

Metabolic Impact of Frailty Changes Diabetes Trajectory
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Diabetes and Frailty
3. Diabetogenic Effects of Ageing
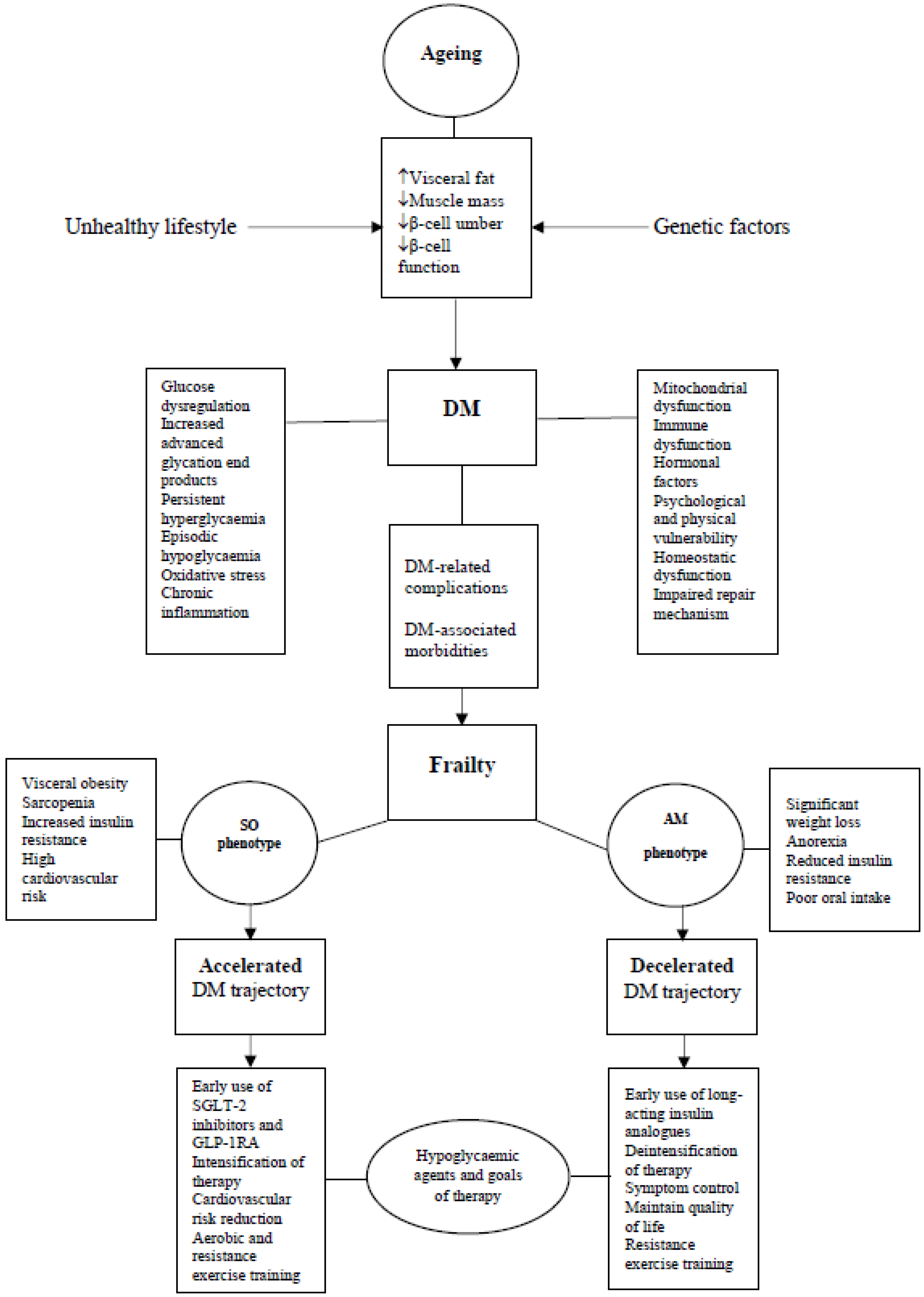
4. Diabetes Trajectory
5. Impact of Frailty on Body Composition
6. Impact of Frailty on Diabetes Trajectory
6.1. Sarcopenic Obese Phenotype (SO)-Accelerated Diabetes Trajectory
6.2. Anorexic Malnourished Phenotype (AM)-Decelerated Diabetes Trajectory
7. Clinical Implications
8. SO Phenotype
8.1. Hypoglycaemic Agents—Early Use of SGLT-2 Inhibitors and GLP-1RA
8.2. Goals of Therapy-Intensification Approach
9. AM Phenotype
9.1. Hypoglycaemic Agents—Early Use of Insulin
9.2. Goal of Therapy—Deintensification Approach
10. Conclusions
11. Future Perspectives
12. Key Points
Author Contributions
Funding
Conflicts of Interest
References
- Sun, H.; Saeedi, P.; Karuranga, S.; Pinkepank, M.; Ogurtsova, K.; Duncan, B.B.; Stein, C.; Basit, A.; Chan, J.C.; Mbanya, J.C.; et al. IDF Diabetes Atlas: Global, regional and country-level diabetes prevalence estimates for 2021 and projections for 2045. Diabetes Res. Clin. Pr. 2021, 183. [Google Scholar] [CrossRef] [PubMed]
- Sinclair, A.J.; Abdelhafiz, A.H.; Rodríguez-Mañas, L. Frailty and sarcopenia—Newly emerging and high impact complications of diabetes. J. Diabetes its Complicat. 2017, 31, 1465–1473. [Google Scholar] [CrossRef]
- Assar, M.E.; Laosa, O.; Rodríguez Mañas, L. Diabetes and frailty. Curr. Opin. Clin. Nutr. Metab Care 2019, 22, 52–57. [Google Scholar] [CrossRef] [PubMed]
- Collard, R.M.; Boter, H.; Schoevers, R.A.; Oude Voshaar, R.C. Prevalence of frailty in community-dwelling older persons: A sys-tematic review. J. Am. Geriatr. Soc. 2012, 60, 1487–1492. [Google Scholar] [CrossRef] [PubMed]
- Sinclair, A.J.; Rodriguez-Mañas, L. Diabetes and Frailty: Two Converging Conditions? Can J. Diabetes 2016, 40, 77–83. [Google Scholar] [CrossRef] [Green Version]
- Chhetri, J.K.; Zheng, Z.; Xu, X.; Ma, C.; Chan, P. The prevalence and incidence of frailty in Pre-diabetic and diabetic community-dwelling older population: Results from Beijing longitudinal study of aging II (BLSA-II). BMC Geriatr. 2017, 17, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Hanlon, P.; Jani, B.D.; Butterly, E.; Nicholl, B.; Lewsey, J.; McAllister, D.A.; Mair, F.S. An analysis of frailty and multimorbidity in 20,566 UK Biobank participants with type 2 diabetes. Commun. Med. 2021, 1, 1–9. [Google Scholar] [CrossRef]
- Sable-Morita, S.; Tanikawa, T.; Satake, S.; Okura, M.; Tokuda, H.; Arai, H. Microvascular complications and frailty can predict adverse outcomes in older patients with diabetes. Geriatr. Gerontol. Int. 2021, 21, 359–363. [Google Scholar] [CrossRef]
- Ferri-Guerra, J.; Aparicio-Ugarriza, R.; Salguero, D.; Baskaran, D.; Mohammed, Y.N.; Florez, H.; Ruiz, J.G. The Association of Frailty with Hospitalizations and Mortality among Community Dwelling Older Adults with Diabetes. J. Frailty Aging 2020, 9, 94–100. [Google Scholar] [CrossRef]
- A Espeland, M.; Justice, J.N.; Bahnson, J.; Evans, J.K.; Munshi, M.; Hayden, K.M.; Simpson, F.R.; Johnson, K.C.; Johnston, C.; Kritchevsky, S.R. Eight-Year Changes in Multimorbidity and Frailty in Adults With Type 2 Diabetes Mellitus: Associations With Cognitive and Physical Function and Mortality. J. Gerontol. Ser. A 2021, 77, 1691–1698. [Google Scholar] [CrossRef]
- Nguyen, T.N.; Harris, K.; Woodward, M.; Chalmers, J.; Cooper, M.; Hamet, P.; Harrap, S.; Heller, S.; MacMahon, S.; Mancia, G.; et al. The Impact of Frailty on the Effectiveness and Safety of Intensive Glucose Control and Blood Pressure–Lowering Therapy for People With Type 2 Diabetes: Results From the ADVANCE Trial. Diabetes Care 2021, 44, 1622–1629. [Google Scholar] [CrossRef]
- Abdelhafiz, A.H.; Emmerton, D.; Sinclair, A.J. Impact of frailty metabolic phenotypes on the management of older people with type 2 diabetes mellitus. Geriatr. Gerontol. Int. 2021, 21, 614–622. [Google Scholar] [CrossRef]
- American Diabetes Association Professional Practice Committee. 13. Older Adults: Standards of Medical Care in Diabetes-2022. Diabetes Care 2022, 45, S195–S207. [Google Scholar] [CrossRef]
- Sinclair, A.J.; Abdelhafiz, A.; Dunning, T.; Izquierdo, M.; Manas, L.R.; Bourdel-Marchasson, I.; E Morley, J.; Munshi, M.; Woo, J.; Vellas, B. An International Position Statement on the Management of Frailty in Diabetes Mellitus: Summary of Recommendations 2017. J. Frailty Aging 2018, 7, 10–20. [Google Scholar] [CrossRef]
- Blaum, C.S.; Xue, Q.L.; Tian, J.; Semba, R.D.; Fried, L.P.; Walston, J. Is hyperglycemia associated with frailty status in older women? J. Am. Geriatr. Soc. 2009, 57, 840–847. [Google Scholar] [CrossRef] [Green Version]
- Kalyani, R.R.; Tian, J.; Xue, Q.-L.; Walston, J.; Cappola, A.R.; Fried, L.P.; Brancati, F.L.; Blaum, C.S. Hyperglycemia and Incidence of Frailty and Lower Extremity Mobility Limitations in Older Women. J. Am. Geriatr. Soc. 2012, 60, 1701–1707. [Google Scholar] [CrossRef] [Green Version]
- García-Esquinas, E.; Graciani, A.; Guallar-Castillón, P.; López-García, E.; Rodríguez-Mañas, L.; Rodríguez-Artalejo, F. Diabetes and Risk of Frailty and Its Potential Mechanisms: A Prospective Cohort Study of Older Adults. J. Am. Med. Dir. Assoc. 2015, 16, 748–754. [Google Scholar] [CrossRef] [Green Version]
- Howrey, B.T.; Al Snih, S.; Markides, K.S.; Ottenbacher, K.J. Frailty and diabetes among Mexican American older adults. Ann. Epidemiology 2018, 28, 421–426.e1. [Google Scholar] [CrossRef]
- Castrejón-Pérez, R.C.; Gutiérrez-Robledo, L.M.; Cesari, M.; Pérez-Zepeda, M.U. Diabetes mellitus, hypertension and frailty: A population-based, cross-sectional study of Mexican older adults. Geriatr. Gerontol. Int. 2016, 17, 925–930. [Google Scholar] [CrossRef]
- Castrejón-Pérez, R.C.; Aguilar-Salinas, C.A.; Gutiérrez-Robledo, L.M.; Cesari, M.; Pérez-Zepeda, M.U. Frailty, diabetes, and the convergence of chronic disease in an age-related condition: A population-based nationwide cross-sectional analysis of the Mexican nutrition and health survey. Aging Clin. Exp. Res. 2017, 30, 935–941. [Google Scholar] [CrossRef]
- Chao, C.-T.; Wang, J.; Huang, J.-W.; Chan, D.-C.; Chien, K.-L. Hypoglycemic episodes are associated with an increased risk of incident frailty among new onset diabetic patients. J. Diabetes Its Complicat. 2019, 34, 107492. [Google Scholar] [CrossRef] [PubMed]
- Komorita, Y.; Iwase, M.; Fujii, H.; Ohkuma, T.; Ide, H.; Yoshinari, M.; Oku, Y.; Nakamura, U.; Kitazono, T. Both hypo- and hyperglycaemia are associated with increased fracture risk in Japanese people with type 2 diabetes: The Fukuoka Diabetes Registry. Diabet. Med. 2019, 37, 838–847. [Google Scholar] [CrossRef] [PubMed]
- Ntouva, A.; A Toulis, K.; Keerthy, D.; Adderley, N.J.; Hanif, W.; Thayakaran, R.; Gokhale, K.; Thomas, G.N.; Khunti, K.; A Tahrani, A.; et al. Hypoglycaemia is associated with increased risk of fractures in patients with type 2 diabetes mellitus: A cohort study. Eur. J. Endocrinol. 2019, 180, 51–58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hung, Y.C.; Lin, C.C.; Chen, H.J.; Chang, M.P.; Huang, K.C.; Chen, Y.H.; Chen, C.C. Severe hypoglycemia and hip fracture in patients with type 2 diabetes: A nationwide population-based cohort study. Osteoporos. Int. 2017, 28, 2053–2060. [Google Scholar] [CrossRef] [PubMed]
- MacKenzie, H.T.; Tugwell, B.; Rockwood, K.; Theou, O. Frailty and Diabetes in Older Hospitalized Adults: The Case for Routine Frailty Assessment. Can. J. Diabetes 2020, 44, 241–245.e1. [Google Scholar] [CrossRef]
- Yanagita, I.; Fujihara, Y.; Eda, T.; Tajima, M.; Yonemura, K.; Kawajiri, T.; Yamaguchi, N.; Asakawa, H.; Nei, Y.; Kayashima, Y.; et al. Low glycated haemoglobin level is associated with severity of frailty in Japanese elderly diabetes patients. J. Diabetes Investig 2018, 9, 419–425. [Google Scholar] [CrossRef]
- Morita, T.; Okuno, T.; Himeno, T.; Watanabe, K.; Nakajima, K.; Koizumi, Y.; Yano, H.; Iritani, O.; Okuro, M.; Morimoto, S. Glycemic control and disability-free survival in hypoglycemic agent-treated community-dwelling older patients with type 2 diabetes mellitus. Geriatr. Gerontol. Int. 2017, 17, 1858–1865. [Google Scholar] [CrossRef]
- Zaslavsky, O.; Walker, R.L.; Crane, P.K.; Gray, S.L.; Larson, E.B. Glucose Levels and Risk of Frailty. J. Gerontol. Ser. A 2016, 71, 1223–1229. [Google Scholar] [CrossRef] [Green Version]
- Ferrucci, L.; Penninx, B.W.J.H.; Volpato, S.; Harris, T.B.; Bandeen-Roche, K.; Balfour, J.; Leveille, S.G.; Fried, L.P.; Guralnik, J.M. Change in Muscle Strength Explains Accelerated Decline of Physical Function in Older Women With High Interleukin-6 Serum Levels. J. Am. Geriatr. Soc. 2002, 50, 1947–1954. [Google Scholar] [CrossRef] [Green Version]
- Sheetz, M.J.; King, G.L. Molecular understanding of hyperglycemia’s adverse effects for diabetic complications. JAMA 2002, 288, 2579–2588. [Google Scholar] [CrossRef]
- Phielix, E.; Schrauwen-Hinderling, V.B.; Mensink, M.; Lenaers, E.; Meex, R.; Hoeks, J.; Kooi, M.E.; Moonen-Kornips, E.; Sels, J.-P.; Hesselink, M.K.; et al. Lower Intrinsic ADP-Stimulated Mitochondrial Respiration Underlies In Vivo Mitochondrial Dysfunction in Muscle of Male Type 2 Diabetic Patients. Diabetes 2008, 57, 2943–2949. [Google Scholar] [CrossRef] [Green Version]
- Rogers, S.C.; Zhang, X.; Azhar, G.; Luo, S.; Wei, J.Y. Exposure to High or Low Glucose Levels Accelerates the Appearance of Markers of Endothelial Cell Senescence and Induces Dysregulation of Nitric Oxide Synthase. J. Gerontol. Ser. A 2013, 68, 1469–1481. [Google Scholar] [CrossRef] [Green Version]
- Crane, P.K.; Walker, R.; Hubbard, R.A.; Li, G.; Nathan, D.M.; Zheng, H.; Haneuse, S.; Craft, S.; Montine, T.J.; Kahn, S.E.; et al. Glucose Levels and Risk of Dementia. N. Engl. J. Med. 2013, 369, 540–548. [Google Scholar] [CrossRef] [Green Version]
- Araki, A.; Iimuro, S.; Sakurai, T.; Umegaki, H.; Iijima, K.; Nakano, H.; Oba, K.; Yokono, K.; Sone, H.; Yamada, N.; et al. Non-high-density lipoprotein cholesterol: An important predictor of stroke and diabetes-related mortality in Japanese elderly diabetic patients. Geriatr. Gerontol. Int. 2012, 12, 18–28. [Google Scholar] [CrossRef] [Green Version]
- Veronese, N.; Stubbs, B.; Fontana, L.; Trevisan, C.; Bolzetta, F.; De Rui, M.; Sartori, L.; Musacchio, E.; Zambon, S.; Maggi, S.; et al. Frailty Is Associated with an Increased Risk of Incident Type 2 Diabetes in the Elderly. J. Am. Med. Dir. Assoc. 2016, 17, 902–907. [Google Scholar] [CrossRef]
- Kalyani, R.R.; Varadhan, R.; Weiss, C.O.; Fried, L.P.; Cappola, A.R. Frailty Status and Altered Glucose-Insulin Dynamics. J. Gerontol. Ser. A 2011, 67, 1300–1306. [Google Scholar] [CrossRef] [Green Version]
- Evans, W.J. Skeletal muscle loss: Cachexia, sarcopenia, and inactivity. Am. J. Clin. Nutr. 2010, 91, 1123S–1127S. [Google Scholar] [CrossRef] [Green Version]
- Guilherme, A.; Virbasius, J.V.; Puri, V.; Czech, M.P. Adipocyte dysfunctions linking obesity to insulin resistance and type 2 diabetes. Nat. Rev. Mol. Cell Biol. 2008, 9, 367–377. [Google Scholar] [CrossRef] [Green Version]
- Choi, K.M. Sarcopenia and sarcopenic obesity. Korean J. Intern. Med. 2016, 31, 1054–1060. [Google Scholar] [CrossRef] [Green Version]
- Doucet, E.; St Pierre, S.; Alméras, N.; Mauriège, P.; Richard, D.; Tremblay, A. Changes in energy expenditure and substrate oxidation resulting from weight loss in obese men and women: Is there an important contribution of leptin? J. Clin. Endocrinol. Metab. 2000, 85, 1550–1556. [Google Scholar]
- Cartwright, M.J.; Tchkonia, T.; Kirkland, J.L. Aging in adipocytes: Potential impact of inherent, depot-specific mechanisms. Exp. Gerontol. 2007, 42, 463–471. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Szoke, E.; Shrayyef, M.Z.; Messing, S.; Woerle, H.J.; van Haeften, T.W.; Meyer, C.; Mitrakou, A.; Pimenta, W.; Gerich, J.E. Effect of aging on glucose homeostasis: Accelerated deterioration of β-cell function in individuals with impaired glucose tolerance. Diabetes Care 2008, 31, 539–543. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, W.; Egan, J.M. The Role of Incretins in Glucose Homeostasis and Diabetes Treatment. Pharm. Rev. 2008, 60, 470–512. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Farilla, L.; Bulotta, A.; Hirshberg, B.; Calzi, S.L.; Khoury, N.; Noushmehr, H.; Bertolotto, C.; Di Mario, U.; Harlan, D.M.; Perfetti, R. Glucagon-Like Peptide 1 Inhibits Cell Apoptosis and Improves Glucose Responsiveness of Freshly Isolated Human Islets. Endocrinology 2003, 144, 5149–5158. [Google Scholar] [CrossRef] [Green Version]
- Schaap, L.A.; Pluijm, S.M.F.; Smit, J.H.; van Schoor, N.M.; Visser, M.; Gooren, L.J.G.; Lips, P. The association of sex hormone levels with poor mobility, low muscle strength and incidence of falls among older men and women. Clin. Endocrinol. 2005, 63, 152–160. [Google Scholar] [CrossRef] [Green Version]
- O’Donnell, A.B.; Travison, T.G.; Harris, S.S.; Tenover, J.L.; McKinlay, J.B. Testosterone, Dehydroepiandrosterone, and Physical Performance in Older Men: Results from the Massachusetts Male Aging Study. J. Clin. Endocrinol. Metab. 2006, 91, 425–431. [Google Scholar] [CrossRef] [Green Version]
- Lovejoy, J.C.; Champagne, C.M.; de Jonge, L.; Xie, H.; Smith, S.R. Increased visceral fat and decreased energy expenditure during the menopausal transition. Int. J. Obes. 2008, 32, 949–958. [Google Scholar] [CrossRef] [Green Version]
- Sowers, M.R.; Zheng, H.; Tomey, K.; A Karvonengutierrez, C.; Jannausch, M.L.; Li, X.; Yosef, M.; Symons, J.P. Changes in Body Composition in Women over Six Years at Midlife: Ovarian and Chronological Aging. J. Clin. Endocrinol. Metab. 2007, 92, 895–901. [Google Scholar] [CrossRef] [Green Version]
- Kim, G.; Kim, J.H. Impact of Skeletal Muscle Mass on Metabolic Health. Endocrinol. Metab. 2020, 35, 1–6. [Google Scholar] [CrossRef]
- Petermann-Rocha, F.; Chen, M.; Gray, S.R.; Ho, F.K.; Pell, J.P.; Celis-Morales, C. Factors associated with sarcopenia: A cross-sectional analysis using UK Biobank. Maturitas 2020, 133, 60–67. [Google Scholar] [CrossRef]
- Horton, W.B.; Barrett, E.J. Microvascular Dysfunction in Diabetes Mellitus and Cardiometabolic Disease. Endocr. Rev. 2020, 42, 29–55. [Google Scholar] [CrossRef]
- Gaulton, K.J.; Ferreira, T.; Lee, Y.; Raimondo, A.; Mägi, R.; Reschen, M.E.; Mahajan, A.; Locke, A.; Rayner, N.W.; Robertson, N.; et al. DI-Abetes Genetics Replication And Meta-analysis (DIAGRAM) Consortium. Genetic fine mapping and genomic annotation de-fines causal mechanisms at type 2 diabetes susceptibility loci. Nat. Genet. 2015, 47, 1415–1425. [Google Scholar] [CrossRef]
- Chan, J.M.; Rimm, E.B.; A Colditz, G.; Stampfer, M.J.; Willett, W.C. Obesity, Fat Distribution, and Weight Gain as Risk Factors for Clinical Diabetes in Men. Diabetes Care 1994, 17, 961–969. [Google Scholar] [CrossRef] [Green Version]
- Van der Zijl, N.J.; Goossens, G.H.; Moors, C.C.; van Raalte, D.H.; Muskiet, M.H.; Pouwels, P.J.; Blaak, E.E.; Diamant, M. Ectopic fat storage in the pancreas, liver, and abdominal fat depots: Impact on β-cell function in individuals with impaired glucose metabolism. J. Clin. Endocrinol. Metab. 2011, 96, 459–467. [Google Scholar] [CrossRef] [Green Version]
- Skyler, J.S.; Bakris, G.L.; Bonifacio, E.; Darsow, T.; Eckel, R.H.; Groop, L.; Groop, P.H.; Handelsman, Y.; Insel, R.A.; Mathieu, C.; et al. Dif-ferentiation of Diabetes by Pathophysiology, Natural History, and Prognosis. Diabetes 2017, 66, 241–255. [Google Scholar] [CrossRef] [Green Version]
- Phillips, L.S.; Ratner, R.E.; Buse, J.B.; Kahn, S.E. We Can Change the Natural History of Type 2 Diabetes. Diabetes Care 2014, 37, 2668–2676. [Google Scholar] [CrossRef] [Green Version]
- Pette Peuker, D.H.; Staron, R.S. The impact of biochemical methods for single fiber analysis. Acta Physiol. Scand 1999, 166, 261–277. [Google Scholar] [CrossRef]
- Henriksen, E.J.; Bourey, R.E.; Rodnick, K.J.; Koranyi, L.; Permutt, M.A.; Holloszy, J.O. Glucose transporter protein con- tent and glucose transport capacity in rat skeletal muscles. Am. J. Physiol. Endocrinol. Metab. 1990, 259, E593–E598. [Google Scholar] [CrossRef]
- Sonjak, V.; Jacob, K.; Morais, J.A.; Rivera-Zengotita, M.; Spendiff, S.; Spake, C.; Taivassalo, T.; Chevalier, S.; Hepple, R.T. Fidelity of muscle fibre reinnervation modulates ageing muscle impact in elderly women. J. Physiol. 2019, 597, 5009–5023. [Google Scholar] [CrossRef]
- St-Jean-Pelletier, F.; Pion, C.H.; Leduc-Gaudet, J.-P.; Sgarioto, N.; Zovilé, I.; Barbat-Artigas, S.; Reynaud, O.; Alkaterji, F.; Lemieux, F.C.; Grenon, A.; et al. The impact of ageing, physical activity, and pre-frailty on skeletal muscle phenotype, mitochondrial content, and intramyocellular lipids in men. J. Cachexia Sarcopenia Muscle 2017, 8, 213–228. [Google Scholar] [CrossRef]
- Nilwik, R.; Snijders, T.; Leenders, M.; Groen, B.B.; van Kranenburg, J.; Verdijk, L.B.; van Loon, L.J. The decline in skeletal muscle mass with aging is mainly attributed to a reduction in type II muscle fiber size. Exp. Gerontol. 2013, 48, 492–498. [Google Scholar] [CrossRef] [PubMed]
- Miljkovic, N.; Lim, J.-Y.; Miljkovic, I.; Frontera, W.R. Aging of Skeletal Muscle Fibers. Ann. Rehabilitation Med. 2015, 39, 155–162. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Mañas, L.; Féart, C.; Mann, G.; Viña, J.; Chatterji, S.; Chodzko-Zajko, W.; Harmand, M.G.-C.; Bergman, H.; Carcaillon, L.; Nicholson, C.; et al. Searching for an Operational Definition of Frailty: A Delphi Method Based Consensus Statement. The Frailty Operative Definition-Consensus Conference Project. J. Gerontol. Ser. A 2012, 68, 62–67. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fried, L.P.; Tangen, C.M.; Walston, J.; Newman, A.B.; Hirsch, C.; Gottdiener, J.; Seeman, T.; Tracy, R.; Kop, W.J.; Burke, G.; et al. Frailty in Older adults: Evidence for a phenotype. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2001, 56, M146–M156. [Google Scholar] [CrossRef]
- Rockwood, K.; Mitnitski, A. Frailty in Relation to the Accumulation of Deficits. J. Gerontol. Ser. A 2007, 62, 722–727. [Google Scholar] [CrossRef] [Green Version]
- Watanabe, D.; Yoshida, T.; Watanabe, Y.; Yamada, Y.; Kimura, M.; Kyoto-Kameoka Study Group. A U-Shaped Relationship between the Prevalence of Frailty and Body Mass Index in Community-Dwelling Japanese Older Adults: The Kyoto–Kameoka Study. J. Clin. Med. 2020, 9, 1367. [Google Scholar] [CrossRef]
- Chung, J.-Y.; Kang, H.-T.; Lee, D.-C.; Lee, H.-R.; Lee, Y.-J. Body composition and its association with cardiometabolic risk factors in the elderly: A focus on sarcopenic obesity. Arch. Gerontol. Geriatr. 2012, 56, 270–278. [Google Scholar] [CrossRef]
- Tanner, C.J.; Barakat, H.A.; Dohm, G.L.; Pories, W.J.; Macdonald, K.G.; Cunningham, P.R.G.; Swanson, M.S.; Houmard, J.A. Muscle fiber type is associated with obesity and weight loss. Am. J. Physiol. Metab. 2002, 282, E1191–E1196. [Google Scholar] [CrossRef] [Green Version]
- Batsis, J.A.; Villareal, D.T. Sarcopenic obesity in older adults: Aetiology, epidemiology and treatment strategies. Nat. Rev. Endocrinol. 2018, 14, 513–537. [Google Scholar] [CrossRef]
- El Bizri, I.; Batsis, J.A. Linking epidemiology and molecular mechanisms in sarcopenic obesity in populations. Proc. Nutr. Soc. 2020, 79, 448–456. [Google Scholar] [CrossRef]
- Chait, A.; den Hartigh, L.J. Adipose Tissue Distribution, Inflammation and Its Metabolic Consequences, Including Diabetes and Cardiovascular Disease. Front. Cardiovasc. Med. 2020, 7, 22. [Google Scholar] [CrossRef] [Green Version]
- Morley, J.E.; Silver, A.J. Anorexia in the elderly. Neurobiol. Aging 1988, 9, 9–16. [Google Scholar] [CrossRef]
- Jyväkorpi, S.K.; Pitkälä, K.H.; Puranen, T.M.; Björkman, M.P.; Kautiainen, H.; Strandberg, T.E.; Soini, H.H.; Suominen, M.H. High proportions of older people with normal nutritional status have poor protein intake and low diet quality. Arch Gerontol. Geriatr. 2016, 67, 40–45. [Google Scholar] [CrossRef] [Green Version]
- Donini, L.M.; Poggiogalle, E.; Piredda, M.; Pinto, A.; Barbagallo, M.; Cucinotta, D.; Sergi, G. Anorexia and Eating Patterns in the Elderly. PLoS ONE 2013, 8, e63539. [Google Scholar] [CrossRef] [Green Version]
- Morley, J.E. Anorexia of aging. Am. J. Clin. Nutr. 1997, 66, 760–773. [Google Scholar] [CrossRef] [Green Version]
- Young, K.W.; Greenwood, C.E. Shift in diurnal feeding patterns in nursing home residents with Alzheimer’s disease. J. Gerontol. A Biol. Sci. Med. Sci. 2001, 56, M700–M706. [Google Scholar] [CrossRef] [Green Version]
- Theou, O.; Cann, L.; Blodgett, J.; Wallace, L.M.; Brothers, T.D.; Rockwood, K. Modifications to the frailty phenotype criteria: Systematic review of the current literature and investigation of 262 frailty phenotypes in the Survey of Health, Ageing, and Retirement in Europe. Ageing Res. Rev. 2015, 21, 78–94. [Google Scholar] [CrossRef]
- Campitelli, M.A.; Bronskill, S.E.; Hogan, D.B.; Diong, C.; Amuah, J.E.; Gill, S.; Seitz, D.; Thavorn, K.; Wodchis, W.P.; Maxwell, C.J. The prevalence and health consequences of frailty in a population-based older home care cohort: A comparison of different measures. BMC Geriatr. 2016, 16, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Goulet, E.D.; Hassaine, A.; Dionne, I.J.; Gaudreau, P.; Khalil, A.; Fulop, T.; Shatenstein, B.; Tessier, D.; Morais, J.A. Frailty in the elderly is associated with insulin resistance of glucose metabolism in the postabsorptive state only in the presence of increased abdominal fat. Exp. Gerontol. 2009, 44, 740–744. [Google Scholar] [CrossRef]
- Henry, R.R.; Wallace, P.; Olefsky, J.M. Effects of weight loss on mechanisms of hyperglycemia in obese non-insulin-dependent diabetes mellitus. Diabetes 1986, 35, 990–998. [Google Scholar] [CrossRef]
- Lim, E.L.; Hollingsworth, K.G.; Aribisala, B.S.; Chen, M.J.; Mathers, J.C.; Taylor, R. Reversal of type 2 diabetes: Normalisation of beta cell function in association with decreased pancreas and liver triacylglycerol. Diabetologia 2011, 54, 2506–2514. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abdelhafiz, A.H.; Koay, L.; Sinclair, A.J. The Emergence of Frailty May Lead to a State of Burnt Out Type 2 Diabetes. J. Frailty Aging 2016, 5, 162–167. [Google Scholar] [CrossRef] [PubMed]
- Xia, M.-F.; Chen, L.-Y.; Wu, L.; Ma, H.; Li, X.-M.; Li, Q.; Aleteng, Q.; Hu, Y.; He, W.-Y.; Gao, J.; et al. Sarcopenia, sarcopenic overweight/obesity and risk of cardiovascular disease and cardiac arrhythmia: A cross-sectional study. Clin. Nutr. 2020, 40, 571–580. [Google Scholar] [CrossRef] [PubMed]
- Cho, H.-W.; Chung, W.; Moon, S.; Ryu, O.-H.; Kim, M.K.; Kang, J.G. Effect of Sarcopenia and Body Shape on Cardiovascular Disease According to Obesity Phenotypes. Diabetes Metab. J. 2021, 45, 209–218. [Google Scholar] [CrossRef] [PubMed]
- Uchida, S.; Kamiya, K.; Hamazaki, N.; Matsuzawa, R.; Nozaki, K.; Ichikawa, T.; Suzuki, Y.; Nakamura, T.; Yamashita, M.; Kariya, H.; et al. Association between sarcopenia and atherosclerosis in elderly patients with ischemic heart disease. Heart Vessel. 2020, 35, 769–775. [Google Scholar] [CrossRef]
- Yoo, J.H.; Park, S.W.; Jun, J.E.; Jin, S.; Hur, K.Y.; Lee, M.; Kang, M.; Kim, G.; Kim, J.H. Relationship between low skeletal muscle mass, sarcopenic obesity and left ventricular diastolic dysfunction in Korean adults. Diabetes/Metabolism Res. Rev. 2020, 37, e3363. [Google Scholar] [CrossRef]
- Lakkis, J.I.; Weir, M.R. Obesity and kidney disease. Prog. Cardivasc. Dis. 2018, 61, 157–167. [Google Scholar] [CrossRef]
- García-Carro, C.; Vergara, A.; Bermejo, S.; Azancot, M.A.; Sellarés, J.; Soler, M.J. A Nephrologist Perspective on Obesity: From Kidney Injury to Clinical Management. Front. Med. 2021, 8. [Google Scholar] [CrossRef]
- Godoy-Matos, A.F.; Júnior, W.S.S.; Valerio, C.M. NAFLD as a continuum: From obesity to metabolic syndrome and diabetes. Diabetol. Metab. Syndr. 2020, 12, 1–20. [Google Scholar] [CrossRef]
- Abdelhafiz, A.H.; Sinclair, A.J. Cardio-renal protection in older people with diabetes with frailty and medical comorbidities—A focus on the new hypoglycaemic therapy. J. Diabetes Its Complicat. 2020, 34, 107639. [Google Scholar] [CrossRef]
- Marsico, F.; Paolillo, S.; Gargiulo, P.; Bruzzese, D.; Dell’Aversana, S.; Esposito, I.; Renga, F.; Esposito, L.; Marciano, C.; Dellegrottaglie, S.; et al. Effects of glucagon-like peptide-1 receptor agonists on major cardiovascular events in patients with Type 2 diabetes mellitus with or without established cardiovascular disease: A meta-analysis of randomized controlled trials. Eur. Heart J. 2020, 41, 3346–3358. [Google Scholar] [CrossRef]
- Zinman, B.; Wanner, C.; Lachin, J.M.; Fitchett, D.; Bluhmki, E.; Hantel, S.; Mattheus, M.; Devins, T.; Johansen, O.E.; Woerle, H.J.; et al. Empagliflozin, Cardiovascular Outcomes, and Mortality in Type 2 Diabetes. N. Engl. J. Med. 2015, 373, 2117–2128. [Google Scholar] [CrossRef] [Green Version]
- Wiviott, S.D.; Raz, I.; Bonaca, M.P.; Mosenzon, O.; Kato, E.T.; Cahn, A.; Silverman, M.G.; Zelniker, T.A.; Kuder, J.F.; Murphy, S.A.; et al. Dapagliflozin and Cardiovascular Outcomes in Type 2 Diabetes. N. Engl. J. Med. 2019, 380, 347–357. [Google Scholar] [CrossRef]
- McMurray, J.J.; Solomon, S.D.; Inzucchi, S.E.; Køber, L.; Kosiborod, M.N.; Martinez, F.A.; Ponikowski, P.; Sabatine, M.S.; Anand, I.S.; Bělohlávek, J.; et al. Dapagliflozin in patients with heart failure and reduced ejection fraction. N Engl. J. Med. 2019, 381, 1995–2008. [Google Scholar] [CrossRef] [Green Version]
- Adingupu, D.D.; Göpel, S.O.; Grönros, J.; Behrendt, M.; Sotak, M.; Miliotis, T.; Dahlqvist, U.; Gan, L.-M.; Jönsson-Rylander, A.-C. SGLT2 inhibition with empagliflozin improves coronary microvascular function and cardiac contractility in prediabetic ob/ob−/− mice. Cardiovasc. Diabetol. 2019, 18, 1–15. [Google Scholar] [CrossRef] [Green Version]
- Bae, J.H.; Park, E.-G.; Kim, S.; Kim, S.G.; Hahn, S.; Kim, N.H. Effects of Sodium-Glucose Cotransporter 2 Inhibitors on Renal Outcomes in Patients with Type 2 Diabetes: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Sci. Rep. 2019, 9, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Wanner, C.; Inzucchi, S.E.; Lachin, J.M.; Fitchett, D.; Von Eynatten, M.; Mattheus, M.; Johansen, O.E.; Woerle, H.J.; Broedl, U.C.; Zinman, B. Empagliflozin and Progression of Kidney Disease in Type 2 Diabetes. N. Engl. J. Med. 2016, 375, 323–334. [Google Scholar] [CrossRef]
- Vasilakou, D.; Karagiannis, T.; Athanasiadou, E.; Mainou, M.; Liakos, A.; Bekiari, E.; Sarigianni, M.; Matthews, D.R.; Tsapas, A. Sodium–glucose cotransporter 2 inhibitors for Type 2 diabetes: A systematic review and meta-analysis. Ann. Intern. Med. 2013, 159, 262–274. [Google Scholar] [CrossRef] [Green Version]
- Karagiannis, T.; Tsapas, A.; Athanasiadou, E.; Avgerinos, I.; Liakos, A.; Matthews, D.R.; Bekiari, E. GLP-1 receptor agonists and SGLT2 inhibitors for older people with type 2 diabetes: A systematic review and meta-analysis. Diabetes Res. Clin. Pr. 2021, 174, 108737. [Google Scholar] [CrossRef]
- Lv, X.; Dong, Y.; Hu, L.; Lu, F.; Zhou, C.; Qin, S. Glucagon-like peptide-1 receptor agonists (GLP-1 RAs) for the management of nonalcoholic fatty liver disease (NAFLD): A systematic review. Endocrinol. Diabetes Metab. 2020, 3, e00163. [Google Scholar] [CrossRef]
- Zhang, X.; Bai, R.; Jia, Y.; Zong, J.; Wang, Y.; Dong, Y. The effect of liraglutide on nonalcoholic fatty liver disease in type 2 diabetes mellitus. Int. J. Diabetes Dev. Ctries. 2020, 40, 491–499. [Google Scholar] [CrossRef]
- Feig, D.I.; Kang, D.-H.; Johnson, R.J. Uric Acid and Cardiovascular Risk. N. Engl. J. Med. 2008, 359, 1811–1821. [Google Scholar] [CrossRef] [PubMed]
- Sofogianni, A.; Filippidis, A.; Chrysavgis, L.; Tziomalos, K.; Cholongitas, E. Glucagon-like peptide-1 receptor agonists in non-alcoholic fatty liver disease: An update. World J. Hepatol. 2020, 12, 493–505. [Google Scholar] [CrossRef] [PubMed]
- Xing, B.; Zhao, Y.; Dong, B.; Zhou, Y.; Lv, W.; Zhao, W. Effects of sodium–glucose cotransporter 2 inhibitors on non-alcoholic fatty liver disease in patients with type 2 diabetes: A meta-analysis of randomized controlled trials. J. Diabetes Investig. 2020, 11, 1238–1247. [Google Scholar] [CrossRef]
- Emmerton, D.; Abdelhafiz, A. Newer anti-diabetic therapies with low hypoglycemic risk-potential advantages for frail older people. Hosp. Pr. 2021, 49, 164–175. [Google Scholar] [CrossRef]
- Abdelhafiz, A.H.; McNicholas, E.; Sinclair, A.J. Hypoglycemia, frailty and dementia in older people with diabetes: Reciprocal relations and clinical implications. J. Diabetes Its Complicat. 2016, 30, 1548–1554. [Google Scholar] [CrossRef]
- Leroith, D.; Biessels, G.J.; Braithwaite, S.S.; Casanueva, F.F.; Draznin, B.; Halter, J.B.; Hirsch, I.B.; McDonnell, M.; E Molitch, M.E.; Murad, M.H.; et al. TReatment of diabetes in older adults: An endocrine society clinical practice guideline. J. Clin. Endocrinol. Metab. 2019, 104, 1520–1574. [Google Scholar] [CrossRef] [Green Version]
- Hambling, C.E.; Khunti, K.; Cos, X.; Wens, J.; Martinez, L.; Topsever, P.; Del Prato, S.; Sinclair, A.; Schernthaner, G.; Rutten, G.; et al. Factors influencing safe glucose-lowering in older adults with type 2 diabetes: A PeRsOn-centred ApproaCh To IndiVidualisEd (PROACTIVE) Glycemic Goals for older people: A position statement of Primary Care Diabetes Europe. Prim. Care Diabetes 2019, 13, 330–352. [Google Scholar] [CrossRef]
- Cosentino, F.; Grant, P.; Aboyans, V.; Bailey, C.J.; Ceriello, A.; Delgado, V. The Task Force for diabetes, pre-diabetes, and cardiovascular diseases of the European Society of Cardiology (ESC) and the European Association for the Study of Diabetes (EASD). 2019 ESC Guidelines on diabetes, pre-diabetes, and cardiovascular diseases developed in collaboration with the EASD. Eur. Heart J. 2020, 41, 255–323. [Google Scholar]
- Sinclair, A.J.; Pennells, D.; Abdelhafiz, A.H. Hypoglycaemic therapy in frail older people with type 2 diabetes mellitus—A choice determined by metabolic phenotype. Aging Clin. Exp. Res. 2022, 34, 1949–1967. [Google Scholar] [CrossRef]
- Bollig, C.; MedQoL-Group (Medication and Quality of Life in frail older persons); Torbahn, G.; Bauer, J.; Brefka, S.; Dallmeier, D.; Denkinger, M.; Eidam, A.; Klöppel, S.; Zeyfang, A.; et al. Evidence gap on antihyperglycemic pharmacotherapy in frail older adults. Z. Fur Gerontol. Und Geriatr. 2020, 54, 278–284. [Google Scholar] [CrossRef] [Green Version]
- Liu, H.M.; Zhang, Q.; Shen, W.D.; Li, B.Y.; Lv, W.Q.; Xiao, H.M.; Deng, H.W. Sarcopenia-related traits and coronary artery disease: A bi-directional Mendelian randomization study. Aging (Albany NY) 2020, 12, 3340–3353. [Google Scholar] [CrossRef]
- Villareal, D.T.; Aguirre, L.; Gurney, A.B.; Waters, D.L.; Sinacore, D.R.; Colombo, E.; Armamento-Villareal, R.; Qualls, C. Aerobic or Resistance Exercise, or Both, in Dieting Obese Older Adults. N. Engl. J. Med. 2017, 376, 1943–1955. [Google Scholar] [CrossRef] [Green Version]
- Asano, R.Y.; Sales, M.M.; Coelho, J.M.; Moraes, J.F.V.N.; Pereira, L.A.; Simoes, H.G. Exercise, nitric oxide, and endothelial dysfunction: A brief review. J. Exerc. Physiol. Online 2012, 15, 76–86. [Google Scholar]
- Vasconcelos, K.S.D.S.; Dias, J.M.D.; de Araújo, M.C.; Pinheiro, A.C.; Maia, M.M.; Dias, R.C. Land-based versus aquatic resistance therapeutic exercises for older women with sarcopenic obesity: Study protocol for a randomised controlled trial. Trials 2013, 14, 296. [Google Scholar] [CrossRef] [Green Version]
- Wittmann, K.; Sieber, C.; von Stengel, S.; Kohl, M.; Freiberger, E.; Jakob, F.; Lell, M.; Engelke, K.; Kemmler, W. Impact of whole body electromyostimulation on cardiometabolic risk factors in older women with sarcopenic obesity: The randomized controlled FORMOsA-sarcopenic obesity study. Clin. Interv. Aging 2016, 11, 1697–1706. [Google Scholar] [CrossRef] [Green Version]
- Kelly, O.J.; Gilman, J.C. Can unconventional exercise be help- ful in the treatment, management and prevention of osteosar-copenic obesity? Curr. Aging Sci. 2017, 10, 106–121. [Google Scholar] [CrossRef]
- Malafarina, V.; Uriz-Otano, F.; Iniesta, R.; Gil-Guerrero, L. Effectiveness of nutritional supplementation on muscle mass intreatment of sarcopenia in old age: A systematic review. J. Am. Med. Dir. Assoc. 2013, 14, 10–17. [Google Scholar] [CrossRef]
- Gryson, C.; Ratel, S.; Rance, M.; Penando, S.; Bonhomme, C.; Le Ruyet, P.; Duclos, M.; Boirie, Y.; Walrand, S. Four-month course of soluble mil proteins interacts with exercise to improve muscle strength and delay fatigue in elderly participants. J. Am. Med. Dir. Assoc 2014, 15, 958-e1-9. [Google Scholar] [CrossRef]
- Suckale, J.; Solimena, M. The insulin secretory granule as a signaling hub. Trends Endocrinol. Metab. 2010, 21, 599–609. [Google Scholar] [CrossRef]
- Yang, B.-Y.; Zhai, G.; Gong, Y.-L.; Su, J.-Z.; Peng, X.-Y.; Shang, G.-H.; Han, D.; Jin, J.-Y.; Liu, H.-K.; Du, Z.-Y.; et al. Different physiological roles of insulin receptors in mediating nutrient metabolism in zebrafish. Am. J. Physiol. Metab. 2018, 315, E38–E51. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hatting, M.; Tavares, C.D.; Sharabi, K.; Rines, A.K.; Puigserver, P. Insulin regulation of gluconeogenesis. Ann. N. Y. Acad. Sci. 2017, 1411, 21–35. [Google Scholar] [CrossRef] [PubMed]
- Karakelides, H.; Asmann, Y.W.; Bigelow, M.L.; Short, K.R.; Dhatariya, K.; Coenen-Schimke, J.; Kahl, J.; Mukhopadhyay, D.; Nair, K.S. Effect of Insulin Deprivation on Muscle Mitochondrial ATP Production and Gene Transcript Levels in Type 1 Diabetic Subjects. Diabetes 2007, 56, 2683–2689. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davidovici, B.B.; Sattar, N.; Prinz, J.; Puig, L.; Emery, P.; Barker, J.N.; van de Kerkhof, P.; Ståhle, M.; Nestle, F.O.; Girolomoni, G.; et al. Psoriasis and systemic inflammatory diseases: Potential mechanistic links between skin disease and co-morbid conditions. J. Investig. Dermatol. 2010, 130, 1785–1796. [Google Scholar] [CrossRef] [Green Version]
- Abdulla, H.; Smith, K.; Atherton, P.J.; Idris, I. Role of insulin in the regulation of human skeletal muscle protein synthesis and breakdown: A systematic review and meta-analysis. Diabetologia 2015, 59, 44–55. [Google Scholar] [CrossRef]
- Fujita, S.; Glynn, E.L.; Timmerman, K.L.; Rasmussen, B.B.; Volpi, E. Supraphysiological hyperinsulinaemia is necessary to stimulate skeletal muscle protein anabolism in older adults: Evidence of a true age-related insulin resistance of muscle protein metabolism. Diabetologia 2009, 52, 1889–1898. [Google Scholar] [CrossRef] [Green Version]
- Tanaka, K.-I.; Kanazawa, I.; Sugimoto, T. Reduction in Endogenous Insulin Secretion is a Risk Factor of Sarcopenia in Men with Type 2 Diabetes Mellitus. Calcif. Tissue Int. 2015, 97, 385–390. [Google Scholar] [CrossRef]
- Bouchi, R.; Fukuda, T.; Takeuchi, T.; Nakano, Y.; Murakami, M.; Minami, I.; Izumiyama, H.; Hashimoto, K.; Yoshimoto, T.; Ogawa, Y. Insulin Treatment Attenuates Decline of Muscle Mass in Japanese Patients with Type 2 Diabetes. Calcif. Tissue Int. 2017, 101, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Ferrari, U.; Then, C.; Rottenkolber, M.; Selte, C.; Seissler, J.; Conzade, R.; Linkohr, B.; Peters, A.; Drey, M.; Thorand, B. Longitudinal association of type 2 diabetes and insulin therapy with muscle parameters in the KORA-Age study. Acta Diabetol. 2020, 57, 1057–1063. [Google Scholar] [CrossRef]
- Sugimoto, K.; Ikegami, H.; Takata, Y.; Katsuya, T.; Fukuda, M.; Akasaka, H.; Tabara, Y.; Osawa, H.; Hiromine, Y.; Rakugi, H. Glycemic Control and Insulin Improve Muscle Mass and Gait Speed in Type 2 Diabetes: The MUSCLES-DM Study. J. Am. Med. Dir. Assoc. 2021, 22, 834–838.e1. [Google Scholar] [CrossRef]
- Doyle-Delgado, K.; Chamberlain, J.J.; Shubrook, J.H.; Skolnik, N.; Trujillo, J. Pharmacologic Approaches to glycemic treatment of type 2 diabetes: Synopsis of the 2020 American diabetes Association’s standards of medical care in diabetes clinical guideline. Ann. Intern. Med. 2020, 173, 813e21. [Google Scholar] [CrossRef]
- Fujimoto, K.; Iwakura, T.; Aburaya, M.; Matsuoka, N. Twice-daily insulin degludec/insulin aspart effectively improved morning and evening glucose levels and quality of life in patients previously treated with premixed insulin: An observational study. Diabetol. Metab. Syndr. 2018, 10, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Bradley, M.C.; Chillarige, Y.; Lee, H.; Wu, X.; Parulekar, S.; Muthuri, S.; Wernecke, M.; MaCurdy, T.E.; Kelman, J.A.; Graham, D.J. Severe Hypoglycemia Risk With Long-Acting Insulin Analogs vs Neutral Protamine Hagedorn Insulin. JAMA Intern. Med. 2021, 181, 598. [Google Scholar] [CrossRef]
- Betônico, C.C.; Titan, S.M.O.; Lira, A.; Pelaes, T.S.; Correa-Giannella, M.L.C.; Nery, M.; Queiroz, M. Insulin Glargine U100 Improved Glycemic Control and Reduced Nocturnal Hypoglycemia in Patients with Type 2 Diabetes Mellitus and Chronic Kidney Disease Stages 3 and 4. Clin. Ther. 2019, 41, 2008–2020.e3. [Google Scholar] [CrossRef]
- Zçelik, S.; Çelik, M.; Vural, A.; Aydın, B.; Özçelik, M.; Gozu, H. Outcomes of transition from premixed and intensive insulin therapies to insulin aspart/degludec co-formulation in type 2 diabetes mellitus: A real-world experience. Arch. Med. Sci. 2021, 17, 1–8. [Google Scholar] [CrossRef]
- Blonde, L.; Aschner, P.; Bailey, C.; Ji, L.; Leiter, L.A.; Matthaei, S. Global Partnership for Effective Diabetes Management. Matthaei S on behalf of the Global Partnership for Effective Diabetes Management. Gaps and barriers in the control of blood glucose in people with type 2 diabetes. Diabetes Vasc. Dis. Res. 2017, 14, 172e83. [Google Scholar] [CrossRef] [Green Version]
- Reach, G.; Pechtner, V.; Gentilella, R.; Corcos, A.; Ceriello, A. Clinical inertia and its impact on treatment intensification in people with type 2 diabetes mellitus. Diabetes Metab. 2017, 43, 501–511. [Google Scholar] [CrossRef]
- Sjöblom, P.; AndersTengblad, Löfgren, U.B.; Lannering, C.; Anderberg, N.; Rosenqvist, U.; Mölstad, S.; Ostgren, C.J. Can diabetes medication be reduced in elderly patients? An observational study of diabetes drug withdrawal in nursing home patients with tight glycaemic control. Dib. Res. Clin. Pract. 2008, 82, 197–202. [Google Scholar] [CrossRef] [Green Version]
- Abdelhafiz, A.H.; Chakravorty, P.; Gupta, S.; Haque, A.; Sinclair, A.J. Can hypoglycaemic medications be withdrawn in older people with type 2 diabetes? Int. J. Clin. Pract. 2014, 68, 790–792. [Google Scholar] [CrossRef]
- Huang, E.S.; Liu, J.Y.; Moffet, H.H.; John, P.M.; Karter, A.J. Glycemic control, complications, and death in older diabetic patients: The diabetes and aging study. Diabetes Care 2011, 34, 1329–1336. [Google Scholar] [CrossRef] [Green Version]
- Huang, E.S.; Zhang, Q.; Gandra, N.; Chin, M.H.; Meltzer, D.O. The Effect of Comorbid Illness and Functional Status on the Expected Benefits of Intensive Glucose Control in Older Patients with Type 2 Diabetes: A Decision Analysis. Ann. Intern. Med. 2008, 149, 11–19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cox, D.J.; Kovatchev, B.P.; Gonder-Frederick, L.A.; Summers, K.H.; McCall, A.; Grimm, K.J.; Clarke, W.L. Relationships Between Hyperglycemia and Cognitive Performance Among Adults With Type 1 and Type 2 Diabetes. Diabetes Care 2005, 28, 71–77. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, S.J.; Eng, C. Goals of glycemic control in frail older patients with diabetes. JAMA 2011, 305, 1350–1351. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abdelhafiz, A.; Bisht, S.; Kovacevic, I.; Pennells, D.; Sinclair, A. Insulin in Frail, Older People with Type 2 Diabetes—Low Threshold for Therapy. Diabetology 2022, 3, 369–383. [Google Scholar] [CrossRef]
- Abdelhafiz, A.H.; Rodríguez-Mañas, L.; Morley, J.E.; Sinclair, A.J. Hypoglycemia in Older People—A Less Well Recognized Risk Factor for Frailty. Aging Dis. 2015, 6, 156–167. [Google Scholar] [CrossRef] [Green Version]
- Rodriguez-Mañas, L.; Laosa, O.; Vellas, B.; Paolisso, G.; Topinkova, E.; Oliva-Moreno, J.; Bourdel-Marchasson, I.; Izquierdo, M.; Hood, K.; Zeyfang, A.; et al. Effectiveness of a multimodal intervention in functionally impaired older people with type 2 diabetes mellitus. J. Cachex- Sarcopenia Muscle 2019, 10, 721–733. [Google Scholar] [CrossRef] [Green Version]
- De Decker, L.; Hanon, O.; Boureau, A.S.; Chapelet, G.; Dibon, C.; Pichelin, M.; Berrut, G.; Cariou, B. Association between hypoglycemia and the burden of comorbidities in hospitalized vulnerable older diabetic patients: A cross-sectional, population-based study. Diabetes Ther. 2017, 8, 1405–1413. [Google Scholar] [CrossRef] [Green Version]
- Kong, L.; Zhao, H.; Fan, J.; Wang, Q.; Li, J.; Bai, J.; Mao, J. Predictors of frailty among Chinese community-dwelling older adults with type 2 diabetes: A cross-sectional survey. BMJ Open 2021, 11, e041578. [Google Scholar] [CrossRef]
- Bilgin, S.; Aktas, G.; Kurtkulagi, O.; Atak, B.M.; Duman, T.T. Edmonton frail score is associated with diabetic control in elderly type 2 diabetic subjects. J. Diabetes Metab. Disord. 2020, 19, 511–514. [Google Scholar] [CrossRef]
- Hyde, Z.; Smith, K.; Flicker, L.; Atkinson, D.; Fenner, S.; Skeaf, L.; Malay, R.; Giudice, D.L. HbA1c Is Associated with Frailty in a Group of Aboriginal Australians. J. Frailty Aging 2019, 8, 17–20. [Google Scholar] [CrossRef]
- Aguayo, G.A.; Hulman, A.; Vaillant, M.T.; Donneau, A.-F.; Schritz, A.; Stranges, S.; Malisoux, L.; Huiart, L.; Guillaume, M.; Sabia, S.; et al. Prospective Association Among Diabetes Diagnosis, HbA1c, Glycemia, and Frailty Trajectories in an Elderly Population. Diabetes Care 2019, 42, 1903–1911. [Google Scholar] [CrossRef]
- Abdelhafiz, A.; Sinclair, A. Metabolic phenotypes explain the relationship between dysglycaemia and frailty in older people with type 2 diabetes. J. Diabetes Its Complicat. 2022, 36, 108144. [Google Scholar] [CrossRef]
- Ahlqvist, E.; Storm, P.; Käräjämäki, A.; Martinell, M.; Dorkhan, M.; Carlsson, A.; Vikman, P.; Prasad, R.B.; Aly, D.M.; Almgren, P.; et al. Novel subgroups of adult-onset diabetes and their association with outcomes: A data-driven cluster analysis of six variables. Lancet Diabetes Endocrinol. 2018, 6, 361–369. [Google Scholar] [CrossRef] [Green Version]
- Monti, G.; Moreira, D.G.; Richner, M.; Mutsaers, H.A.M.; Ferreira, N.; Jan, A. GLP-1 Receptor Agonists in Neurodegeneration: Neurovascular Unit in the Spotlight. Cells 2022, 11, 2023. [Google Scholar] [CrossRef]
- Ikejima, S.; Kondo, S.; Sakai, T.; Taniai, H.; Takahashi, T.; Umezu, J.; Iseka, M.; Inoue, M.; Nishihara, H.; Murata, K.; et al. Novel Approach to Sarcopenia in Diabetic Patients Treated with GLP-1 Receptor Agonists (GLP-1RA). Diabetes 2018, 67, 673-P. [Google Scholar] [CrossRef]
- Sasaki, T.; Sugawara, M.; Fukuda, M. Sodium-glucose cotransporter 2 inhibitor-induced changes in body composition and simultaneous changes in metabolic profile: 52-week prospective LIGHT (Luseogliflozin: The Components of Weight Loss in Japanese Patients with Type 2 Diabetes Mellitus) Study. J. Diabetes Investig. 2018, 10, 108–117. [Google Scholar] [CrossRef]
- Bouchi, R.; Terashima, M.; Sasahara, Y.; Asakawa, M.; Fukuda, T.; Takeuchi, T.; Nakano, Y.; Murakami, M.; Minami, I.; Izumiyama, H.; et al. Luseogliflozin reduces epicardial fat accumulation in patients with type 2 diabetes: A pilot study. Cardiovasc. Diabetol. 2017, 16, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Cefalu, W.T.; Leiter, L.A.; Yoon, K.H.; Arias, P.; Niskanen, L.; Xie, J.; Balis, D.A.; Canovatchel, W.; Meininger, G. Efficacy and safety of canagliflozin versus glimepiride in patients with type 2 diabetes inadequately controlled with metformin (CANTATA-SU): 52 week results from a randomised, double-blind, phase 3 non-inferiority trial. Lancet 2013, 382, 941–950. [Google Scholar] [CrossRef]
- Sugiyama, S.; Jinnouchi, H.; Kurinami, N.; Hieshima, K.; Yoshida, A.; Jinnouchi, K.; Nishimura, H.; Suzuki, T.; Miyamoto, F.; Kajiwara, K.; et al. Dapagliflozin Reduces Fat Mass without Affecting Muscle Mass in Type 2 Diabetes. J. Atheroscler. Thromb. 2018, 25, 467–476. [Google Scholar] [CrossRef] [Green Version]
- Sano, M.; Meguro, S.; Kawai, T.; Suzuki, Y. Increased grip strength with sodium–glucose cotransporter 2. J. Diabetes 2016, 8, 736–737. [Google Scholar] [CrossRef] [Green Version]
- Bajaj, H.S.; Bergenstal, R.M.; Christoffersen, A.; Davies, M.J.; Gowda, A.; Isendahl, J.; Lingvay, I.; Senior, P.A.; Silver, R.J.; Trevisan, R.; et al. Switching to Once-Weekly Insulin Icodec Versus Once-Daily Insulin Glargine U100 in Type 2 Diabetes Inadequately Controlled on Daily Basal Insulin: A Phase 2 Randomized Controlled Trial. Diabetes Care 2021, 44, 1586–1594. [Google Scholar] [CrossRef] [PubMed]


Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sinclair, A.J.; Abdelhafiz, A.H. Metabolic Impact of Frailty Changes Diabetes Trajectory. Metabolites 2023, 13, 295. https://doi.org/10.3390/metabo13020295
Sinclair AJ, Abdelhafiz AH. Metabolic Impact of Frailty Changes Diabetes Trajectory. Metabolites. 2023; 13(2):295. https://doi.org/10.3390/metabo13020295
Chicago/Turabian StyleSinclair, Alan J., and Ahmed H. Abdelhafiz. 2023. "Metabolic Impact of Frailty Changes Diabetes Trajectory" Metabolites 13, no. 2: 295. https://doi.org/10.3390/metabo13020295
APA StyleSinclair, A. J., & Abdelhafiz, A. H. (2023). Metabolic Impact of Frailty Changes Diabetes Trajectory. Metabolites, 13(2), 295. https://doi.org/10.3390/metabo13020295