


Sitting Interruption Modalities during Prolonged Sitting Acutely Improve Postprandial Metabolome in a Crossover Pilot Trial among Postmenopausal Women




Abstract
:1. Introduction
2. Methods
2.1. Study Overview
2.2. Participants
2.3. Study Visits
Condition Protocols
2.4. Metabolomics
2.4.1. Sample Preparation
2.4.2. Gas Chromatography–Mass Spectrometry
2.4.3. Data Processing
2.5. Statistical Analyses
3. Results
3.1. Participant Characteristics
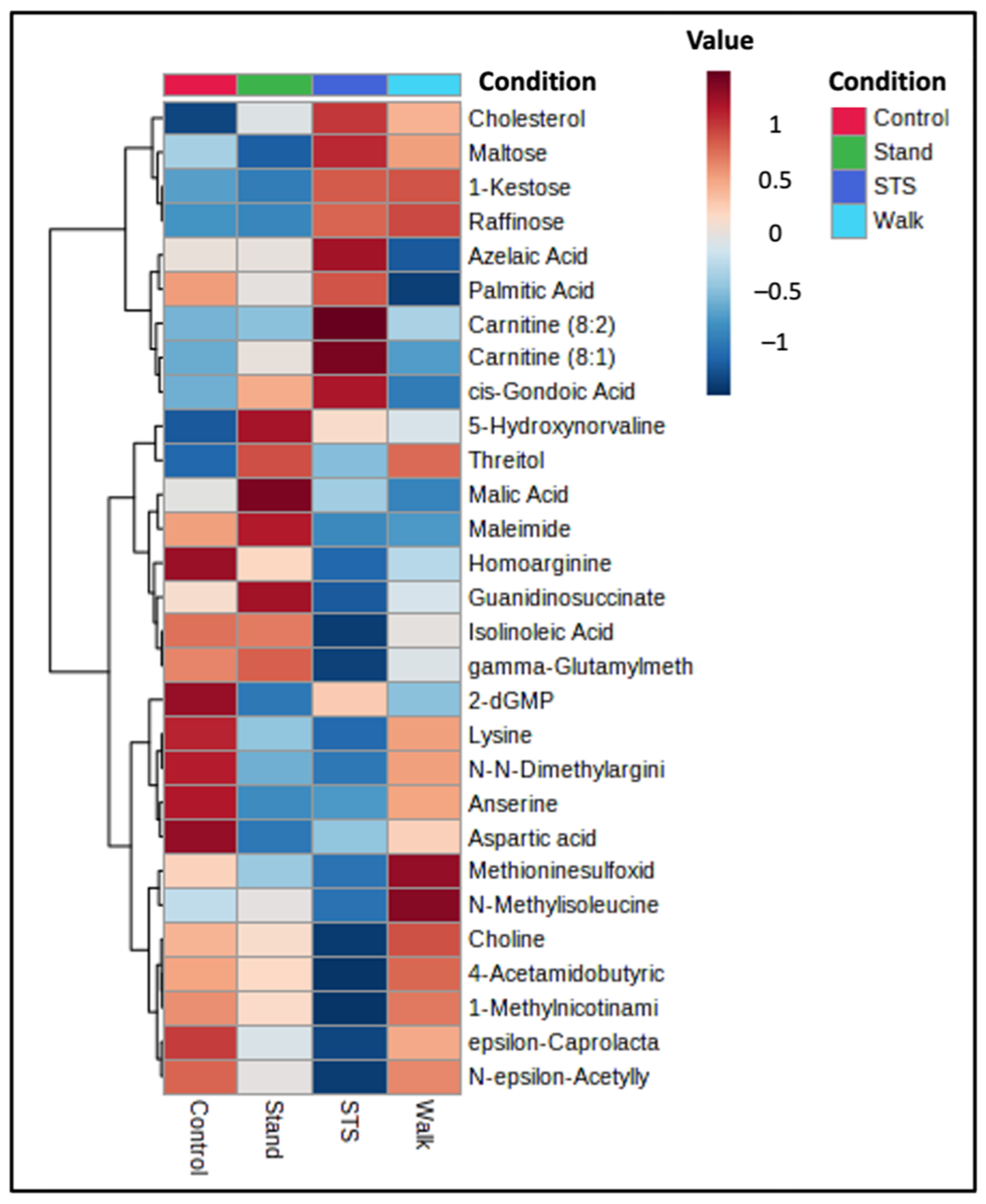
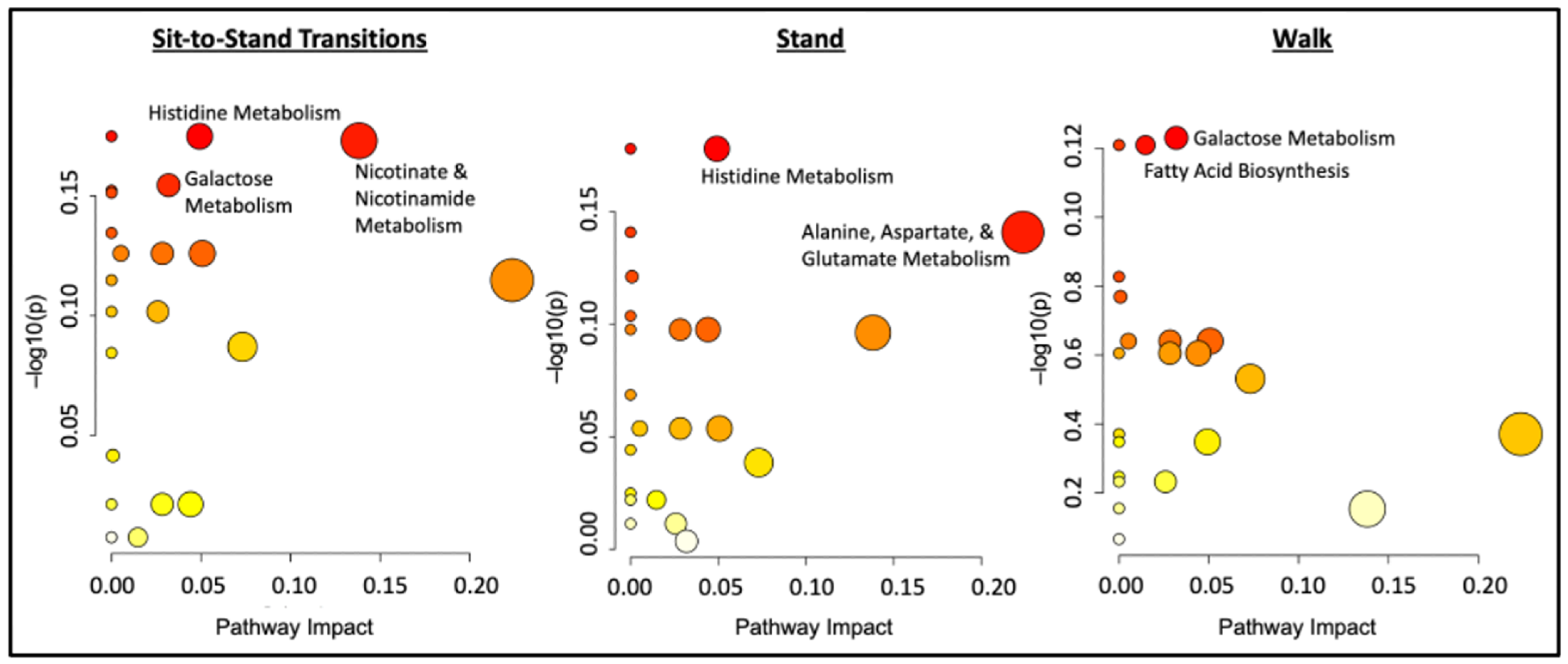
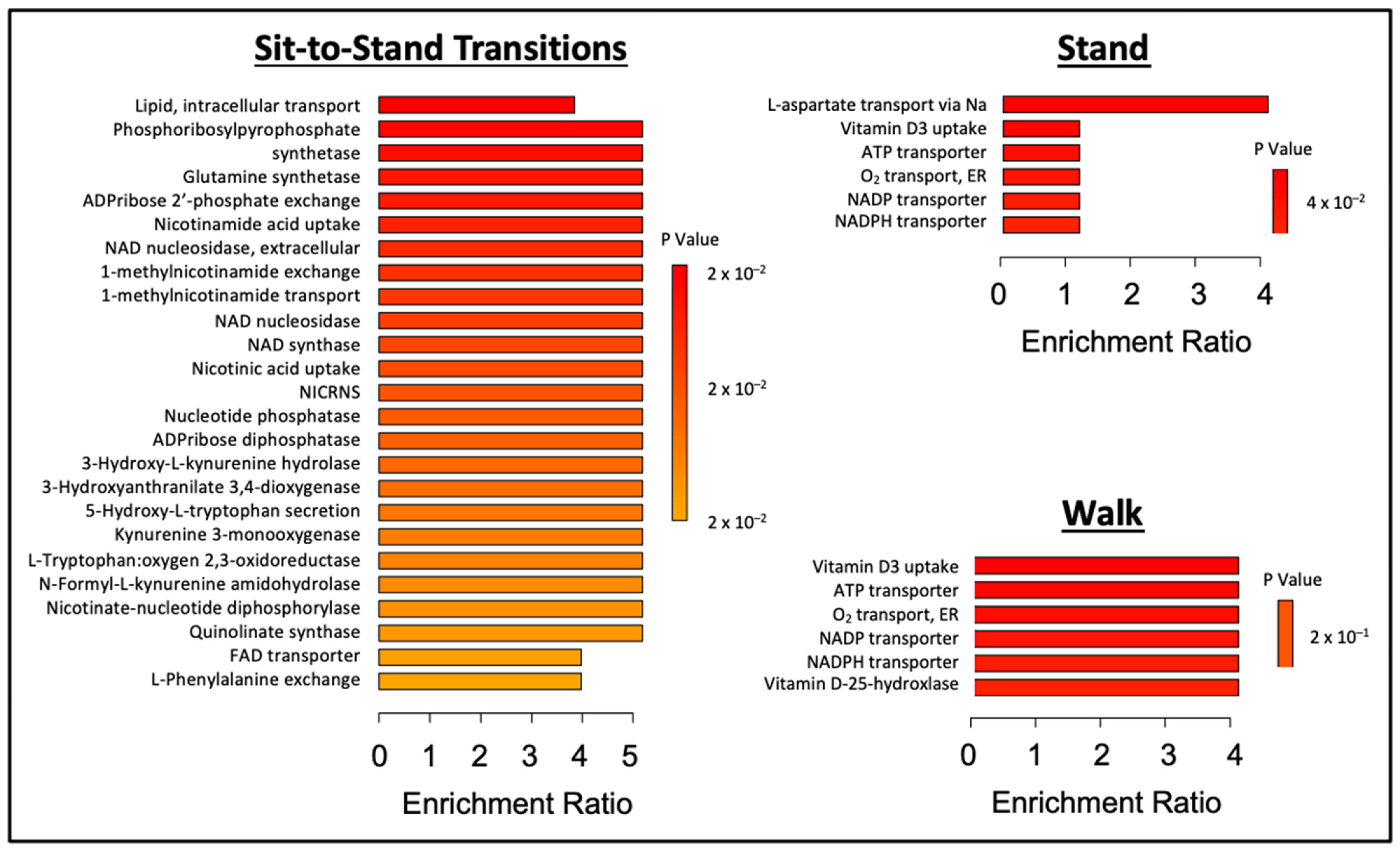
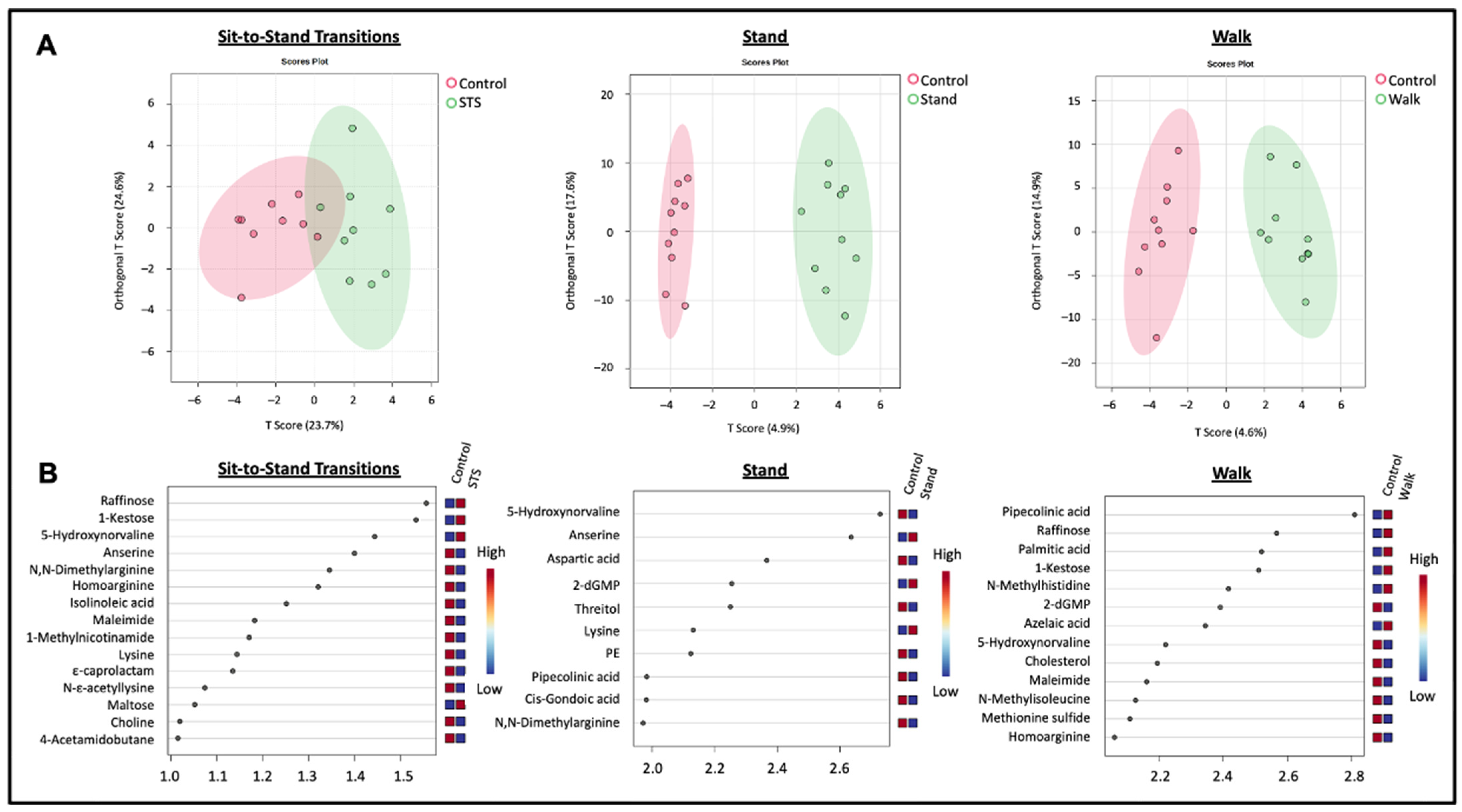
3.2. Postprandial Metabolome Alterations during Experimental Sitting Conditions
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mayo Clinic Health System. Learn More about Menopause. Available online: https://www.mayoclinichealthsystem.org/hometown-health/speaking-of-health/too-embarrassed-to-ask-part-3 (accessed on 20 March 2024).
- De Rezende, L.F.M.; Rey-López, J.P.; Matsudo, V.K.R.; Luiz, O.D.C. Sedentary behavior and health outcomes among older adults: A systematic review. BMC Public Health 2014, 14, 333. [Google Scholar] [CrossRef]
- Henson, J.; Davies, M.J.; Bodicoat, D.H.; Edwardson, C.L.; Gill, J.M.R.; Stensel, D.J.; Tolfrey, K.; Dunstan, D.W.; Khunti, K.; Yates, T. Breaking Up Prolonged Sitting with Standing or Walking Attenuates the Postprandial Metabolic Response in Postmenopausal Women: A Randomized Acute Study. Diabetes Care 2016, 39, 130–138. [Google Scholar] [CrossRef] [PubMed]
- Ekelund, U.; Brown, W.J.; Steene-Johannessen, J.; Fagerland, M.W.; Owen, N.; Powell, K.E.; Bauman, A.E.; Lee, I.M. Do the associations of sedentary behaviour with cardiovascular disease mortality and cancer mortality differ by physical activity level? A systematic review and harmonised meta-analysis of data from 850,060 participants. Br. J. Sports Med. 2019, 53, 886–894. [Google Scholar] [CrossRef] [PubMed]
- Patterson, R.; McNamara, E.; Tainio, M.; de Sá, T.H.; Smith, A.D.; Sharp, S.J.; Edwards, P.; Woodcock, J.; Brage, S. Wijndaele. Sedentary behaviour and risk of all-cause, cardiovascular and cancer mortality, and incident type 2 diabetes: A systematic review and dose response meta-analysis. Eur. J. Epidemiol. 2018, 33, 811–829. [Google Scholar] [CrossRef] [PubMed]
- Lee, I.M.; Shiroma, E.J.; Lobelo, F.; Puska, P.; Blair, S.N.; Katzmarzyk, P.T.; Alkandari, J.R.; Andersen, L.B.; Bauman, A.E.; Brownson, R.C.; et al. Impact of Physical Inactivity on the World’s Major Non-Communicable Diseases. Lancet. 2012, 380, 219. [Google Scholar] [CrossRef]
- Booth, F.W.; Roberts, C.K.; Laye, M.J. Lack of exercise is a major cause of chronic diseases. Compr. Physiol. 2012, 2, 1143. [Google Scholar] [CrossRef]
- Health Policy Data Requests—Percent of, U.S. Adults 55 and Over with Chronic Conditions. Available online: https://www.cdc.gov/nchs/health_policy/adult_chronic_conditions.htm (accessed on 13 February 2022).
- Wang, Q.; Ferreira, D.L.S.; Nelson, S.M.; Sattar, N.; Ala-Korpela, M.; Lawlor, D.A. Metabolic characterization of menopause: Cross-sectional and longitudinal evidence. BMC Med. 2018, 16, 17. [Google Scholar] [CrossRef]
- Kapoor, E.; Collazo-Clavell, M.L.; Faubion, S.S. Weight Gain in Women at Midlife: A Concise Review of the Pathophysiology and Strategies for Management. Mayo Clin. Proc. 2017, 92, 1552–1558. [Google Scholar] [CrossRef]
- Ko, S.-H.; Jung, Y. Energy Metabolism Changes and Dysregulated Lipid Metabolism in Postmenopausal Women. Nutrients 2021, 13, 4556. [Google Scholar] [CrossRef]
- Paterson, C.; Fryer, S.; Zieff, G.; Stone, K.; Credeur, D.P.; Gibbs, B.B.; Padilla, J.; Parker, J.K.; Stoner, L. The Effects of Acute Exposure to Prolonged Sitting, With and Without Interruption, on Vascular Function among Adults: A Meta-analysis. Sport. Med. 2020, 50, 1929–1942. [Google Scholar] [CrossRef]
- Pekas, E.J.; Allen, M.F.; Park, S.Y. Prolonged sitting and peripheral vascular function: Potential mechanisms and methodological considerations. J. Appl. Physiol. 2023, 134, 810–822. [Google Scholar] [CrossRef]
- Ekelund, U.; Steene-Johannessen, J.; Brown, W.J.; Fagerland, M.W.; Owen, N.; Powell, K.E.; Bauman, A.; Lee, I.M.; Ding, D.; Heath, G.; et al. Does physical activity attenuate, or even eliminate, the detrimental association of sitting time with mortality? A harmonised meta-analysis of data from more than 1 million men and women. Lancet 2016, 388, 1302–1310. [Google Scholar] [CrossRef]
- Thosar, S.S.; Bielko, S.L.; Mather, K.J.; Johnston, J.D.; Wallace, J.P. Effect of prolonged sitting and breaks in sitting time on endothelial function. Med. Sci. Sports Exerc. 2015, 47, 843–849. [Google Scholar] [CrossRef]
- Li, Y.S.J.; Haga, J.H.; Chien, S. Molecular basis of the effects of shear stress on vascular endothelial cells. J. Biomech. 2005, 38, 1949–1971. [Google Scholar] [CrossRef] [PubMed]
- Kerr, J.; Crist, K.; Vital, D.G.; Dillon, L.; Aden, S.A.; Trivedi, M.; Castellanos, L.R.; Godbole, S.; Li, H.; Allison, M.A.; et al. Acute glucoregulatory and vascular outcomes of three strategies for interrupting prolonged sitting time in postmenopausal women: A pilot, laboratory-based, randomized, controlled, 4-condition, 4-period crossover trial. PLoS ONE 2017, 12, e0188544. [Google Scholar] [CrossRef] [PubMed]
- Matthews, C.E.; Chen, K.Y.; Freedson, P.S.; Buchowski, M.S.; Beech, B.M.; Pate, R.R.; Troiano, R.P. Amount of Time Spent in Sedentary Behaviors in the United States, 2003–2004. Am. J. Epidemiol. 2008, 167, 875. [Google Scholar] [CrossRef]
- Saunders, T.J.; Larouche, R.; Colley, R.C.; Tremblay, M.S. Acute Sedentary Behaviour and Markers of Cardiometabolic Risk: A Systematic Review of Intervention Studies. J. Nutr. Metab. 2012, 2012, 712435. [Google Scholar] [CrossRef] [PubMed]
- Menni, C.; Zhai, G.; Macgregor, A.; Prehn, C.; Römisch-Margl, W.; Suhre, K.; Adamski, J.; Cassidy, A.; Illig, T.; Spector, T.D.; et al. Targeted metabolomics profiles are strongly correlated with nutritional patterns in women. Metabolomics 2013, 9, 506–514. [Google Scholar] [CrossRef] [PubMed]
- Barton, S.; Navarro, S.L.; Buas, M.F.; Schwarz, Y.; Gu, H.; Djukovic, D.; Raftery, D.; Kratz, M.; Neuhouser, M.L.; Lampe, J.W. Targeted plasma metabolome response to variations in dietary glycemic load in a randomized, controlled, crossover feeding trial in healthy adults. Food Funct. 2015, 6, 2949–2956. [Google Scholar] [CrossRef]
- Gu, H.; Zhang, P.; Zhu, J.; Raftery, D. Globally Optimized Targeted Mass Spectrometry: Reliable Metabolomics Analysis with Broad Coverage. Anal. Chem. 2015, 87, 12355–12362. [Google Scholar] [CrossRef]
- Shi, X.; Wang, S.; Jasbi, P.; Turner, C.; Hrovat, J.; Wei, Y.; Liu, J.; Gu, H. Database Assisted Globally Optimized Targeted Mass Spectrometry (dGOT-MS): Broad and Reliable Metabolomics Analysis with Enhanced Identification. Anal. Chem. 2019, 91, 13737–13745. [Google Scholar] [CrossRef]
- Mamas, M.; Dunn, W.B.; Neyses, L.; Goodacre, R. The role of metabolites and metabolomics in clinically applicable biomarkers of disease. Arch. Toxicol. 2011, 85, 5–17. [Google Scholar] [CrossRef]
- Zhao, H.; Shen, J.; Djukovic, D.; Daniel-MacDougall, C.; Gu, H.; Wu, X.; Chow, W.-H. Metabolomics-identified metabolites associated with body mass index and prospective weight gain among Mexican American women. Obes. Sci. Pract. 2016, 2, 309–317. [Google Scholar] [CrossRef] [PubMed]
- Jasbi, P.; Baker, O.; Shi, X.; Gonzalez, L.A.; Wang, S.; Anderson, S.; Xi, B.; Gu, H.; Johnston, C.S. Daily red wine vinegar ingestion for eight weeks improves glucose homeostasis and affects the metabolome but does not reduce adiposity in adults. Food Funct. 2019, 10, 7343–7355. [Google Scholar] [CrossRef] [PubMed]
- Patterson, J.; Shi, X.; Bresette, W.; Eghlimi, R.; Atlas, S.; Farr, K.; Vega-López, S.; Gu, H. A Metabolomic Analysis of the Sex-Dependent Hispanic Paradox. Metabolites 2021, 11, 552. [Google Scholar] [CrossRef] [PubMed]
- Thalacker-Mercer, A.E.; Ingram, K.H.; Guo, F.; Ilkayeva, O.; Newgard, C.B.; Garvey, W.T. BMI, diabetes, and sex affect the relationships between amino acids and clamp measures of insulin action in humans. Diabetes 2014, 63, 791–800. [Google Scholar] [CrossRef]
- Shah, S.H.; Newgard, C.B. Integrated Metabolomics and Genomics: Systems Approaches to Biomarkers and Mechanisms of Cardiovascular Disease. Circ. Cardiovasc. Genet. 2015, 8, 410. [Google Scholar] [CrossRef]
- Kurland, I.J.; Accili, D.; Burant, C.; Fischer, S.M.; Kahn, B.B.; Newgard, C.B.; Ramagiri, S.; Ronnett, G.V.; Ryals, J.A.; Sanders, M.; et al. Application of combined omics platforms to accelerate biomedical discovery in diabesity. Ann. N. Y. Acad. Sci. 2013, 1287, 1–16. [Google Scholar] [CrossRef]
- Wang, T.J.; Larson, M.G.; Vasan, R.S.; Cheng, S.; Rhee, E.P.; McCabe, E.; Lewis, G.D.; Fox, C.S.; Jacques, P.F.; Fernandez, C.; et al. Metabolite profiles and the risk of developing diabetes. Nat. Med. 2011, 17, 448–453. [Google Scholar] [CrossRef]
- Wang, T.J.; Ngo, D.; Psychogios, N.; Dejam, A.; Larson, M.G.; Vasan, R.S.; Ghorbani, A.; O’Sullivan, J.; Cheng, S.; Rhee, E.P.; et al. 2-Aminoadipic acid is a biomarker for diabetes risk. J. Clin. Investig. 2013, 123, 4309–4317. [Google Scholar] [CrossRef]
- Würtz, P.; Havulinna, A.S.; Soininen, P.; Tynkkynen, T.; Prieto-Merino, D.; Tillin, T.; Ghorbani, A.; Artati, A.; Wang, Q.; Tiainen, M.; et al. Metabolite profiling and cardiovascular event risk: A prospective study of 3 population-based cohorts. Circulation 2015, 131, 774–785. [Google Scholar] [CrossRef] [PubMed]
- Roberts, L.D.; Gerszten, R.E. Toward new biomarkers of cardiometabolic diseases. Cell Metab. 2013, 18, 43–50. [Google Scholar] [CrossRef]
- Magnusson, M.; Wang, T.J.; Clish, C.; Engström, G.; Nilsson, P.; Gerszten, R.E.; Melander, O. Dimethylglycine Deficiency and the Development of Diabetes. Diabetes 2015, 64, 3010–3016. [Google Scholar] [CrossRef] [PubMed]
- Bakar, M.H.A.; Sarmidi, M.R.; Cheng, K.-K.; Khan, A.A.; Suan, C.L.; Huri, H.Z.; Yaakob, H. Metabolomics—The complementary field in systems biology: A review on obesity and type 2 diabetes. Mol. Biosyst. 2015, 11, 1742–1774. [Google Scholar] [CrossRef]
- Jasbi, P.; Wang, D.; Cheng, S.L.; Fei, Q.; Cui, J.Y.; Liu, L.; Wei, Y.; Raftery, D.; Gu, H. Breast cancer detection using targeted plasma metabolomics. J. Chromatogr. B Anal. Technol. Biomed. Life Sci. 2019, 1105, 26–37. [Google Scholar] [CrossRef] [PubMed]
- Parent, B.A.; Seaton, M.; Djukovic, D.; Gu, H.; Wheelock, B.; Navarro, S.L.; Raftery, D.; O’Keefe, G.E. Parenteral and enteral nutrition in surgical critical care: Plasma metabolomics demonstrates divergent effects on nitrogen, fatty-acid, ribonucleotide, and oxidative metabolism. J. Trauma Acute Care Surg. 2017, 82, 704–713. [Google Scholar] [CrossRef]
- Newgard, C.B. Metabolomics and Metabolic Diseases: Where Do We Stand? Cell Metab. 2017, 25, 43–56. [Google Scholar] [CrossRef]
- Jasbi, P.; Nikolich-Žugich, J.; Patterson, J.; Knox, K.S.; Jin, Y.; Weinstock, G.M.; Smith, P.; Twigg, H.L.; Gu, H. Targeted metabolomics reveals plasma biomarkers and metabolic alterations of the aging process in healthy young and older adults. GeroScience 2023, 45, 3131–3146. [Google Scholar] [CrossRef]
- Remie, C.M.E.; Janssens, G.E.; Bilet, L.; van Weeghel, M.; Duvivier, B.M.F.M.; de Wit, V.H.W.; Connell, N.J.; Jörgensen, J.A.; Schomakers, B.V.; Schrauwen-Hinderling, V.B.; et al. Sitting less elicits metabolic responses similar to exercise and enhances insulin sensitivity in postmenopausal women. Diabetologia 2021, 64, 2817–2828. [Google Scholar] [CrossRef]
- Pinto, A.J.; Meireles, K.; Peçanha, T.; Mazzolani, B.C.; Smaira, F.I.; Rezende, D.; Benatti, F.B.; Ribeiro, A.C.M.; Pinto, A.L.S.; Lima, F.R.; et al. Acute cardiometabolic effects of brief active breaks in sitting for patients with rheumatoid arthritis. Am. J. Physiol.—Endocrinol. Metab. 2021, 321, E782–E794. [Google Scholar] [CrossRef]
- Skogerson, K.; Wohlgemuth, G.; Barupal, D.K.; Fiehn, O. The volatile compound BinBase mass spectral database. BMC Bioinformatics. 2011, 12, 321. [Google Scholar] [CrossRef]
- Johnsen, L.G.; Skou, P.B.; Khakimov, B.; Bro, R. Gas chromatography—Mass spectrometry data processing made easy. J. Chromatogr. A 2017, 1503, 57–64. [Google Scholar] [CrossRef]
- Chong, J.; Soufan, O.; Li, C.; Caraus, I.; Li, S.; Bourque, G.; Wishart, D.S.; Xia, J. MetaboAnalyst 4.0: Towards more transparent and integrative metabolomics analysis. Nucleic Acids Res. 2018, 46, W486–W494. [Google Scholar] [CrossRef] [PubMed]
- Fukai, K.; Harada, S.; Iida, M.; Kurihara, A.; Takeuchi, A.; Kuwabara, K.; Sugiyama, D.; Okamura, T.; Akiyama, M.; Nishiwaki, Y.; et al. Metabolic Profiling of Total Physical Activity and Sedentary Behavior in Community-Dwelling Men. PLoS ONE 2016, 11, e0164877. [Google Scholar] [CrossRef]
- Takahashi, S.; Nakashima, Y.; Toda, K.I. Carnosine facilitates nitric oxide production in endothelial f-2 cells. Biol. Pharm. Bull. 2009, 32, 1836–1839. [Google Scholar] [CrossRef]
- Matthews, J.J.; Dolan, E.; Swinton, P.A.; Santos, L.; Artioli, G.G.; Turner, M.D.; Elliott-Sale, K.J.; Sale, C. Effect of Carnosine or β-Alanine Supplementation on Markers of Glycemic Control and Insulin Resistance in Humans and Animals: A Systematic Review and Meta-analysis. Adv. Nutr. 2021, 12, 2216–2231. [Google Scholar] [CrossRef] [PubMed]
- de Jager, S.; Blancquaert, L.; Van der Stede, T.; Lievens, E.; De Baere, S.; Croubels, S.; Gilardoni, E.; Regazzoni, L.G.; Aldini, G.; Bourgois, J.G.; et al. The ergogenic effect of acute carnosine and anserine supplementation: Dosing, timing, and underlying mechanism. J. Int. Soc. Sports Nutr. 2022, 19, 70–91. [Google Scholar] [CrossRef] [PubMed]
- Ririe, D.G.; Roberts, P.R.; Shouse, M.N.; Zaloga, G.P. Vasodilatory actions of the dietary peptide carnosine. Nutrition 2000, 16, 168–172. [Google Scholar] [CrossRef] [PubMed]
- Matthews, J.J.; Turner, M.D.; Santos, L.; Elliott-Sale, K.J.; Sale, C. Carnosine increases insulin-stimulated glucose uptake and reduces methylglyoxal-modified proteins in type-2 diabetic human skeletal muscle cells. Amino Acids 2023, 55, 413–420. [Google Scholar] [CrossRef]
- Holeček, M. Aspartic Acid in Health and Disease. Nutrients 2023, 15, 4023. [Google Scholar] [CrossRef]
- Nieman, D.C.; Scherr, J.; Luo, B.; Meaney, M.P.; Dréau, D.; Sha, W.; Dew, D.A.; Henson, D.A.; Pappan, K.L. Influence of pistachios on performance and exercise-induced inflammation, oxidative stress, immune dysfunction, and metabolite shifts in cyclists: A randomized, crossover trial. PLoS ONE 2014, 9, e113725. [Google Scholar] [CrossRef]
- Mach, N.; Fuster-Botella, D. Endurance exercise and gut microbiota: A review. J. Sport Heal. Sci. 2017, 6, 179. [Google Scholar] [CrossRef]
- Gilinsky, M.A.; Polityko, Y.K.; Markel, A.L.; Latysheva, T.V.; Samson, A.O.; Polis, B.; Naumenko, S.E. Norvaline Reduces Blood Pressure and Induces Diuresis in Rats with Inherited Stress-Induced Arterial Hypertension. Biomed. Res. Int. 2020, 2020, 4935386. [Google Scholar] [CrossRef]
- Javrushyan, H.; Nadiryan, E.; Grigoryan, A.; Avtandilyan, N.; Maloyan, A. Antihyperglycemic activity of L-norvaline and L-arginine in high-fat diet and streptozotocin-treated male rats. Exp. Mol. Pathol. 2022, 126, 104763. [Google Scholar] [CrossRef]
- Zhang, S.W.; Xu, J.Y.; Zhang, T. DGMP: Identifying Cancer Driver Genes by Jointing DGCN and MLP from Multi-omics Genomic Data. Genom. Proteom. Bioinform. 2022, 20, 928. [Google Scholar] [CrossRef]
- Leandro, J.; Houten, S.M. The lysine degradation pathway: Subcellular compartmentalization and enzyme deficiencies. Mol. Genet. Metab. 2020, 131, 14–22. [Google Scholar] [CrossRef]
- Thach, T.T.; Wu, C.; Hwang, K.Y.; Lee, S.J. Azelaic Acid Induces Mitochondrial Biogenesis in Skeletal Muscle by Activation of Olfactory Receptor 544. Front. Physiol. 2020, 11, 514842. [Google Scholar] [CrossRef]
- Wang, X.; Zhu, L.; Liu, J.; Ma, Y.; Qiu, C.; Liu, C.; Gong, Y.; Yuwen, Y.; Guan, G.; Zhang, Y.; et al. Palmitic acid in type 2 diabetes mellitus promotes atherosclerotic plaque vulnerability via macrophage Dll4 signaling. Nat. Commun. 2024, 15, 1281. [Google Scholar] [CrossRef]
- Elango, D.; Rajendran, K.; Van der Laan, L.; Sebastiar, S.; Raigne, J.; Thaiparambil, N.A.; El Haddad, N.; Raja, B.; Wang, W.; Ferela, A.; et al. Raffinose Family Oligosaccharides: Friend or Foe for Human and Plant Health? Front. Plant Sci. 2022, 13, 829118. [Google Scholar] [CrossRef] [PubMed]
- Tochio, T.; Kadota, Y.; Tanaka, T.; Koga, Y. the Smallest Fructooligosaccharide Component, Which Efficiently Stimulates Faecalibacterium prausnitzii as Well as Bifidobacteria in Humans. Foods 2018, 7, 140. [Google Scholar] [CrossRef]
- Chang, Y.J.; Bellettiere, J.; Godbole, S.; Keshavarz, S.; Maestas, J.P.; Unkart, J.T.; Ervin, D.; Allison, M.A.; Rock, C.L.; Patterson, R.E.; et al. Total Sitting Time and Sitting Pattern in Postmenopausal Women Differ by Hispanic Ethnicity and are Associated With Cardiometabolic Risk Biomarkers. J. Am. Hear. Assoc. Cardiovasc. Cerebrovasc. Dis. 2020, 9, e013403. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Measurement | |
|---|---|
| N | 10 |
| Age (y) | 66 ± 9.0 |
| BMI (kg/m2) | 30.6 ± 4.2 |
| Body mass (kg) | 79.4 ± 12.3 |
| Height (cm) | 161 ± 5.9 |
| Waist circumference (cm) | 95.9 ± 11.8 |
| Hip circumference (cm) | 104.5 ± 15.2 |
| Waist/hip ratio | 0.92 ± 0.07 |
| HbA1c (%) | 5.7 ± 0.5 |
| HbA1c (mmol/mol) | 39 ± 6.0 |
| Fasting plasma glucose (mg/dL) | 107.2 ± 17.4 |
| Fasting plasma insulin (uIU/mL) | 9.3 ± 4.8 |
| HOMA-IR | 2.5 ± 1.5 |
| Systolic BP (mmHg) | 123 ± 8.0 |
| Diastolic BP (mmHg) | 66 ± 7.0 |
| Heart rate (bpm) | 65 ± 8.0 |
| Race | Count |
| White | 9 |
| Asian | 1 |
| Ethnicity | |
| Hispanic | 2 |
| Non-Hispanic | 8 |
| Medications | |
| β-blockers | 1 |
| β-3 adrenergic agonists | 1 |
| Calcium channel blockers | 1 |
| Loop diuretics | 1 |
| Metformin | 2 |
| Statins | 2 |
| Metabolite | Fold Change | p-Value |
|---|---|---|
| Palmitoleic acid | 0.14 | <0.001 |
| Palmitic acid | 0.64 | <0.001 |
| Oleic acid | 0.17 | <0.001 |
| Myristic acid | 0.35 | <0.001 |
| Linolenic acid | 0.41 | <0.001 |
| Linoleic acid | 0.34 | <0.001 |
| Heptadecanoic acid | 0.55 | <0.001 |
| Arachidonic acid | 0.63 | <0.001 |
| Glycerol | 0.67 | <0.001 |
| Metabolites | Control v. | ||
|---|---|---|---|
| Sit-to-Stand | Stand | Walk | |
| Amino Acid Metabolism | |||
| Anserine | 0.048 (1.27, 0.72) | ||
| Aspartic acid | 0.047 (1.72, 1.87) | ||
| 5-Hydroxynorvaline | 0.048 (0.71, 0.94) | 0.011 (0.71, 1.72) | |
| γ-Glutamylmethionine | 0.020 (1.43, 0.97) | ||
| Glutamine | 0.042 (1.13, 0.97) | ||
| Homoarginine | 0.030 (1.57, 0.95) | ||
| Lysine | 0.033 (1.62, 1.10) | ||
| N-N-Dimethylarginine | 0.044 (1.30, 0.88) | ||
| N-ε-Acetyllysine | 0.026 (1.65, 1.14) | ||
| Pipecolinic Acid | 0.016 (0.69, 1.09) | ||
| Fat Metabolism | |||
| Cholesterol | 0.047 (0.89, 0.98) | ||
| Palmitic Acid | 0.028 (0.64, 0.50) | ||
| Sugar Metabolism | |||
| Threitol | 0.020 (0.99, 1.19) | ||
| Other Organic Compounds | |||
| Azelaic Acid | 0.043 (0.72, 0.58) | ||
| ε-Caprolactam | 0.018 (1.60, 0.83) | ||
| 2-dGMP | 0.028 (1.49, 0.72) | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Patterson, J.S.; Rana, B.K.; Gu, H.; Sears, D.D. Sitting Interruption Modalities during Prolonged Sitting Acutely Improve Postprandial Metabolome in a Crossover Pilot Trial among Postmenopausal Women. Metabolites 2024, 14, 478. https://doi.org/10.3390/metabo14090478
Patterson JS, Rana BK, Gu H, Sears DD. Sitting Interruption Modalities during Prolonged Sitting Acutely Improve Postprandial Metabolome in a Crossover Pilot Trial among Postmenopausal Women. Metabolites. 2024; 14(9):478. https://doi.org/10.3390/metabo14090478
Chicago/Turabian StylePatterson, Jeffrey S., Brinda K. Rana, Haiwei Gu, and Dorothy D. Sears. 2024. "Sitting Interruption Modalities during Prolonged Sitting Acutely Improve Postprandial Metabolome in a Crossover Pilot Trial among Postmenopausal Women" Metabolites 14, no. 9: 478. https://doi.org/10.3390/metabo14090478