
Is Lymphedema a Systemic Disease? A Paired Molecular and Histological Analysis of the Affected and Unaffected Tissue in Lymphedema Patients


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Tissue Collection and Histology
2.3. Immunohistochemistry
2.4. RNA Extraction and Quantitative Polymerase Chain Reactions
2.5. Statistics
3. Results
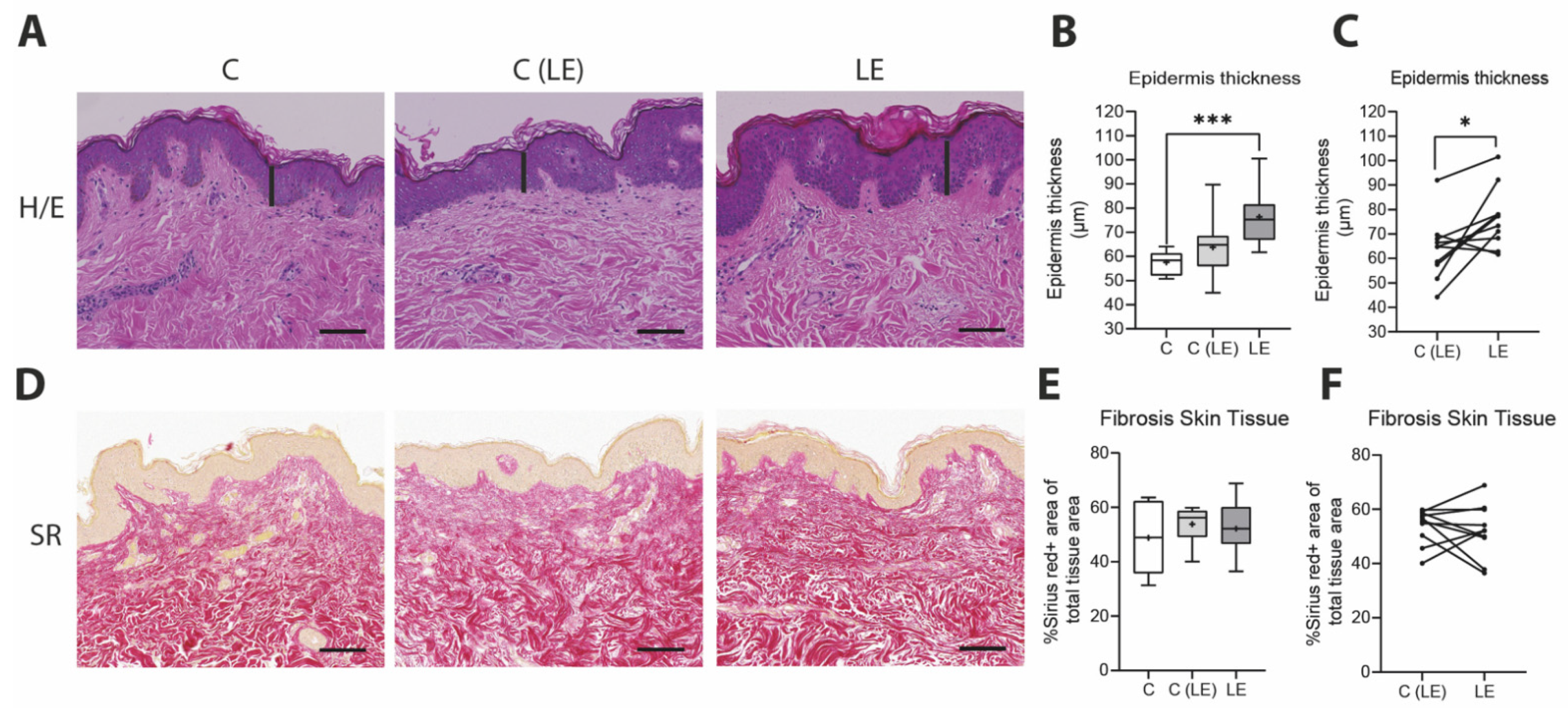
3.1. Increased Epidermis Thickness in Lymphedema Patients
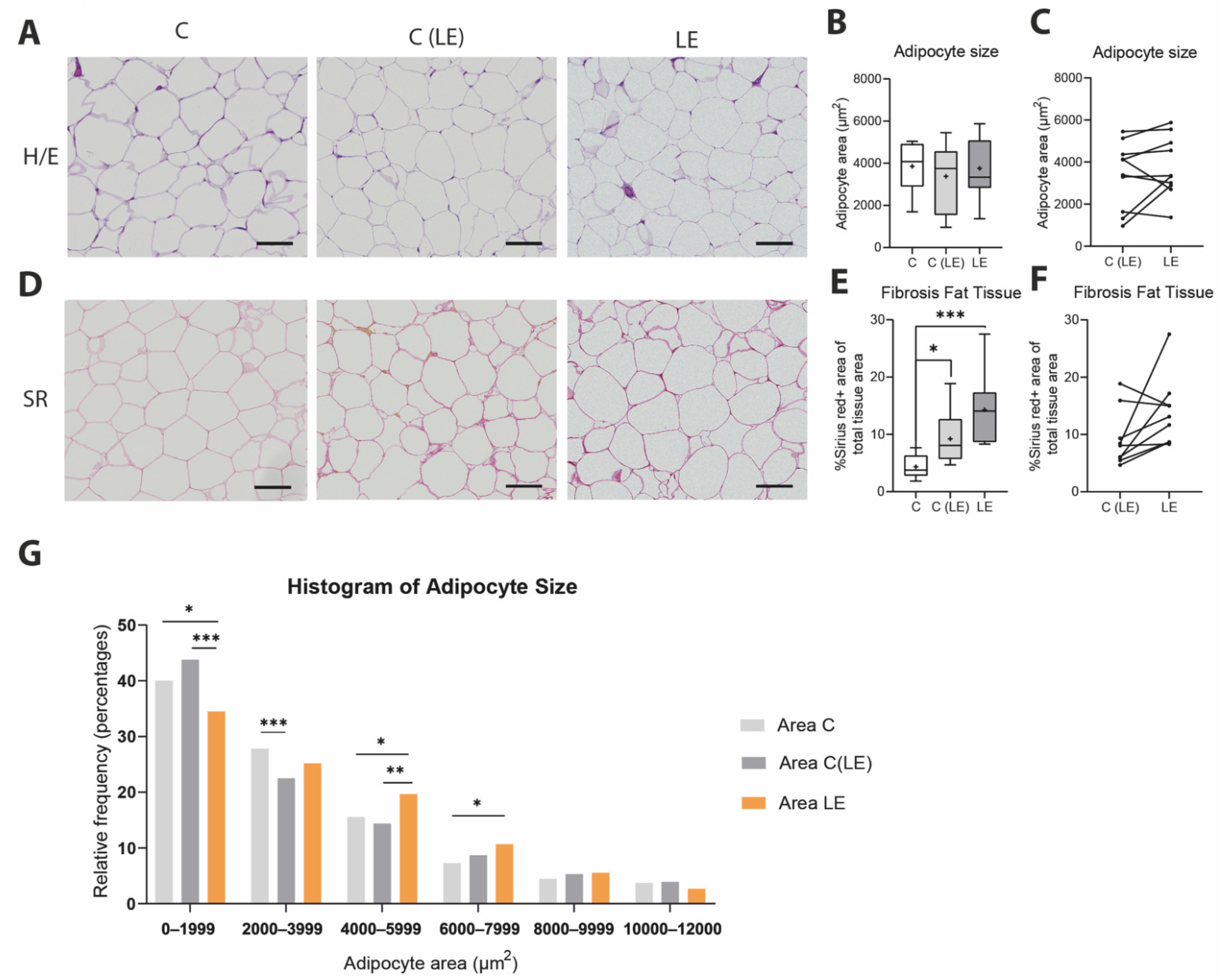
3.2. Increased Fibroadipose Tissue in Lymphedema Patients
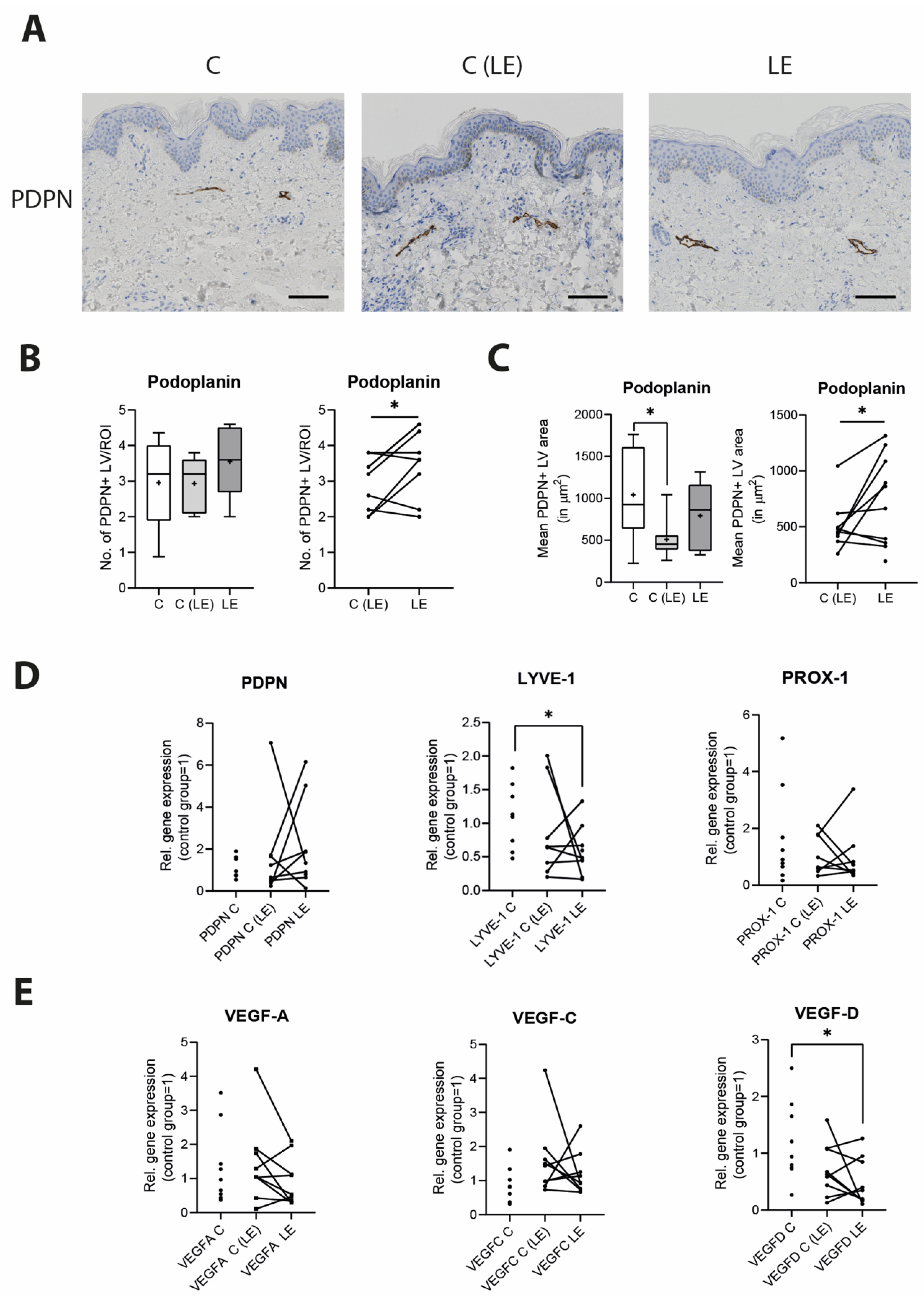
3.3. Morphological Changes in the Lymphatic Vasculature in Lymphedema
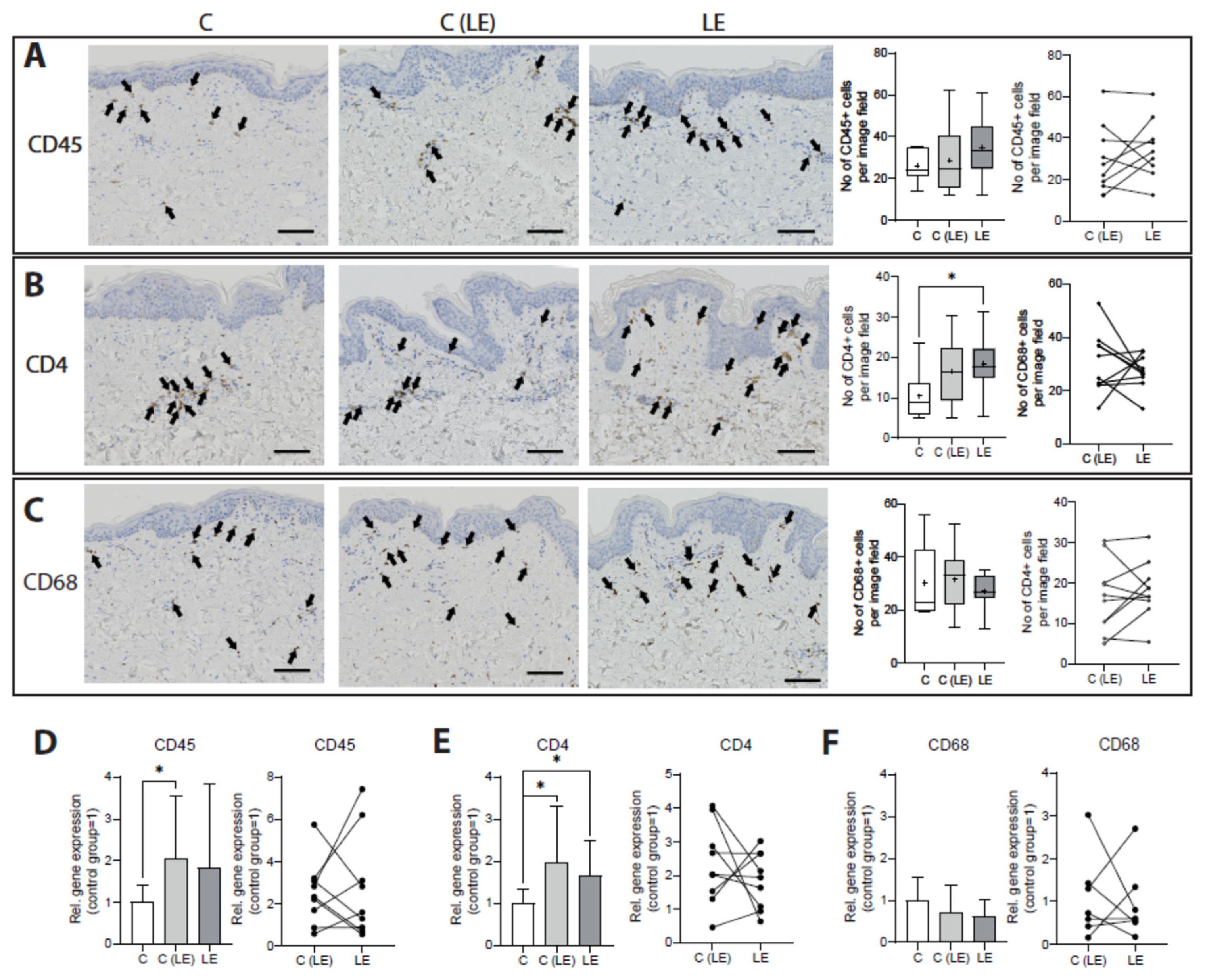
3.4. Systemic Increase in CD4+ T Cells in Lymphedema
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Petrek, J.A.; Senie, R.T.; Peters, M.; Rosen, P.P. Lymphedema in a cohort of breast carcinoma survivors 20 years after diagnosis. Cancer 2001, 92, 1368–1377. [Google Scholar] [CrossRef]
- Arie, A.; Yamamoto, T. Lymphedema secondary to melanoma treatments: Diagnosis, evaluation, and treatments. Glob. Health Med. 2020, 2, 227–234. [Google Scholar] [CrossRef] [PubMed]
- Friedmann, D.; Wunder, J.S.; Ferguson, P.; O’Sullivan, B.; Roberge, D.; Catton, C.; Freeman, C.; Saran, N.; Turcotte, R.E. Incidence and Severity of Lymphoedema following Limb Salvage of Extremity Soft Tissue Sarcoma. Sarcoma 2011, 2011, 289673. [Google Scholar] [CrossRef] [Green Version]
- Dessources, K.; Aviki, E.; Leitao, M.M., Jr. Lower extremity lymphedema in patients with gynecologic malignancies. Int. J. Gynecol. Cancer 2020, 30, 252–260. [Google Scholar] [CrossRef] [PubMed]
- Okeke, A.A.; Bates, D.O.; Gillatt, D.A. Lymphoedema in urological cancer. Eur. Urol. 2004, 45, 18–25. [Google Scholar] [CrossRef] [PubMed]
- International Society of Lymphology. The diagnosis and treatment of peripheral lymphedema: 2013 Consensus Document of the International Society of Lymphology. Lymphology 2013, 46, 1–11. [Google Scholar]
- Li, C.Y.; Kataru, R.P.; Mehrara, B.J. Histopathologic Features of Lymphedema: A Molecular Review. Int. J. Mol. Sci. 2020, 21, 2546. [Google Scholar] [CrossRef] [Green Version]
- Zampell, J.C.; Yan, A.; Elhadad, S.; Avraham, T.; Weitman, E.; Mehrara, B.J. CD4(+) cells regulate fibrosis and lymphangiogenesis in response to lymphatic fluid stasis. PLoS ONE 2012, 7, e49940. [Google Scholar] [CrossRef] [Green Version]
- Avraham, T.; Zampell, J.C.; Yan, A.; Elhadad, S.; Weitman, E.S.; Rockson, S.G.; Bromberg, J.; Mehrara, B.J. Th2 differentiation is necessary for soft tissue fibrosis and lymphatic dysfunction resulting from lymphedema. FASEB J. 2013, 27, 1114–1126. [Google Scholar] [CrossRef] [Green Version]
- Mehrara, B.J.; Park, H.J.; Kataru, R.P.; Bromberg, J.; Coriddi, M.; Baik, J.E.; Shin, J.; Li, C.; Cavalli, M.R.; Encarnacion, E.M.; et al. Pilot Study of Anti-Th2 Immunotherapy for the Treatment of Breast Cancer-Related Upper Extremity Lymphedema. Biology 2021, 10, 934. [Google Scholar] [CrossRef]
- Gousopoulos, E.; Proulx, S.T.; Bachman, S.B.; Scholl, J.; Dionyssiou, D.; Demiri, E.; Halin, C.; Dieterich, L.C.; Detmar, M. Regulatory T-cell transfer ameliorates lymphedema and promotes lymphatic vessel function. JCI Insight 2016, 1, e89081. [Google Scholar] [CrossRef]
- Gardenier, J.C.; Kataru, R.P.; Hespe, G.E.; Savetsky, I.L.; Torrisi, J.S.; Nores, G.D.; Jowhar, D.K.; Nitti, M.D.; Schofield, R.C.; Carlow, D.C.; et al. Topical tacrolimus for the treatment of secondary lymphedema. Nat. Commun. 2017, 8, 14345. [Google Scholar] [CrossRef]
- Stanton, A.W.; Modi, S.; Bennett Britton, T.M.; Purushotham, A.D.; Peters, A.M.; Levick, J.R.; Mortimer, P.S. Lymphatic drainage in the muscle and subcutis of the arm after breast cancer treatment. Breast Cancer Res. Treat. 2009, 117, 549–557. [Google Scholar] [CrossRef] [PubMed]
- Bains, S.K.; Peters, A.M.; Zammit, C.; Ryan, N.; Ballinger, J.; Glass, D.M.; Allen, S.; Stanton, A.W.B.; Mortimer, P.S.; Purushotham, A.D. Global abnormalities in lymphatic function following systemic therapy in patients with breast cancer. Br. J. Surg. 2015, 102, 534–540. [Google Scholar] [CrossRef] [PubMed]
- Cintolesi, V.; Stanton, A.W.; Bains, S.K.; Cousins, E.; Peters, A.M.; Purushotham, A.D.; Levick, J.R.; Mortimer, P.S. Constitutively Enhanced Lymphatic Pumping in the Upper Limbs of Women Who Later Develop Breast Cancer-Related Lymphedema. Lymphat. Res. Biol. 2016, 14, 50–61. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Felmerer, G.; Stylianaki, A.; Hagerling, R.; Wang, A.; Strobel, P.; Hollmen, M.; Lindenblatt, N.; Gousopoulos, E. Adipose Tissue Hypertrophy, An Aberrant Biochemical Profile and Distinct Gene Expression in Lipedema. J. Surg. Res. 2020, 253, 294–303. [Google Scholar] [CrossRef] [PubMed]
- Mellor, R.H.; Bush, N.L.; Stanton, A.W.; Bamber, J.C.; Levick, J.R.; Mortimer, P.S. Dual-frequency ultrasound examination of skin and subcutis thickness in breast cancer-related lymphedema. Breast J. 2004, 10, 496–503. [Google Scholar] [CrossRef] [PubMed]
- Brorson, H.; Ohlin, K.; Olsson, G.; Karlsson, M.K. Breast cancer-related chronic arm lymphedema is associated with excess adipose and muscle tissue. Lymphat. Res. Biol. 2009, 7, 3–10. [Google Scholar] [CrossRef]
- Zhang, J.; Hoffner, M.; Brorson, H. Adipocytes are larger in lymphedematous extremities than in controls. J. Plast. Surg. Hand Surg. 2021, 56, 172–179. [Google Scholar] [CrossRef]
- Zampell, J.C.; Aschen, S.; Weitman, E.S.; Yan, A.; Elhadad, S.; De Brot Andrade, M.; Mehrara, B.J. Regulation of adipogenesis by lymphatic fluid stasis: Part I. Adipogenesis, fibrosis, and inflammation. Plast. Reconstr. Surg. 2012, 129, 825–834. [Google Scholar] [CrossRef] [Green Version]
- Aschen, S.; Zampell, J.C.; Elhadad, S.; Weitman, E.; De Brot Andrade, M.; Mehrara, B.J. Regulation of adipogenesis by lymphatic fluid stasis: Part II. Expression of adipose differentiation genes. Plast. Reconstr. Surg. 2012, 129, 838–847. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stanton, A.W.; Modi, S.; Mellor, R.H.; Levick, J.R.; Mortimer, P.S. Recent advances in breast cancer-related lymphedema of the arm: Lymphatic pump failure and predisposing factors. Lymphat. Res. Biol. 2009, 7, 29–45. [Google Scholar] [CrossRef] [PubMed]
- Aldrich, M.B.; Guilliod, R.; Fife, C.E.; Maus, E.A.; Smith, L.; Rasmussen, J.C.; Sevick-Muraca, E.M. Lymphatic abnormalities in the normal contralateral arms of subjects with breast cancer-related lymphedema as assessed by near-infrared fluorescent imaging. Biomed. Opt. Express 2012, 3, 1256–1265. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jensen, M.R.; Simonsen, L.; Karlsmark, T.; Bulow, J. Microvascular filtration is increased in the forearms of patients with breast cancer-related lymphedema. J. Appl. Physiol. 2013, 114, 19–27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gousopoulos, E.; Proulx, S.T.; Bachmann, S.B.; Dieterich, L.C.; Scholl, J.; Karaman, S.; Bianchi, R.; Detmar, M. An Important Role of VEGF-C in Promoting Lymphedema Development. J. Investig. Dermatol. 2017, 137, 1995–2004. [Google Scholar] [CrossRef] [Green Version]
- Tashiro, K.; Feng, J.; Wu, S.H.; Mashiko, T.; Kanayama, K.; Narushima, M.; Uda, H.; Miyamoto, S.; Koshima, I.; Yoshimura, K. Pathological changes of adipose tissue in secondary lymphoedema. Br. J. Dermatol. 2017, 177, 158–167. [Google Scholar] [CrossRef]
- Rockson, S.G.; Tian, W.; Jiang, X.; Kuznetsova, T.; Haddad, F.; Zampell, J.; Mehrara, B.; Sampson, J.P.; Roche, L.; Kim, J.; et al. Pilot studies demonstrate the potential benefits of antiinflammatory therapy in human lymphedema. JCI Insight 2018, 3, e123775. [Google Scholar] [CrossRef]
- Mihara, M.; Hara, H.; Hayashi, Y.; Narushima, M.; Yamamoto, T.; Todokoro, T.; Iida, T.; Sawamoto, N.; Araki, J.; Kikuchi, K.; et al. Pathological steps of cancer-related lymphedema: Histological changes in the collecting lymphatic vessels after lymphadenectomy. PLoS ONE 2012, 7, e41126. [Google Scholar] [CrossRef] [Green Version]
- Jensen, M.R.; Simonsen, L.; Karlsmark, T.; Lanng, C.; Bulow, J. Higher vascular endothelial growth factor-C concentration in plasma is associated with increased forearm capillary filtration capacity in breast cancer-related lymphedema. Physiol. Rep. 2015, 3, e12403. [Google Scholar] [CrossRef] [Green Version]
- Koc, M.; Wald, M.; Varaliova, Z.; Ondrujova, B.; Cizkova, T.; Brychta, M.; Kračmerová, J.; Beranová, L.; Pala, J.; Šrámková, V.; et al. Lymphedema alters lipolytic, lipogenic, immune and angiogenic properties of adipose tissue: A hypothesis-generating study in breast cancer survivors. Sci. Rep. 2021, 11, 8171. [Google Scholar] [CrossRef]
- Lin, S.; Kim, J.; Lee, M.J.; Roche, L.; Yang, N.L.; Tsao, P.S.; Rockson, S.G. Prospective transcriptomic pathway analysis of human lymphatic vascular insufficiency: Identification and validation of a circulating biomarker panel. PLoS ONE 2012, 7, e52021. [Google Scholar] [CrossRef] [PubMed]
- Cooper, G. Early diagnosis of lymphoedema helps to reduce its psychological and social impact. Nurs. Times 2010, 106, 15–17. [Google Scholar] [PubMed]
- Gergich, N.L.S.; Pfalzer, L.A.; McGarvey, C.; Springer, B.; Gerber, L.H.; Soballe, P. Preoperative assessment enables the early diagnosis and successful treatment of lymphedema. Cancer 2008, 112, 2809–2819. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient Characteristics | Lymphedema Patients | Control Patients |
|---|---|---|
| Number of cases | 10 | 10 |
| Gender | ||
| Female | 8 | 7 |
| Male | 2 | 3 |
| Mean age (in years) | 58.10 ± 10.86 | 43.18 ± 18.77 |
| Mean BMI (in kg/m2) | 28.02 ± 5.55 | 26.54 ± 5.63 |
| Lymphedema stage | ||
| Stage I | 1 | |
| Stage II | 6 | |
| Stage III | 3 | |
| Affected extremity | ||
| Leg | 8 | |
| Arm | 2 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wolf, S.; von Atzigen, J.; Kaiser, B.; Grünherz, L.; Kim, B.-S.; Giovanoli, P.; Lindenblatt, N.; Gousopoulos, E. Is Lymphedema a Systemic Disease? A Paired Molecular and Histological Analysis of the Affected and Unaffected Tissue in Lymphedema Patients. Biomolecules 2022, 12, 1667. https://doi.org/10.3390/biom12111667
Wolf S, von Atzigen J, Kaiser B, Grünherz L, Kim B-S, Giovanoli P, Lindenblatt N, Gousopoulos E. Is Lymphedema a Systemic Disease? A Paired Molecular and Histological Analysis of the Affected and Unaffected Tissue in Lymphedema Patients. Biomolecules. 2022; 12(11):1667. https://doi.org/10.3390/biom12111667
Chicago/Turabian StyleWolf, Stefan, Julia von Atzigen, Bettina Kaiser, Lisanne Grünherz, Bong-Sung Kim, Pietro Giovanoli, Nicole Lindenblatt, and Epameinondas Gousopoulos. 2022. "Is Lymphedema a Systemic Disease? A Paired Molecular and Histological Analysis of the Affected and Unaffected Tissue in Lymphedema Patients" Biomolecules 12, no. 11: 1667. https://doi.org/10.3390/biom12111667
APA StyleWolf, S., von Atzigen, J., Kaiser, B., Grünherz, L., Kim, B.-S., Giovanoli, P., Lindenblatt, N., & Gousopoulos, E. (2022). Is Lymphedema a Systemic Disease? A Paired Molecular and Histological Analysis of the Affected and Unaffected Tissue in Lymphedema Patients. Biomolecules, 12(11), 1667. https://doi.org/10.3390/biom12111667