

Iron Homeostasis-Related Parameters and Hepcidin/Ferritin Ratio: Emerging Sex-Specific Predictive Markers for Metabolic Syndrome

 , , ,
, , ,  and
and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Participants
2.2. Specimen Collection and Laboratory Investigations
2.3. Statistical Analysis
3. Results
3.1. Clinicolaboratory Characteristics of the Study Population
3.2. Association between HOMA-IR Index and Iron-Related Parameters
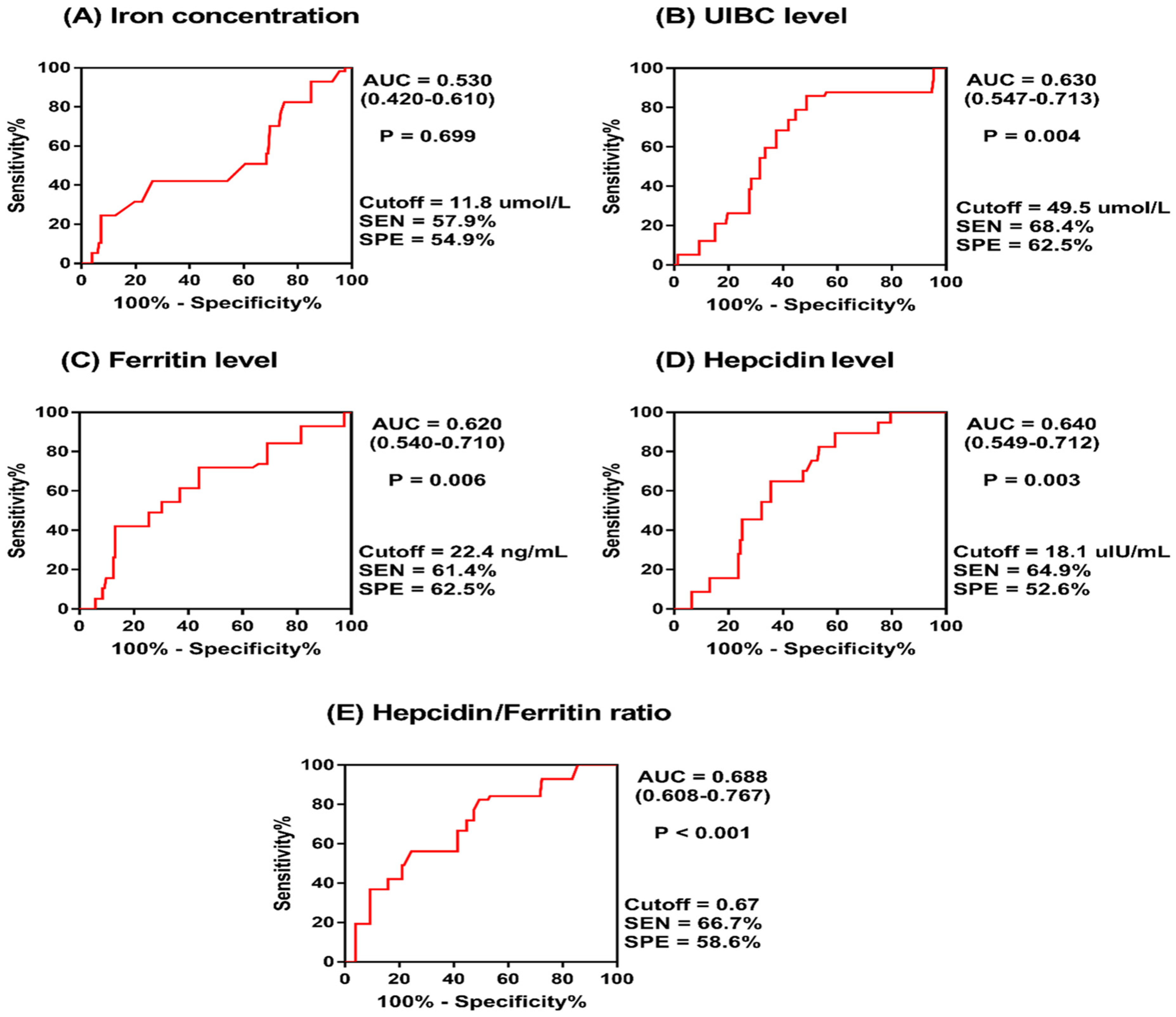
3.3. Diagnostic Relevance of Circulatory Iron-Related Parameters for Metabolic Syndrome
3.4. Logistic Regression Analysis of Factors Influencing the Risk of Developing Metabolic Syndrome in the Study Population
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mohamed, S.M.; Shalaby, M.A.; El-Shiekh, R.A.; El-Banna, H.A.; Emam, S.R.; Bakr, A.F. Metabolic syndrome: Risk factors, diagnosis, pathogenesis, and management with natural approaches. Food Chem. Adv. 2023, 3, 100335. [Google Scholar] [CrossRef]
- Aljuhani, O.; Alkahtani, S.; Alhussain, M.; Smith, L.; Habib, S.S. Associations of Physical Activity and Sedentary Time with Metabolic Syndrome in Saudi Adult Males. Risk Manag. Healthc. Policy 2020, 13, 1839–1847. [Google Scholar] [CrossRef] [PubMed]
- Wu, S.; Xu, W.; Guan, C.; Lv, M.; Jiang, S.; Jinhua, Z. Global burden of cardiovascular disease attributable to metabolic risk factors, 1990-2019: An analysis of observational data from a 2019 Global Burden of Disease study. BMJ Open 2023, 13, e069397. [Google Scholar] [CrossRef] [PubMed]
- Gosadi, I.M. Assessment of the environmental and genetic factors influencing prevalence of metabolic syndrome in Saudi Arabia. Saudi Med. J. 2016, 37, 12–20. [Google Scholar] [CrossRef]
- Fahed, G.; Aoun, L.; Bou Zerdan, M.; Allam, S.; Bou Zerdan, M.; Bouferraa, Y.; Assi, H.I. Metabolic Syndrome: Updates on Pathophysiology and Management in 2021. Int. J. Mol. Sci. 2022, 23, 786. [Google Scholar] [CrossRef] [PubMed]
- Ho, C.Y.; Lee, J.I.; Huang, S.P.; Chen, S.C.; Geng, J.H. A Genome-Wide Association Study of Metabolic Syndrome in the Taiwanese Population. Nutrients 2023, 16, 77. [Google Scholar] [CrossRef]
- Jha, B.K.; Sherpa, M.L.; Imran, M.; Mohammed, Y.; Jha, L.A.; Paudel, K.R.; Jha, S.K. Progress in Understanding Metabolic Syndrome and Knowledge of Its Complex Pathophysiology. Diabetology 2023, 4, 134–159. [Google Scholar] [CrossRef]
- Ahmadabad, A.D.; Jahangiry, L.; Gilani, N.; Farhangi, M.A.; Mohammadi, E.; Ponnet, K. Lifestyle patterns, nutritional, and metabolic syndrome determinants in a sample of the older Iranian population. BMC Geriatr. 2024, 24, 36. [Google Scholar] [CrossRef]
- Lin, Y.; Fan, R.; Hao, Z.; Li, J.; Yang, X.; Zhang, Y.; Xia, Y. The Association Between Physical Activity and Insulin Level Under Different Levels of Lipid Indices and Serum Uric Acid. Front. Physiol. 2022, 13, 809669. [Google Scholar] [CrossRef]
- Chomiuk, T.; Niezgoda, N.; Mamcarz, A.; Sliz, D. Physical activity in metabolic syndrome. Front. Physiol. 2024, 15, 1365761. [Google Scholar] [CrossRef]
- Clemente-Suarez, V.J.; Martin-Rodriguez, A.; Redondo-Florez, L.; Lopez-Mora, C.; Yanez-Sepulveda, R.; Tornero-Aguilera, J.F. New Insights and Potential Therapeutic Interventions in Metabolic Diseases. Int. J. Mol. Sci. 2023, 24, 10672. [Google Scholar] [CrossRef] [PubMed]
- Kraft, P.; Kraft, B. Explaining socioeconomic disparities in health behaviours: A review of biopsychological pathways involving stress and inflammation. Neurosci. Biobehav. Rev. 2021, 127, 689–708. [Google Scholar] [CrossRef] [PubMed]
- Hill-Briggs, F.; Adler, N.E.; Berkowitz, S.A.; Chin, M.H.; Gary-Webb, T.L.; Navas-Acien, A.; Thornton, P.L.; Haire-Joshu, D. Social Determinants of Health and Diabetes: A Scientific Review. Diabetes Care 2020, 44, 258–279. [Google Scholar] [CrossRef] [PubMed]
- Srikanthan, K.; Feyh, A.; Visweshwar, H.; Shapiro, J.I.; Sodhi, K. Systematic Review of Metabolic Syndrome Biomarkers: A Panel for Early Detection, Management, and Risk Stratification in the West Virginian Population. Int. J. Med. Sci. 2016, 13, 25–38. [Google Scholar] [CrossRef]
- Akinyemiju, T.; Moore, J.X.; Judd, S.E.; Pisu, M.; Goodman, M.; Howard, V.J.; Long, L.; Safford, M.; Gilchrist, S.C.; Cushman, M. Pre-diagnostic biomarkers of metabolic dysregulation and cancer mortality. Oncotarget 2018, 9, 16099–16109. [Google Scholar] [CrossRef]
- Fawzy, M.S.; AlSel, B.T.A. Association of Serum Uric Acid Levels with Components of Metabolic Syndrome: A Cross-Sectional Analysis in a Saudi Adult Population. Int. J. Biomed. 2020, 10, 457–466. [Google Scholar] [CrossRef]
- Camaschella, C.; Nai, A.; Silvestri, L. Iron metabolism and iron disorders revisited in the hepcidin era. Haematologica 2020, 105, 260–272. [Google Scholar] [CrossRef]
- Park, S.K.; Ryoo, J.H.; Kim, M.G.; Shin, J.Y. Association of serum ferritin and the development of metabolic syndrome in middle-aged Korean men: A 5-year follow-up study. Diabetes Care 2012, 35, 2521–2526. [Google Scholar] [CrossRef]
- Shim, Y.S.; Kang, M.J.; Oh, Y.J.; Baek, J.W.; Yang, S.; Hwang, I.T. Association of serum ferritin with insulin resistance, abdominal obesity, and metabolic syndrome in Korean adolescent and adults: The Korean National Health and Nutrition Examination Survey, 2008 to 2011. Medicine 2017, 96, e6179. [Google Scholar] [CrossRef]
- Chen, L.; Li, Y.; Zhang, F.; Zhang, S.; Zhou, X.; Ji, L. Association of serum ferritin levels with metabolic syndrome and insulin resistance in a Chinese population. J. Diabetes Its Complicat. 2017, 31, 364–368. [Google Scholar] [CrossRef]
- Hao, H.; Chen, Y.; Xiaojuan, J.; Siqi, Z.; Hailiang, C.; Xiaoxing, S.; Qikai, W.; Mingquan, X.; Jiangzhou, F.; Hongfeng, G. The Association Between METS-IR and Serum Ferritin Level in United States Female: A Cross-Sectional Study Based on NHANES. Front. Med. 2022, 9, 925344. [Google Scholar] [CrossRef] [PubMed]
- GBD 2017 Saudi Arabia Collaborators. The burden of disease in Saudi Arabia 1990–2017: Results from the Global Burden of Disease Study 2017. Lancet. Planet. Health 2020, 4, e195–e208. [Google Scholar] [CrossRef]
- Alshehri, F.F. Understanding the prevalence, progression, and management of metabolic syndrome in Saudi Arabia. Saudi Med. J. 2023, 44, 973–986. [Google Scholar] [CrossRef] [PubMed]
- Azizi, F.; Hadaegh, F.; Hosseinpanah, F.; Mirmiran, P.; Amouzegar, A.; Abdi, H.; Asghari, G.; Parizadeh, D.; Montazeri, S.A.; Lotfaliany, M.; et al. Metabolic health in the Middle East and north Africa. Lancet. Diabetes Endocrinol. 2019, 7, 866–879. [Google Scholar] [CrossRef]
- Grundy, S.M.; Cleeman, J.I.; Daniels, S.R.; Donato, K.A.; Eckel, R.H.; Franklin, B.A.; Gordon, D.J.; Krauss, R.M.; Savage, P.J.; Smith, S.C., Jr.; et al. Diagnosis and management of the metabolic syndrome: An American Heart Association/National Heart, Lung, and Blood Institute Scientific Statement. Circulation 2005, 112, 2735–2752. [Google Scholar] [CrossRef] [PubMed]
- Al-Rubean, K.; Youssef, A.M.; AlFarsi, Y.; Al-Sharqawi, A.H.; Bawazeer, N.; AlOtaibi, M.T.; AlRumaih, F.I.; Zaidi, M.S. Anthropometric cutoff values for predicting metabolic syndrome in a Saudi community: From the SAUDI-DM study. Ann. Saudi Med. 2017, 37, 21–30. [Google Scholar] [CrossRef]
- Huang, P.L. A comprehensive definition for metabolic syndrome. Dis. Models Mech. 2009, 2, 231–237. [Google Scholar] [CrossRef]
- Scott, R.; Donoghoe, M.; Watts, G.F.; O’Brien, R.; Pardy, C.; Taskinen, M.R.; Davis, T.M.; Colman, P.G.; Manning, P.; Fulcher, G.; et al. Impact of metabolic syndrome and its components on cardiovascular disease event rates in 4900 patients with type 2 diabetes assigned to placebo in the FIELD randomised trial. Cardiovasc. Diabetol. 2011, 10, 102. [Google Scholar] [CrossRef]
- Al-Rubeaan, K.; Bawazeer, N.; Al Farsi, Y.; Youssef, A.M.; Al-Yahya, A.A.; AlQumaidi, H.; Al-Malki, B.M.; Naji, K.A.; Al-Shehri, K.; Al Rumaih, F.I. Prevalence of metabolic syndrome in Saudi Arabia—A cross sectional study. BMC Endocr. Disord. 2018, 18, 16. [Google Scholar] [CrossRef]
- Friedewald, W.T.; Levy, R.I.; Fredrickson, D.S. Estimation of the concentration of low-density lipoprotein cholesterol in plasma, without use of the preparative ultracentrifuge. Clin. Chem. 1972, 18, 499–502. [Google Scholar] [CrossRef]
- Vogeser, M.; Konig, D.; Frey, I.; Predel, H.G.; Parhofer, K.G.; Berg, A. Fasting serum insulin and the homeostasis model of insulin resistance (HOMA-IR) in the monitoring of lifestyle interventions in obese persons. Clin. Biochem. 2007, 40, 964–968. [Google Scholar] [CrossRef]
- Ruze, R.; Liu, T.; Zou, X.; Song, J.; Chen, Y.; Xu, R.; Yin, X.; Xu, Q. Obesity and type 2 diabetes mellitus: Connections in epidemiology, pathogenesis, and treatments. Front. Endocrinol. 2023, 14, 1161521. [Google Scholar] [CrossRef]
- Alberti, K.G.; Zimmet, P.; Shaw, J. Metabolic syndrome—A new world-wide definition. A Consensus Statement from the International Diabetes Federation. Diabet. Med. 2006, 23, 469–480. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez-Dominguez, A.; Visiedo-Garcia, F.M.; Dominguez-Riscart, J.; Gonzalez-Dominguez, R.; Mateos, R.M.; Lechuga-Sancho, A.M. Iron Metabolism in Obesity and Metabolic Syndrome. Int. J. Mol. Sci. 2020, 21, 5529. [Google Scholar] [CrossRef]
- Kerkadi, A.; Mohsen Ali, R.; Shehada, A.A.H.; Abdelnasser AbouHassanein, E.; Moawad, J.; Bawadi, H.; Shi, Z. Association between central obesity indices and iron status indicators among Qatari adults. PLoS ONE 2021, 16, e0250759. [Google Scholar] [CrossRef] [PubMed]
- Al Akl, N.S.; Khalifa, O.; Errafii, K.; Arredouani, A. Association of dyslipidemia, diabetes and metabolic syndrome with serum ferritin levels: A middle eastern population-based cross-sectional study. Sci. Rep. 2021, 11, 24080. [Google Scholar] [CrossRef]
- Wang, J.W.; Jin, C.H.; Ke, J.F.; Ma, Y.L.; Wang, Y.J.; Lu, J.X.; Li, M.F.; Li, L.X. Serum iron is closely associated with metabolic dysfunction-associated fatty liver disease in type 2 diabetes: A real-world study. Front. Endocrinol. 2022, 13, 942412. [Google Scholar] [CrossRef]
- Hilton, C.; Sabaratnam, R.; Drakesmith, H.; Karpe, F. Iron, glucose and fat metabolism and obesity: An intertwined relationship. Int. J. Obes. 2023, 47, 554–563. [Google Scholar] [CrossRef] [PubMed]
- Tang, Q.; Liu, Z.; Tang, Y.; Tan, A.; Gao, Y.; Lu, Z.; Wang, Q.; Chen, Y.; Wu, C.; Zhang, H.; et al. High serum ferritin level is an independent risk factor for metabolic syndrome in a Chinese male cohort population. Diabetol. Metab. Syndr. 2015, 7, 11. [Google Scholar] [CrossRef]
- Lee, M.K.; Han, K.; Kwon, H.S. Age-specific diabetes risk by the number of metabolic syndrome components: A Korean nationwide cohort study. Diabetol. Metab. Syndr. 2019, 11, 112. [Google Scholar] [CrossRef]
- Tran, T.N.; Tran, H.D.; Tran-Huu, T.T.; Tran, D.M.; Tran, Q.N. A Cross-Sectional Study of Serum Ferritin Levels in Vietnamese Adults with Metabolic Syndrome. Diabetes Metab. Syndr. Obes. Targets Ther. 2022, 15, 1517–1523. [Google Scholar] [CrossRef] [PubMed]
- Srivastav, S.K.; Mir, I.A.; Bansal, N.; Singh, P.K.; Kumari, R.; Deshmukh, A. Serum Ferritin in Metabolic Syndrome-Mechanisms and Clinical Applications. Pathophysiology 2022, 29, 319–325. [Google Scholar] [CrossRef] [PubMed]
- Momeni, A.; Behradmanesh, M.S.; Kheiri, S.; Abasi, F. Serum ferritin has correlation with HbA1c in type 2 diabetic patients. Adv. Biomed. Res. 2015, 4, 74. [Google Scholar] [CrossRef]
- Duan, Y.; Zhang, W.; Li, Z.; Niu, Y.; Chen, Y.; Liu, X.; Dong, Z.; Zheng, Y.; Chen, X.; Feng, Z.; et al. Predictive ability of obesity- and lipid-related indicators for metabolic syndrome in relatively healthy Chinese adults. Front. Endocrinol. 2022, 13, 1016581. [Google Scholar] [CrossRef]
- Stanciu, S.; Rusu, E.; Miricescu, D.; Radu, A.C.; Axinia, B.; Vrabie, A.M.; Ionescu, R.; Jinga, M.; Sirbu, C.A. Links between Metabolic Syndrome and Hypertension: The Relationship with the Current Antidiabetic Drugs. Metabolites 2023, 13, 87. [Google Scholar] [CrossRef]
- Rattanatham, R.; Tangpong, J.; Chatatikun, M.; Sun, D.; Kawakami, F.; Imai, M.; Klangbud, W.K. Assessment of eight insulin resistance surrogate indexes for predicting metabolic syndrome and hypertension in Thai law enforcement officers. PeerJ 2023, 11, e15463. [Google Scholar] [CrossRef]
- Cho, M.R.; Park, J.K.; Choi, W.J.; Cho, A.R.; Lee, Y.J. Serum ferritin level is positively associated with insulin resistance and metabolic syndrome in postmenopausal women: A nationwide population-based study. Maturitas 2017, 103, 3–7. [Google Scholar] [CrossRef]
- Suarez-Ortegon, M.F.; Ensaldo-Carrasco, E.; Shi, T.; McLachlan, S.; Fernandez-Real, J.M.; Wild, S.H. Ferritin, metabolic syndrome and its components: A systematic review and meta-analysis. Atherosclerosis 2018, 275, 97–106. [Google Scholar] [CrossRef]
- Vaquero, M.P.; Martinez-Maqueda, D.; Gallego-Narbon, A.; Zapatera, B.; Perez-Jimenez, J. Relationship between iron status markers and insulin resistance: An exploratory study in subjects with excess body weight. PeerJ 2020, 8, e9528. [Google Scholar] [CrossRef]
- Wang, M.; Zhao, A.; Szeto, I.M.; Wu, W.; Ren, Z.; Li, T.; Feng, H.; Wang, P.; Wang, Y.; Zhang, Y. Association of serum ferritin with metabolic syndrome in eight cities in China. Food Sci. Nutr. 2020, 8, 1406–1414. [Google Scholar] [CrossRef]
- Datz, C.; Felder, T.K.; Niederseer, D.; Aigner, E. Iron homeostasis in the metabolic syndrome. Eur. J. Clin. Investig. 2013, 43, 215–224. [Google Scholar] [CrossRef]
- Qiu, F.; Wu, L.; Yang, G.; Zhang, C.; Liu, X.; Sun, X.; Chen, X.; Wang, N. The role of iron metabolism in chronic diseases related to obesity. Mol. Med. 2022, 28, 130. [Google Scholar] [CrossRef] [PubMed]
- Galetti, V.; Stoffel, N.U.; Sieber, C.; Zeder, C.; Moretti, D.; Zimmermann, M.B. Threshold ferritin and hepcidin concentrations indicating early iron deficiency in young women based on upregulation of iron absorption. EClinicalMedicine 2021, 39, 101052. [Google Scholar] [CrossRef]
- Lotfi, R.; Kroll, C.; Plonne, D.; Jahrsdorfer, B.; Schrezenmeier, H. Hepcidin/Ferritin Quotient Helps to Predict Spontaneous Recovery from Iron Loss following Blood Donation. Transfus. Med. Hemother. 2015, 42, 390–395. [Google Scholar] [CrossRef]
- Chibanda, Y.; Brookes, M.; Churchill, D.; Al-Hassi, H. The Ferritin, Hepcidin and Cytokines Link in the Diagnoses of Iron Deficiency Anaemia during Pregnancy: A Review. Int. J. Mol. Sci. 2023, 24, 13323. [Google Scholar] [CrossRef]
- Han, L.L.; Wang, Y.X.; Li, J.; Zhang, X.L.; Bian, C.; Wang, H.; Du, S.; Suo, L.N. Gender differences in associations of serum ferritin and diabetes, metabolic syndrome, and obesity in the China Health and Nutrition Survey. Mol. Nutr. Food Res. 2014, 58, 2189–2195. [Google Scholar] [CrossRef] [PubMed]
- Calcaterra, V.; Larizza, D.; De Silvestri, A.; Albertini, R.; Vinci, F.; Regalbuto, C.; Dobbiani, G.; Montalbano, C.; Pelizzo, G.; Cena, H. Gender-based differences in the clustering of metabolic syndrome factors in children and adolescents. J. Pediatr. Endocrinol. Metab. 2020, 33, 279–288. [Google Scholar] [CrossRef] [PubMed]
- Nouri-Keshtkar, M.; Shojaei Shahrokhabadi, M.; Ghaheri, A.; Hosseini, R.; Ketabi, H.; Farjam, M.; Chen, D.G.; Rezaeian, M.; Homayounfar, R.; Tahamtani, Y.; et al. Role of gender in explaining metabolic syndrome risk factors in an Iranian rural population using structural equation modelling. Sci. Rep. 2023, 13, 16007. [Google Scholar] [CrossRef]
- Ramezankhani, A.; Azizi, F.; Hadaegh, F. Gender differences in changes in metabolic syndrome status and its components and risk of cardiovascular disease: A longitudinal cohort study. Cardiovasc. Diabetol. 2022, 21, 227. [Google Scholar] [CrossRef]
- Chang, S.H.; Chang, Y.Y.; Jeng, W.J.; Wai, J.P.M. Efficacy of a multidimensional self-management intervention on low-education women with metabolic syndrome: A cluster randomized controlled trial. Sci. Rep. 2023, 13, 10358. [Google Scholar] [CrossRef]
- Dev, R.; Behlouli, H.; Parry, M.; Raparelli, V.; Norris, C.M.; Pilote, L.; Consortium, G.-F. Impact of Sex and Gender on Metabolic Syndrome in Adults: A Retrospective Cohort Study from the Canadian Primary Care Sentinel Surveillance Network. Can. J. Diabetes 2024, 48, 36–43.e2. [Google Scholar] [CrossRef]
- Boisvenue, J.J.; Oliva, C.U.; Manca, D.P.; Johnson, J.A.; Yeung, R.O. Identifying Sex-Specific Differences in Young-Onset Metabolic Syndrome Using Primary Care Electronic Medical Record. Metab. Syndr. Relat. Disord. 2023, 21, 133–140. [Google Scholar] [CrossRef] [PubMed]
- Pucci, G.; Alcidi, R.; Tap, L.; Battista, F.; Mattace-Raso, F.; Schillaci, G. Sex- and gender-related prevalence, cardiovascular risk and therapeutic approach in metabolic syndrome: A review of the literature. Pharmacol. Res. 2017, 120, 34–42. [Google Scholar] [CrossRef]
- Ye, Y.; Zhou, Q.; Dai, W.; Peng, H.; Zhou, S.; Tian, H.; Shen, L.; Han, H. Gender differences in metabolic syndrome and its components in southern china using a healthy lifestyle index: A cross-sectional study. BMC Public Health 2023, 23, 686. [Google Scholar] [CrossRef]
- Gharipour, M.; Nezafati, P.; Sadeghian, L.; Eftekhari, A.; Rothenberg, I.; Jahanfar, S. Precision medicine and metabolic syndrome. ARYA Atheroscler. 2022, 18, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Wang, R.C.; Wang, Z. Precision Medicine: Disease Subtyping and Tailored Treatment. Cancers 2023, 15, 3837. [Google Scholar] [CrossRef] [PubMed]
- Ding, X.; Fang, T.; Pang, X.; Pan, X.; Tong, A.; Lin, Z.; Zheng, S.; Zheng, N. Mitochondrial DNA abnormalities and metabolic syndrome. Front. Cell Dev. Biol. 2023, 11, 1153174. [Google Scholar] [CrossRef]
- Galaris, D.; Barbouti, A.; Pantopoulos, K. Iron homeostasis and oxidative stress: An intimate relationship. Biochim. Biophys. Acta Mol. Cell Res. 2019, 1866, 118535. [Google Scholar] [CrossRef]
- Fillebeen, C.; Lam, N.H.; Chow, S.; Botta, A.; Sweeney, G.; Pantopoulos, K. Regulatory Connections between Iron and Glucose Metabolism. Int. J. Mol. Sci. 2020, 21, 7773. [Google Scholar] [CrossRef]
- Masenga, S.K.; Kabwe, L.S.; Chakulya, M.; Kirabo, A. Mechanisms of Oxidative Stress in Metabolic Syndrome. Int. J. Mol. Sci. 2023, 24, 7898. [Google Scholar] [CrossRef]
- Moreira, A.C.; Mesquita, G.; Gomes, M.S. Ferritin: An Inflammatory Player Keeping Iron at the Core of Pathogen-Host Interactions. Microorganisms 2020, 8, 589. [Google Scholar] [CrossRef] [PubMed]
- Mahroum, N.; Alghory, A.; Kiyak, Z.; Alwani, A.; Seida, R.; Alrais, M.; Shoenfeld, Y. Ferritin—From iron, through inflammation and autoimmunity, to COVID-19. J. Autoimmun. 2022, 126, 102778. [Google Scholar] [CrossRef] [PubMed]
- Silvestri, L.; Pettinato, M.; Furiosi, V.; Bavuso Volpe, L.; Nai, A.; Pagani, A. Managing the Dual Nature of Iron to Preserve Health. Int. J. Mol. Sci. 2023, 24, 3995. [Google Scholar] [CrossRef]
- Barbalho, S.M.; Laurindo, L.F.; Tofano, R.J.; Flato, U.A.P.; Mendes, C.G.; de Alvares Goulart, R.; Briguezi, A.M.G.M.; Bechara, M.D. Dysmetabolic Iron Overload Syndrome: Going beyond the Traditional Risk Factors Associated with Metabolic Syndrome. Endocrines 2023, 4, 18–37. [Google Scholar] [CrossRef]

{kind=link}
| Variables | Non-Metabolic Syndrome | Metabolic Syndrome | p-Value | |
|---|---|---|---|---|
| Number | (n = 106) | (n = 103) | ||
| Age | Mean ± SD | 38.2 ± 11.1 | 50.2 ± 9.1 | <0.001 |
| ≤40 years | 60 (56.6) | 17 (16.5) | <0.001 | |
| >40 years | 46 (43.3) | 86 (83.5) | ||
| Sex | Female | 70 (66) | 71 (68.9) | 0.661 |
| Male | 36 (34) | 32 (31.1) | ||
| Weight, kg | Mean ± SD | 76.9 ± 16.7 | 95.3 ± 17.7 | <0.001 |
| Height, cm | Mean ± SD | 160.5 ± 8.2 | 161.9 ± 10.6 | 0.287 |
| BMI, Kg/m2 | Mean ± SD | 30.1 ± 7.06 | 36.3 ± 5.7 | <0.001 |
| Abdominal obesity | Negative | 59 (55.7) | 9 (8.7) | <0.001 |
| Positive | 47 (44.3) | 94 (91.3) | ||
| Hypertension | Negative | 95 (89.6) | 33 (32.0) | <0.001 |
| Positive | 11 (10.4) | 70 (68.0) | ||
| Diabetes mellitus | Negative | 97 (91.5) | 39 (37.9) | <0.001 |
| Positive | 9 (8.5) | 64 (62.1) | ||
| Dyslipidemia | Negative | 67 (63.2) | 0 (0.0) | <0.001 |
| Positive | 39 (36.8) | 103 (100) | ||
| TC, mmol/L mean ± SE | 4.50 ± 0.08 | 5.35 ± 0.10 | <0.001 | |
| TG, mmol/L mean ± SE | 1.14 ± 0.04 | 2.30 ± 0.10 | <0.001 | |
| LDL-c, mmol/L mean ± SE | 2.62 ± 0.07 | 3.15 ± 0.08 | <0.001 | |
| HDL-c, mmol/L mean ± SE | 1.3 ± 0.03 | 1.02 ± 0.02 | <0.001 | |
| HOMA-IR mean ± SE | 1.26 ± 0.09 | 2.11 ± 0.1 | <0.001 | |
| FBS, mg/dL mean ± SE | 97.8 ± 1.70 | 174 ± 2.3 | <0.001 | |
| HbA1c% mean ± SE | 2.9 ± 0.05 | 7.0 ± 0.17 | <0.001 | |
| Insulin, μLU/mL mean ± SE | 3.90 ± 0.38 | 10.4 ±1.23 | <0.001 | |
| Fe, μmol/L mean ± SE | 13.8 ± 0.48 | 12.14 ± 0.39 | 0.07 | |
| UIBC, μmol/L mean ± SE | 48.0 ± 1.36 | 51.5 ± 1.1 | 0.05 | |
| Ferritin, ng/mL mean ± SE | 44.5 ± 5.4 | 69.7 ± 7.09 | 0.05 | |
| Hepcidin, μLU/mL mean ± SE | 17.2 ± 2.25 | 24.2 ± 1.93 | 0.03 | |
| Variables | IS (n = 106) | EIR (n = 43) | SIR (n = 60) | p-Value |
|---|---|---|---|---|
| Fe (μmol/L) | 13.8 ± 0.48 | 11.8 ± 0.5 | 9.2 ± 0.4 | 0.002 a |
| UIBC (μmol/L) | 48.0 ± 1.36 | 48.9 ± 1.3 | 58.05 ± 1.8 | 0.001 ab |
| Ferritin (ng/mL) | 44.5 ± 5.4 | 57.8 ± 6.1 | 70.8 ± 5.9 | 0.001 a 0.01 b |
| Hepcidin (μLU/mL) | 17.2 ± 2.25 | 20.8 ± 1.2 | 25.6 ± 1.4 | 0.001 a 0.013 b |
| Variable | Overall (n = 209) | Women (n = 141) | Men (n = 68) | |||
|---|---|---|---|---|---|---|
| AUC | p-Value | AUC | p-Value | AUC | p-Value | |
| Fe, μmol/L | 0.530 | 0.699 | 0.531 | 0.581 | 0.349 | 0.043 |
| UIBC, μmol/L | 0.630 | 0.004 | 0.579 | 0.164 | 0.753 | 0.001 |
| Ferritin, ng/mL | 0.620 | 0.006 | 0.447 | 0.355 | 0.248 | 0.001 |
| Hepcidin, μLU/mL | 0.640 | 0.003 | 0.655 | 0.007 | 0.535 | 0.336 |
| H/F ratio | 0.688 | <0.001 | 0.639 | 0.015 | 0.792 | <0.001 |
| Variable | OR | 95% CI | p-Value |
|---|---|---|---|
| Obesity | 0.832 | 0.333–2.082 | 0.695 |
| Hypertension | 3.957 | 1.840–8.508 | <0.001 |
| Fe, μmol/L | 1.066 | 0.968–1.174 | 0.196 |
| UIBC, μmol/L | 1.045 | 1.004–1.088 | 0.032 |
| H/F ratio | 1.068 | 1.028–1.229 | 0.043 |
| FBS | 1.009 | 1.002–1.015 | 0.007 |
| Constant | 0.003 | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Abu AlSel, B.T.; Mahmoud, A.A.; Hamed, E.O.; Hakim, N.A.; Sindi, A.A.A.; Jawad, N.M.M.; Gusti, A.M.T.; Fawzy, M.S.; Abd El-Fadeal, N.M. Iron Homeostasis-Related Parameters and Hepcidin/Ferritin Ratio: Emerging Sex-Specific Predictive Markers for Metabolic Syndrome. Metabolites 2024, 14, 473. https://doi.org/10.3390/metabo14090473
Abu AlSel BT, Mahmoud AA, Hamed EO, Hakim NA, Sindi AAA, Jawad NMM, Gusti AMT, Fawzy MS, Abd El-Fadeal NM. Iron Homeostasis-Related Parameters and Hepcidin/Ferritin Ratio: Emerging Sex-Specific Predictive Markers for Metabolic Syndrome. Metabolites. 2024; 14(9):473. https://doi.org/10.3390/metabo14090473
Chicago/Turabian StyleAbu AlSel, Baraah T., Abdelrahman A. Mahmoud, Elham O. Hamed, Noor A. Hakim, Abdulmajeed A. A. Sindi, Najlaa M. M. Jawad, Amani M. T. Gusti, Manal S. Fawzy, and Noha M. Abd El-Fadeal. 2024. "Iron Homeostasis-Related Parameters and Hepcidin/Ferritin Ratio: Emerging Sex-Specific Predictive Markers for Metabolic Syndrome" Metabolites 14, no. 9: 473. https://doi.org/10.3390/metabo14090473
APA StyleAbu AlSel, B. T., Mahmoud, A. A., Hamed, E. O., Hakim, N. A., Sindi, A. A. A., Jawad, N. M. M., Gusti, A. M. T., Fawzy, M. S., & Abd El-Fadeal, N. M. (2024). Iron Homeostasis-Related Parameters and Hepcidin/Ferritin Ratio: Emerging Sex-Specific Predictive Markers for Metabolic Syndrome. Metabolites, 14(9), 473. https://doi.org/10.3390/metabo14090473