
Effects of Different Capsulotomy and Fragmentation Energy Levels on the Generation of Oxidative Stress Following Femtosecond Laser-Assisted Cataract Surgery
 , , , and
, , , and
Abstract
:1. Introduction
2. Patients and Methods
2.1. Experimental Study
2.2. Clinical Study
2.3. Quantification of Aqueous Free Radicals
3. Statistical Analysis
4. Results
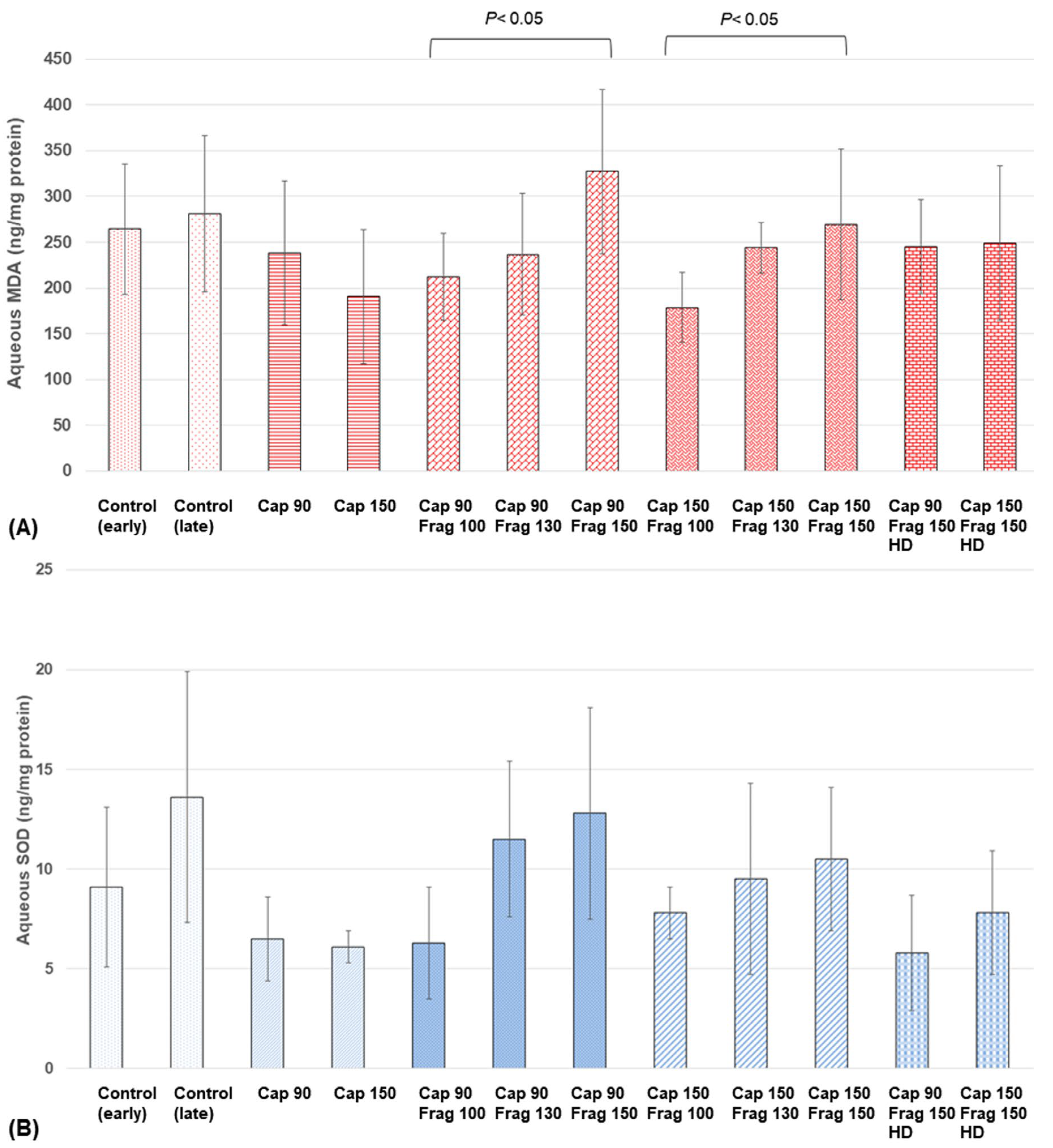
4.1. Experimental Study
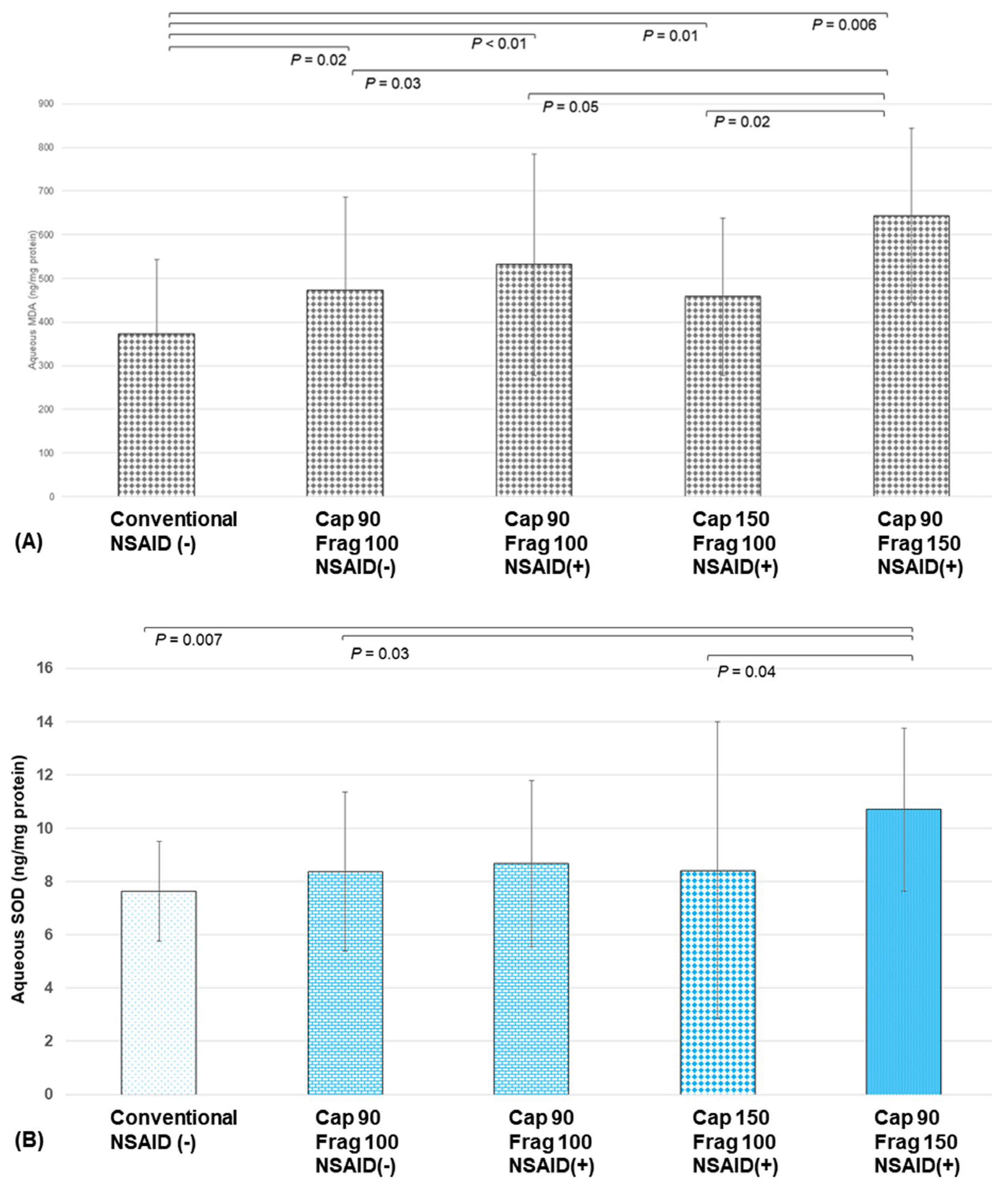
4.2. Clinical Study
5. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Liu, Y.C.; Wilkins, M.; Kim, T.; Malyugin, B.; Mehta, J.S. Cataracts. Lancet 2017, 390, 600–612. [Google Scholar] [CrossRef]
- Friedman, N.J.; Palanker, D.V.; Schuele, G.; Andersen, D.; Marcellino, G.; Seibel, B.S.; Batlle, J.; Feliz, R.; Talamo, J.H.; Blumenkranz, M.S.; et al. Femtosecond laser capsulotomy. J. Cataract. Refract. Surg. 2011, 37, 1189–1198. [Google Scholar] [CrossRef] [PubMed]
- Nagy, Z.Z.; Kranitz, K.; Takacs, A.I.; Miháltz, K.; Kovács, I.; Knorz, M.C. Comparison of intraocular lens decentration parameters after femtosecond and manual capsulotomies. J. Refract. Surg. 2011, 27, 564–569. [Google Scholar] [CrossRef] [PubMed]
- Palanker, D.V.; Blumenkranz, M.S.; Andersen, D.; Wiltberger, M.; Marcellino, G.; Gooding, P.; Angeley, D.; Schuele, G.; Woodley, B.; Simoneau, M.; et al. Femtosecond laser-assisted cataract surgery with integrated optical coherence tomography. Sci. Transl. Med. 2010, 2, 58ra85. [Google Scholar] [CrossRef] [PubMed]
- Berk, T.A.; Schlenker, M.B.; Campos-Moller, X.; Pereira, A.M.; Ahmed, I.I. Visual and Refractive Outcomes in Manual versus Femtosecond Laser-Assisted Cataract Surgery: A Single-Center Retrospective Cohort Analysis of 1838 Eyes. Ophthalmology 2018, 125, 1172–1180. [Google Scholar] [CrossRef]
- Roberts, T.V.; Lawless, M.; Chan, C.C.; Jacobs, M.; Ng, D.; Bali, S.J.; Hodge, C.; Sutton, G. Femtosecond laser cataract surgery: Technology and clinical practice. Clin. Exp. Ophthalmol. 2013, 41, 180–186. [Google Scholar] [CrossRef] [PubMed]
- Abell, R.G.; Kerr, N.M.; Vote, B.J. Femtosecond laser-assisted cataract surgery compared with conventional cataract surgery. Clin. Exp. Ophthalmol. 2013, 41, 455–462. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.C.; Setiawan, M.; Ang, M.; Yam, G.H.; Mehta, J.S. Changes in aqueous oxidative stress, prostaglandins, and cytokines: Comparisons of low-energy femtosecond laser-assisted cataract surgery versus conventional phacoemulsification. J. Cataract. Refract. Surg. 2019, 45, 196–203. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.C.; Morales-Wong, F.; Patil, M.; Han, S.B.; Lwin, N.C.; Teo, E.P.; Ang, H.P.; Yussof, N.Z.; Mehta, J.S. Femtosecond laser-assisted corneal transplantation with a low-energy, liquid-interface system. Sci. Rep. 2022, 12, 6959. [Google Scholar] [CrossRef]
- Williams, G.P.; Ang, H.P.; George, B.L.; Liu, Y.C.; Peh, G.; Izquierdo, L.; Tan, D.T.; Mehta, J.S. Comparison of intra-ocular pressure changes with liquid or flat applanation interfaces in a femtosecond laser platform. Sci. Rep. 2015, 5, 14742. [Google Scholar] [CrossRef]
- Stewart, S.; Liu, Y.C.; Setiawan, M.; Lin, M.T.; Lee, I.X.; Sim, N.; Htoon, H.M.; Ong, H.S.; Mehta, J.S. The Effects of High Energy Capsulotomy on Aqueous Cytokine Profiles and Pupil Size During Femtosecond Laser-Assisted Cataract Surgery. J. Refract. Surg. 2022, 38, 587–594. [Google Scholar] [CrossRef]
- Riau, A.K.; Liu, Y.C.; Lwin, N.C.; Ang, H.P.; Tan, N.Y.; Yam, G.H.; Tan, D.T.; Mehta, J.S. Comparative study of nJ- and μJ-energy level femtosecond lasers: Evaluation of flap adhesion strength, stromal bed quality, and tissue responses. Investig. Ophthalmol. Vis. Sci. 2014, 55, 3186–3194. [Google Scholar] [CrossRef]
- Hull, D.S.; Green, K.; Thomas, L.; Alderman, N. Hydrogen peroxide-mediated corneal endothelial damage. Induction by oxygen free radical. Investig. Ophthalmol. Vis. Sci. 1984, 25, 1246–1253. [Google Scholar]
- Masuda, Y.; Igarashi, T.; Oki, K.; Kobayashi, M.; Takahashi, H.; Nakano, T. Free radical production by femtosecond laser lens irradiation in porcine eyes. J. Cataract. Refract. Surg. 2019, 45, 1168–1171. [Google Scholar] [CrossRef] [PubMed]
- Walkenbach, R.J.; Boney, F.; Ye, G.S. Corneal function after storage in dexsol or optisol. Investig. Ophthalmol. Vis. Sci. 1992, 33, 2454–2458. [Google Scholar]
- Liu, Y.C.; Setiawan, M.; Chin, J.Y.; Wu, B.; Ong, H.S.; Lamoureux, E.; Mehta, J.S. Randomized Controlled Trial Comparing 1-Year Outcomes of Low-Energy Femtosecond Laser-Assisted Cataract Surgery versus Conventional Phacoemulsification. Front. Med. 2021, 8, 811093. [Google Scholar] [CrossRef]
- Ghanem, A.A.; Arafa, L.F.; El-Baz, A. Oxidative stress markers in patients with primary open-angle glaucoma. Curr. Eye Res. 2010, 35, 295–301. [Google Scholar] [CrossRef] [PubMed]
- Kulaksızoglu, S.; Karalezli, A. Aqueous Humour and Serum Levels of Nitric Oxide, Malondialdehyde and Total Antioxidant Status in Patients with Type 2 Diabetes with Proliferative Diabetic Retinopathy and Nondiabetic Senile Cataracts. Can. J. Diabetes 2016, 40, 115–119. [Google Scholar] [CrossRef] [PubMed]
- Majsterek, I.; Malinowska, K.; Stanczyk, M.; Kowalski, M.; Blaszczyk, J.; Kurowska, A.K.; Kaminska, A.; Szaflik, J.; Szaflik, J.P. Evaluation of oxidative stress markers in pathogenesis of primary open-angle glaucoma. Exp. Mol. Pathol. 2011, 90, 231–237. [Google Scholar] [CrossRef] [PubMed]
- Goyal, A.; Srivastava, A.; Sihota, R.; Kaur, J. Evaluation of oxidative stress markers in aqueous humor of primary open angle glaucoma and primary angle closure glaucoma patients. Curr. Eye Res. 2014, 39, 823–829. [Google Scholar] [CrossRef]
- Takahashi, H.; Sakamoto, A.; Takahashi, R.; Ohmura, T.; Shimmura, S.; Ohara, K. Free radicals in phacoemulsification and aspiration procedures. Arch. Ophthalmol. 2002, 120, 1348–1352. [Google Scholar] [CrossRef]
- Cameron, M.D.; Poyer, J.F.; Aust, S.D. Identification of free radicals produced during phacoemulsification. J. Cataract. Refract. Surg. 2001, 27, 463–470. [Google Scholar] [CrossRef]
- Takahashi, H. Free radical development in phacoemulsification cataract surgery. J. Nippon. Med. Sch. 2005, 72, 4–12. [Google Scholar] [CrossRef]
- Menapace, R.; Schartmüller, D.; Röggla, V.; Reiter, G.S.; Leydolt, C.; Schwarzenbacher, L. Ultrasound energy consumption and macular changes with manual and femtolaser-assisted high-fluidics cataract surgery: A prospective randomized comparison. Acta Ophthalmol. 2022, 100, e414–e422. [Google Scholar] [CrossRef]
- Mansoor, H.; Liu, Y.C.; Wong, Y.R.; Lwin, N.C.; Seah, X.Y.; Mehta, J.S. Evaluation of femtosecond laser-assisted anterior capsulotomy in the presence of ophthalmic viscoelastic devices (OVDs). Sci. Rep. 2020, 10, 21542. [Google Scholar] [CrossRef] [PubMed]
- Chung, H.S.; Lee, J.; Lee, H.; Kim, J.Y.; Tchah, H. Evaluation of the Optical Aspects of the Ophthalmic Viscosurgical Device During Femtosecond Laser-Assisted Cataract Surgery. Transl. Vis. Sci. Technol. 2022, 11, 2. [Google Scholar] [CrossRef] [PubMed]
- Wu, B.M.; Williams, G.P.; Tan, A.; Mehta, J.S. A Comparison of Different Operating Systems for Femtosecond Lasers in Cataract Surgery. J. Ophthalmol. 2015, 2015, 616478. [Google Scholar] [CrossRef] [PubMed]
- Schultz, T.; Joachim, S.C.; Stellbogen, M.; Dick, H.B. Prostaglandin release during femtosecond laser-assisted cataract surgery: Main inducer. J. Refract. Surg. 2015, 31, 78–81. [Google Scholar] [CrossRef]
- Chen, X.; Chen, K.; He, J.; Yao, K. Comparing the Curative Effects between Femtosecond Laser-Assisted Cataract Surgery and Conventional Phacoemulsification Surgery: A Meta-Analysis. PLoS ONE 2016, 11, e0152088. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Yu, Y.; Song, X.; Zhu, Y.; Wang, W.; Yao, K. Clinical outcomes of femtosecond laser-assisted cataract surgery versus conventional phacoemulsification surgery for hard nuclear cataracts. J. Cataract. Refract. Surg. 2017, 43, 486–491. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Group | Capsulotomy Energy | Fragmentation Energy |
|---|---|---|
| Control (early) | None | None |
| Control (late) | None | None |
| Cap 90 | Capsulotomy energy 90% | None |
| Cap 150 | Capsulotomy energy 150% | None |
| Cap 90, frag 100 | Capsulotomy energy 90% | Fragmentation energy 100% Standard laser spot density |
| Cap 90, frag 130 | Capsulotomy energy 90% | Fragmentation energy 130% Standard laser spot density |
| Cap 90, frag 150 | Capsulotomy energy 90% | Fragmentation energy 150% Standard laser spot density |
| Cap 150, frag 100 | Capsulotomy energy 150% | Fragmentation energy 100% Standard laser spot density |
| Cap 150, frag 130 | Capsulotomy energy 150% | Fragmentation energy 130% Standard laser spot density |
| Cap 150, frag 150 | Capsulotomy energy 150% | Fragmentation energy 150% Standard laser spot density |
| Cap 90, frag 150, high spot density (HD) | Capsulotomy energy 90% | Fragmentation energy 150% Higher laser spot density |
| Cap 150, frag 150, HD | Capsulotomy energy 150% | Fragmentation energy 150% Higher laser spot density |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Han, S.B.; Liu, Y.-C.; Setiawan, M.; Lee, I.X.Y.; Patil, M.; Ong, H.S.; Mehta, J.S. Effects of Different Capsulotomy and Fragmentation Energy Levels on the Generation of Oxidative Stress Following Femtosecond Laser-Assisted Cataract Surgery. Biomolecules 2024, 14, 318. https://doi.org/10.3390/biom14030318
Han SB, Liu Y-C, Setiawan M, Lee IXY, Patil M, Ong HS, Mehta JS. Effects of Different Capsulotomy and Fragmentation Energy Levels on the Generation of Oxidative Stress Following Femtosecond Laser-Assisted Cataract Surgery. Biomolecules. 2024; 14(3):318. https://doi.org/10.3390/biom14030318
Chicago/Turabian StyleHan, Sang Beom, Yu-Chi Liu, Melina Setiawan, Isabelle Xin Yu Lee, Moushmi Patil, Hon Shing Ong, and Jodhbir S. Mehta. 2024. "Effects of Different Capsulotomy and Fragmentation Energy Levels on the Generation of Oxidative Stress Following Femtosecond Laser-Assisted Cataract Surgery" Biomolecules 14, no. 3: 318. https://doi.org/10.3390/biom14030318