
Lipidomic and Metabolomic Signature of Progression of Chronic Kidney Disease in Patients with Severe Obesity

 , , , , ,
, , , , ,  , and
, and
Abstract
:1. Introduction
2. Results
2.1. Impact on the Metabolomic and Lipidomic Fingerprint in Severe Obese Individuals with Chronic Kidney Disease
2.1.1. Cohort Characterization: Body Weight and Biochemical Analyses
2.1.2. De Novo Synthesis of Phospholipids and Fatty Acid Remodeling Were Significantly Increased in Patients with CKD
2.1.3. Short Chain TG Showed a Negative Correlation with eGFR in OD Patients
2.1.4. Essential Amino Acids Are Increased in Obese Patients with CKD
2.2. Bariatric Surgery Improves the Serum Lipidomic Profile and Metabolomic Fingerprint in Obese Patients with CKD
2.2.1. Diglycerides and Medium-Chain Triglycerides Presented a Positive Correlation with Uric Acid in Obese Patients with CKD after Surgery
2.2.2. Isoleucine and Proline Decreased in the Serum of CKD Patients with Obesity after Bariatric Surgery
2.3. Bariatric Surgery Decreased Levels of Valine and Glutamine in Urine from Patients with CKD
3. Discussion
4. Materials and Methods
4.1. Study Cohort
4.1.1. Bariatric Surgery
4.1.2. Clinical Parameters Tests
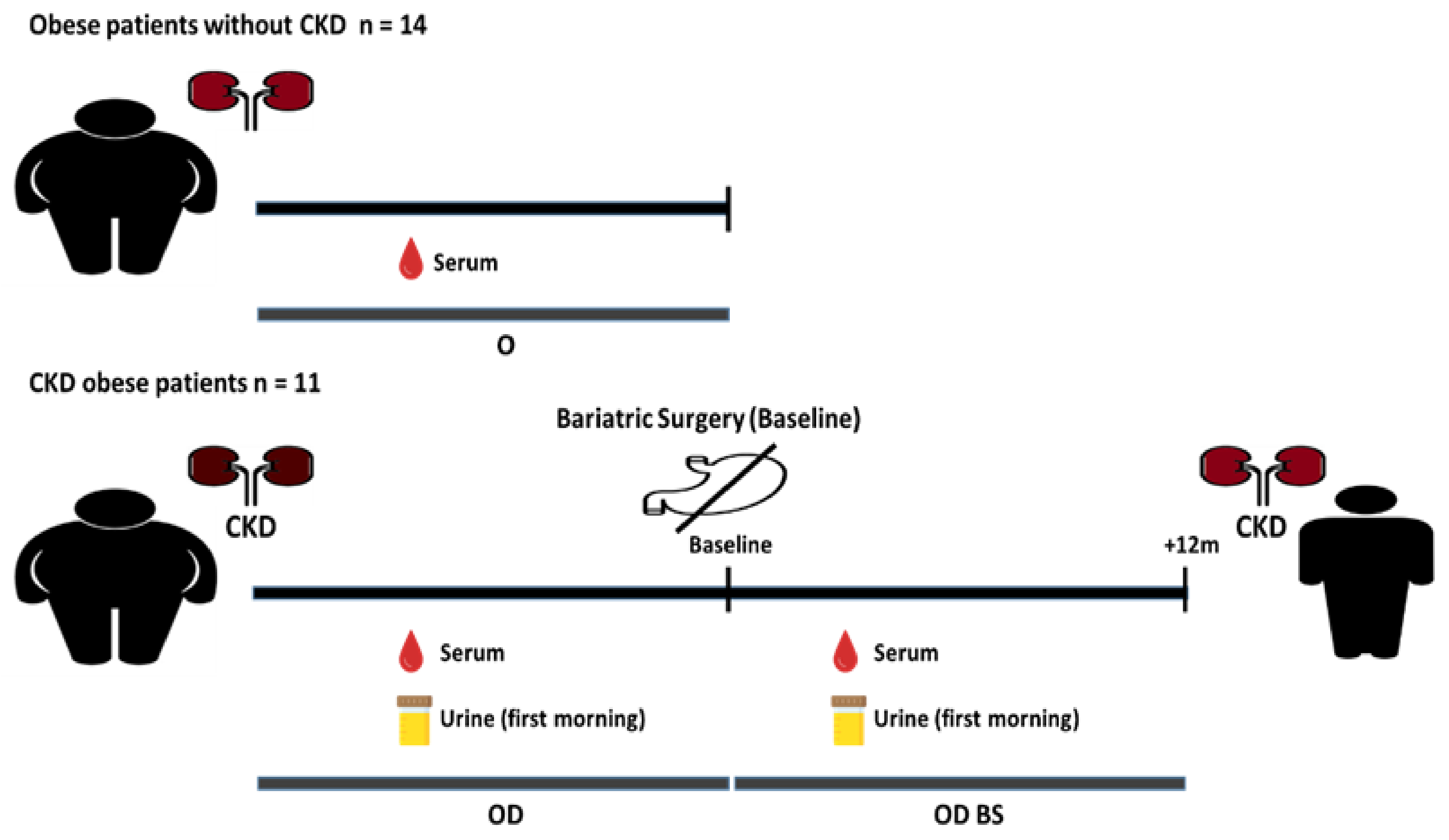
4.1.3. Study Design
4.1.4. Samples Collection
4.2. Lipidomic Untargeted Analysis in Serum Samples by Liquid Chromatography Coupled to Mass Spectrometry (LC-MS)
4.2.1. Lipidomic Extraction, Sample Preparation
4.2.2. UHPLC-ESI-Q-TOF-MS Analysis
4.2.3. MS Signals Processing
4.2.4. Data Pre-Treatment
4.2.5. Statistical Analysis
4.2.6. Annotation of Unknown Features
4.3. Polar Metabolites Untargeted Analysis in Serum and Urine Samples by Gas Chromatography Coupled to High-Resolution Accurate Mass Spectrometry (GC-HRAM-MS)
4.3.1. Extraction of Polar Metabolites, Sample Preparation
4.3.2. GC-HRAM-MS Analysis
4.3.3. MS Signals Processing for Serum Samples
4.3.4. MS Signals Processing for Urine Samples
4.3.5. Data Pre-Treatment
4.3.6. Statistical Analysis
4.3.7. Annotation of Unknown Features
4.4. Correlation, Curve ROC Test Analyses and Heatmaps
4.5. Lipidomic and Amino Acid Pathways
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Di Cesare, M.; Bentham, J.; Stevens, G.A.; Zhou, B.; Danaei, G.; Lu, Y.; Bixby, H.; Cowan, M.J.; Riley, L.M.; Hajifathalian, K.; et al. Trends in adult body-mass index in 200 countries from 1975 to 2014: A pooled analysis of 1698 population-based measurement studies with 19.2 million participants. Lancet 2016, 387, 1377–1396. [Google Scholar] [CrossRef] [Green Version]
- Meldrum, D.R.; Morris, M.A.; Gambone, J.C. Obesity pandemic: Causes, consequences, and solutions—but do we have the will? Fertil. Steril. 2017, 107, 833–839. [Google Scholar] [CrossRef] [Green Version]
- Sharma, I.; Liao, Y.; Zheng, X.; Kanwar, Y.S. New Pandemic: Obesity and Associated Nephropathy. Front. Med. 2021, 8, 673556. [Google Scholar] [CrossRef] [PubMed]
- Kovesdy, C.P.; Furth, S.L.; Zoccali, C. Obesity and Kidney Disease: Hidden Consequences of the Epidemic. Can. J. Kidney Health Dis. 2017, 4, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Melsom, T.; Mathisen, U.D.; Ingebretsen, O.C.; Jenssen, T.G.; Njølstad, I.; Solbu, M.D.; Toft, I.; Eriksen, B.O. Impaired fasting glucose is associated with renal hyperfiltration in the general population. Diabetes Care 2011, 34, 1546–1551. [Google Scholar] [CrossRef] [Green Version]
- Adair, K.E.; Bowden, R.G. Ameliorating chronic kidney disease using a whole food plant-based diet. Nutrients 2020, 12, 1007. [Google Scholar] [CrossRef] [Green Version]
- Zhao, Y.Y.; Lin, R.C. Metabolomics in Nephrotoxicity. In Advances in Clinical Chemistry, 1st ed.; Elsevier Inc.: Amsterdam, The Netherlands, 2014; Volume 65. [Google Scholar] [CrossRef]
- Graessler, J.; Schwudke, D.; Schwarz, P.E.H.; Herzog, R.; Schevchenko, A.; Bornstein, S.R. Top-down lipidomics reveals ether lipid deficiency in blood plasma of hypertensive patients. PLoS ONE 2009, 4, e6261. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Y.; Vaziri, N.D.; Lin, R. Lipidomics: New Insight Into Kidney Disease. In Advances in Clinical Chemistry, 1st ed.; Elsevier Inc.: Amsterdam, The Netherlands, 2015; Volume 68. [Google Scholar] [CrossRef]
- Docherty, N.G.; le Roux, C.W. Bariatric surgery for the treatment of chronic kidney disease in obesity and type 2 diabetes mellitus. Nat. Rev. Nephrol. 2020, 16, 709–720. [Google Scholar] [CrossRef]
- Sjöström, L.; Lindroos, A.K.; Peltonen, M.; Torgerson, J.; Bouchard, C.; Carlsson, B.; Dahlgren, S.; Larsson, B.; Narbro, K.; Sjöström, C.D.; et al. Lifestyle, diabetes, and cardiovascular risk factors 10 years after bariatric surgery. N. Engl. J. Med. 2004, 351, 2683–2693. [Google Scholar] [CrossRef]
- Morales, E.; Porrini, E.; Martin-Taboada, M.; Luis-Lima, S.; Vila-Bedmar, R.; González de Pablos, I.; Gómez, P.; Rodríguez, E.; Torres, L.; Lanzón, B.; et al. Renoprotective role of bariatric surgery in patients with established chronic kidney disease. Clin. Kidney J. 2020, 14, 2037–2046. [Google Scholar] [CrossRef] [PubMed]
- Ting, S.M.S.; Nair, H.; Ching, I.; Taheri, S.; Dasgupta, I. Overweight, obesity and chronic kidney disease. Nephron Clin. Pract. 2009, 112, 121–127. [Google Scholar] [CrossRef]
- Chertow, G.M.; Hsu, C.Y.; Johansen, K.L. The enlarging body of evidence: Obesity and chronic kidney disease. J. Am. Soc. Nephrol. 2006, 17, 1501–1502. [Google Scholar] [CrossRef] [Green Version]
- Yim, H.E.; Yoo, K.H. Obesity and chronic kidney disease: Prevalence, mechanism, and management. Clin. Exp. Pediatrics 2021, 64, 511–518. [Google Scholar] [CrossRef]
- Jung, U.J.; Choi, M.S. Obesity and its metabolic complications: The role of adipokines and the relationship between obesity, inflammation, insulin resistance, dyslipidemia and nonalcoholic fatty liver disease. Int. J. Mol. Sci. 2014, 15, 6184–6223. [Google Scholar] [CrossRef] [Green Version]
- Escasany, E.; Izquierdo-Lahuerta, A.; Medina-Gomez, G. Underlying mechanisms of renal lipotoxicity in obesity. Nephron 2019, 143, 28–32. [Google Scholar] [CrossRef]
- Gai, Z.; Wang, T.; Visentin, M.; Kullak-Ublick, G.A.; Fu, X.; Wang, Z. Lipid accumulation and chronic kidney disease. Nutrients 2019, 11, 722. [Google Scholar] [CrossRef] [Green Version]
- Toth, P.P.; Philip, S.; Hull, M.; Granowitz, C. Elevated Triglycerides (≥150 mg/dL) and High Triglycerides (200–499 mg/dL) Are Significant Predictors of Hospitalization for New-Onset Kidney Disease: A Real-World Analysis of High-Risk Statin-Treated Patients. Cardiorenal Med. 2019, 9, 400–407. [Google Scholar] [CrossRef] [PubMed]
- Tsuruya, K.; Yoshida, H.; Nagata, M.; Kitazono, T.; Iseki, K.; Iseki, C.; Fujimoto, S.; Konta, T.; Moriyama, T.; Yamagata, K.; et al. Impact of the triglycerides to high-density lipoprotein cholesterol ratio on the incidence and progression of CKD: A longitudinal study in a large Japanese population. Am. J. Kidney Dis. 2015, 66, 972–983. [Google Scholar] [CrossRef] [PubMed]
- Vaziri, N.D. HDL abnormalities in nephrotic syndrome and chronic kidney disease. Nat. Rev. Nephrol. 2016, 12, 37–47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bandet, C.L.; Tan-Chen, S.; Bourron, O.; Le Stunff, H.; Hajduch, E. Sphingolipid metabolism: New insight into ceramide-induced lipotoxicity in muscle cells. Int. J. Mol. Sci. 2019, 20, 479. [Google Scholar] [CrossRef] [Green Version]
- Sieber, J.; Weins, A.; Kampe, K.; Gruber, S.; Lindenmeyer, M.T.; Cohen, C.D.; Orellana, J.M.; Mundel, P.; Jehle, A.W. Susceptibility of podocytes to palmitic acid is regulated by stearoyl-CoA desaturases 1 and 2. Am. J. Pathol. 2013, 183, 735–744. [Google Scholar] [CrossRef] [Green Version]
- Ferro, C.J.; Mark, P.B.; Kanbay, M.; Sarafidis, P.; Heine, G.H.; Rossignol, P.; Massy, Z.A.; Mallamaci, F.; Valdivielso, J.M.; Malyszko, J.; et al. Lipid management in patients with chronic kidney disease. Nat. Rev. Nephrol. 2018, 14, 727–749. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, H.; Cao, G.; Chen, D.Q.; Wang, M.; Vaziri, N.D.; Zhang, Z.H.; Mao, J.-R.; Bai, X.; Zhao, Y.-Y. Metabolomics insights into activated redox signaling and lipid metabolism dysfunction in chronic kidney disease progression. Redox Biol. 2016, 10, 168–178. [Google Scholar] [CrossRef] [Green Version]
- Yang, W.L.; Bai, Q.; Li, D.D.; A, T.-L.; Wang, S.; Zhao, R.S.; Nie, H.G.; Zhang, A.-H.; Wang, T.; Fan, M.-H. Changes of urinary phospholipids in the chronic kidney disease patients. Biomarkers 2013, 18, 601–606. [Google Scholar] [CrossRef]
- Michalczyk, A.; Dołȩgowska, B.; Heryć, R.; Chlubek, D.; Safranow, K. Associations between plasma lysophospholipids concentrations, chronic kidney disease and the type of renal replacement therapy. Lipids Health Dis. 2019, 18, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Strazzella, A.; Ossoli, A.; Calabresi, L. High-Density Lipoproteins and the Kidney. Cells 2021, 10, 764. [Google Scholar] [CrossRef]
- Mantovani, A.; Lunardi, G.; Bonapace, S.; Dugo, C.; Altomari, A.; Molon, G.; Conti, A.; Bovo, C.; Laaksonen, R.; Byrne, C.D.; et al. Association between increased plasma ceramides and chronic kidney disease in patients with and without ischemic heart disease. Diabetes Metab. 2021, 47, 101152. [Google Scholar] [CrossRef]
- Turner, N.; Lim, X.Y.; Toop, H.D.; Osborne, B.; Brandon, A.E.; Taylor, E.N.; Fiveash, C.E.; Govindaraju, H.; Teo, J.D.; McEwen, H.P.; et al. A selective inhibitor of ceramide synthase 1 reveals a novel role in fat metabolism. Nat. Commun. 2018, 9, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Hartmann, D.; Lucks, J.; Fuchs, S.; Schiffmann, S.; Schreiber, Y.; Ferreirós, N.; Merkens, J.; Marschalek, R.; Geisslinger, G.; Grösch, S. Long chain ceramides and very long chain ceramides have opposite effects on human breast and colon cancer cell growth. Int. J. Biochem. Cell Biol. 2012, 44, 620–628. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.S.; Liang, S.; Zong, M.H.; Yang, J.G.; Lou, W.Y. Microbial synthesis of functional odd-chain fatty acids: A review. World J. Microbiol. Biotechnol. 2020, 36, 1–9. [Google Scholar] [CrossRef]
- Rangel-Huerta, O.D.; Pastor-Villaescusa, B.; Gil, A. Are we close to defining a metabolomic signature of human obesity? A systematic review of metabolomics studies. Metabolomics 2019, 15, 93. [Google Scholar] [CrossRef] [Green Version]
- Arneth, B.; Arneth, R.; Shams, M. Metabolomics of type 1 and type 2 diabetes. Int. J. Mol. Sci. 2019, 20, 2467. [Google Scholar] [CrossRef] [Green Version]
- Maggioni, A.P.; Maseri, A.; Fresco, C.; Franzosi, M.G.; Mauri, F.; Santoro, E.; Tognoni, G. Age-related increase in mortality among patients with first myocardial infarctions treated with thrombolysis. N. Engl. J. Med. 1993, 329, 1442–1448. [Google Scholar] [CrossRef]
- Newgard, C.B.; An, J.; Bain, J.R.; Muehlbauer, M.J.; Stevens, R.D.; Lien, L.F.; Haqq, A.M.; Shah, S.H.; Arlotto, M.; Slentz, C.A.; et al. A BCAA Related Metabolic Signature that differentiates obese and lean humans and contributes to insulin resistance. Cell Metab. 2009, 9, 311–326. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mahbub, M.H.; Yamaguchi, N.; Hase, R.; Takahashi, H.; Ishimaru, Y.; Watanabe, R.; Saito, H.; Shimokawa, J.; Yamamoto, H.; Kikuchi, S.; et al. Plasma branched-chain and aromatic amino acids in relation to hypertension. Nutrients 2020, 12, 3791. [Google Scholar] [CrossRef]
- Jia, Z. Impaired Citric Acid Cycle in Nondiabetic Chronic Kidney Disease. EBioMedicine 2017, 26, 6–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mika, A.; Stepnowski, P.; Kaska, L.; Proczko, M.; Wisniewski, P.; Sledzinski, M.; Sledzinski, T. A comprehensive study of serum odd- and branched-chain fatty acids in patients with excess weight. Obesity 2016, 24, 1669–1676. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jenkins, B.; West, J.A.; Koulman, A. A review of odd-chain fatty acid metabolism and the role of pentadecanoic acid (C15:0) and heptadecanoic acid (C17:0) in health and disease. Molecules 2015, 20, 2425–2444. [Google Scholar] [CrossRef] [Green Version]
- Asztalos, B.F.; Swarbrick, M.M.; Schaefer, E.J.; Dallal, G.E.; Horvath, K.V.; Ai, M.; Stanhope, K.L.; Austrheim-Smith, I.; Wolfe, B.M.; Havel, P.J.; et al. Effects of weight loss, induced by gastric bypass surgery, on HDL remodeling in obese women. J. Lipid Res. 2010, 51, 2405–2412. [Google Scholar] [CrossRef]
- Shah, S.H.; Crosslin, D.R.; Haynes, C.S.; Nelson, S.; Turer, C.B.; Stevens, R.D.; Muehlbauer, M.J.; Wenner, B.R.; Bain, J.R.; Laferrère, B.; et al. Branched-chain amino acid levels are associated with improvement in insulin resistance with weight loss. Diabetologia 2012, 55, 321–330. [Google Scholar] [CrossRef] [Green Version]
- Cummings, N.E.; Williams, E.M.; Kasza, I.; Konon, E.N.; Schaid, M.D.; Schmidt, B.A.; Poudel, C.; Sherman, D.S.; Yu, D.; Arriola Apelo, S.I.; et al. Restoration of metabolic health by decreased consumption of branched-chain amino acids. J. Physiol. 2018, 596, 623–645. [Google Scholar] [CrossRef] [Green Version]
- Li, Y.; Deng, H.; Ju, L.; Zhang, X.; Zhang, Z.; Yang, Z.; Wang, L.; Hou, Z.; Zhang, Y. Screening and validation for plasma biomarkers of nephrotoxicity based on metabolomics in male rats. Toxicol. Res. 2015, 5, 259–267. [Google Scholar] [CrossRef]
- Turgeon, N.A.; Perez, S.; Mondestin, M.; Davis, S.S.; Lin, E.; Tata, S.; Kirk, A.D.; Larsen, C.P.; Pearson, T.C.; Sweeney, J.F. The impact of renal function on outcomes of bariatric surgery. J. Am. Soc. Nephrol. 2012, 23, 885–894. [Google Scholar] [CrossRef] [Green Version]
- Witte, E.C.; Heerspink, H.J.L.; De Zeeuw, D.; Bakker, S.J.L.; De Jong, P.E.; Gansevoort, R. First morning voids are more reliable than spot urine samples to assess microalbuminuria. J. Am. Soc. Nephrol. 2009, 20, 436–443. [Google Scholar] [CrossRef] [Green Version]
- Bi, H.; Guo, Z.; Jia, X.; Liu, H.; Ma, L.; Xue, L. The key points in the pre-analytical procedures of blood and urine samples in metabolomics studies. Metabolomics 2020, 16, 1–15. [Google Scholar] [CrossRef]
- Duranton, F.; Lundin, U.; Gayrard, N.; Mischak, H.; Aparicio, M.; Mourad, G.; Daurès, J.P.; Weinberger, K.M.; Argilés, À. Plasma and urinary amino acid metabolomic profiling in patients with different levels of kidney function. Clin. J. Am. Soc. Nephrol. 2014, 9, 37–45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yu, T.H.; Tang, W.H.; Lu, Y.C.; Wang, C.P.; Hung, W.C.; Wu, C.C.; Tsai, I.-T.; Chung, F.-M.; Houng, H.-Y.; Lan, W.-C.; et al. Association between hippuric acid and left ventricular hypertrophy in maintenance hemodialysis patients. Clin. Chim. Acta 2018, 484, 47–51. [Google Scholar] [CrossRef] [PubMed]
- Groth, T.; Tengström, B. A simple method for the estimation of glomerular filtration rate. Scand. J. Clin. Lab. Investig. 1977, 37, 39–47. [Google Scholar] [CrossRef]
- Means, J.H. Basal Metabolism and Body Surface. J. Biol. Chem. 1915, 21, 263–268. [Google Scholar] [CrossRef]
- O’Gorman, A.; Suvitaival, T.; Ahonen, L.; Cannon, M.; Zammit, S.; Lewis, G.; Roche, H.M.; Mattila, I.; Hyotylainen, T.; Oresic, M.; et al. Identification of a plasma signature of psychotic disorder in children and adolescents from the Avon Longitudinal Study of Parents and Children (ALSPAC) cohort. Transl. Psychiatry 2017, 7, e1240. [Google Scholar] [CrossRef] [Green Version]
- Folch, J.; Lees, M.; Sloane, G.H.S. A simple method for the isolation and purification of total lipides from animal tissues. J. Biol. Chem. 1957, 226, 497–509. [Google Scholar] [CrossRef]
- Pluskal, T.; Castillo, S.; Villar-Briones, A.; Orešič, M. MZmine 2: Modular framework for processing, visualizing, and analyzing mass spectrometry-based molecular profile data. BMC Bioinform. 2010, 11, 395. [Google Scholar] [CrossRef] [Green Version]
- Gonzalez-Riano, C.; León-Espinosa, G.; Regalado-Reyes, M.; García, A.; Defelipe, J.; Barbas, C. Metabolomic Study of Hibernating Syrian Hamster Brains: In Search of Neuroprotective Agents. J. Proteome Res. 2019, 18, 1175–1190. [Google Scholar] [CrossRef] [PubMed]
- Ruttkies, C.; Schymanski, E.L.; Wolf, S.; Hollender, J.; Neumann, S. MetFrag relaunched: Incorporating strategies beyond in silico fragmentation. J. Cheminform. 2016, 8, 1–16. [Google Scholar] [CrossRef] [Green Version]
- Wishart, D.S.; Feunang, Y.D.; Marcu, A.; Guo, A.C.; Liang, K.; Vázquez-Fresno, R.; Sajed, T.; Johnson, D.; Li, C.; Karu, N.; et al. HMDB 4.0: The human metabolome database for 2018. Nucleic Acids Res. 2018, 46, D608–D617. [Google Scholar] [CrossRef]
- Godzien, J.; Ciborowski, M.; Martínez-Alcázar, M.P.; Samczuk, P.; Kretowski, A.; Barbas, C. Rapid and Reliable Identification of Phospholipids for Untargeted Metabolomics with LC-ESI-QTOF-MS/MS. J. Proteome Res. 2015, 14, 3204–3216. [Google Scholar] [CrossRef]
- Godzien, J.; Ciborowski, M.; Whiley, L.; Legido-Quigley, C.; Ruperez, F.J.; Barbas, C. In-vial dual extraction liquid chromatography coupled to mass spectrometry applied to streptozotocin-treated diabetic rats. Tips and pitfalls of the method. J. Chromatogr. A 2013, 1304, 52–60. [Google Scholar] [CrossRef]
- Castillo, S.; Mattila, I.; Miettinen, J.; Orešič, M.; Hyötyläinen, T. Data analysis tool for comprehensive two-dimensional gas chromatography/time-of-flight mass spectrometry. Anal. Chem. 2011, 83, 3058–3067. [Google Scholar] [CrossRef]
- Castro-Alves, V.; Kalbina, I.; Nilsen, A.; Aronsson, M.; Rosenqvist, E.; Jansen, M.A.K.; Qian, M.; Öströmb, Å.; Hyötyläinen, T.; Strid, Å. Integration of non-target metabolomics and sensory analysis unravels vegetable plant metabolite signatures associated with sensory quality: A case study using dill (Anethum graveolens). Food Chem. 2021, 344, 128714. [Google Scholar] [CrossRef] [PubMed]
- Smirnov, A.; Qiu, Y.; Jia, W.; Walker, D.I.; Jones, D.P.; Du, X. ADAP-GC 4.0: Application of Clustering-Assisted Multivariate Curve Resolution to Spectral Deconvolution of Gas Chromatography-Mass Spectrometry Metabolomics Data. Anal. Chem. 2019, 91, 9069–9077. [Google Scholar] [CrossRef] [PubMed]
- Dieterle, F.; Ross, A.; Senn, H. Probabilistic Quotient Normalization as Robust method to aacount for dilution of complex biuological mixtures. Anal. Chem. 2006, 78, 4281–4290. [Google Scholar] [CrossRef] [PubMed]
- Hummel, J.; Strehmel, N.; Bölling, C.; Schmidt, S.; Walther, D.; Kopka, J. Mass Spectral Search and Analysis Using the Golm Metabolome Database. In The Handbook of Plant Metabolomics; Wiley: Hoboken, NJ, USA, 2013; pp. 321–343. [Google Scholar] [CrossRef]
- Chong, J.; Wishart, D.S.; Xia, J. Using MetaboAnalyst 4.0 for Comprehensive and Integrative Metabolomics Data Analysis. Curr. Protoc. Bioinform. 2019, 68, e86. [Google Scholar] [CrossRef] [PubMed]
- Slenter, D.N.; Kutmon, M.; Hanspers, K.; Riutta, A.; Windsor, J.; Nunes, N.; Mélius, J.; Cirillo, E.; Coort, S.L.; Digles, D.; et al. WikiPathways: A multifaceted pathway database bridging metabolomics to other omics research. Nucleic Acids Res. 2018, 46, D661–D667. [Google Scholar] [CrossRef] [PubMed]
- Mathews, C.K.; van Holde, K.E. Biochemistry; Pearson: New York, NY, USA, 2012. [Google Scholar]
- Sud, M.; Fahy, E.; Cotter, D.; Azam, K.; Vadivelu, I.; Burant, C.; Edison, A.; Fiehn, O.; Higashi, R.; Sreekumaran Nair, K.; et al. Metabolomics Workbench: An international repository for metabolomics data and metadata, metabolite standards, protocols, tutorials and training, and analysis tools. Nucleic Acids Res. 2016, 44, D463–D470. [Google Scholar] [CrossRef] [PubMed] [Green Version]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group | |||
|---|---|---|---|
| Parameters | Patients without CKD | CKD Patients | |
| CKD Patients before BS | CKD Patients after BS | ||
| Acronym | O | OD | OD BS |
| n | 14 | 11 | |
| Age (years), mean ± SD (range) | 51.76 ± 10.92 (35–66) | 53.09 ± 15.16 (29–71) | 54.09 ± 15.16 |
| Gender (Male/Female) (%) | 38.47/61.53 | 66.64/33.36 | 66.64/33.36 |
| Body weight (kg), mean ± SD (range) | 120.51 ± 16.96 (84–152) | 116.72 ± 25.33 (93.5–170) | 81.07 ± 22.42 (65–125) # |
| BMI (kg/m2), mean ± SD (range) | 42.9 ± 3.72 (36.48–50.0) | 41.9 ± 5.98 (36.6–53.3) | 28.6 ± 5.69 (22.68–39.78) # |
| Diabetes mellitus (%) | 28.6 | 63.6 | 9.1 |
| Hypertension (%) | 35.7 | 90.9 | 63.6 |
| Lipid-lowering drugs (%) | 14.3 | 63.6 | 18.1 |
| Glucose (mg/dL), median (range) | 100 (79–171) | 174 (98–299) * | 86 (67–141) # |
| HbA1c (%), mean ± SD | 6.02 ± 0.72 | 7.46 ± 1.81 * | 5.55 ± 0.83 # |
| Cholesterol (mg/dL), mean ± SD | 183 ± 34.74 | 194 ± 49.62 | 160 ± 41.70 # |
| HDL (mg/dL), median (range) | 45.9 (35.0–94.0) | 35 (21.6–57.3) * | 45 (27–78) # |
| LDL (mg/dL), mean ± SD | 103.63 ± 26.19 | 98.50 ± 37.70 | 89.27 ± 37.85 |
| TG (mg/dL), mean ± SD | 183.46 ± 126.29 | 314.54 ± 106.16 * | 116.36 ± 45.82 # |
| Uric acid (mg/dL), mean ± SD | 5.52 ± 0.83 | 7.10 ± 1.69 * | 5.64 ± 1.10 # |
| Serum Creatinine (mg/dL), mean ± SD | 0.80 ± 0.18 | 1.16 ± 0.43 * | 1.03 ± 0.39 |
| eGFR (mL/min), mean ± SD | 94.18 ± 20.35 | 73.02 ± 30.76 * | 80.72 ± 31.02 |
| Proteinuria (g/24 h), median (range) | 0.14 (0.10–0.53) | 1.48 (0.77–11.40) * | 0.68 (0.34–3.78) # |
| UACR (mg/g), median (range) | 7.6 (3.6–110.4) | 1004 (158.0–6825) * | 321.79 (38.69–3104) # |
| O | OD | |||
|---|---|---|---|---|
| Highlighted | Relationship | Highlighted | Relationship | |
| Glucose | Cer, PE, LysoPC, DG, TG | Positive | — | — |
| Cholesterol | Cer, PS, PC | Positive | TG | Positive |
| LDL | — | — | LysoPC | Positive |
| Uric Acid | LysoPC, PC | Positive | TG | Positive |
| Creatinine | SM, PC, LysoPC, TG | Negative SM, Positive PC, LysoPC, TG | TG | Positive |
| eGFR | — | — | TG | Negative |
| Proteinuria | — | — | DG, TG | Positive |
| UACR | SM, PC | Positive | — | — |
| OD BS | OD | |||
|---|---|---|---|---|
| Highlighted | Relationship | Highlighted | Relationship | |
| Glucose | — | — | — | — |
| Cholesterol | SM, LysoPC, PI | Positive | TG | Positive |
| LDL | SM | Positive | LysoPC | Positive |
| Uric Acid | DG, TG (medium) | Positive | TG (short) | Positive |
| Creatinine | — | — | TG | Positive |
| eGFR | — | — | TG | Negative |
| Proteinuria | — | — | DG, TG | Positive |
| UACR | — | — | — | — |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lanzon, B.; Martin-Taboada, M.; Castro-Alves, V.; Vila-Bedmar, R.; González de Pablos, I.; Duberg, D.; Gomez, P.; Rodriguez, E.; Orešič, M.; Hyötyläinen, T.; et al. Lipidomic and Metabolomic Signature of Progression of Chronic Kidney Disease in Patients with Severe Obesity. Metabolites 2021, 11, 836. https://doi.org/10.3390/metabo11120836
Lanzon B, Martin-Taboada M, Castro-Alves V, Vila-Bedmar R, González de Pablos I, Duberg D, Gomez P, Rodriguez E, Orešič M, Hyötyläinen T, et al. Lipidomic and Metabolomic Signature of Progression of Chronic Kidney Disease in Patients with Severe Obesity. Metabolites. 2021; 11(12):836. https://doi.org/10.3390/metabo11120836
Chicago/Turabian StyleLanzon, Borja, Marina Martin-Taboada, Victor Castro-Alves, Rocio Vila-Bedmar, Ignacio González de Pablos, Daniel Duberg, Pilar Gomez, Elias Rodriguez, Matej Orešič, Tuulia Hyötyläinen, and et al. 2021. "Lipidomic and Metabolomic Signature of Progression of Chronic Kidney Disease in Patients with Severe Obesity" Metabolites 11, no. 12: 836. https://doi.org/10.3390/metabo11120836