
Electrocardiogram Signal Classification Based on Mix Time-Series Imaging


Abstract
:1. Introduction
- (1)
- (2)
- Employ the image classification neural network to perform feature extraction, and then through feature fusion to lessen the impact of the inherent defects of a single feature.
- (3)
- Evaluate the effectiveness of the proposed method.
- We transform the one-dimensional ECG signals into two-dimensional images to explore the nonlinearity and temporality of the raw data, opening a new direction for ECG research.
- We employ several effective networks to extract features and perform feature fusion to exploit the hidden information fully.
- To verify the proposed method, we perform extensive experiments on a classic dataset, and the results show our model demonstrates a high capability of classifying ECG signals.
2. Methods
2.1. EC-MTSI Framework Model
2.2. Mix Time-Series Imaging Method
| Algorithm 1: The pseudocode for the MTSI. |
Data: The original signal s Result: Mix-encoded three-channel image I 1 2 3 4 5 |
2.3. Feature Extraction
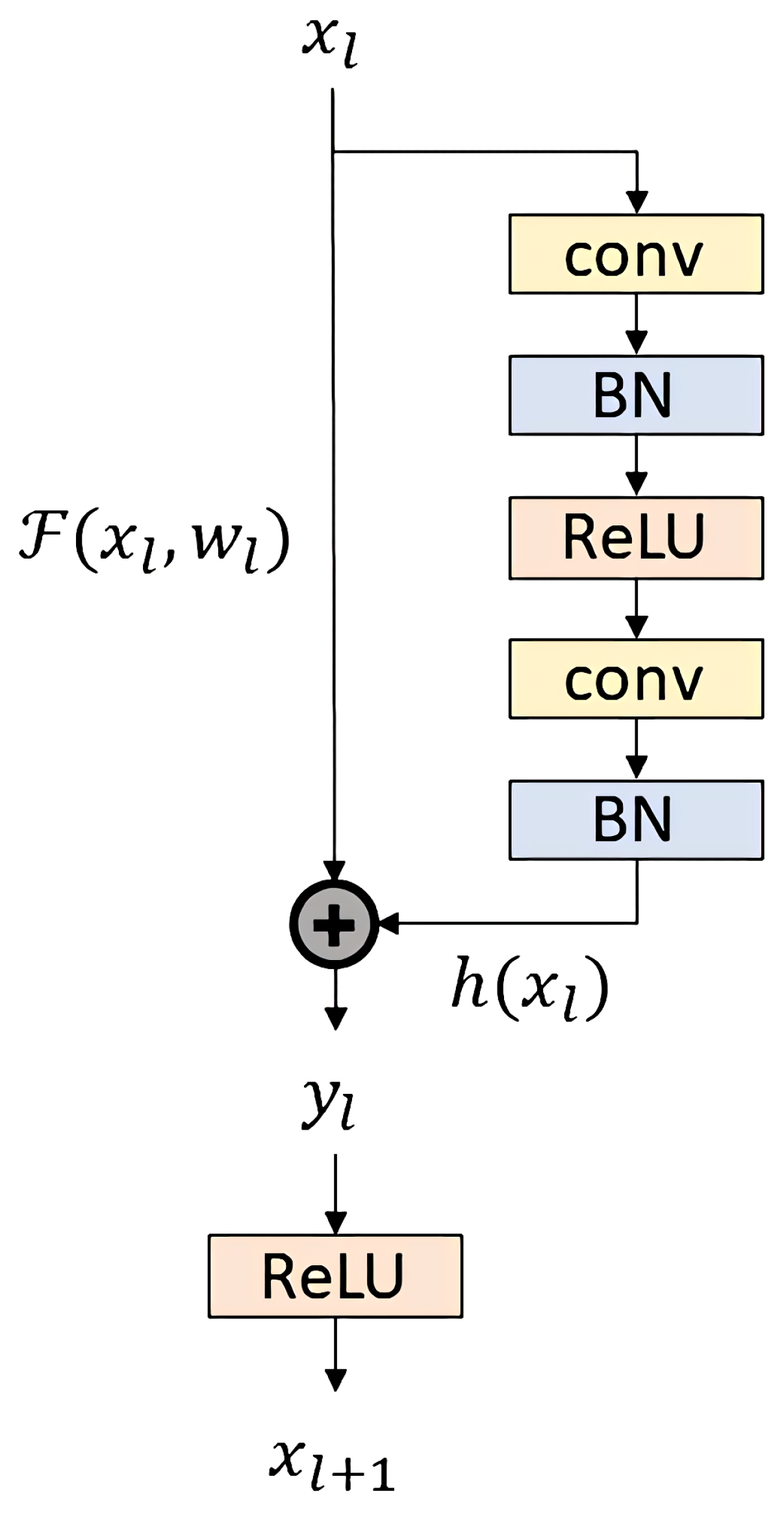
2.3.1. ECG Feature Extraction Based on ResNetV2
- ResNetV2 does not easily change the value of the “identity” branch on the left side of the residual structure. The input is consistent with the output, . Forward parameters and reverse gradients can be directly passed from shallow to deep layers without hindrance, effectively alleviating the problem of gradient disappearance during training.
- The distribution of features is no longer changed after the addition operation. In ResNetV2, is always equal to ; the ReLU at the end of ResNetV1 makes the output of the residual block always non-negative, which restricts the expressive ability of the model.
2.3.2. ECG Feature Extraction Based on DenseNet
2.4. ECG Feature Fusion
3. Experiment
3.1. Datasets and Data Pre-Processing
3.2. Experimental Evaluation Metrics
3.3. Analysis
3.3.1. Discussion of the Parameters
3.3.2. Comparison
4. Discussion
5. Conclusions and Future Work
Author Contributions
Funding
Conflicts of Interest
References
- World Health Organization. 2019 Global Health Estimates, 2000–2019; World Health Organization: Geneva, Switzerland, 2019.
- Huikuri, H.V.; Castellanos, A.; Myerburg, R.J. Sudden death due to cardiac arrhythmias. N. Engl. J. Med. 2001, 345, 1473–1482. [Google Scholar] [CrossRef]
- Hammad, M.; Iliyasu, A.M.; Subasi, A.; Ho, E.S.; Abd El-Latif, A.A. A multitier deep learning model for arrhythmia detection. IEEE Trans. Instrum. Meas. 2020, 70, 1–9. [Google Scholar] [CrossRef]
- Lazzerini, P.E.; Capecchi, P.L.; El-Sherif, N.; Laghi-Pasini, F.; Boutjdir, M. Emerging arrhythmic risk of autoimmune and inflammatory cardiac channelopathies. J. Am. Heart Assoc. 2018, 7, e010595. [Google Scholar] [CrossRef] [Green Version]
- Brouillette, J.; Cyr, S.; Fiset, C. Mechanisms of arrhythmia and sudden cardiac death in patients with HIV infection. Can. J. Cardiol. 2019, 35, 310–319. [Google Scholar] [CrossRef]
- Tuncer, T.; Dogan, S.; Pławiak, P.; Acharya, U.R. Automated arrhythmia detection using novel hexadecimal local pattern and multilevel wavelet transform with ECG signals. Knowl.-Based Syst. 2019, 186, 104923. [Google Scholar] [CrossRef]
- Sigvardsen, P.E.; Pham, M.H.; Kühl, J.T.; Fuchs, A.; Afzal, S.; Møgelvang, R.; Nordestgaard, B.G.; Køber, L.; Kofoed, K.F. Left ventricular myocardial crypts: Morphological patterns and prognostic implications. Eur. Heart J.-Cardiovasc. Imaging 2021, 22, 75–81. [Google Scholar] [CrossRef]
- Alfaras, M.; Soriano, M.C.; Ortín, S. A fast machine learning model for ECG-based heartbeat classification and arrhythmia detection. Front. Phys. 2019, 7, 103. [Google Scholar] [CrossRef] [Green Version]
- Ismail Fawaz, H.; Forestier, G.; Weber, J.; Idoumghar, L.; Muller, P.A. Deep learning for time series classification: A review. Data Min. Knowl. Discov. 2019, 33, 917–963. [Google Scholar] [CrossRef] [Green Version]
- Xing, W.; Bei, Y. Medical health big data classification based on KNN classification algorithm. IEEE Access 2019, 8, 28808–28819. [Google Scholar] [CrossRef]
- Dash, S.; Rengaswamy, R.; Venkatasubramanian, V. Fuzzy-logic based trend classification for fault diagnosis of chemical processes. Comput. Chem. Eng. 2003, 27, 347–362. [Google Scholar] [CrossRef]
- Moghimihanjani, M.; Vaferi, B. A combined wavelet transform and recurrent neural networks scheme for identification of hydrocarbon reservoir systems from well testing signals. J. Energy Resour. Technol. 2021, 143, 013001. [Google Scholar] [CrossRef]
- Ballabio, D.; Consonni, V. Classification tools in chemistry. Part 1: Linear models. PLS-DA. Anal. Methods 2013, 5, 3790–3798. [Google Scholar] [CrossRef]
- Yang, W.; Si, Y.; Wang, D.; Zhang, G. A novel method for identifying electrocardiograms using an independent component analysis and principal component analysis network. Measurement 2020, 152, 107363. [Google Scholar] [CrossRef]
- Venkatesh, N.; Jayaraman, S. Human electrocardiogram for biometrics using DTW and FLDA. In Proceedings of the 2010 20th International Conference on Pattern Recognition, Istanbul, Turkey, 23–26 August 2010; pp. 3838–3841. [Google Scholar]
- Pandey, S.K.; Janghel, R.R. ECG arrhythmia classification using artificial neural networks. In Proceedings of the 2nd International Conference on Communication, Computing and Networking, Larache, Morocco, 14–16 November 2019; pp. 645–652. [Google Scholar]
- Varatharajan, R.; Manogaran, G.; Priyan, M. A big data classification approach using LDA with an enhanced SVM method for ECG signals in cloud computing. Multimed. Tools Appl. 2018, 77, 10195–10215. [Google Scholar] [CrossRef]
- Kumari, L.; Sai, Y.P. Classification of ECG beats using optimized decision tree and adaptive boosted optimized decision tree. Signal Image Video Process. 2022, 16, 695–703. [Google Scholar]
- Pyakillya, B.; Kazachenko, N.; Mikhailovsky, N. Deep learning for ECG classification. J. Phys. Conf. Ser. 2017, 913, 012004. [Google Scholar] [CrossRef]
- Saadatnejad, S.; Oveisi, M.; Hashemi, M. LSTM-based ECG classification for continuous monitoring on personal wearable devices. IEEE J. Biomed. Health Inform. 2019, 24, 515–523. [Google Scholar] [CrossRef] [Green Version]
- Kiranyaz, S.; Ince, T.; Hamila, R.; Gabbouj, M. Convolutional neural networks for patient-specific ECG classification. In Proceedings of the 2015 37th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Milan, Italy, 25–29 August 2015; pp. 2608–2611. [Google Scholar]
- Thanaraj, K.P.; Parvathavarthini, B.; Tanik, U.J.; Rajinikanth, V.; Kadry, S.; Kamalanand, K. Implementation of deep neural networks to classify EEG signals using gramian angular summation field for epilepsy diagnosis. arXiv 2020, arXiv:2003.04534. [Google Scholar]
- Shahverdy, M.; Fathy, M.; Berangi, R.; Sabokrou, M. Driver behavior detection and classification using deep convolutional neural networks. Expert Syst. Appl. 2020, 149, 113240. [Google Scholar] [CrossRef]
- Wang, Z.; Oates, T. Imaging time-series to improve classification and imputation. In Proceedings of the Twenty-Fourth International Joint Conference on Artificial Intelligence, Buenos Aires, Argentina, 25–31 July 2015. [Google Scholar]
- Mincholé, A.; Camps, J.; Lyon, A.; Rodríguez, B. Machine learning in the electrocardiogram. J. Electrocardiol. 2019, 57, S61–S64. [Google Scholar] [CrossRef]
- Wickramaratne, S.D.; Mahmud, M.S. A deep learning based ternary task classification system using gramian angular summation field in fNIRS neuroimaging data. In Proceedings of the 2020 IEEE International Conference on E-Health Networking, Application & Services (HEALTHCOM), Shenzhen, China, 1–2 March 2021; pp. 1–4. [Google Scholar]
- Mathunjwa, B.M.; Lin, Y.T.; Lin, C.H.; Abbod, M.F.; Shieh, J.S. ECG arrhythmia classification by using a recurrence plot and convolutional neural network. Biomed. Signal Process. Control 2021, 64, 102262. [Google Scholar] [CrossRef]
- Heinen, N. Using Lightweight Image Classifiers for Electrocardiogram Classification on Embedded Devices. Bachelor’s Thesis, University of Twente, Enschede, The Netherlands, 2020. [Google Scholar]
- Marwan, N.; Wessel, N.; Meyerfeldt, U.; Schirdewan, A.; Kurths, J. Recurrence-plot-based measures of complexity and their application to heart-rate-variability data. Phys. Rev. E 2002, 66, 026702. [Google Scholar] [CrossRef] [Green Version]
- Arn, R.T.; Narayana, P.; Emerson, T.; Draper, B.A.; Kirby, M.; Peterson, C. Motion segmentation via generalized curvatures. IEEE Trans. Pattern Anal. Mach. Intell. 2018, 41, 2919–2932. [Google Scholar] [CrossRef]
- Dong, P.T. A review on image feature extraction and representation techniques. Int. J. Multimed. Ubiquitous Eng. 2013, 8, 385–396. [Google Scholar]
- He, K.; Zhang, X.; Ren, S.; Sun, J. Identity mappings in deep residual networks. In Proceedings of the European Conference on Computer Vision, Munich, Germany, 8–14 September 2016; pp. 630–645. [Google Scholar]
- Huang, G.; Liu, Z.; Van Der Maaten, L.; Weinberger, K.Q. Densely connected convolutional networks. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Honolulu, HI, USA, 21–26 July 2017; pp. 4700–4708. [Google Scholar]
- Ram Prabhakar, K.; Sai Srikar, V.; Venkatesh Babu, R. Deepfuse: A deep unsupervised approach for exposure fusion with extreme exposure image pairs. In Proceedings of the IEEE International Conference on Computer Vision, Venice, Italy, 22–29 October 2017; pp. 4714–4722. [Google Scholar]
- Chaib, S.; Liu, H.; Gu, Y.; Yao, H. Deep feature fusion for VHR remote sensing scene classification. IEEE Trans. Geosci. Remote Sens. 2017, 55, 4775–4784. [Google Scholar] [CrossRef]
- Apandi, Z.F.M.; Ikeura, R.; Hayakawa, S. Arrhythmia detection using MIT-BIH dataset: A review. In Proceedings of the 2018 International Conference on Computational Approach in Smart Systems Design and Applications (ICASSDA), Kuching, Malaysia, 15–17 August 2018; pp. 1–5. [Google Scholar]
- Goldberger, A.L.; Amaral, L.A.; Glass, L.; Hausdorff, J.M.; Ivanov, P.C.; Mark, R.G.; Mietus, J.E.; Moody, G.B.; Peng, C.K.; Stanley, H.E. PhysioBank, PhysioToolkit, and PhysioNet: Components of a new research resource for complex physiologic signals. Circulation 2000, 101, e215–e220. [Google Scholar] [CrossRef] [Green Version]
- Alizadeh, S.; Khodabakhshi, A.; Abaei Hassani, P.; Vaferi, B. Smart identification of petroleum reservoir well testing models using deep convolutional neural networks (GoogleNet). J. Energy Resour. Technol. 2021, 143, 073008. [Google Scholar] [CrossRef]
- Hatami, N.; Gavet, Y.; Debayle, J. Classification of time-series images using deep convolutional neural networks. In Proceedings of the Tenth International Conference on Machine Vision (ICMV 2017), Vienna, Austria, 13–15 November 2018; Volume 10696, p. 106960Y. [Google Scholar]
- De Lannoy, G.; François, D.; Delbeke, J.; Verleysen, M. Weighted conditional random fields for supervised interpatient heartbeat classification. IEEE Trans. Biomed. Eng. 2011, 59, 241–247. [Google Scholar] [CrossRef]
- Park, K.; Cho, B.; Lee, D.; Song, S.; Lee, J.; Chee, Y.; Kim, I.; Kim, S. Hierarchical support vector machine based heartbeat classification using higher order statistics and hermite basis function. In Proceedings of the 2008 Computers in Cardiology, Bologna, Italy, 14–17 September 2008; pp. 229–232. [Google Scholar]
- Ye, C.; Kumar, B.V.; Coimbra, M.T. Combining general multi-class and specific two-class classifiers for improved customized ECG heartbeat classification. In Proceedings of the 21st International Conference on Pattern Recognition (ICPR2012), Tsukuba, Japan, 11–15 November 2012; pp. 2428–2431. [Google Scholar]
- Zhang, Z.; Dong, J.; Luo, X.; Choi, K.S.; Wu, X. Heartbeat classification using disease-specific feature selection. Comput. Biol. Med. 2014, 46, 79–89. [Google Scholar] [CrossRef]
- Zhang, Z.; Luo, X. Heartbeat classification using decision level fusion. Biomed. Eng. Lett. 2014, 4, 388–395. [Google Scholar] [CrossRef]
- Mar, T.; Zaunseder, S.; Martínez, J.P.; Llamedo, M.; Poll, R. Optimization of ECG classification by means of feature selection. IEEE Trans. Biomed. Eng. 2011, 58, 2168–2177. [Google Scholar] [CrossRef]
- Soria, M.L.; Martínez, J. Analysis of multidomain features for ECG classification. In Proceedings of the 2009 36th Annual Computers in Cardiology Conference (CinC), Park City, UT, USA, 13–16 September 2009; pp. 561–564. [Google Scholar]
- Bazi, Y.; Alajlan, N.; AlHichri, H.; Malek, S. Domain adaptation methods for ECG classification. In Proceedings of the 2013 International Conference on Computer Medical Applications (ICCMA), Sousse, Tunisia, 20–22 January 2013; pp. 1–4. [Google Scholar]
- Lin, C.C.; Yang, C.M. Heartbeat classification using normalized RR intervals and morphological features. Math. Probl. Eng. 2014, 2014. [Google Scholar] [CrossRef]
- Zhang, H.; Cisse, M.; Dauphin, Y.N.; Lopez-Paz, D. mixup: Beyond empirical risk minimization. arXiv 2017, arXiv:1710.09412. [Google Scholar]
- Yun, S.; Han, D.; Oh, S.J.; Chun, S.; Choe, J.; Yoo, Y. Cutmix: Regularization strategy to train strong classifiers with localizable features. In Proceedings of the IEEE/CVF International Conference on Computer Vision, Seoul, Korea, 27 October–2 November 2019; pp. 6023–6032. [Google Scholar]
- Liu, Z.; Lin, Y.; Cao, Y.; Hu, H.; Wei, Y.; Zhang, Z.; Lin, S.; Guo, B. Swin transformer: Hierarchical vision transformer using shifted windows. In Proceedings of the IEEE/CVF International Conference on Computer Vision, Montreal, QC, Canada, 10–17 October 2021; pp. 10012–10022. [Google Scholar]
- Liu, Z.; Mao, H.; Wu, C.Y.; Feichtenhofer, C.; Darrell, T.; Xie, S. A convnet for the 2020s. In Proceedings of the IEEE/CVF Conference on Computer Vision and Pattern Recognition, New Orleans, LA, USA, 19–24 June 2022; pp. 11976–11986. [Google Scholar]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| AAMI Classes | Heartbeat Types |
|---|---|
| Normal beats | Normal beats, Left bundle branch block, Right bundle branch block, Atrial escape beat, Nodal (junctional) escape beat |
| Supraventricular beats | Atrial premature beat, Aberrated atrial premature beat, Nodal (junctional) premature beat, Supraventricular premature beat |
| Ventricular beats | Premature ventricular contraction, Ventricular escape beat |
| Unknown beats | Paced beat, Fusion of paced and normal beat, Unclassified beat |
| Fusion beats | The fusion of ventricular and normal beat |
| Window Size | 25 | 51 | 75 | 101 | |
|---|---|---|---|---|---|
| Polyorder | |||||
| 2 | 92.58 | 93.23 | 88.68 | 89.02 | |
| 4 | 89.02 | 90.12 | 89.02 | 89.02 |
| Transformation | Network | VEB | SVEB | Acc | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Acc | Pp | Se | Sp | Acc | Pp | Se | Sp | |||
| GAF | ResNet50V2 | 95.35 | 91.91 | 31.08 | 99.81 | 87.36 | 5.41 | 14.66 | 90.15 | 82.49 |
| RP | ResNet50V2 | 94.06 | 52.73 | 84.83 | 94.71 | 95.34 | 6.06 | 1.79 | 98.93 | 88.82 |
| TILING | ResNet50V2 | 94.8 | 56.75 | 84.02 | 95.55 | 96.14 | 22.82 | 1.85 | 99.76 | 89.84 |
| Mix | ResNet50V2 | 95.74 | 67.1 | 67.58 | 97.7 | 96.27 | 0 | 0 | 99.96 | 91.25 |
| Transformation | Network | VEB | SVEB | Acc | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Acc | Pp | Se | Sp | Acc | Pp | Se | Sp | |||
| Mix | ResNet50 | 95.57 | 67.86 | 60.18 | 98.02 | 95.66 | 12.11 | 2.78 | 99.23 | 90.57 |
| Mix | ResNet50V2 | 95.74 | 67.1 | 67.58 | 97.7 | 96.27 | 0 | 0 | 99.96 | 91.25 |
| Mix | DenseNet121 | 97.21 | 79.68 | 76.41 | 98.65 | 93.75 | 6.52 | 5.18 | 97.15 | 88.99 |
| Mix | DenseNet169 | 95.58 | 67.8 | 60.62 | 98.0 | 96.24 | 8.75 | 0.16 | 99.93 | 91.11 |
| Mix | DenseNet201 | 95.74 | 66.59 | 69.01 | 99.53 | 95.55 | 8.44 | 2.07 | 99.14 | 90.66 |
| Mix | MobileNet | 93.41 | 12.35 | 0.96 | 99.53 | 96.3 | 0 | 0 | 100 | 88.64 |
| Mix | MobileNetV2 | 93.31 | 20.79 | 1.15 | 99.7 | 96.3 | 0 | 0 | 99.99 | 88.88 |
| Mix | ResNet50V2+ DenseNet169 | 97.40 | 83.57 | 74.63 | 98.98 | 96.3 | 0 | 0 | 100 | 93.23 |
| Methods | Feature Set | Classifier | Accuracy (%) |
|---|---|---|---|
| De Lannoy et al. [40] | HBF, morphological, ECG-segments, HOS, RR intervals | Weighted conditional random fields | 85.0 |
| Park et al. [41] | HOS, HBF | Hierarchical support vector machine | 85.0 |
| Ye et al. [42] | ICA, RR interval, wavelet, PCA, morphological features | Combined support vector machine | 86.0 |
| Zhang et al. [43] | ECG segments and intervals, morphological features, RR intervals features, RR intervals, wavelet coefficients | Combined support vector machine | 86.0 |
| Zhang and Luo [44] | Morphological features, statistical features, temporal features, SFFS | Multilayer perceptron, weighted linear discriminants | 89.0 |
| Mar et al. [45] | Morphological features, RR Intervals, VCG, FFS | weighted linear discriminants | 90.0 |
| Soria and Martinez [46] | Morphological features, wavelet | Support vector machine, IWKLR, DTSVM | 93.0 |
| Bazi et al. [47] | Normalized RR interval | Weighted linear discriminants | 93.0 |
| EC-MTSI | Encoded three-channel images | Softmax | 93.7 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cai, H.; Xu, L.; Xu, J.; Xiong, Z.; Zhu, C. Electrocardiogram Signal Classification Based on Mix Time-Series Imaging. Electronics 2022, 11, 1991. https://doi.org/10.3390/electronics11131991
Cai H, Xu L, Xu J, Xiong Z, Zhu C. Electrocardiogram Signal Classification Based on Mix Time-Series Imaging. Electronics. 2022; 11(13):1991. https://doi.org/10.3390/electronics11131991
Chicago/Turabian StyleCai, Hao, Lingling Xu, Jianlong Xu, Zhi Xiong, and Changsheng Zhu. 2022. "Electrocardiogram Signal Classification Based on Mix Time-Series Imaging" Electronics 11, no. 13: 1991. https://doi.org/10.3390/electronics11131991