Abstract
Background: Despite existing evidence of the high predictive value of natriuretic peptides (NPs) in patients with heart failure (HF), patients treated with guideline-directed therapy who have low or near-normal NP levels are unlikely to be correctly stratified for risk of clinical outcomes. The aim of this study is to detect plausible predictors for poor one-year clinical outcomes in patients with HFpEF and low NT-proBNP treated with in accordance with conventional guidelines. Methods: A total of 337 patients with HF with preserved ejection fraction (HFpEF) who had low levels of N-terminal natriuretic pro-peptide (NT-proBNP) at discharge due to optimal guideline-based therapy were enrolled in the study. The course of the observation was 3 years. Echocardiography and the assessment of conventional hematological and biochemical parameters, including NT-proBNP, tumor necrosis factor-alpha, high-sensitivity C-reactive protein (hs-CRP), adropin, irisin, visfatin, and fetuin-A, were performed at baseline and at the end of the study. Results: Three-year cumulative clinical endpoints (cardiovascular death, myocardial infarction or unstable angina or acute coronary syndrome, worsening HF, sudden cardiac death, or cardiac-related surgery or all-cause death) were detected in 104 patients, whereas 233 did not meet the endpoint. After adjusting for an age ≥ 64 years and a presence of atrial fibrillation, diabetes mellitus, chronic kidney disease (CKD) stages 1–3 and dilated cardiomyopathy, the multivariable Cox regression analysis showed that an irisin level of ≤7.2 ng/mL was an independent predictor of cumulative clinical endpoint. Moreover, patients with levels of irisin > 7.2 ng/mL had a better Kaplan–Meier survival rate than those with a lower serum irisin level (≤7.2 ng/mL). Conclusions: Multivariable analysis showed that an age ≥ 64 years; the presence of atrial fibrillation, diabetes mellitus, CKD stages 1–3 and dilated cardiomyopathy; an LAVI ≥ 39 mL/m2; and serum levels of hs-CRP ≥ 6.10 mg/L, irisin ≤ 7.2 ng/mL, and visfatin ≤ 1.1 ng/mL were predictors of poor clinical outcomes in HFpEF with low levels of NT-proBNP. A serum level of irisin ≤ 7.2 ng/mL could emerge as valuable biomarker for predicting long-term prognosis among HFpEF patients with low or near-normal levels of NT-proBNP.
1. Introduction
Heart failure (HF) remains a highly prevalent life-threatening condition in older adults that is associated with a high 1-year risk of death and hospitalization, as well as poor functional capacity and quality of life [1]. The median prevalence rate of all HF phenotypes is 11.8% (range 4.7–13.3%), but over the last decade, HF with preserved ejection fraction (HFpEF) has been more common [median prevalence 4.9% (range 3.8–7.4%)] than HF with reduced ejection fraction (HFrEF) [median prevalence 3.3% (range 2.4–5.8%)] [2]. However, HF prevalence, new incidence and survival varied widely in close connection with age, gender, ethnicity, HF phenotype, concomitant comorbidity profile, and certain socio-demographic factors, including affordability of health system resources and guideline-directed medical therapies [3,4,5]. On the other hand, early-to-moderate stages of HFpEF remain more frequently under-recognized than symptomatic HFrEF or HF with mildly reduced ejection fraction (HFmrEF) in everyday practice due to a wide range of comorbidity patterns, including metabolic syndrome, obesity, diabetes mellitus, chronic kidney disease, respiratory and autoimmune diseases [6,7].
Although patients with any HF phenotypes showed a strict similarity in short-term hospitalization rate, the long-term survival rate may vary sufficiently depending on age, HF etiology, comorbidity status and N-terminal brain natriuretic pro-peptide (NT-proBNP) levels [8]. In fact, HF patients with low (<300 ng/L)/near-normal (<125 ng/L) NT-proBNP levels had a better prognosis than those with elevated NT-proBNP levels (>300 ng/L), regardless of HF phenotype [9]. A high proportion of the individuals with any HF phenotype with low NT-proBNP levels exhibits a high incidence of diabetes and obesity. In alignment with this, among of those who reached target levels of NT-proBNP (<1000 ng/L), there were no significant differences in the presence of metabolic comorbidities, but many patients had better clinical status and cardiac performance, including improved left ventricular ejection fraction (LVEF) and quality of life and greater longevity than those with higher levels of NT-proBNP [10,11].
Another aspect concerns patients with HF who were discharged from hospital after decompensation with hemodynamic stability, improved LVEF and low NT-proBNP. More of these individuals were treated with conventional guideline-based therapy, including renin-angiotensin-aldosterone system antagonists, beta-blockers, mineralocorticoid receptor antagonists and sodium-glucose cotransporter-2 (SGLT2i) inhibitors [12]. However, near-normal/low levels of NT-proBNP seem not to be a significant predictive factor for further adverse clinical outcomes, including mortality and HF-related outcomes, when compared with elevated concentrations of this pro-peptide [13]. In fact, there are no evidence-based recommendations for clinical risk assessment in patients with HF with improved LVEF (HFimpEF)/HFpEF with low or near-normal NT-proBNP [14]. Although numerous clinical studies have identified numerous plausible predictors (male sex, left atrial volume index, left ventricular end diastolic dimension, anemia, neutrophil count, the levels of myokines/hepatokines including irisin and adropin, glomerular filtration rate, creatinine, pre-existing kidney failure, atrial fibrillation, diabetes mellitus) for these patients [15,16,17,18,19], reliable predictors corresponding with this clinical presentation remain to be discussed scientifically. Moreover, the predictive utility of metabolic-related factors for HF outcomes, such as adipokines with inflammatory activity, myokines, hepatokines, and inflammatory cytokines, is not still fully recognized [20,21,22].
Indeed, visceral, perivascular and epicardial adipose tissues, the myocardium, skeletal muscles, and the liver are considered endocrine organs that synthesize and release a broad spectrum of cytokines with pro- and anti-inflammatory properties, many of which are directly and indirectly involved in the pathogenesis of adverse cardiac remodeling and are responsible for HF development and progression [23]. Apelin is an anti-inflammatory and angiopoetic adipokine, whose levels are markedly reduced in patients with chronic HF and upregulated after reversible structure cardiac remodeling [24]. Circulating levels of visfatin—a metabolic regulator of oxidative phosphorylation and suppressor of oxidative stress—were found to be significantly lower in patients with HF [25]. Fetuin-A—multifunctional adipokine/hepatokines (known as tissue chaperone) with organoprotective properties—presented a link with liver hypoperfusion in HFrEF and was inversely correlated with exercise tolerance and survival [26]. Patients with HF, especially those with HFrEF and HFmrEF, had sufficiently reduced serum concentrations of adipokine/myokines irisin, which has organ-protective and anti-inflammatory properties, and increased levels of inflammatory cytokines such as tumor necrosis factor-alpha and C-reactive protein [27]. Indeed, the synthesis of irisin—an out-membrane part of fibronectin type III domain-containing 5 protein—may be activated in skeletal muscles, the myocardium and adipose tissue by peroxisome proliferator-activated receptor γ coactivator-1α during physical exercise [28]. Irisin acts by binding to its receptor integrin, αV/β5, to induce the browning of white adipose tissue, maintain glucose homeostasis, maintain bone homeostasis and attenuate cardiac injury. Along with this, irisin may regulate muscle regeneration, promote neurogenesis and angiogenesis, maintain hepatic gluconeogenesis, and ameliorate cardiac injury [29,30]. In numerous pathological conditions, irisin attenuates mitochondrial dysfunction, suppresses oxidative stress, and improves metabolic imbalance and energy expenditure [31]. Irisin levels are inversely associated with the severity of HF, especially with HFrEF, and negatively correlated with myocardial infarct area [31,32]. However, their discriminative abilities in patients with HFpEF with low NT-proBNP have not yet been deeply studied. The aim of this study is to detect plausible predictors for poor one-year clinical outcomes in patients with HFpEF and low NT-proBNP treated with in accordance with conventional guidelines.
2. Materials and Methods
2.1. Study Population
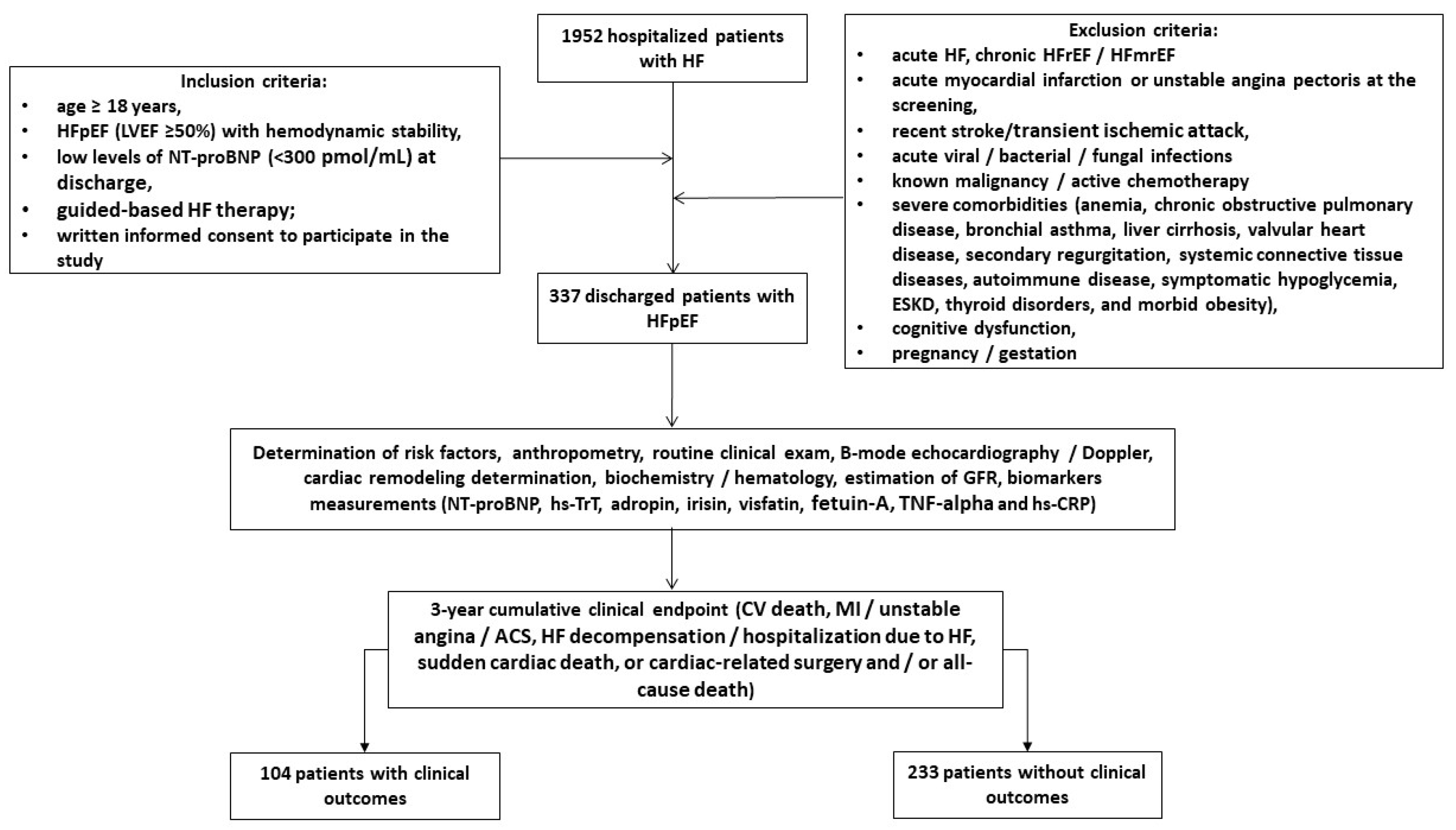
Using our local database, we pre-screened 1952 patients with HF who were hospitalized for HF progression and had elevated NT-proBNP (≥450 pg/mL) at discharge with a descending trajectory of NT-proBNP during hospital stay. Finally, we enrolled 337 discharged patients according to the following inclusion criteria: age ≥ 18 years, hemodynamic stability and established HFpEF at hospital discharge, low levels of NT-proBNP (<300 pg/mL) at hospital discharge, and written informed consent to participate in the study (Figure 1). The major exclusion criteria included the following: patients with acute HF, HF with reduced (HFrEF) and mildly reduced (HFmrEF) ejection fraction, acute myocardial infarction, unstable angina, recent stroke/transient ischemic attack, acute viral and bacterial infection, known malignancy, active chemotherapy, with severe comorbidities, including end stage renal disease (ESRD), cognitive dysfunction, dementia, pregnancy or gestation. We followed patients for 3 years and divided them into two cohorts depending on the presence of clinical combined outcomes.
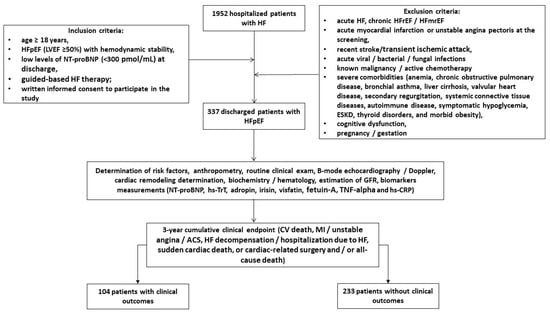
Figure 1.
Flowchart of the study design. Abbreviations: ACS, acute coronary syndrome; CV, cardiovascular; ESRD, end-stage renal disease; HF, heart failure; HFpEF, heart failure with preserved ejection fraction; HFrEF, heart failure with reduced ejection fraction; HFmrEF, heart failure with mildly reduced ejection fraction; LVEF, left ventricular ejection fraction; MI, myocardial infarct; TNF-alpha, tumor necrosis factor-alpha; hs-CRP, high-sensitivity C-reactive protein; hs-TrT, high-sensitivity troponin T; NT-proBNP, N-terminal natriuretic pro-peptide.
2.2. Determination of Clinical Outcomes and Follow-Up
We determined a 3-year cumulative clinical endpoint that included CV death, myocardial infarction or unstable angina or acute coronary syndrome, HF decompensation or hospitalization due to HF, sudden cardiac death, or cardiac-related surgery and/or all-cause death. To detect the cumulative clinical endpoint, we conducted direct interviews with patients and their relatives, contacted general practitioners, and reviewed databases, discharge and autopsy reports. Data were collected via clinic visits at baseline (at discharge from the hospital) and during the 36 months following the start of the study.
2.3. Echocardiography Examination
In the study, all patents underwent a routine transthoracic B-mode and Doppler ultrasound examination, which was performed by experienced echo cardiographer in apical two- and four-chamber views using a GE Healthcare Vivid E95 scanner (General Electric Company, Horton, Norway). The conventional hemodynamic parameters included the left ventricular ejection fraction (LVEF) using Simpson’s method, the left ventricular end-diastolic (LVEDV) and end-systolic (LVESV) volumes, the left atrial volume index (LAVI), early diastolic blood filling (E), and the mean longitudinal strain ratio (e′), which were evaluated according to the 2018 guidelines of the American Society of Echocardiography [33]. The estimated E/e′ ratio was expressed as the ratio of the E-wave velocity to the average of the medial and lateral e’ velocities. After the acquisition of high-quality echocardiographic data during at least three cardiac cycles, LV GLS was obtained by 2D speckle-tracking image analysis. The data were stored in the DICOM format for subsequent analysis. The left ventricular mass index (LVMI) was defined as ≥95 g/m2 in women or ≥115 g/m2 in men [33].
2.4. Blood Sampling
Blood samples were obtained from all participants in fasting condition and collected in BD Vacutainer Serum Plus tubes. After centrifugation at 3000 rpm for 10 min, the supernatant was collected and stored at −70 °C until analysis.
2.5. Biomarkers Assessment
Conventional hematological and biochemical parameters were determined with a Roche P800 analyzer (Basel, Switzerland) in the local laboratory of the Vita Centre (Zaporozhye, Ukraine). Data on routine blood indices, including glucose, total cholesterol, triglycerides, high-density lipoprotein (HDL-C) and low-density lipoprotein (LDL-C) cholesterol, serum uric acid, and serum creatinine, were recorded. In addition, we measured circulating biomarkers (NT-proBNP, tumor necrosis factor-alpha [TNF-alpha], high-sensitivity C-reactive protein [hs-CRP], adropin, irisin, visfatin, fetuin-A) in serum using ELISA kits (Elabscience, Houston, TX, USA) in accordance with the instructions provided by the manufacturer at the initial baseline measurement and at the end of the study. The data obtained from the ELISA analysis were subjected to a standard curve-based evaluation. Each sample was analyzed in duplicate, and the mean value was employed for the final analysis. Both intra- and inter-assay coefficients of variability for each marker were <10%.
2.6. Glomerular Filtration Rate Estimation
A conventional CKD-EPI formula was to estimate the glomerular filtration rate (eGFR) [34].
2.7. Statistics
All statistical analyses were conducted using SPSS 11.0 for Windows and Graph Pad Prism, version 9 (Graph Pad Software, San Diego, CA, USA). A Kolmogorov–Smirnov test was used to determine whether data were normally distributed. All continues variables were expressed as mean ± standard deviation [SD] median and interquartile range [IQR] depending on whether the data were normally distributed, whereas categorical variables were presented as number (n) and percentage (%). Categorical variables were compared using the chi-squared test. The Mann–Whitey U test was used to compare differences in continuous variables between cohorts with and without combined clinical events. Receiver operating characteristic (ROC) curves were used to calculate the cutoff values of irisin for predicting combined clinical events. To determine the optimal cutoff value for the predictors, Youden’s index (sensitivity + specificity − 1) was used. Univariate and multivariate Cox proportional hazard models were constructed to predict the independent prognostic factors for the clinical endpoint. Significant variables (p < 0.05) comparing cohorts with and without cumulative endpoints were entered into univariate Cox regression analysis, and those retaining statistical significance (p < 0.05) were entered into the multivariate Cox proportional hazards model. The odds ratio (OR) and 95% confidence interval (CI) were reported for each predictor variable. The Kaplan–Meier method was used to compare the survival rates, and survival curves were plotted. A p-value of less than 0.05 was considered to indicate a statistically significant difference.
3. Results
3.1. Baseline Clinical Characteristics
A total of 337 patients with HFpEF, New York Heart Association class II (n = 133)/III (n = 204), and low NT-proBNP at discharge were enrolled in the study and divided into two cohorts depending on the presence of a 3-year cumulative endpoint (n = 104) or an absent of it (n = 233). The follow-up time was 3 years. The clinical characteristics of the patients are outlined in Table 1.

Table 1.
Basic characteristics of the patients involved in this study.
Patients in the entire group were respectively young (a mean age of 61 years), mainly male, and had a low presentation frequency of atrial fibrillation, diabetes mellitus, abdominal obesity, and chronic kidney disease. However, there was a high presence of hypertension, left ventricular hypertrophy and the NYHA III functional class. They were well-treated with antagonists of renin-angiotensin-aldosterone system (ACE inhibitors, or angiotensin-II receptor blockers or angiotensin receptor-neprilysin inhibitors), beta-blockers, mineralocorticoid receptor antagonists and sodium–glucose cotransporter-2 inhibitors according to guidelines, whereas only 58% of the patients had a need for maintenance loop diuretics at discharge.
There were no significant differences between the two cohorts with respect to sex, body mass index, anthropometric parameters, presence of dyslipidemia, hypertension, stable coronary artery disease, smoking, abdominal obesity, systolic and diastolic blood pressure, left ventricular dimensions, LVEF, LVMI, E/e′, GLS, eGFR, lipid profile, glucose levels, TNF-alpha, NT-proBNP, adropin, visfatin, fetuin-A, or hs-TrT. Patients in the cumulative clinical endpoint cohort were older; more likely to have atrial fibrillation and diabetes mellitus; be in CKD stages 1–3; and have dilated cardiomyopathy, higher LAVI and lower irisin levels than those in the free endpoint cohort. The patients in the cumulative clinical endpoint cohort tended to be treated frequently with angiotensin-II receptor blockers, anticoagulants, metformin when compared with those who had no clinical endpoint.
3.2. Receiver Operating Characteristic Curve Analysis for Predictive Factors of Cumulative Clinical Endpoint
ROC curve analysis was performed to determine the optimal cutoff for possible predictors of clinical outcomes, shown in Table 2. We identified the following factors: age ≥ 64 years, hemoglobin < 125 g/L, body mass index ≥ 27.5 kg/m2, LAVI ≥ 39 mL/m2, hs-CRP ≥ 6.10 mg/L irisin and visfatin ≤ 7.2 ng/ and ≤1.1 ng/mL, respectively.
Table 2.
Receiver operating characteristic (ROC) curve analysis for predictive factors of 3-year cumulative clinical outcome.
3.3. Predictive Factors for 3-Year Cumulative Clinical Endpoint: Unadjusted and Adjusted for Multivariate Cox Proportional Hazard Models
A Cox proportional hazards model was constructed for the assessment of independent predictors of the 3-year cumulative clinical endpoint (Table 3).
Table 3.
Cox regression analysis for predictive factors of cumulative clinical endpoint.
After adjusting for an age ≥ 64 years and the presence of atrial fibrillation, diabetes mellitus, CKD stages 1–3 and dilated cardiomyopathy (Model 2), the multivariable Cox regression analysis revealed that a level of irisin ≤ 7.2 ng/mL was an independent predictor of the cumulative clinical endpoint.
3.4. Kaplan–Meier Curves Survival Analysis
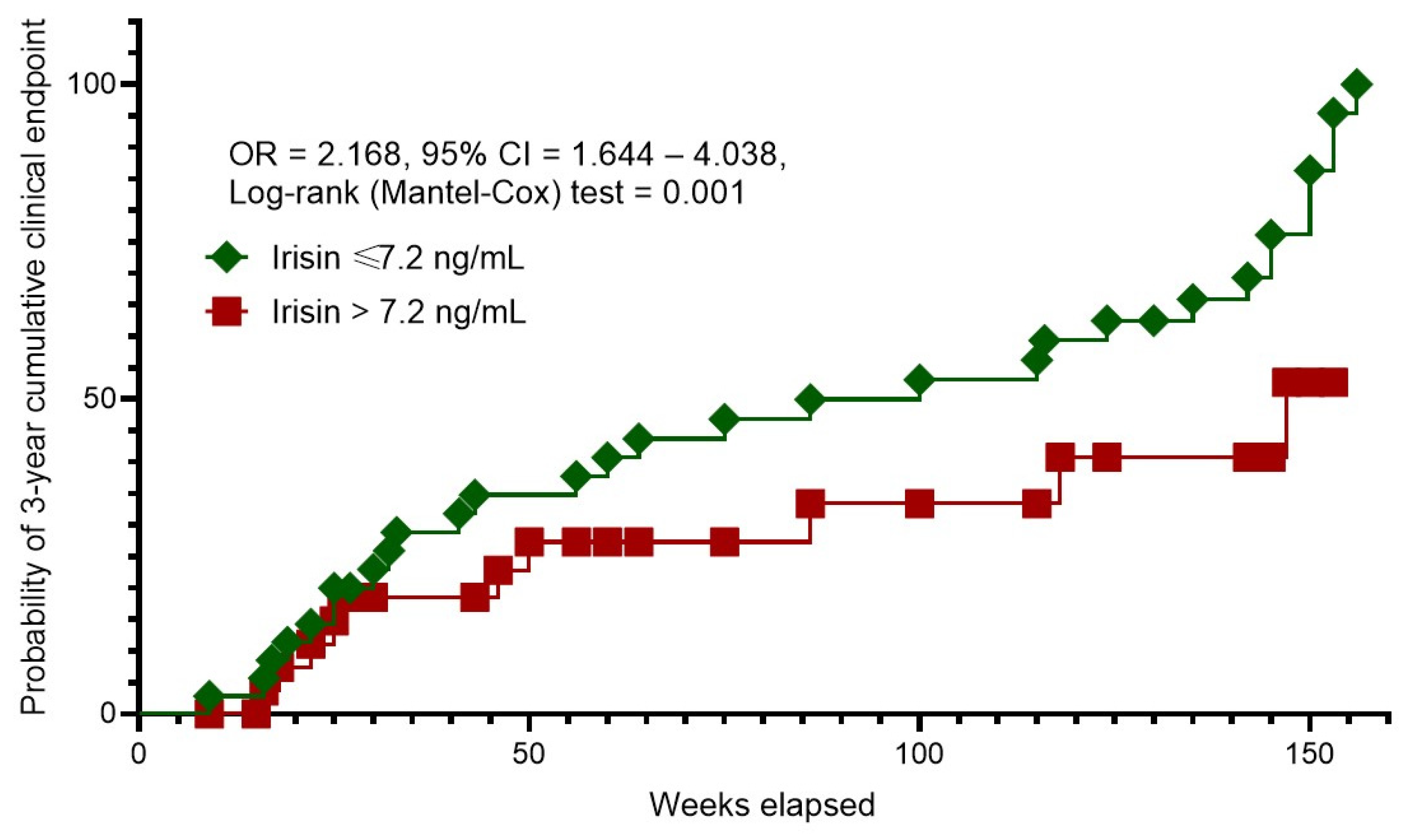
The Kaplan–Meier curves revealed different probability rates of 3-year cumulative clinical endpoint between patients with HFpEF and serum irisin levels of ≤7.2 ng/mL and >7.2 ng/mL (Figure 2). Of note, patients with irisin levels > 7.2 ng/mL had a sufficient benefit in terms of survival than those with serum irisin levels ≤ 7.2 ng/mL.
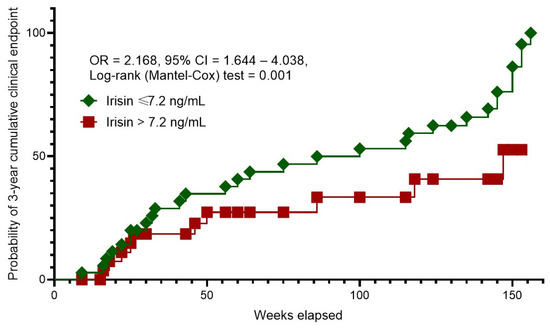
Figure 2.
Kaplan–Meier curves for 3-year cumulative clinical endpoint. Abbreviations: OR, odds ratio; CI, confidence interval.
4. Discussion
Only HFpEF patients who responded to optimal guided-based therapy and at discharge gave the impression of adequately compensated low-risk patients were included in this study. We identified an age ≥ 64 years, the presence of atrial fibrillation, diabetes mellitus, CKD stages 1–3 and dilated cardiomyopathy, an LAVI ≥ 39 mL/m2, and serum levels of hs-CRP ≥ 6.10 mg/L, irisin ≤ 7.2 ng/mL and visfatin ≤ 1.1 ng/mL as predictors of poor clinical outcome in HFpEF patients treated with guideline-based optimal therapy with target level of NT-proBNP less than 300 pmol/mL. After adjusting for concomitant comorbidities and age, serum levels of irisin ≤ 7.2 ng/mL remained an independent predictive factor for the 3-year cumulative clinical endpoint. Moreover, the individuals with circulating irisin > 7.2 ng/mL exerted a significant superiority in survival rate when compared with those with lower irisin levels (≤7.2 ng/mL). These findings offer new perspectives in the stratification of patients with HFpEF who have achieved target NT-proBNP levels as a result of conventional management and/or concomitant comorbidities such as obesity.
The hypothesis is as follows: this is an apparently low risk that does not reflect the population level of risk in people without HFpEF, and these patients are under-screened individuals for whom the risk of adverse outcomes is underestimated. Irisin is likely to be the molecule that overcomes the limitations of natriuretic peptides in identifying patients at residual risk in the context of optimal treatment.
Previous studies and systematic reviews highlighted the plausible prognostic role of BNP and NT-proBNP in predicting adverse clinical outcomes, including all-cause mortality, cardiovascular events, and hospitalization in HFpEF patients, [13,35,36]. However, the predictive role of NPs in HFpEF seem to be controversial, because low levels of NT-proBNP often leave the risk of HF progression underestimated [37]. Meanwhile, patients hospitalized with HFpEF often have low NT-proBNP levels, which was associated with age < 65 years, ischemic etiology, obesity, higher LVEF, eGFR > 80 mL/kg/1.73 m2, and a lower NYHA class, whereas chronic kidney disease and diabetes mellitus were associated with elevated levels of NT-proBNP [9,38,39]. Moreover, clinical status was similarly impaired in HF patients with lower and higher NT-proBNP levels [40]. Azzo JD et al. (2024) [41] reported that higher levels of NT-proBNP were more associated with inflammation and fibrosis than low concentrations of the biomarker. On the other hand, the elevation of NT-proBNP in serial measurements reflected a dynamic change in risk for HF events and death, whereas stable levels of NT-proBNP were related to a lower risk of incident HF and mortality [42]. Thus, the risk of patients with low NP levels remains often out of the zone of interest or is only used as a reference level when comparing to higher values of NT-proBNP. The use of cardiac troponins as an alternative biomarker for risk stratification in a patient with low NT-proBNP levels also remains inadequate because a positive troponin test improves the predictive and diagnostic value of natriuretic peptides only when their concentrations are high [43]. In this context, the search for new biomarkers with independent predictive value for adverse clinical events in HFpEF and low NT-proBNP remains very relevant.
We hypothesized that the comorbidity signature may not only contribute to adverse cardiac remodeling but may also be associated with a distinct cytokine profile reflecting the metabolic homeostasis of distant organs, such as skeletal muscle, adipose tissue, and liver. Although these organs synthesize and secrete a wide range of metabolically active molecules involved in the development and progression of HF, their discriminative properties for HF, particularly in people with HFpEF, have not been established. In this study, we established that apart from older age and known concomitant comorbidities such as atrial fibrillation, diabetes mellitus, CKD stages 1–3 and dilated cardiomyopathy, altered levels of hs-CRP, visfatin and irisin (which belong to the adipokines/myokines) were predictors for cumulative clinical endpoint for 3 years in patients with HFpEF and low levels of NT-proBNP. In fact, an irisin level ≤ 7.2 ng/mL alone was found to be an independent predictor of adverse clinical outcomes for patients with HFpEF after adjusting for age and concomitant comorbidities.
Previous studies have shown that irisin can be synthesized and secreted not only by skeletal muscle but also by the myocardium to maintain energy homeostasis [44]. The alteration of irisin levels in HF is considered a possible mechanism of skeletal muscle metabolic remodeling, cardiac hypertrophy and the persistence of a clinical sign such as fatigue [45]. Moreover, in chronic HFpEF patients rather than those with HFmrEF and HFrEF, low levels of irisin exerted predictive potency for adverse outcomes [15,46,47]. Since irisin has shown an inverse correlation with inflammatory biomarkers such as CRP and TNF-alpha, and LDL in previous studies, it was hypothesized that one of the possible molecular mechanisms for the negative impact of altered levels of irisin on prognosis is excessive inflammatory response, oxidative stress/damage and mitochondrial dysfunction due to activation of apoptosis/pyroptosis and autophagy via irisin precursor fibronectin type III domain-containing protein 5 and the AKT/GSK3β/FYN/Nrf2 axis in an mTOR-independent manner [48,49]. In this context, altered irisin regulation links adverse cardiac remodeling and skeletal muscle dysfunction with metabolic comorbidities such as diabetes mellitus, obesity and metabolic syndrome [50,51]. In addition, irisin may have the ability to modify cellular plasticity through alternative signaling pathways such as cAMP/PKA/CREB and Wnt signaling [52]. In this context, the molecular targets of irisin may correspond to those of lysine β-hydroxybutyrylation (Kbhb), a regulator of post-translational modification [53]. This may suggest that irisin acting through the Kbhb-related enhancement of mitochondrial enzyme activity such as glutamate oxaloacetate transaminase is likely to be crucial for preventing mitochondrial dysfunction and the progression of structural cardiac remodeling. Therefore, irisin along with a product of histone Kbhb activation β-hydroxybutyrate—the main component of the ketone body—may induce the ketogenesis, which, acting through SIRT3-dependent pathways, ensures adaptive metabolic changes in mitochondria [54]. Finally, the cardioprotective effects (anti-arrhythmic and anti-ischemic effects) of several agents, which are included in optimal guideline-based HF therapy, such as sodium-glucose co-transporter 2 inhibitors, can be mediated by restoring circulating irisin levels [15,55,56,57].
However, the predictive value of irisin for distant events in patients with HFpEF requires further explanation. An indirect effect of irisin deficiency on the number of cardiovascular events through the progression of microvascular inflammation and impaired myocardial perfusion cannot be excluded. This suggestion seems to be a reason for further investigations.
5. Study Limitations
The study has several limitations. The first limitation is the lack of data regarding the trajectory of biological markers during the observational period in connection with the rate of adverse clinical outcomes. However, we did not investigate the quality of life of the patients and its association with the changes in irisin levels. Finally, we did not compare the discriminative value of irisin with previously validated risk scores. However, we do not believe that these limitations will have an impact on the interpretation of the results.
6. Conclusions
Multivariable analysis showed that an age ≥ 64 years; the presence of atrial fibrillation, diabetes mellitus, CKD stages 1–3 and dilated cardiomyopathy; an LAVI ≥ 39 mL/m2; and serum levels of hs-CRP ≥ 6.10 mg/L, irisin ≤ 7.2 ng/mL and visfatin ≤ 1.1 ng/mL were predictors of poor clinical outcome in HFpEF. A serum level of irisin ≤ 7.2 ng/mL could emerge as valuable biomarker for predicting long-term prognosis among HFpEF patients with low or near-normal levels of NT-proBNP.
Author Contributions
Conceptualization, A.E.B.; methodology, A.E.B.; software, O.O.B.; validation, T.A.B., A.E.B. and M.L.; formal analysis, O.O.B., T.A.B. and A.E.B.; investigation, O.O.B. and T.A.B.; resources, T.A.B. and O.O.B.; data curation, A.E.B. and T.A.B.; writing—original draft preparation: T.A.B., O.O.B., E.V.N., M.L. and A.E.B.; writing—review and editing, T.A.B., O.O.B., E.V.N., M.L. and A.E.B.; visualization, O.O.B. and E.V.N.; supervision, A.E.B.; project administration, T.A.B. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
This study was conducted according to the guidelines of the Declaration of Helsinki and was approved by the Institutional Ethics Committee of Zaporozhye Medical Academy of Post-graduate Education (protocol number: 8; date of approval: 10 October 2020).
Informed Consent Statement
Written informed consent has been obtained from all patients in this study.
Data Availability Statement
The data presented in this study are available on request from the corresponding author due to privacy restrictions.
Acknowledgments
We thank all the patients who gave their consent to participate in this study and all the administrative staff and doctors of the private hospital “Vita Centre” for their assistance in the study.
Conflicts of Interest
The authors declare no competing interests.
References
- Emmons-Bell, S.; Johnson, C.; Roth, G. Prevalence, incidence and survival of heart failure: A systematic review. Heart 2022, 108, 1351–1360. [Google Scholar] [CrossRef] [PubMed]
- Van Riet, E.E.; Hoes, A.W.; Wagenaar, K.P.; Limburg, A.; Landman, M.A.; Rutten, F.H. Epidemiology of heart failure: The prevalence of heart failure and ventricular dysfunction in older adults over time. A systematic review. Eur. J. Heart Fail. 2016, 18, 242–252. [Google Scholar] [CrossRef] [PubMed]
- Yu, B.; Akushevich, I.; Yashkin, A.P.; Yashin, A.I.; Lyerly, H.K.; Kravchenko, J. Epidemiology of geographic disparities in heart failure among US older adults: A Medicare-based analysis. BMC Public. Health 2022, 22, 1280. [Google Scholar] [CrossRef]
- Savarese, G.; Becher, P.M.; Lund, L.H.; Seferovic, P.; Rosano, G.M.C.; Coats, A.J.S. Global burden of heart failure: A comprehensive and updated review of epidemiology. Cardiovasc. Res. 2023, 118, 3272–3287. [Google Scholar] [CrossRef] [PubMed]
- Desai, R.J.; Stonely, D.; Ikram, N.; Levin, R.; Bhatt, A.S.; Vaduganathan, M. County-Level Variation in Triple Guideline-Directed Medical Therapy in Heart Failure With Reduced Ejection Fraction. JACC Adv. 2024, 3, 101014. [Google Scholar] [CrossRef]
- Campbell, P.; Rutten, F.H.; Lee, M.M.; Hawkins, N.M.; Petrie, M.C. Heart failure with preserved ejection fraction: Everything the clinician needs to know. Lancet 2024, 403, 1083–1092. [Google Scholar] [CrossRef] [PubMed]
- Palazzuoli, A.; Ruocco, G.; Gronda, E. Noncardiac comorbidity clustering in heart failure: An overlooked aspect with potential therapeutic door. Heart Fail. Rev. 2022, 27, 767–778. [Google Scholar] [CrossRef] [PubMed]
- Borlaug, B.A.; Sharma, K.; Shah, S.J.; Ho, J.E. Heart Failure With Preserved Ejection Fraction: JACC Scientific Statement. J. Am. Coll. Cardiol. 2023, 81, 1810–1834. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.Y.; Liang, L.; Tian, P.C.; Feng, J.Y.; Huang, L.Y.; Huang, B.P.; Zhao, X.M.; Wu, Y.H.; Wang, J.; Guan, J.Y.; et al. Clinical characteristics and outcomes of patients hospitalized with heart failure with preserved ejection fraction and low NT-proBNP levels. Medicine 2023, 102, e36351. [Google Scholar] [CrossRef] [PubMed]
- Pieske, B.; Wachter, R.; Shah, S.J.; Baldridge, A.; Szeczoedy, P.; Ibram, G.; Shi, V.; Zhao, Z.; Cowie, M.R.; PARALLAX Investigators and Committee members. Effect of Sacubitril/Valsartan vs Standard Medical Therapies on Plasma NT-proBNP Concentration and Submaximal Exercise Capacity in Patients With Heart Failure and Preserved Ejection Fraction: The PARALLAX Randomized Clinical Trial. JAMA 2021, 326, 1919–1929. [Google Scholar] [CrossRef]
- Januzzi, J.L., Jr.; Prescott, M.F.; Butler, J.; Felker, G.M.; Maisel, A.S.; McCague, K.; Camacho, A.; Piña, I.L.; Rocha, R.A.; Shah, A.M.; et al. Association of Change in N-Terminal Pro-B-Type Natriuretic Peptide Following Initiation of Sacubitril-Valsartan Treatment with Cardiac Structure and Function in Patients with Heart Failure with Reduced Ejection Fraction. JAMA 2019, 322, 1085–1095. [Google Scholar] [CrossRef] [PubMed]
- Wilcox, J.E.; Fang, J.C.; Margulies, K.B.; Mann, D.L. Heart Failure With Recovered Left Ventricular Ejection Fraction: JACC Scientific Expert Panel. J. Am. Coll. Cardiol. 2020, 76, 719–734. [Google Scholar] [CrossRef]
- Ammar, L.A.; Massoud, G.P.; Chidiac, C.; Booz, G.W.; Altara, R.; Zouein, F.A. BNP and NT-proBNP as prognostic biomarkers for the prediction of adverse outcomes in HFpEF patients: A systematic review and meta-analysis. Heart Fail. Rev. 2024, 30, 45–54. [Google Scholar] [CrossRef] [PubMed]
- Pensa, A.V.; Khan, S.S.; Shah, R.V.; Wilcox, J.E. Heart failure with improved ejection fraction: Beyond diagnosis to trajectory analysis. Prog. Cardiovasc. Dis. 2024, 82, 102–112. [Google Scholar] [CrossRef] [PubMed]
- Berezina, T.A.; Fushtey, I.M.; Berezin, A.A.; Pavlov, S.V.; Berezin, A.E. Predictors of Kidney Function Outcomes and Their Relation to SGLT2 Inhibitor Dapagliflozin in Patients with Type 2 Diabetes Mellitus Who Had Chronic Heart Failure. Adv. Ther. 2024, 41, 292–314. [Google Scholar] [CrossRef]
- Çavuşoğlu, Y.; Çelik, A.; Altay, H.; Nalbantgil, S.; Özden, Ö.; Temizhan, A.; Ural, D.; Ünlü, S.; Yılmaz, M.B.; Zoghi, M. Heart failure with non-reduced ejection fraction: Epidemiology, pathophysiology, phenotypes, diagnosis and treatment approaches. Turk. Kardiyol. Dern. Ars. 2022, 50 (Suppl. 1), S1–S34. [Google Scholar] [CrossRef] [PubMed]
- Berezin, A.A.; Obradovic, A.B.; Fushtey, I.M.; Berezina, T.A.; Lichtenauer, M.; Berezin, A.E. Low Plasma Levels of Irisin Predict Acutely Decompensated Heart Failure in Type 2 Diabetes Mellitus Patients with Chronic Heart Failure. J. Cardiovasc. Dev. Dis. 2023, 10, 136. [Google Scholar] [CrossRef]
- Li, Q.; Qiao, Y.; Tang, J.; Guo, Y.; Liu, K.; Yang, B.; Zhou, Y.; Yang, K.; Shen, S.; Guo, T.; et al. Frequency, predictors, and prognosis of heart failure with improved left ventricular ejection fraction: A single-centre retrospective observational cohort study. ESC Heart Fail. 2021, 8, 2755–2764. [Google Scholar] [CrossRef] [PubMed]
- Wu, N.; Lang, X.; Zhang, Y.; Zhao, B.; Zhang, Y. Predictors and Prognostic Factors of Heart Failure with Improved Ejection Fraction. Rev. Cardiovasc. Med. 2024, 25, 280. [Google Scholar] [CrossRef]
- Berezin, A.E.; Berezin, A.A.; Lichtenauer, M. Myokines and Heart Failure: Challenging Role in Adverse Cardiac Remodeling, Myopathy, and Clinical Outcomes. Dis. Markers 2021, 2021, 6644631. [Google Scholar] [CrossRef] [PubMed]
- Tomita, Y.; Misaka, T.; Yoshihisa, A.; Ichijo, Y.; Ishibashi, S.; Matsuda, M.; Yamadera, Y.; Ohara, H.; Sugawara, Y.; Hotsuki, Y.; et al. Decreases in hepatokine Fetuin-A levels are associated with hepatic hypoperfusion and predict cardiac outcomes in patients with heart failure. Clin. Res. Cardiol. 2022, 111, 1104–1112. [Google Scholar] [CrossRef] [PubMed]
- Kalkan, A.K.; Cakmak, H.A.; Erturk, M.; Kalkan, K.E.; Uzun, F.; Tasbulak, O.; Diker, V.O.; Aydin, S.; Celik, A. Adropin and Irisin in Patients with Cardiac Cachexia. Arq. Bras. Cardiol. 2018, 111, 39–47. [Google Scholar] [CrossRef] [PubMed]
- Li, C.; Qin, D.; Hu, J.; Yang, Y.; Hu, D.; Yu, B. Inflamed adipose tissue: A culprit underlying obesity and heart failure with preserved ejection fraction. Front. Immunol. 2022, 13, 947147. [Google Scholar] [CrossRef] [PubMed]
- Rafaqat, S. Adipokines and Their Role in Heart Failure: A Literature Review. J. Innov. Card. Rhythm. Manag. 2023, 14, 5657–5669. [Google Scholar] [CrossRef] [PubMed]
- Straburzyńska-Migaj, E.; Pilaczyńska-Szcześniak, L.; Nowak, A.; Straburzyńska-Lupa, A.; Sliwicka, E.; Grajek, S. Serum concentration of visfatin is decreased in patients with chronic heart failure. Acta Biochim. Pol. 2012, 59, 339–343. [Google Scholar] [CrossRef] [PubMed]
- Tomita, Y.; Misaka, T.; Sugawara, Y.; Ichijo, Y.; Anzai, F.; Sato, Y.; Kimishima, Y.; Yokokawa, T.; Sato, T.; Oikawa, M.; et al. Reduced Fetuin-A Levels Are Associated with Exercise Intolerance and Predict the Risk of Adverse Outcomes in Patients With Heart Failure: The Role of Cardiac-Hepatic-Peripheral Interaction. J. Am. Heart Assoc. 2024, 13, e035139. [Google Scholar] [CrossRef] [PubMed]
- Abd El-Mottaleb, N.A.; Galal, H.M.; El Maghraby, K.M.; Gadallah, A.I. Serum irisin level in myocardial infarction patients with or without heart failure. Can. J. Physiol. Pharmacol. 2019, 97, 932–938. [Google Scholar] [CrossRef] [PubMed]
- Liu, S.; Cui, F.; Ning, K.; Wang, Z.; Fu, P.; Wang, D.; Xu, H. Role of irisin in physiology and pathology. Front. Endocrinol. 2022, 13, 962968. [Google Scholar] [CrossRef]
- He, X.; Hua, Y.; Li, Q.; Zhu, W.; Pan, Y.; Yang, Y.; Li, X.; Wu, M.; Wang, J.; Gan, X. FNDC5/irisin facilitates muscle-adipose-bone connectivity through ubiquitination-dependent activation of runt-related transcriptional factors RUNX1/2. J. Biol. Chem. 2022, 298, 101679. [Google Scholar] [CrossRef] [PubMed]
- Guo, W.; Peng, J.; Su, J.; Xia, J.; Deng, W.; Li, P.; Chen, Y.; Liu, G.; Wang, S.; Huang, J. The role and underlying mechanisms of irisin in exercise-mediated cardiovascular protection. PeerJ 2024, 12, e18413. [Google Scholar] [CrossRef]
- Grzeszczuk, M.; Dzięgiel, P.; Nowińska, K. The Role of FNDC5/Irisin in Cardiovascular Disease. Cells 2024, 13, 277. [Google Scholar] [CrossRef] [PubMed]
- Ho, M.Y.; Wang, C.Y. Role of Irisin in Myocardial Infarction, Heart Failure, and Cardiac Hypertrophy. Cells 2021, 10, 2103. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, C.; Rahko, P.S.; Blauwet, L.A.; Canaday, B.; Finstuen, J.A.; Foster, M.C.; Horton, K.; Ogunyankin, K.O.; Palma, R.A.; Velazquez, E.J. Guidelines for Performing a Comprehensive Transthoracic Echocardiographic Examination in Adults: Recommendations from the American Society of Echocardiography. J. Am. Soc. Echocardiogr. 2018, 32, 1–64. [Google Scholar] [CrossRef]
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.L.; Castro, A.F., 3rd; Feldman, H.I.; Kusek, J.W.; Eggers, P.; van Lente, F.; Greene, T.; et al. A new equation to estimate glomerular filtration rate. Ann. Intern. Med. 2009, 150, 604–612. [Google Scholar] [CrossRef]
- Cao, J.; Jin, X.J.; Zhou, J.; Chen, Z.Y.; Xu, D.L.; Yang, X.C.; Dong, W.; Li, L.W.; Luo, J.; Chen, L.; et al. Prognostic value of N-terminal B-type natriuretic peptide on all-cause mortality in heart failure patients with preserved ejection fraction. Zhonghua Xin Xue Guan Bing Za Zhi 2019, 47, 875–881. [Google Scholar] [CrossRef] [PubMed]
- Schmitt, W.; Rühs, H.; Burghaus, R.; Diedrich, C.; Duwal, S.; Eissing, T.; Garmann, D.; Meyer, M.; Ploeger, B.; Lippert, J. NT-proBNP Qualifies as a Surrogate for Clinical End Points in Heart Failure. Clin. Pharmacol. Ther. 2021, 110, 498–507. [Google Scholar] [CrossRef] [PubMed]
- Kosyakovsky, L.B.; Liu, E.E.; Wang, J.K.; Myers, L.; Parekh, J.K.; Knauss, H.; Lewis, G.D.; Malhotra, R.; Nayor, M.; Robbins, J.M.; et al. Uncovering Unrecognized Heart Failure with Preserved Ejection Fraction Among Individuals with Obesity and Dyspnea. Circ. Heart Fail. 2024, 17, e011366. [Google Scholar] [CrossRef]
- Zheng, Y.R.; Ye, L.F.; Cen, X.J.; Lin, J.Y.; Fu, J.W.; Wang, L.H. Low NT-proBNP levels: An early sign for the diagnosis of ischemic heart failure. Int. J. Cardiol. 2017, 228, 666–671. [Google Scholar] [CrossRef] [PubMed]
- Ceriello, A.; Lalic, N.; Montanya, E.; Valensi, P.; Khunti, K.; Hummel, M.; Schnell, O. NT-proBNP point-of-care measurement as a screening tool for heart failure and CVD risk in type 2 diabetes with hypertension. J. Diabetes Complicat. 2023, 37, 108410. [Google Scholar] [CrossRef]
- Kondo, T.; Campbell, R.; Jhund, P.S.; Anand, I.S.; Carson, P.E.; Lam, C.S.P.; Shah, S.J.; Vaduganathan, M.; Zannad, F.; Zile, M.R.; et al. Low Natriuretic Peptide Levels and Outcomes in Patients With Heart Failure and Preserved Ejection Fraction. JACC Heart Fail. 2024, 12, 1442–1455. [Google Scholar] [CrossRef] [PubMed]
- Azzo, J.D.; Dib, M.J.; Zagkos, L.; Zhao, L.; Wang, Z.; Chang, C.P.; Ebert, C.; Salman, O.; Gan, S.; Zamani, P.; et al. Proteomic Associations of NT-proBNP (N-Terminal Pro-B-Type Natriuretic Peptide) in Heart Failure With Preserved Ejection Fraction. Circ. Heart Fail. 2024, 17, e011146. [Google Scholar] [CrossRef]
- Jia, X.; Al Rifai, M.; Hoogeveen, R.; Echouffo-Tcheugui, J.B.; Shah, A.M.; Ndumele, C.E.; Virani, S.S.; Bozkurt, B.; Selvin, E.; Ballantyne, C.M.; et al. Association of Long-term Change in N-Terminal Pro-B-Type Natriuretic Peptide with Incident Heart Failure and Death. JAMA Cardiol. 2023, 8, 222–230. [Google Scholar] [CrossRef]
- Averina, M.; Stylidis, M.; Brox, J.; Schirmer, H. NT-ProBNP and high-sensitivity troponin T as screening tests for subclinical chronic heart failure in a general population. ESC Heart Fail. 2022, 9, 1954–1962. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Xie, S.; Guo, L.; Jiang, J.; Chen, H. Irisin: Linking metabolism with heart failure. Am. J. Transl. Res. 2020, 12, 6003–6014. [Google Scholar]
- Lyu, J.X.; Guo, D.D.; Song, Y.C.; Zhang, M.R.; Ge, F.Q.; Zhao, J.; Zhu, H.; Hang, P.Z. Circulating Myokines as Novel Biomarkers for Cardiovascular Diseases. Rev. Cardiovasc. Med. 2024, 25, 56. [Google Scholar] [CrossRef]
- Berezin, A.A.; Lichtenauer, M.; Boxhammer, E.; Stöhr, E.; Berezin, A.E. Discriminative Value of Serum Irisin in Prediction of Heart Failure with Different Phenotypes among Patients with Type 2 Diabetes Mellitus. Cells 2022, 11, 2794. [Google Scholar] [CrossRef] [PubMed]
- Berezina, T.A.; Berezin, O.O.; Hoppe, U.C.; Lichtenauer, M.; Berezin, A.E. Trajectory of Irisin as a Predictor of Kidney-Related Outcomes in Patients with Asymptomatic Heart Failure. Biomedicines 2024, 12, 1827. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Hu, C.; Kong, C.Y.; Song, P.; Wu, H.M.; Xu, S.C.; Yuan, Y.P.; Deng, W.; Ma, Z.G.; Tang, Q.Z. FNDC5 alleviates oxidative stress and cardiomyocyte apoptosis in doxorubicin-induced cardiotoxicity via activating AKT. Cell Death Differ. 2020, 27, 540–555. [Google Scholar] [CrossRef]
- Rabiee, F.; Lachinani, L.; Ghaedi, S.; Nasr-Esfahani, M.H.; Megraw, T.L.; Ghaedi, K. New insights into the cellular activities of Fndc5/Irisin and its signaling pathways. Cell Biosci. 2020, 10, 51. [Google Scholar] [CrossRef]
- Behera, J.; Ison, J.; Voor, M.J.; Tyagi, N. Exercise-Linked Skeletal Irisin Ameliorates Diabetes-Associated Osteoporosis by Inhibiting the Oxidative Damage-Dependent miR-150-FNDC5/Pyroptosis Axis. Diabetes 2022, 71, 2777–2792. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Ma, E.B.; Sahar, N.E.; Jeong, M.; Huh, J.Y. Irisin Exerts Inhibitory Effect on Adipogenesis Through Regulation of Wnt Signaling. Front. Physiol. 2019, 10, 1085. [Google Scholar] [CrossRef] [PubMed]
- Waseem, R.; Shamsi, A.; Mohammad, T.; Hassan, M.I.; Kazim, S.N.; Chaudhary, A.A.; Rudayni, H.A.; Al-Zharani, M.; Ahmad, F.; Islam, A. FNDC5/Irisin: Physiology and Pathophysiology. Molecules 2022, 27, 1118. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.; Li, X.; Yu, N.; Yan, R.; Sun, Y.; Tang, C.; Ding, W.; Ling, M.; Song, Y.; Gao, H.; et al. Proteomics and β-hydroxybutyrylation Modification Characterization in the Hearts of Naturally Senescent Mice. Mol. Cell Proteomics 2023, 22, 100659. [Google Scholar] [CrossRef] [PubMed]
- Zhou, T.; Cheng, X.; He, Y.; Xie, Y.; Xu, F.; Xu, Y.; Huang, W. Function and mechanism of histone β-hydroxybutyrylation in health and disease. Front. Immunol. 2022, 13, 981285. [Google Scholar] [CrossRef] [PubMed]
- Cesaro, A.; Gragnano, F.; Paolisso, P.; Bergamaschi, L.; Gallinoro, E.; Sardu, C.; Mileva, N.; Foà, A.; Armillotta, M.; Sansonetti, A.; et al. In-hospital arrhythmic burden reduction in diabetic patients with acute myocardial infarction treated with SGLT2-inhibitors: Insights from the SGLT2-I AMI PROTECT study. Front. Cardiovasc. Med. 2022, 9, 1012220. [Google Scholar] [CrossRef]
- Palmiero, G.; Cesaro, A.; Vetrano, E.; Pafundi, P.C.; Galiero, R.; Caturano, A.; Moscarella, E.; Gragnano, F.; Salvatore, T.; Rinaldi, L.; et al. Impact of SGLT2 Inhibitors on Heart Failure: From Pathophysiology to Clinical Effects. Int. J. Mol. Sci. 2021, 22, 5863. [Google Scholar] [CrossRef] [PubMed]
- Huerta-Delgado, A.S.; Roffe-Vazquez, D.N.; Luna-Ceron, E.; Gonzalez-Gil, A.M.; Casillas-Fikentscher, A.; Villarreal-Calderon, J.R.; Enriquez, C.; de la Peña-Almaguer, E.; Castillo, E.C.; Silva-Platas, C.; et al. Association of irisin levels with cardiac magnetic resonance, inflammatory, and biochemical parameters in patients with chronic heart failure versus controls. Magn. Reason. Imaging 2022, 93, 62–72. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).