, S.; Rasouli, M.R.; Masoumi, G. Identifying the Challenges of Simulating the Hospital Emergency Department in the Event of Emergencies and Providing Effective Solutions: A Qualitative Study. Disaster Med. Public Health Prep. 2022, 17, e202. [Google Scholar] [CrossRef]
- Ugelvik, K.S.; Thomassen, Ø.; Braut, G.S.; Geisner, T.; Sjøvold, J.E.; Agri, J.; Montan, C. Evaluation of prehospital preparedness for major incidents on a national level, with focus on mass casualty incidents. Eur. J. Trauma Emerg. Surg. Off. Publ. Eur. Trauma Soc. 2024, 50, 945–957. [Google Scholar] [CrossRef]
- Wu, C.-S.; Chen, M.-F.; Hwang, H.-L.; Lee, B.-O. Effectiveness of a nursing board games in psychiatric nursing course for undergraduate nursing students: An experimental design. Nurse Educ. Pract. 2023, 70, 103657. [Google Scholar] [CrossRef]
- Orbanes, P. Everything I Know About Business I Learned from Monopoly. Harvard Business Review, 1 March 2002. Available online: https://hbr.org/2002/03/everything-i-know-about-business-i-learned-from-monopoly (accessed on 2 May 2023).
- Donovan, T. It’s All a Game: The History of Board Games from Monopoly to Settlers of Catan; Thomas Dunne Books: New York, NY, USA, 2017. [Google Scholar]
- Rider, E.A.; Comeau, M.; Truog, R.D.; Boyer, K.; Meyer, E.C. Identifying intangible assets in interprofessional healthcare organizations: Feasibility of an asset inventory. J. Interprof. Care 2019, 33, 583–586. [Google Scholar] [CrossRef]
- Nellhaus, T. Online Role-playing Games and the Definition of Theatre. New Theatre Q. 2017, 33, 345–359. [Google Scholar] [CrossRef]
- Mavros, P.; Dalton, R.C.; Kuliga, S.; Morad, M.G.; Robson, S.; Hölscher, C. Architectural cognition cards: A card-based method for introducing spatial cognition research and user-centred thinking into the design process. Archit. Sci. Rev. 2022, 65, 120–137. [Google Scholar] [CrossRef]
- Maraza-Quispe, B.; Torres-Loayza, J.L.; Reymer-Morales, G.T.; Solórzano-Bernuy, R.M.; Choquehuayta-Palomino, S.A.; Pacori-Aviles, F.M. Impact of the Use of the Video Game SimCity on the Development of Critical Thinking in Students: A Quantitative Experimental Approach. IEEE Rev. Iberoam. Tecnol. Aprendiz. 2023, 18, 411–418. [Google Scholar] [CrossRef]
- de Andrade Melo, F.S.; de Magalhães Porto, C. Educação e diversão: A franquia ‘The sims’ no processo de aprendizado com jogos eletrônicos. Rev. EDaPECI 2023, 23, 14–25. [Google Scholar] [CrossRef]
- Zhang, C.; Härenstam, K.P.; Meijer, S.; Darwich, A.S. Serious Gaming of Logistics Management in Pediatric Emergency Medicine. Int. J. Serious Games 2020, 7, 47–77. [Google Scholar] [CrossRef]
- Cimino, A.; Longo, F.; Mirabelli, G.; Solina, V.; Veltri, P. Enhancing internal supply chain management in manufacturing through a simulation-based digital twin platform. Comput. Ind. Eng. 2024, 198, 110670. [Google Scholar] [CrossRef]
- Egashira, M.; Son, D.; Ema, A. Serious Game for Change in Behavioral Intention Toward Lifestyle-Related Diseases: Experimental Study With Structural Equation Modeling Using the Theory of Planned Behavior. JMIR Serious Games 2022, 10, e28982. [Google Scholar] [CrossRef]
- Khimani, K.; Koshevarova, V.; Mathew, A.A.; Gupta, A.K.; Schmitz-Brown, M.; Gupta, P.K. Video Game Warm-Up May Suggest Improvement in Ophthalmic Surgical Simulator Performance in Surgically Naïve Students. Clin. Ophthalmol. 2022, 16, 2561–2568. [Google Scholar] [CrossRef]
- Zagata, K.; Medyńska-Gulij, B. Mini-Map Design Features as a Navigation Aid in the Virtual Geographical Space Based on Video Games. ISPRS Int. J. Geo-Inf. 2023, 12, 58. [Google Scholar] [CrossRef]
- Lozano Muñoz, A. Modos y estéticas de la espera en los videojuegos. Artnodes 2022, 30, 1–9. [Google Scholar] [CrossRef]
- Hall, A. A Methodology for Systems Engineering; Nostrand Company: New York, NY, USA, 1962. [Google Scholar]
- Boysen, M.S.W.; Lund, O.; Jørnø, R.L.; Skovbjerg, H.M. The role of expertise in playful learning activities: A design-based self-study within teacher education aimed at the development of tabletop role-playing games. Teach. Teach. Educ. 2023, 128, 104128. [Google Scholar] [CrossRef]
- Harteveld, C. Triadic Game Design: Balancing Reality, Meaning and Play, 2011th ed.; Springer: London, UK; New York, NY, USA, 2011. [Google Scholar]
- Renger, R.; Renger, J.; Basson, M.D.; Van Eck, R.N.; Renger, J.; Souvannasacd, E.; Hart, G. Using the Homeland Security Exercise and Evaluation Program (HSEEP) Building Block Approach to Implement System Evaluation Theory (SET). Am. J. Eval. 2021, 42, 586–601. [Google Scholar] [CrossRef] [PubMed]
- Lordemann, A.G.; Sommerfeldt, D.; Mileder, L. Latent safety threats in a pediatric emergency department: Using in situ simulation to test a new trauma room concept. Z. Evidenz Fortbild. Qual. Gesundheitswesen 2024, 187, 15–21. [Google Scholar] [CrossRef]
- Alipour, F.; Jamshidizadeh, S.; Bastani, P.; Mehralian, G. The balanced scorecard as a strategic management tool in hospital pharmacies: An experimental study. J. Health Organ. Manag. 2022; ahead-of-print. [Google Scholar] [CrossRef]
- Carvalho, P.; Spataru, C. Co-designing a just resilience balance scorecard with experts in islands and coastal cities. Clim. Risk Manag. 2024, 43, 100577. [Google Scholar] [CrossRef]
- Soujaa, I.; Nukpezah, J.A.; Dimitrijevska-Markoski, T. A Balanced Scorecard approach to the Homeland Security Evaluation and Exercise Program. Risk Hazards Crisis Public Policy 2023, 15, 393–407. [Google Scholar] [CrossRef]
- Singleton, C.-M.; DeBastiani, S.; Rose, D.; Kahn, E.B. An Analysis of Root Cause Identification and Continuous Quality Improvement in Public Health H1N1 After-Action Reports. J. Public Health Manag. Pract. 2014, 20, 197–204. [Google Scholar] [CrossRef]
- Davidson, R.K.; Magalini, S.; Brattekås, K.; Bertrand, C.; Brancaleoni, R.; Rafalowski, C.; Nakstad, E.R. Preparedness for chemical crisis situations: Experiences from European medical response exercises. Eur. Rev. Med. Pharmacol. Sci. 2019, 23, 1239–1247. [Google Scholar] [CrossRef]
- Thornton, M.I.; Iannotti, A.; Quaranta, R.; Russo, C. The Effectiveness of Table-Top Exercises in Improving Pandemic Crisis Preparedness. Int. J. Saf. Secur. Eng. 2021, 11, 463–471. [Google Scholar] [CrossRef]
- Mirzaei, S.; Eftekhari, A.; Mohammadinia, L.; Tafti, A.A.D.; Norouzinia, R.; Nasiriani, K. Comparison of the Effect of Lecturing and Tabletop Exercise Methods on Level of Preparedness of Nurses against Natural Disasters. J. Holist. Nurs. Midwifery 2020, 30, 17–26. [Google Scholar] [CrossRef]
- Mafuko-Nyandwi, B.; Kervyn, M.; Habiyaremye, F.M.; Vanwing, T.; Kervyn, F.; Jacquet, W.; Mitengezo, V.; Michellier, C. Building a prepared community to volcanic risk in the global south: Assessment of awareness raising tools for high school students in Goma, (East DR Congo). Prog. Disaster Sci. 2024, 24, 100370. [Google Scholar] [CrossRef]
- Healthy Heart Hospital. BoardGameGeek. Available online: https://boardgamegeek.com/boardgame/186721/healthy-heart-hospital (accessed on 25 January 2024).
- Rapp, A. Drawing Inspiration from World of Warcraft: Gamification Design Elements for Behavior Change Technologies. Interact. Comput. 2017, 29, 648–678. [Google Scholar] [CrossRef]
- Opromolla, A.; Volpi, V.; Parente, G.A. Co-Designing Game Solutions for Hybrid Urban Spaces. How Game Elements Can Improve People Experience with the Mobility Services. Interact. Des. Archit. 2019, 40, 9–23. [Google Scholar] [CrossRef]
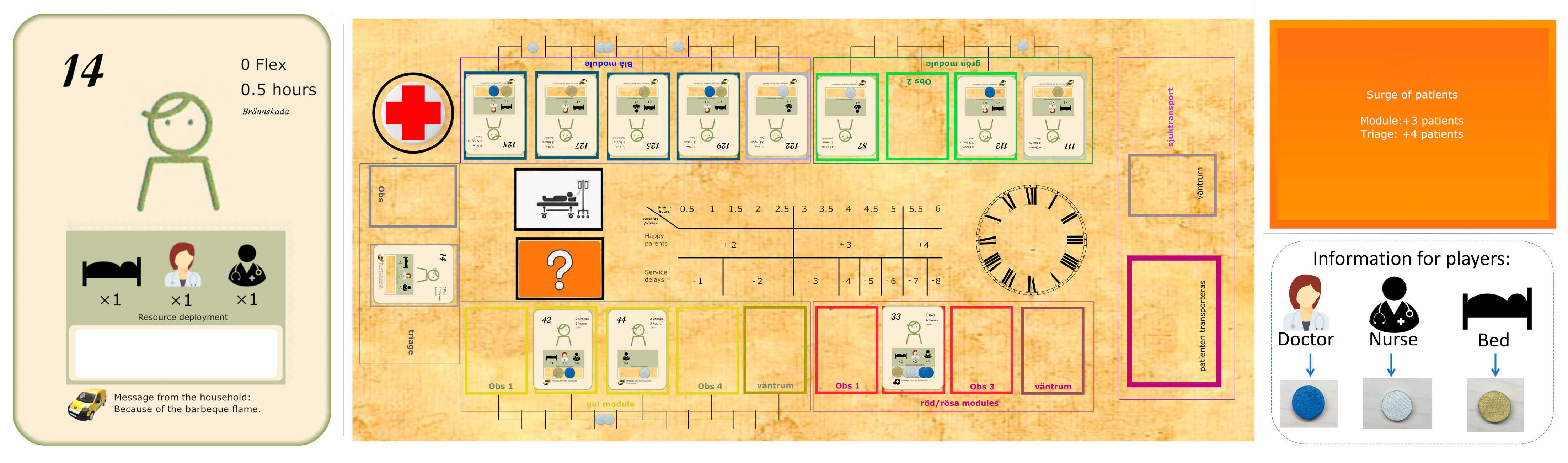
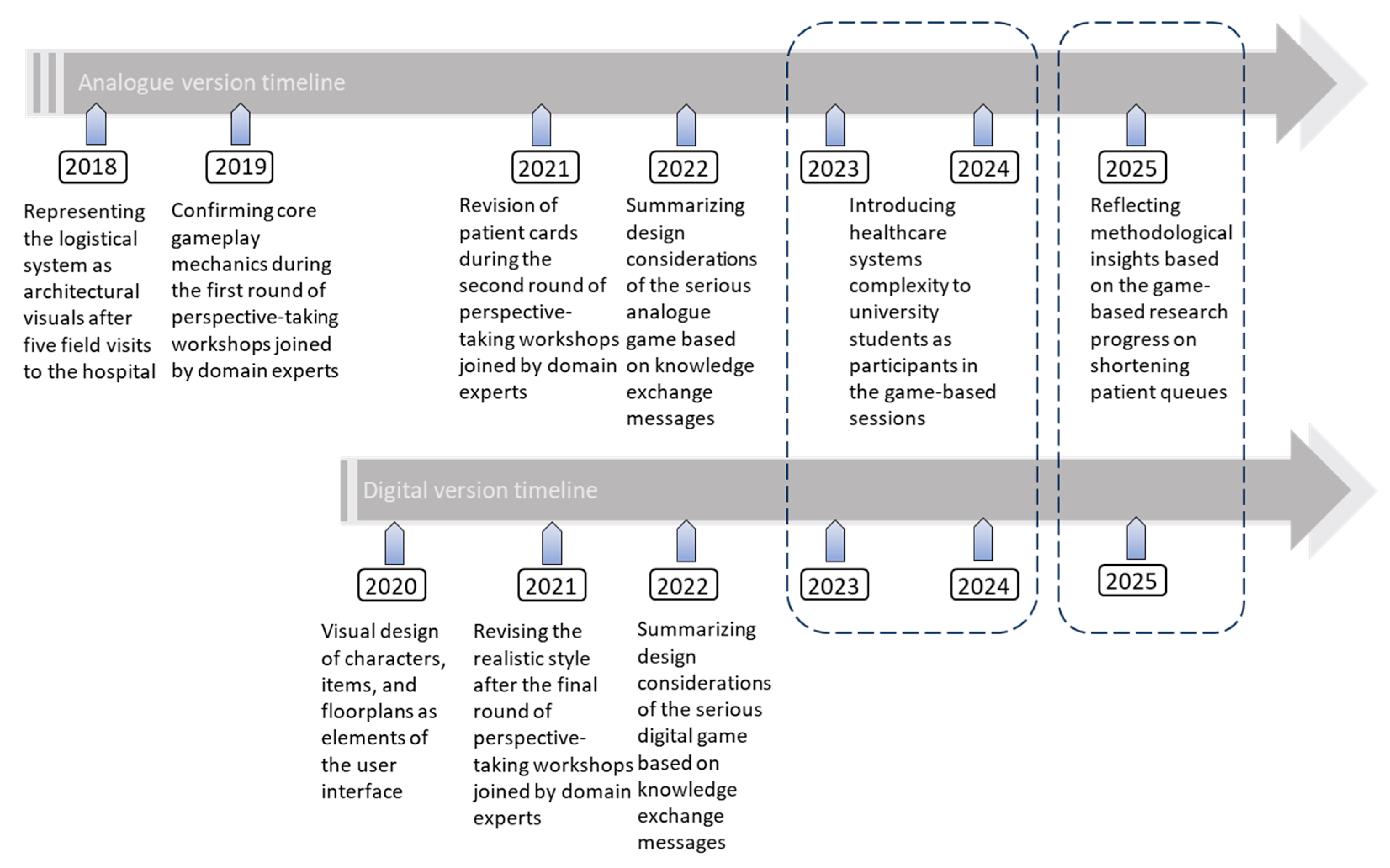
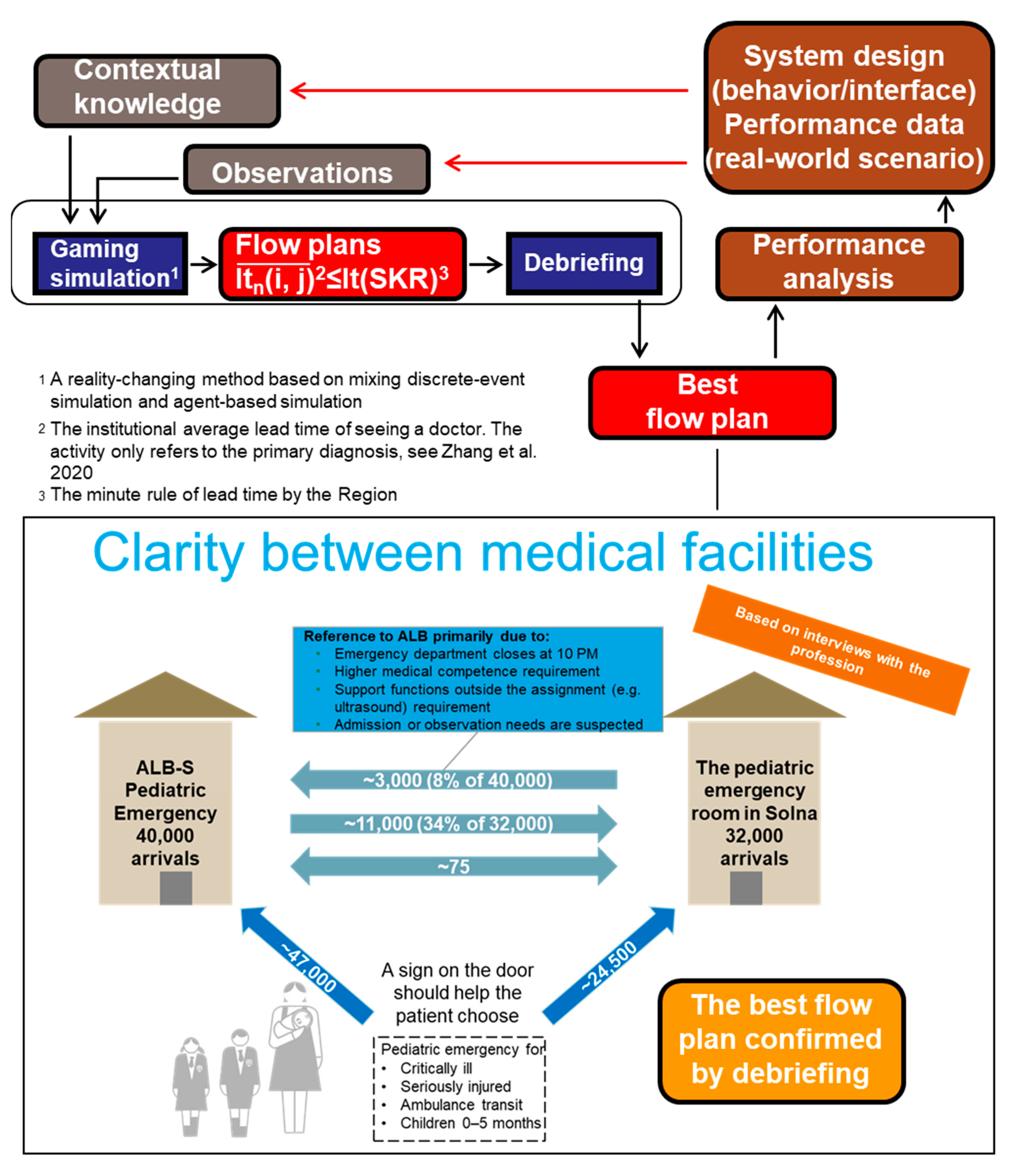
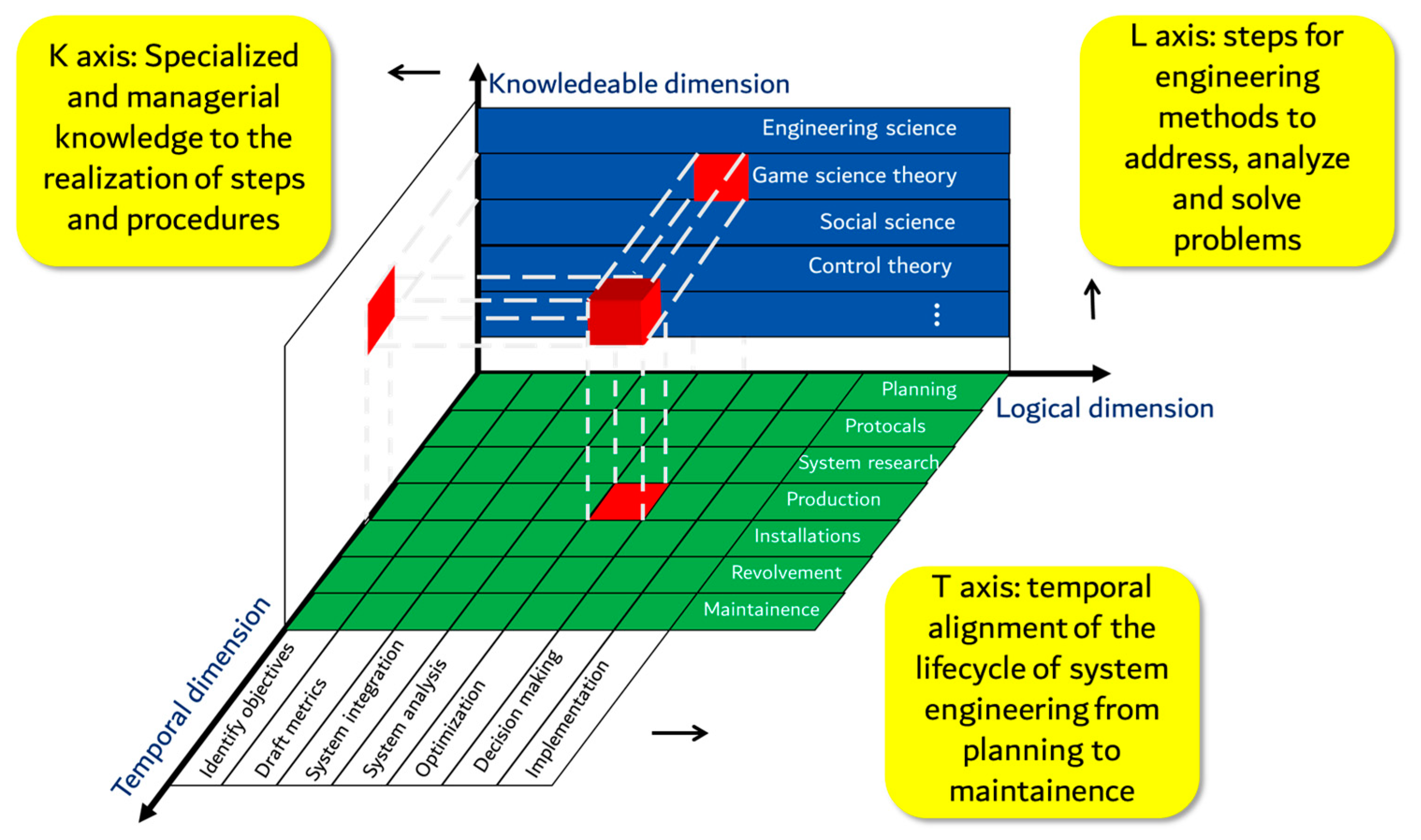
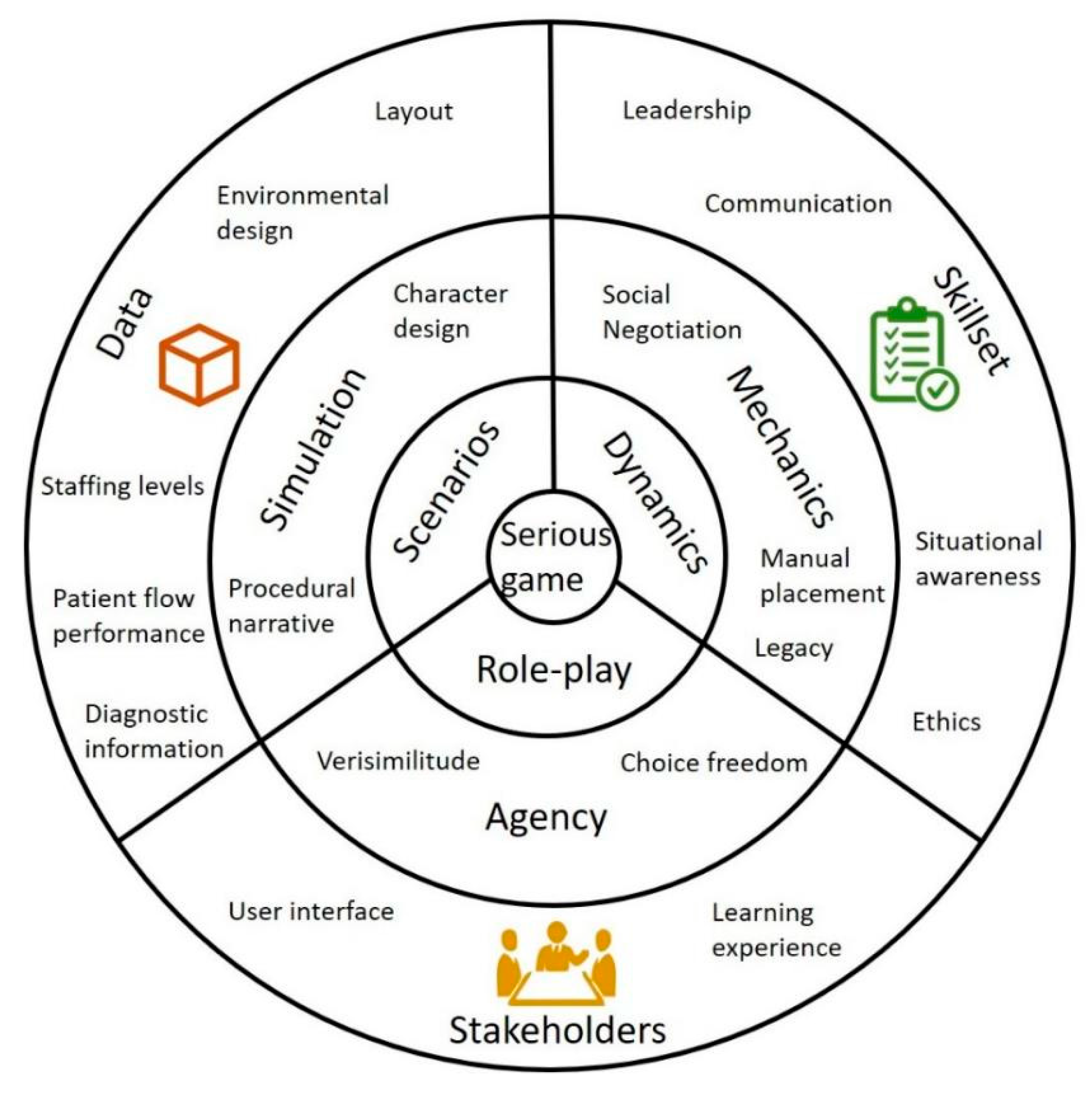
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).