
Carbon Dioxide Laser Vulvovaginal Rejuvenation: A Systematic Review



Abstract
:1. Introduction
1.1. Genitourinary Syndrome of Menopause (GSM)
1.2. Vulvovaginal Rejuvenation
1.3. Study Objectives and Design
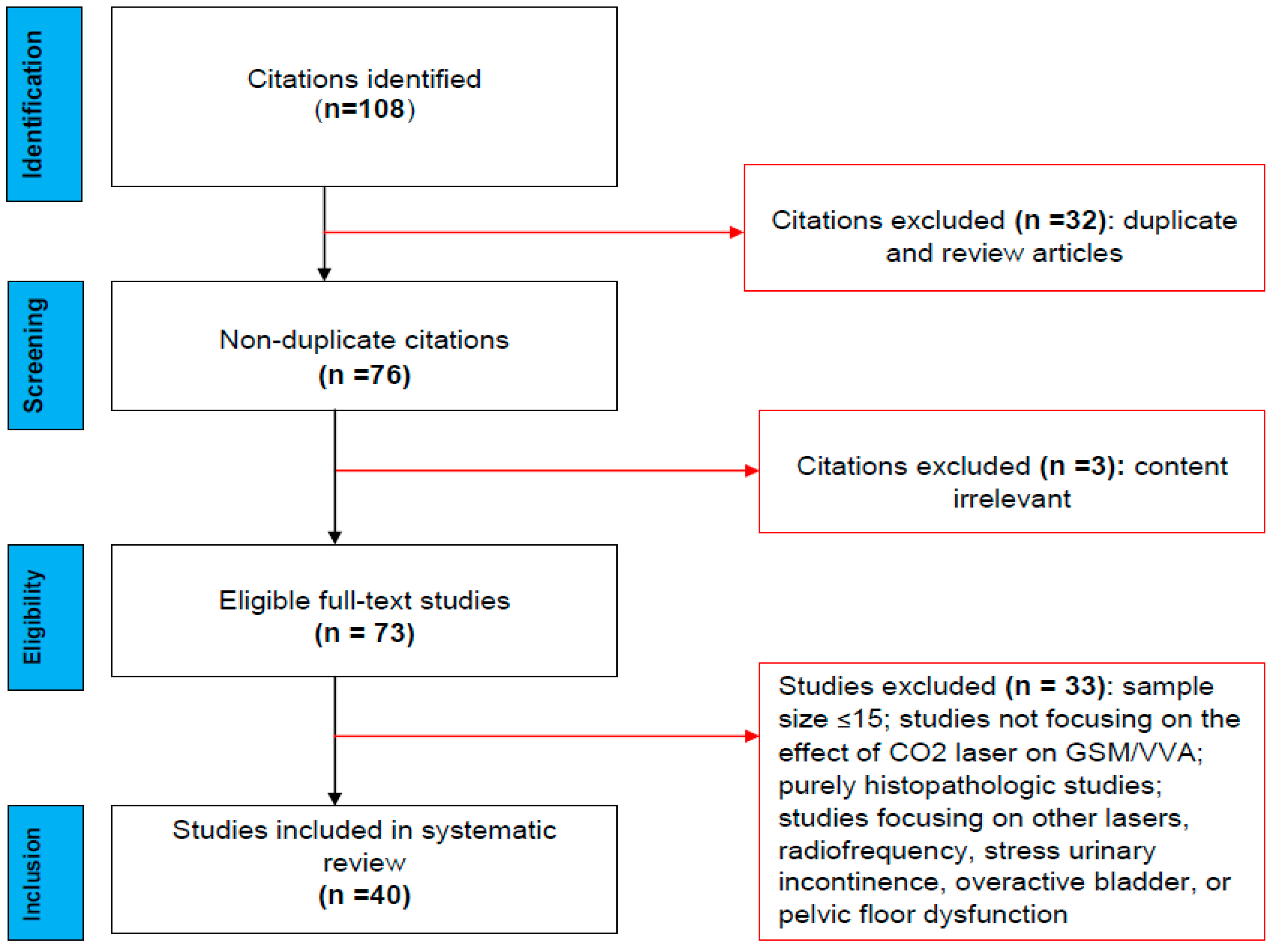
2. Methods
3. Results
4. Discussion
4.1. GSM Management
4.2. CO2 Laser Mechanism of Rejuvenation
4.3. Clinical Efficacy of CO2 Laser Therapy for GSM
4.4. CO2 Laser Therapy for GSM: Effects on Sexual Function
4.5. CO2 Laser Therapy for GSM: Adverse Effects, QoL, and Patient Satisfaction
4.6. Limitations
5. Conclusions and Future Directions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Iosif, C.S.; Batra, S.; Ek, A.; Åstedt, B. Estrogen receptors in the human female lower urinary tract. Am. J. Obstet. Gynaecol. 1981, 141, 817–820. [Google Scholar] [CrossRef]
- Portman, D.J.; Gass, M.L.S. Genitourinary syndrome of menopause: New terminology for vulvovaginal atrophy from the international society for the study of womens sexual health and the North American Menopause Society. Climacteric 2014, 17, 557–563. [Google Scholar] [CrossRef]
- Briggs, P. Genitourinary syndrome of menopause. Post Reprod. Health 2019, 26, 111–114. [Google Scholar] [CrossRef]
- Hulmes, D.J. Building collagen molecules, fibrils, and suprafibrillar structures. J. Struct. Biol. 2002, 137, 2–10. [Google Scholar] [CrossRef]
- Palma, F.; Xholli, A.; Cagnacci, A. The most bothersome symptom of vaginal atrophy: Evidence from the observational AGATA Study. Maturitas 2018, 108, 18–23. [Google Scholar] [CrossRef] [PubMed]
- Palacios, S.; Nappi, R.E.; Bruyniks, N.; Particco, M.; Panay, N. The European Vulvovaginal Epidemiological Survey (EVES): Prevalence, symptoms and impact of vulvovaginal atrophy of menopause. Climacteric 2018, 21, 286–291. [Google Scholar] [CrossRef]
- Bride, M.B.M.; Rhodes, D.J.; Shuster, L.T. Vulvovaginal atrophy. Mayo. Clin. Proc. 2010, 85, 87–94. [Google Scholar] [CrossRef] [Green Version]
- Kim, H.-K.; Kang, S.-Y.; Chung, Y.-J.; Kim, J.-H.; Kim, M.-R. The recent review of the genitourinary syndrome of menopause. J. Menopausal Med. 2015, 21, 65. [Google Scholar] [CrossRef] [Green Version]
- Murina, F.; Francesco, S.D.; Oneda, S. Vulvar vestibular effects of ospemifene: A pilot study. Gynecol. Endocrinol. 2018, 34, 631–635. [Google Scholar] [CrossRef] [PubMed]
- Moral, E.; Delgado, J.L.; Carmona, F.; Caballero, B.; Guillán, C.; González, P.M.; Suárez-Almarza, J.; Velasco-Ortega, S.; Nieto, C. Genitourinary syndrome of menopause. prevalence and quality of life in spanish postmenopausal women. GENISSE Study. Climacteric 2018, 21, 167–173. [Google Scholar] [CrossRef]
- Barbara, G.; Facchin, F.; Buggio, L.; Alberico, D.; Frattaruolo, M.; Kustermann, A. Vaginal rejuvenation: Current perspectives. Int. J. Womens Health 2017, 9, 513–519. [Google Scholar] [CrossRef] [Green Version]
- Karcher, C.; Sadick, N. Vaginal rejuvenation using energy-based devices. Int. J. Womens Dermatol. 2016, 2, 85–88. [Google Scholar] [CrossRef] [Green Version]
- Desai, S.A.; Kroumpouzos, G.; Sadick, N. Vaginal rejuvenation: From scalpel to wands. Int. J. Womens Dermatol. 2019, 5, 79–84. [Google Scholar] [CrossRef]
- Qureshi, A.A.; Tenenbaum, M.M.; Myckatyn, T.M. Nonsurgical vulvovaginal rejuvenation with radiofrequency and laser devices: A literature review and comprehensive update for aesthetic surgeons. Aesthet. Surg. J. 2017, 38, 302–311. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gambacciani, M.; Palacios, S. Laser therapy for the restoration of vaginal function. Maturitas 2017, 99, 10–15. [Google Scholar] [CrossRef] [PubMed]
- ACOG Committee. Vaginal “rejuvenation” and cosmetic vaginal procedures. Obstet. Gynecol. 2007, 110, 737–738. [Google Scholar] [CrossRef]
- RANZCOG. Women’s Health Committee. Vaginal ‘rejuvenation’ and cosmetic vaginal procedures. Aust. NZ J. Obstet. Gynaecol. 2019. [Google Scholar] [CrossRef]
- Center for Devices and Radiological Health. FDA Warns against Energy-Based Devices to Perform Vaginal Rejuvenation. Available online: https://www.fda.gov/medical-devices/safety-communications/fda-warns-against-use-energy-based-devices-perform-vaginal-rejuvenation-or-vaginal-cosmetic (accessed on 16 April 2021).
- Salvatore, S.; Maggiore, U.L.R.; Origoni, M.; Parma, M.; Quaranta, L.; Sileo, F.; Cola, A.; Baini, I.; Ferrero, S.; Candiani, M.; et al. Microablative fractional CO2 laser improves dyspareunia related to vulvovaginal atrophy: A pilot study. J. Endometr. Pelvic Pain Disord. 2014, 6, 150–156. [Google Scholar] [CrossRef]
- Salvatore, S.; Nappi, R.E.; Zerbinati, N.; Calligaro, A.; Ferrero, S.; Origoni, M.; Candiani, M.; Maggiore, U.L.R. A 12-week treatment with fractional CO2 laser for vulvovaginal atrophy: A pilot study. Climacteric 2014, 17, 363–369. [Google Scholar] [CrossRef]
- Salvatore, S.; Nappi, R.E.; Parma, M.; Chionna, R.; Lagona, F.; Zerbinati, N.; Ferrero, S.; Origoni, M.; Candiani, M.; Leone Roberti Maggiore, U. Sexual function after fractional microablative CO2 laser in women with vulvovaginal atrophy. Climacteric 2014, 18, 219–225. [Google Scholar] [CrossRef]
- Perino, A.; Calligaro, A.; Forlani, F.; Tiberio, C.; Cucinella, G.; Svelato, A.; Saitta, S.; Calagna, G. Vulvo-vaginal atrophy: A new treatment modality using thermoablative fractional CO2 laser. Maturitas 2015, 80, 296–301. [Google Scholar] [CrossRef] [PubMed]
- Pagano, T.; Rosa, P.D.; Vallone, R.; Schettini, F.; Arpino, G.; Placido, S.D.; Nazzaro, G.; Locci, M.; Placido, G.D. Fractional microablative CO2 laser for vulvovaginal atrophy in women treated with chemotherapy and/or hormonal therapy for breast cancer: A retrospective study. Menopause 2016, 23, 1108–1113. [Google Scholar] [CrossRef]
- Pieralli, A.; Fallani, M.G.; Becorpi, A.; Bianchi, C.; Corioni, S.; Longinotti, M.; Tredici, Z.; Guaschino, S. Fractional CO2 laser for vulvovaginal atrophy (VVA) dyspareunia relief in breast cancer survivors. Arch. Gynecol. Obstet. 2016, 294, 841–846. [Google Scholar] [CrossRef] [PubMed]
- Pitsouni, E.; Grigoriadis, T.; Tsiveleka, A.; Zacharakis, D.; Salvatore, S.; Athanasiou, S. Microablative fractional CO2 laser therapy and the genitourinary syndrome of menopause: An observational study. Maturitas 2016, 94, 131–136. [Google Scholar] [CrossRef]
- Sokol, E.R.; Karram, M.M. An assessment of the safety and efficacy of a fractional CO2 laser system for the treatment of vulvovaginal atrophy. Menopause 2016, 23, 1102–1107. [Google Scholar] [CrossRef]
- Arroyo, C. Fractional CO2 laser treatment for vulvovaginal atrophy symptoms and vaginal rejuvenation in perimenopausal women. Int. J. Womens Health 2017, 9, 591–595. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Athanasiou, S.; Pitsouni, E.; Falagas, M.E.; Salvatore, S.; Grigoriadis, T. CO2 laser for the genitourinary syndrome of menopause. How many laser sessions? Maturitas 2017, 104, 24–28. [Google Scholar] [CrossRef]
- Behnia-Willison, F.; Sarraf, S.; Miller, J.; Mohamadi, B.; Care, A.S.; Lam, A.; Willison, N.; Behnia, L.; Salvatore, S. Safety and long-term efficacy of fractional CO2 laser treatment in women suffering from genitourinary syndrome of menopause. Eur. J. Obstet. Gynecol. Reprod. Biol. 2017, 213, 39–44. [Google Scholar] [CrossRef]
- Filippini, M.; Duca, E.D.; Negosanti, F.; Bonciani, D.; Negosanti, L.; Sannino, M.; Cannarozzo, G.; Nisticò, S.P. Fractional CO2 laser: From skin rejuvenation to vulvo-vaginal reshaping. Photomed. Laser Surg. 2017, 35, 171–175. [Google Scholar] [CrossRef]
- Pagano, I.; Gieri, S.; Nocera, F.; Scibilia, G.; Fraggetta, F.; Galia, A.; Gioè, M.; Pecorino, B.; Scollo, P. Evaluation of the CO2 laser therapy on vulvo-vaginal atrophy (VVA) in oncological patients: Preliminary results. J. Cancer Ther. 2017, 8, 452–463. [Google Scholar] [CrossRef] [Green Version]
- Pieralli, A.; Bianchi, C.; Longinotti, M.; Corioni, S.; Auzzi, N.; Becorpi, A.; Fallani, M.G.; Cariti, G.; Petraglia, F. Long-term reliability of fractioned CO2 Laser as a treatment for vulvovaginal atrophy (VVA) symptoms. Arch. Gynecol. Obstet. 2017, 296, 973–978. [Google Scholar] [CrossRef]
- Pitsouni, E.; Grigoriadis, T.; Falagas, M.; Tsiveleka, A.; Salvatore, S.; Athanasiou, S. Microablative fractional CO2 laser for the genitourinary syndrome of menopause: Power of 30 or 40 w? Lasers Med. Sci. 2017, 32, 1865–1872. [Google Scholar] [CrossRef]
- Siliquini, G.P.; Tuninetti, V.; Bounous, V.E.; Bert, F.; Biglia, N. Fractional CO2 laser therapy: A new challenge for vulvovaginal atrophy in postmenopausal women. Climacteric 2017, 20, 379–384. [Google Scholar] [CrossRef]
- Sokol, E.R.; Karram, M.M. Use of a novel fractional CO2 laser for the treatment of genitourinary syndrome of menopause: 1-year outcomes. Menopause 2017, 24, 810–814. [Google Scholar] [CrossRef]
- Becorpi, A.; Campisciano, G.; Zanotta, N.; Tredici, Z.; Guaschino, S.; Petraglia, F.; Pieralli, A.; Sisti, G.; Seta, F.D.; Comar, M. Fractional CO2 laser for genitourinary syndrome of menopause in breast cancer survivors: Clinical, immunological, and microbiological aspects. Lasers Med. Sci. 2018, 33, 1047–1054. [Google Scholar] [CrossRef]
- Cruz, V.L.; Steiner, M.L.; Pompei, L.M.; Strufaldi, R.; Fonseca, F.L.A.; Santiago, L.H.S.; Wajsfeld, T.; Fernandes, C.E. Randomized, double-blind, placebo-controlled clinical trial for evaluating the efficacy of fractional CO2 laser compared with topical estriol in the treatment of vaginal atrophy in postmenopausal women. Menopause 2018, 25, 21–28. [Google Scholar] [CrossRef]
- Eder, S.E. Early effect of fractional CO2 laser treatment in post-menopausal women with vaginal atrophy. Laser Ther. 2018, 27, 41–47. [Google Scholar] [CrossRef] [Green Version]
- Gittens, P.; Mullen, G. The effects of fractional microablative CO2 laser therapy on sexual function in postmenopausal women and women with a history of breast cancer treated with endocrine therapy. J. Cosmet. Laser Ther. 2018, 21, 127–131. [Google Scholar] [CrossRef]
- Pagano, T.; Rosa, P.D.; Vallone, R.; Schettini, F.; Arpino, G.; Giuliano, M.; Lauria, R.; Santo, I.D.; Conforti, A.; Gallo, A.; et al. Fractional microablative CO2 laser in breast cancer survivors affected by iatrogenic vulvovaginal atrophy after failure of nonestrogenic local treatments: A retrospective study. Menopause 2018, 25, 657–662. [Google Scholar] [CrossRef]
- Samuels, J.B.; Garcia, M.A. Treatment to external labia and vaginal canal with CO2 laser for symptoms of vulvovaginal atrophy in postmenopausal women. Aesthet. Surg. J. 2018, 39, 83–93. [Google Scholar] [CrossRef] [Green Version]
- Athanasiou, S.; Pitsouni, E.; Grigoriadis, T.; Zacharakis, D.; Falagas, M.E.; Salvatore, S.; Protopapas, A.; Loutradis, D. Microablative fractional CO2 laser for the genitourinary syndrome of menopause: Up to 12-month results. Menopause 2019, 26, 248–255. [Google Scholar] [CrossRef]
- Eder, S.E. Long-term safety and efficacy of fractional CO2 laser treatment in post-menopausal women with vaginal atrophy. Laser Ther. 2019, 28, 103–109. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Filippini, M.; Luvero, D.; Salvatore, S.; Pieralli, A.; Montera, R.; Plotti, F.; Candiani, M.; Angioli, R. Efficacy of fractional CO2 laser treatment in postmenopausal women with genitourinary syndrome: A multicenter study. Menopause 2019, 27, 43–49. [Google Scholar] [CrossRef] [PubMed]
- Pearson, A.; Booker, A.; Tio, M.; Marx, G. Vaginal CO2 laser for the treatment of vulvovaginal atrophy in women with breast cancer: LAAVA pilot study. Breast Cancer Res. Treat. 2019, 178, 135–140. [Google Scholar] [CrossRef]
- Politano, C.A.; Costa-Paiva, L.; Aguiar, L.B.; Machado, H.C.; Baccaro, L.F. Fractional CO2 laser versus promestriene and lubricant in genitourinary syndrome of menopause: A randomized clinical trial. Menopause 2019, 26, 833–840. [Google Scholar] [CrossRef]
- Paraiso, M.F.R.; Ferrando, C.A.; Sokol, E.R.; Rardin, C.R.; Matthews, C.A.; Karram, M.M.; Iglesia, C.B. A randomized clinical trial comparing vaginal laser therapy to vaginal estrogen therapy in women with genitourinary syndrome of menopause: The VeLVET trial. Menopause 2019, 27, 50–56. [Google Scholar] [CrossRef]
- Tovar-Huamani, J.; Mercado-Olivares, F.; Grandez-Urbina, J.A.; Pichardo-Rodriguez, R.; Tovar-Huamani, M.; García-Perdomo, H. Efficacy of fractional CO2 laser in the treatment of genitourinary syndrome of menopause in Latin-American population: First Peruvian experience. Lasers Surg. Med. 2019, 51, 509–515. [Google Scholar] [CrossRef]
- Adabi, K.; Golshahi, F.; Niroomansh, S.; Razzaghi, Z.; Ghaemi, M. Effect of the fractional CO2 laser on the quality of life, general health, and genitourinary symptoms in postmenopausal women with vaginal atrophy: A prospective cohort. J. Lasers Med. Sci. 2020, 11, 65–69. [Google Scholar] [CrossRef] [Green Version]
- Angioli, R.; Stefano, S.; Filippini, M.; Pieralli, A.; Montera, R.; Plotti, F.; Gatti, A.; Bartolone, M.; Luvero, D. Effectiveness of CO2 laser on urogenital syndrome in women with a previous gynecological neoplasia: A multicentric study. Int. J. Gynecol. Cancer 2020, 30, 590–595. [Google Scholar] [CrossRef]
- Ghanbari, Z.; Sohbati, S.; Eftekhar, T.; Sahebi, L.; Darvish, S.; Alasiri, S.; Pasikhani, M.D. Fractional CO2 laser for treatment of vulvovaginal atrophy: A short time follow-up. J. Family Reprod. Health 2020, 14, 68–73. [Google Scholar] [CrossRef]
- Li, J.; Li, H.; Zhou, Y.; Xie, M.; Miao, Y.; Wang, L.; Zhao, Y.; Ying, T.; Hu, Y.; Chen, Y.; et al. The fractional CO2 laser for the treatment of genitourinary syndrome of menopause: A prospective multicenter cohort study. Lasers Surg. Med. 2021, 53, 647–653. [Google Scholar] [CrossRef]
- Marin, J.; Lipa, G.; Dunet, E. The results of new low dose fractional CO2 laser—A prospective clinical study in France. J. Gynecol. Obstet. Hum. Reprod. 2020, 49, 101614. [Google Scholar] [CrossRef]
- Ruanphoo, P.; Bunyavejchevin, S. Treatment for vaginal atrophy using microablative fractional CO2 laser: A randomized double-blinded sham-controlled trial. Menopause 2020, 27, 858–863. [Google Scholar] [CrossRef]
- Takacs, P.; Sipos, A.G.; Kozma, B.; Cunningham, T.D.; Larson, K.; Lampé, R.; Poka, R. The effect of vaginal microablative fractional CO2 laser treatment on vaginal cytology. Lasers Surg. Med. 2020, 52, 708–712. [Google Scholar] [CrossRef]
- Sindou-Faurie, T.; Louis-Vahdat, C.; Cheikh, E.O.E.; Canlorbe, G.; Mergui, J.L.; Uzan, C.; Azaïs, H. Evaluation of the efficacy of fractional CO2 laser in the treatment of vulvar and vaginal menopausal symptoms. Arch. Gynecol. Obstet. 2020, 303, 955–963. [Google Scholar] [CrossRef]
- Salvatore, S.; Pitsouni, E.; Grigoriadis, T.; Zacharakis, D.; Pantaleo, G.; Candiani, M.; Athanasiou, S. CO2 laser and the genitourinary syndrome of menopause: A randomized sham-controlled trial. Climacteric 2020, 24, 187–193. [Google Scholar] [CrossRef] [PubMed]
- Siliquini, G.P.; Bounous, V.E.; Novara, L.; Giorgi, M.; Bert, F.; Biglia, N. Fractional CO2; vaginal laser for the genitourinary syndrome of menopause in breast cancer survivors. Breast J. 2021, 27, 448–455. [Google Scholar] [CrossRef] [PubMed]
- Jannini, E.A.; Nappi, R.E. Couplepause: A new paradigm in treating sexual dysfunction during menopause and andropause. Sex Med. Rev. 2018, 6, 384–395. [Google Scholar] [CrossRef] [PubMed]
- Nappi, R.E.; Kokot-Kierepa, M. Vaginal Health: Insights, views & attitudes (VIVA)–results from an international survey. Climacteric 2011, 15, 36–44. [Google Scholar]
- Nappi, R.E.; Palacios, S.; Bruyniks, N.; Particco, M.; Panay, N. The burden of vulvovaginal atrophy on womens daily living: Implications on quality of life from a face-to-face real-life survey. Menopause 2019, 26, 485–491. [Google Scholar] [CrossRef]
- Nappi, R.E.; Particco, M.; Biglia, N.; Cagnacci, A.; Carlo, C.D.; Luisi, S.; Paoletti, A.M. Attitudes and perceptions towards vulvar and vaginal atrophy in italian post-menopausal women: Evidence from the European REVIVE survey. Maturitas 2016, 91, 74–80. [Google Scholar] [CrossRef] [Green Version]
- Kagan, R.; Kellogg-Spadt, S.; Parish, S.J. Practical treatment considerations in the management of genitourinary syndrome of menopause. Drugs Aging 2019, 36, 897–908. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tadir, Y.; Gaspar, A.; Lev-Sagie, A.; Alexiades, M.; Alinsod, R.; Bader, A.; Calligaro, A.; Elias, J.A.; Gambaciani, M.; Gaviria, J.E.; et al. Light and energy based therapeutics for genitourinary syndrome of menopause: Consensus and controversies. Lasers Surg. Med. 2017, 49, 137–159. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- The North American Menopause Society. Management of symptomatic vulvovaginal atrophy: 2013 position statement. Menopause 2013, 20, 888–892. [Google Scholar] [CrossRef] [PubMed]
- Palacios, S.; Castelo-Branco, C.; Currie, H.; Mijatovic, V.; Nappi, R.E.; Simon, J.; Rees, M. Update on management of genitourinary syndrome of menopause: A practical guide. Maturitas 2015, 82, 308–313. [Google Scholar] [CrossRef]
- Tanzi, E.L.; Lupton, J.R.; Alster, T.S. Lasers in dermatology: Four decades of progress. J. Am. Acad Dermatol. 2003, 49, 1–34. [Google Scholar] [CrossRef]
- Xu, Y.; Deng, Y. Ablative fractional CO2 laser for facial atrophic acne scars. Facial Plast. Surg. 2018, 34, 205–219. [Google Scholar] [CrossRef]
- Ansari, F.; Sadeghi-Ghyassi, F.; Yaaghoobian, B. The clinical effectiveness and cost-effectiveness of fractional CO2 laser in acne scars and skin rejuvenation: A meta-analysis and economic evaluation. J. Cosmet. Laser Ther. 2018, 20, 248–251. [Google Scholar] [CrossRef]
- Zerbinati, N.; Serati, M.; Origoni, M.; Candiani, M.; Iannitti, T.; Salvatore, S.; Marotta, F.; Calligaro, A. Microscopic and ultrastructural modifications of postmenopausal atrophic vaginal mucosa after fractional carbon dioxide laser treatment. Lasers Med. Sci. 2014, 30, 429–436. [Google Scholar] [CrossRef]
- Salvatore, S.; França, K.; Lotti, T.; Parma, M.; Palmieri, S.; Candiani, M.; Deste, E.; Viglio, S.; Cornaglia, A.I.; Farina, A.; et al. Early regenerative modifications of human postmenopausal atrophic vaginal mucosa following fractional CO2 laser treatment. Open Access Maced. J. Med. Sci. 2018, 6, 6–14. [Google Scholar] [CrossRef] [Green Version]
- Salvatore, S.; Maggiore, U.L.R.; Athanasiou, S.; Origoni, M.; Candiani, M.; Calligaro, A.; Zerbinati, N. Histological study on the effects of microablative fractional CO2 laser on atrophic vaginal tissue. Menopause 2015, 22, 845–849. [Google Scholar] [CrossRef] [PubMed]
- Athanasiou, S.; Pitsouni, E.; Antonopoulou, S.; Zacharakis, D.; Salvatore, S.; Falagas, M.E.; Grigoriadis, T. The effect of microablative fractional CO2 laser on vaginal flora of postmenopausal women. Climacteric 2016, 19, 512–518. [Google Scholar] [CrossRef]
- Guo, J.Z.; Souders, C.; Mcclelland, L.; Anger, J.T.; Scott, V.C.; Eilber, K.S.; Ackerman, A.L. Vaginal laser treatment of genitourinary syndrome of menopause: Does the evidence support the FDA safety communication? Menopause 2020, 27, 1177–1184. [Google Scholar] [CrossRef]
- Preminger, B.A.; Kurtzman, J.S.; Dayan, E.A. Systematic review of nonsurgical vulvovaginal restoration devices: An evidence-based examination of safety and efficacy. Plast Reconstr. Surg. 2020, 146, 552e–564e. [Google Scholar] [CrossRef] [PubMed]
- Desai, A.S.; Kroumpouzos, G. Histological changes of the female genitalia using energy-based devices. In Surgical Manual of Cosmetic Medicine and Surgery; Thomas, M., James, N., Eds.; Jaypee Publishers: New Delhi, India, 2020. [Google Scholar]
- Flint, R.; Cardozo, L.; Grigoriadis, T.; Rantell, A.; Pitsouni, E.; Athanasiou, S. Rationale and design for fractional microablative CO2 laser versus photothermal non-ablative Erbium:YAG laser for the management of genitourinary syndrome of menopause: A non-inferiority, single-blind randomized controlled trial. Climacteric 2019, 22, 307–311. [Google Scholar] [CrossRef] [PubMed]
- Desai, A.S.; Vakil, Z.; Kroumpouzos, G. Transcutaneous temperature-controlled radiofrequency treatment: Improvement in female genital appearance, sexual dysfunction, and stress urinary incontinence. Aesthet. Surg. J. 2021. [Google Scholar] [CrossRef]

{kind=link}
| First Author, Year [ref] | Device Name | Study Type, Participants | Level of Evidence | Efficacy | Follow-up (mos) | Adverse Effects |
|---|---|---|---|---|---|---|
| Salvatore et al. 2014 [19] | SmartXide2 V2LR, Monalisa Touch | Prospective cohort (VVA), n = 15 | II | Dyspareunia impr (p < 0.001), other VVA symptoms (p < 0.05); VHIS (p < 0.001): FSFI in all domains (p < 0.001); SF-12: physical (p < 0.001), mental (p = 0.048) | 3 | None |
| Salvatore et al., 2014 [20] | SmartXide2 V2LR, Monalisa Touch | Prospective cohort (VVA), n = 50 | II | Vaginal dryness, burning, itching, dyspareunia impr (p < 0.001); VHIS and SF-12 (p < 0.001); 84% of pts satisfied | 3 | None |
| Salvatore et al., 2014 [21] | SmartXide2 V2LR, Monalisa Touch | Prospective cohort (GSM), n = 77 | II | VVA symptoms impr (p < 0.001); total FSFI (p < 0.001); SF-12: physical (p = 0.013), mental (p = 0.001); 17/20 pts able to resume sexual function | 3 | None |
| Perino et al. 2015 [22] | SmartXide2 V2LR, Monalisa Touch | Prospective cohort (GSM), n = 48 | II | Impr vaginal dryness, burning, itching, dyspareunia (all p < 0.0001); 91.7% of pts “satisfied’’ or “very satisfied’’; cosmetic outcome: complete vaginal resurfacing at 1-mo fu | 1 | None |
| Pagano et al. 2016 [23] | SmartXide2 V2LR, Monalisa Touch | Retrospective cohort (VVA), n = 26, BCS | III | Impr dyspareunia, dryness, itching, sensitivity during sexual intercourse (p < 0.0001) | 1 | None |
| Pieralli et al. 2016 [24] | SmartXide2 V2LR, Monalisa Touch | Prospective cohort (VVA), n = 50, BCS | II | Impr dyspareunia (p < 1.86 × 10−22), VHIS (p < 0.0001); 52% pts satisfied at 11 mos | ≤25 | None |
| Pitsouni et al., 2016 [25] | SmartXide2 V2LR, Monalisa Touch | Prospective cohort (GSM), n = 53 | II | Impr dyspareunia, dryness, burning, itching, dysuria, VMV, VHIS, FSFI; satisfaction with procedure impr (PGI-I) | 3 | Mild irritation of the introitus. |
| Sokol et Karram, 2016 [26] | SmartXide2 V2LR, Monalisa Touch | Prospective cohort (VVA), n = 30 (3 lost at fu) | II | Impr burning sensation (p = 0.018), itching (p = 0.001), vaginal dryness (p < 0.001), dyspareunia (p < 0.001), dysuria (p < 0.035), VHIS & FSFI (p < 0.001); 96% of pts “satisfied’’ or “extremely satisfied’’ | 3 | Mild-to-moderate pain, minimal bleeding. |
| Arroyo, 2017 [27] | CO2RE Intima | prospective cohort (VVA), n = 21 perimenopausal | II | VHI impr (p < 0.01); “sexual gratification’’ increased; all pts satisfied; impr “vaginal rejuvenation’’ (94%) | 8 | Mild discomfort, itching (most common). |
| Athanasiouet al, 2017 [28] | SmartXide2 V2LR, Monalisa Touch | Prospective cohort (GSM), n = 55 | II | Impr dyspareunia, dryness, VHIS (adjusted p < 0.001); 41% of pts regained normal sexual activity | 1 | Mild irritation of the introitus. |
| Behnia-Willison et al., 2017 [29] | SmartXide2 V2LR, Monalisa Touch | Prospective cohort (GSM), n = 102 | II | Impr GSM symptoms (p < 0.001); sexual function scores impr over time (p = 0.005), including dyspareunia (p = 0.002), sexual issues (p = 0.001) | 24 | Post-coital UTIs, vaginal discharge/infection, postmenopausal bleeding, lower pelvic pain |
| Filippini, et al. 2017 [30] | SmartXide2 V2LR, Monalisa Touch | Prospective cohort (VVA), n = 386 postmenopausal | II | Complete improvement of dryness, vaginal introitus pain, burning sensation, dyspareunia, itching, soreness after 3 Rxs; cosmetic effect “hypertrophic vulvar dystrophy’’ after 1st Rx and at 1-mo fu | 12 | Mild burning, discomfort during probe movement, minimum blood–serum secretions for 1–2 days, vulvar pain |
| Pagano et al. 2017 [31] | The FemiLift CO2 Laser. | Prospective cohort (VVA), n = 33, postmenopausal; VVA (n = 16) and/or SUI (n = 17) | II | Dryness, burning, dyspareunia, VHIS impr (p < 0.01); 90 % of pts satisfied with procedure, reported impr QoL | 3 | None |
| Pieralli et al. 2017 [32] | SmartXide2 V2LR, Monalisa Touch | Prospective cohort (VVA), n = 184 (128 spontaneous & 56 oncological menopause) | II | At 12, 18, 24 mos: 72%, 63%, 25% of pts satisfied, respectively; between 18–24 mos: decrease in patient satisfaction | 24 | None |
| Pitsouni et al., 2017 [33] | SmartXide2 V2LR, Monalisa Touch | Retrospective case-control (GSM), n = 50, 30-W (n = 25) vs. 40-W (n = 25) | III | Impr dyspareunia, dryness, itching/burning, FSFI, VMV, VHIS (all p < 0.001); no differences between 30- and 40-W power groups | 1 | Mild irritation, burning sensation at the introitus. |
| Siliquini et al. 2017 [34] | SmartXide2 V2LR, Monalisa Touch | Prospective cohort (VVA), n = 87 postmenopausal | II | VAS, VHI, VVHI impr at end of Rx and during fu (p < 0.001); DIVA impr (p < 0.001); 37.7% of pts very satisfied, 52.9% satisfied | 15 | None |
| Sokol et Karram, 2017 [35] | SmartXide2 V2LR, Monalisa Touch | Prospective cohort (GSM), n = 30 | II | Pain (p = 0.01), burning sensation (p = 0.007), itching (p = 0.002), vaginal dryness (p < 0.0001), dyspareunia (p < 0.0001), VHIS (p < 0.0001), FSFI (p < 0.0001) impr; no difference in SF-12; 92% of pts “satisfied’’ or extremely satisfied at 12-mo fu | 12 | Mild to moderate pain following therapy and minimal bleeding |
| Becorpi et al. 2018 [36] | SmartXide2 V2LR, Monalisa Touch | Prospective cohort (GSM), n = 20, BCS | II | Impr VHIS (p = 0.000), VRS (p range: 0.000–0.012), FSFI (p = 0.003); no difference in FSDSr (p = 0.074) | 1 | Not specified |
| Cruz et al. 2018 [37] | SmartXide2 V2LR, Monalisa Touch | RCT (GSM), n = 45, CO2 (n = 15) vs. vaginal estriol (n = 15) vs. CO2 + vaginal estriol (n = 15) comparison | I | All groups: VHIS impr (p < 0.01); laser + estriol group, and laser only group: impr dryness (p < 0.001), dyspareunia (p = 0.009), burning (p = 0.002); estriol group: dryness (p < 0.001); laser + estriol group: total FSFI impr (p = 0.02) | 5 | None |
| Eder, 2018 [38] | AcuPulse System, FemTouch Handpiece | Prospective cohort (VVA), n = 28 postmenopausal | II | VHIS and most VVA symptoms impr (p < 0.05) at 1-mo post-first Rx and during fu; FSFI (p < 0.05) | 6 | Vaginal bleeding (one episode) |
| Gittens et Mullen, 2018 [39] | SmartXide2 V2LR, Monalisa Touch | Retrospective observational (GSM), n = 25, postmenopausal (n = 17), BCS (n = 8) | lll | Impr VVA symptoms, FSDS-R, total FSFI, and all FSFI domains post-3 Rxs; no difference in sexual function improvement between postmenopausal pts and BCS treated with endocrine Rx | 1.5 | Not specified |
| Pagano et al., 2018 [40] | SmartXide2 V2LR, Monalisa Touch | Retrospective cohort (VVA), n = 82, BCS | III | Sensitivity during sexual intercourse, Impr vaginal dryness, itching, dyspareunia, dysuria (p < 0.001 for all), bleeding, probe insertion (p = 0.001 for both), movement-related pain (p = 0.011) | 1 | Persistent discomfort (3 pts discontinued Rx) |
| Samuels et Garcia, 2018 [41] | CO2RE Intima | Prospective cohort (VVA), n = 40 postmenopausal | II | Vaginal dryness, itching, dyspareunia impr (p < 0.05), VHIS (p < 0.001), FSFI (p < 0.001); 50% of pts “very satisfied”; cosmetic outcome: improvement in labial and vulvar tissue | 12 | Itching, swelling, vulvar discomfort, burning on urination, vaginal fungal infection. |
| Athanasiou et al. 2019 [42] | SmartXide2 V2LR, Monalisa Touch | Retrospective cohort (GSM), n = 94 | III | Vaginal dryness, dyspareunia impr (p < 0.001 for both), FSFI: (p < 0.001); no difference between 4 and 5 Rxs | 12 | None |
| Eder, 2019 [43] | AcuPulse System, FemTouch Handpiece | Case series (VVA), n = 20 | IV | VHIS, VAS, total FSFI impr (p < 0.05); 90% of pts were satisfied | 24 | None |
| Filippini et al., 2019 [44] | SmartXide2 V2LR, Monalisa Touch | Retrospective cohort (GSM), n = 645 | lll | Dyspareunia, vaginal orifice pain, dryness, itching, burning impr (p < 0.0001) | 1 | None |
| Pearson et al., 2019 [45] | SmartXide2 V2LR, Monalisa Touch | Prospective cohort., n = 26 (postmenopausal BCS with VVA) | ll | Vaginal dryness, itching, dyspareiunia, dysuria (p < 0.001), burning (p = 0.003), total FSFI impr (p ≤0.001) | 3 | Not specified. |
| Politano, et al., 2019 [46] | SmartXide2 V2LR, Monalisa Touch | RCT (GSM), n = 72, CO2 laser vs. vaginal promestriene vs. vaginal lubricant comparison | I | VHIS, VMI significantly higher in laser group than promestriene cream and vaginal lubricant (p < 0.001); FSFI: impr desire and lubrication domains in laser group; total FSFI: no differences among groups | 3.5 | None |
| Paraiso et al., 2019 [47] | SmartXide2 V2LR, Monalisa Touch | RCT (GSM), n = 69 (7 lost at follow up); laser (n = 30) vs. estriol cream (n = 32) comparison | l | Laser group: 85.5% of pts “better’’ or “much better’’, 78.5% “satisfied’’ or “very satisfied’’; estriol cream group: 70% “better or “much better’’, and 73.3% “satisfied or very satisfied’’; FSFI did not differ between groups; high vaginal maturation in estriol group (p = 0.02) | 6 | None |
| Tovar-Huamani et al. 2019 [48] | SmartXide2 V2LR, Monalisa Touch | Prospective cohort (GSM), n = 60 | II | Impr vaginal dryness, itching, burning, dyspareunia, dysuria, VHIS (all p < 0.001), FSFI (p = 0.001), VMV (p < 0.0001) | 4 | dysuria and urinary frequency (one patient). |
| Adabi et al. 2020 [49] | The fractional micro ablative CO2 laser system (Smaxel) | Prospective cohort (VVA), n = 140, postmenopausal | II | VHIS: vaginal resilience, fluid, epithelial integrity, and lubrication impr (p < 0.0001) FSFI: impr only in arousal and satisfaction status; QoL: impr somatic, social function, mental health components | 1 | None |
| Angioli et al., 2020 [50] | SmartXide2 V2LR, Monalisa Touch | Retrospective cohort (VVA), n = 165 | III | Impr vaginal dryness (66%), burning (66%), dyspareunia (59%), pain at introitus (54%), itching (54%) (all p < 0.00001) | 1 | None |
| Ghanbari et al., 2020 [51] | SmartXide2 V2LR, Monalisa Touch | Prospective observational (VVA), n = 47 | II | Impr vaginal dryness, dyspareunia, vaginal discharge, itching (all p <0.001). | 2 | None |
| Li et al., 2020 [52] | SmartXide2 V2LR, Monalisa Touch | Prospective cohort (GSM), n = 162; laser (n = 108) vs. estriol cream (n = 54) | ll | Laser group: VHIS (p < 0.01), VAS (p < 0.001) impr; control group: VHIS (p < 0.05), VAS (p < 0.001). At 3-, 6-mo fu: no difference between groups (p < 0.05). | 12 | None |
| Marin et al., 2020 [53] | Aphrodite | Prospective cohort (VVA), n = 50 (25 menopausal + 25 non-menopausal) | ll | Impr FSFI and QoL (p < 0.05 for both) at 3- and 6-mo fu | 6 | Mild itching, vaginal discharge, vaginal edema, “heating sensation’’. |
| Ruanphoo et Bunyavejchevin, 2020 [54] | SmartXide2 V2LR, Monalisa Touch | Double-blind RCT (VVA), n = 88 postmenopausal; laser (n = 44) vs. sham (n = 44) | I | Impr VHIS (p < 0.001), VAS (p = 0.03); more ‘‘very satisfied or satisfied’’ pts in laser group (p = 0.002) | 3 | Vaginal inflammation, pain post-procedure, vaginal bleeding. |
| Takacs et al., 2020 [55] | SmartXide2 V2LR, Monalisa Touch | Prospective cohort (VA), n = 52 (34 postmenopausal, 18 pre-menopausal) | ll | Impr vaginal dryness in both premenopausal and postmenopausal groups (p < 0.01) | 1 | Not specified |
| Sindou-Faurie et al. 2020 [56] | SmartXide2 V2LR, Monalisa Touch | Prospective cohort (GSM), n = 46 | II | Impr vaginal dryness (p = 6.34 × 10−6), dyspareunia (p = 0.001), sensitivity during intercourse (p = 0.001); pts able to achieve (p = 0.026) and maintain (p = 0.018) lubrication during coitus | 3 | “Vaginal evisceration’’ in a BCS |
| Salvatore et al. 2020 [57] | SmartXide2 V2LR, Monalisa Touch | Double-blinded RCT (GSM), n = 58, laser (n = 28) vs. sham (n = 30) | I | Laser group: vaginal dryness, dyspareunia, itching, burning, dysuria, total FSFI impr; sham group: vaginal dryness, itching, and burning impr; dyspareunia & sexual dysfunction significantly lower in laser than sham group (p < 0.05) | 4 | None |
| Siliquini et al., 2021 [58] | SmartXide2 V2LR, Monalisa Touch | Retrospective cohort (GSM), n = 135, postmenopausal, BCS (n = 45), healthy women (n = 90) | III | Both groups: VHI VVHI, dyspareunia, and vaginal dryness impr; improvement lasted up to 12-mo fu and was slower in BCS than healthy women | 12 | None |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Messas, T.; Messas, A.; Kroumpouzos, G. Carbon Dioxide Laser Vulvovaginal Rejuvenation: A Systematic Review. Cosmetics 2021, 8, 56. https://doi.org/10.3390/cosmetics8030056
Messas T, Messas A, Kroumpouzos G. Carbon Dioxide Laser Vulvovaginal Rejuvenation: A Systematic Review. Cosmetics. 2021; 8(3):56. https://doi.org/10.3390/cosmetics8030056
Chicago/Turabian StyleMessas, Tassahil, Achraf Messas, and George Kroumpouzos. 2021. "Carbon Dioxide Laser Vulvovaginal Rejuvenation: A Systematic Review" Cosmetics 8, no. 3: 56. https://doi.org/10.3390/cosmetics8030056
APA StyleMessas, T., Messas, A., & Kroumpouzos, G. (2021). Carbon Dioxide Laser Vulvovaginal Rejuvenation: A Systematic Review. Cosmetics, 8(3), 56. https://doi.org/10.3390/cosmetics8030056