Trastuzumab Specific Epitope Evaluation as a Predictive and Prognostic Biomarker in Gastric Cancer Patients

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients and Samples
2.2. HER2 IHC and SISH
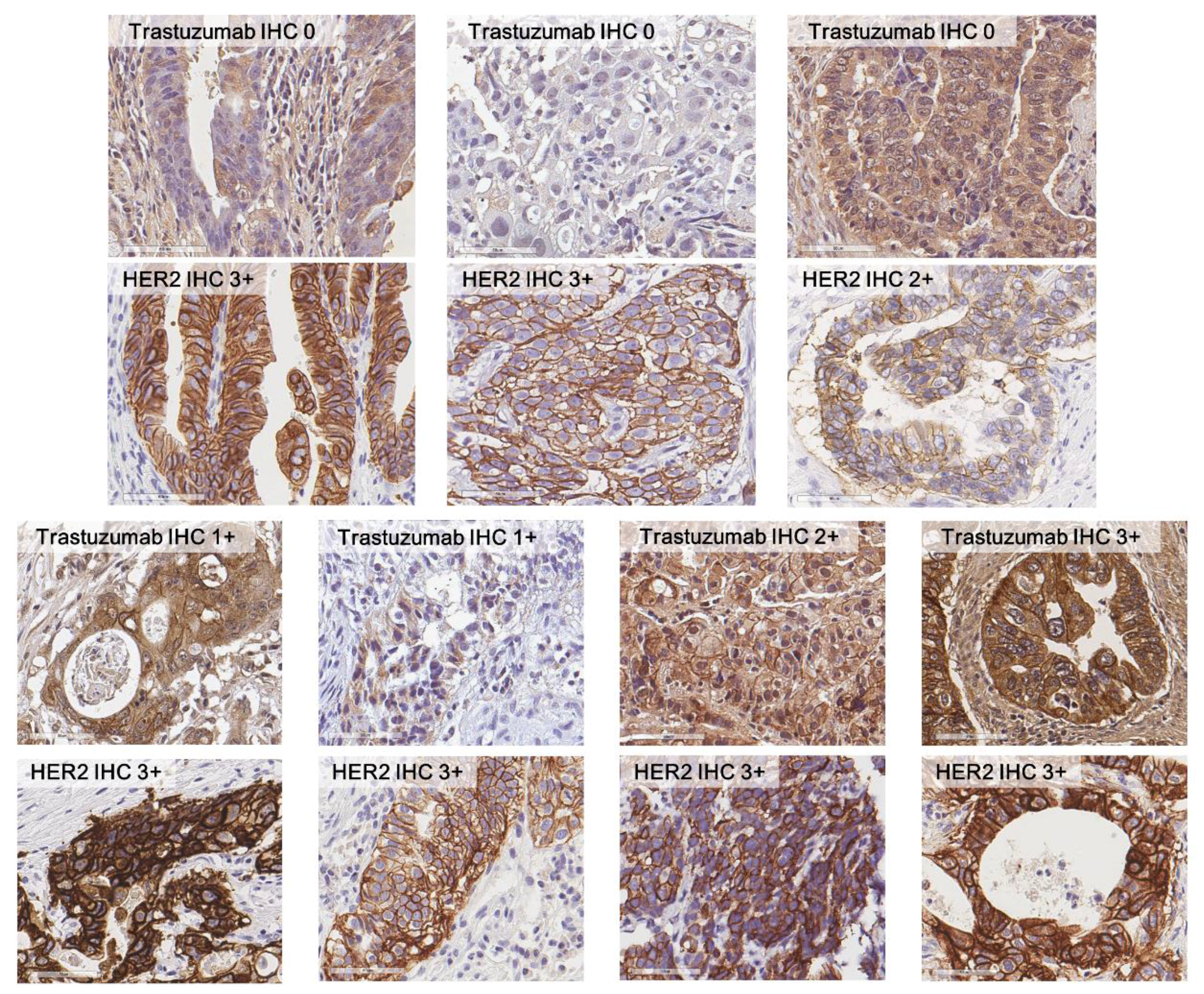
2.3. Trastuzumab IHC
2.4. Evaluation of HER2 and Trastuzumab IHC
2.5. Validation Using GC Cell Line
2.6. Statistical Analysis
3. Results
3.1. Clinicopathologjcal Characteristics of The Study Population
3.2. Comparison between HER2 IHC and Trastuzumab IHC
3.3. Survival Analysis According to Trastuzumab IHC
3.4. HER2 Assessments in 528 Consecutive GC Patients
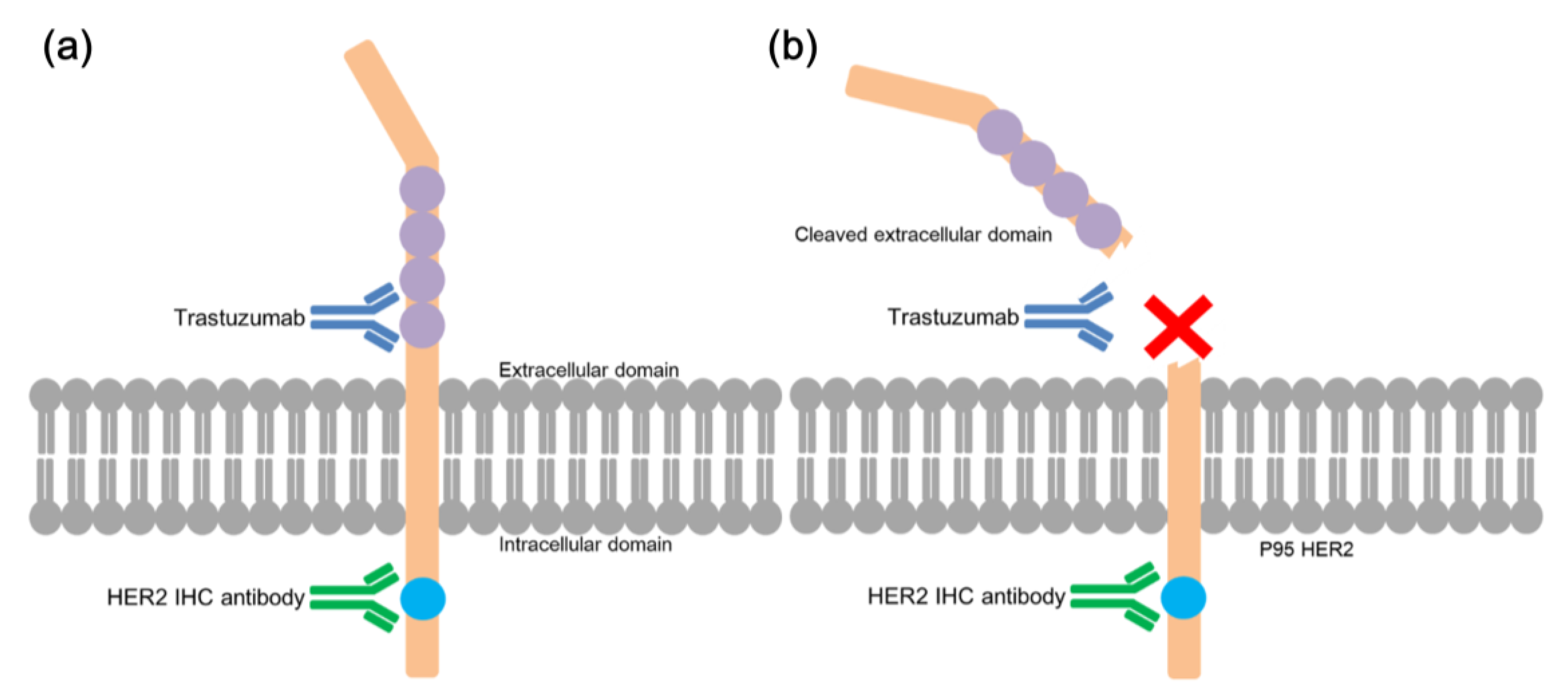
3.5. Validation of Different Epitopes for Each Antibody Using GC Cell Line
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Jemal, A.; Center, M.M.; DeSantis, C.; Ward, E.M. Global Patterns of Cancer Incidence and Mortality Rates and Trends. Cancer Epidemiol. Biomark. Prev. 2010, 19, 1893–1907. [Google Scholar] [CrossRef]
- Nashimoto, A.; Akazawa, K.; Isobe, Y.; Miyashiro, I.; Katai, H.; Kodera, Y.; Tsujitani, S.; Seto, Y.; Furukawa, H.; Oda, I.; et al. Gastric cancer treated in 2002 in Japan: 2009 annual report of the JGCA nationwide registry. Gastric Cancer 2012, 16, 1–27. [Google Scholar] [CrossRef]
- Digklia, A.; Wagner, A.D. Advanced gastric cancer: Current treatment landscape and future perspectives. World J. Gastroenterol. 2016, 22, 2403–2414. [Google Scholar] [CrossRef]
- Sanford, M. Trastuzumab: A Review of Its Use in HER2-Positive Advanced Gastric Cancer. Drugs 2013, 73, 1605–1615. [Google Scholar] [CrossRef]
- Choi, Y.Y.; Noh, S.H.; Cheong, J.-H. Molecular Dimensions of Gastric Cancer: Translational and Clinical Perspectives. J. Pathol. Transl. Med. 2016, 50, 1–9. [Google Scholar] [CrossRef]
- Slamon, D.J.; Leyland-Jones, B.; Shak, S.; Fuchs, H.; Paton, V.; Bajamonde, A.; Fleming, T.; Eiermann, W.; Wolter, J.; Pegram, M.; et al. Use of Chemotherapy plus a Monoclonal Antibody against HER2 for Metastatic Breast Cancer That Overexpresses HER2. New Engl. J. Med. 2001, 344, 783–792. [Google Scholar] [CrossRef]
- Kos, Z.; Dabbs, D.J. Biomarker assessment and molecular testing for prognostication in breast cancer. Histopathology 2015, 68, 70–85. [Google Scholar] [CrossRef]
- Kim, K.C.; Koh, Y.W.; Chang, H.-M.; Kim, T.H.; Yook, J.H.; Kim, B.S.; Jang, S.J.; Park, Y.S. Evaluation of HER2 Protein Expression in Gastric Carcinomas: Comparative Analysis of 1414 Cases of Whole-Tissue Sections and 595 Cases of Tissue Microarrays. Ann. Surg. Oncol. 2011, 18, 2833–2840. [Google Scholar] [CrossRef]
- Nakajima, M.; Sawada, H.; Yamada, Y.; Watanabe, A.; Tatsumi, M.; Yamashita, J.; Matsuda, M.; Sakaguchi, T.; Hirao, T.; Nakano, H. The prognostic significance of amplification and overexpression of c-met and c-erb B-2 in human gastric carcinomas. Cancer 1999, 85, 1894–1902. [Google Scholar] [CrossRef]
- Ock, C.-Y.; Kim, T.-Y.; Lee, K.-H.; Han, S.-W.; Im, S.-A.; Kim, T.-Y.; Bang, Y.-J.; Oh, D.-Y. Metabolic landscape of advanced gastric cancer according to HER2 and its prognostic implications. Gastric Cancer 2015, 19, 421–430. [Google Scholar] [CrossRef]
- Bang, Y.-J.; Van Cutsem, E.; Feyereislova, A.; Chung, H.C.; Shen, L.; Sawaki, A. Trastuzumab in combination with chemotherapy versus chemotherapy alone for treatment of HER2-positive advanced gastric or gastro-oesophageal junction cancer (ToGA): a phase 3, open-label, randomised controlled trial. Lancet 2010, 376, 687–697. [Google Scholar] [CrossRef]
- Shen, L.; Shan, Y.-S.; Hu, H.-M.; Price, T.J.; Sirohi, B.; Yeh, K.-H.; Yang, Y.-H.; Sano, T.; Yang, H.-K.; Zhang, X.; et al. Management of gastric cancer in Asia: resource-stratified guidelines. Lancet Oncol. 2013, 14, e535–e547. [Google Scholar] [CrossRef]
- Ock, C.-Y.; Lee, K.-W.; Kim, J.W.; Kim, J.-S.; Kim, T.-Y.; Lee, K.-H.; Han, S.-W.; Im, S.-A.; Kim, T.-Y.; Kim, W.H.; et al. Optimal Patient Selection for Trastuzumab Treatment in HER2-Positive Advanced Gastric Cancer. Clin. Cancer Res. 2015, 21, 2520–2529. [Google Scholar] [CrossRef]
- Koopman, T.; Louwen, M.; Hage, M.; Smits, M.M.; Imholz, A.L. Pathologic Diagnostics of HER2 Positivity in Gastroesophageal Adenocarcinoma. Am. J. Clin. Pathol. 2015, 143, 257–264. [Google Scholar] [CrossRef]
- Kang, J.; Yi, J.; Hwang, I.; Ahn, H.; Lee, S.; Won, Y.-W.; Ji, J.; Kim, H.; Rha, S.; Oh, S.; et al. P-057 * A retrospective analysis for patients with HER2 positive gastric cancer who were treated with trastuzumab-based chemotherapy. Ann. Oncol. 2015, 26. [Google Scholar] [CrossRef]
- Okines, A.F.; Cunningham, D. Trastuzumab: A novel standard option for patients with HER-2-positive advanced gastric or gastro-oesophageal junction cancer. Ther. Adv. Gastroenterol. 2012, 5, 301–318. [Google Scholar] [CrossRef]
- Gajria, D.; Chandarlapaty, S. HER2-amplified breast cancer: mechanisms of trastuzumab resistance and novel targeted therapies. Expert Rev. Anticancer. Ther. 2011, 11, 263–275. [Google Scholar] [CrossRef]
- Nahta, R. Insulin-like Growth Factor-I Receptor/Human Epidermal Growth Factor Receptor 2 Heterodimerization Contributes to Trastuzumab Resistance of Breast Cancer Cells. Cancer Res. 2005, 65, 11118–11128. [Google Scholar] [CrossRef]
- Wen, Y.-G.; Qiu, G.-Q.; Wang, Q.; Zhou, C.-Z.; Peng, Z.-H.; Tang, H.-M. Mutation analysis of tumor suppressor gene PTEN in patients with gastric carcinomas and its impact on PI3K/AKT pathway. Oncol. Rep. 2010, 24, 89–95. [Google Scholar]
- Lee, H.E.; Park, K.U.; Yoo, S.B.; Nam, S.K.; Park, D.J.; Kim, H.-H.; Lee, H.S. Clinical significance of intratumoral HER2 heterogeneity in gastric cancer. Eur. J. Cancer 2013, 49, 1448–1457. [Google Scholar] [CrossRef]
- Hudis, C.A. Trastuzumab—Mechanism of Action and Use in Clinical Practice. New Engl. J. Med. 2007, 357, 39–51. [Google Scholar] [CrossRef]
- Tse, C.; Gauchez, A.-S.; Jacot, W.; Lamy, P.-J. HER2 shedding and serum HER2 extracellular domain: Biology and clinical utility in breast cancer. Cancer Treat. Rev. 2012, 38, 133–142. [Google Scholar] [CrossRef]
- Price-Schiavi, S.A.; Jepson, S.; Li, P.; Arango, M.; Rudland, P.S.; Yee, L.; Carraway, K.L.; Price-Schiavi, S.A. Rat Muc4 (sialomucin complex) reduces binding of anti-ErbB2 antibodies to tumor cell surfaces, a potential mechanism for herceptin resistance. Int. J. Cancer 2002, 99, 783–791. [Google Scholar] [CrossRef]
- Hofmann, M.; Stoss, O.; Shi, D.; Büttner, R.; Van De Vijver, M.; Kim, W.; Ochiai, A.; Rüschoff, J.; Henkel, T. Assessment of a HER2 scoring system for gastric cancer: results from a validation study. Histopathology 2008, 52, 797–805. [Google Scholar] [CrossRef]
- Bates, S. Progress towards personalized medicine. Drug Discov. Today 2010, 15, 115–120. [Google Scholar] [CrossRef]
- Lenz, H.-J.; Van Cutsem, E.; Khambata-Ford, S.; Mayer, R.J.; Gold, P.; Stella, P.; Mirtsching, B.; Cohn, A.L.; Pippas, A.W.; Azarnia, N.; et al. Multicenter Phase II and Translational Study of Cetuximab in Metastatic Colorectal Carcinoma Refractory to Irinotecan, Oxaliplatin, and Fluoropyrimidines. J. Clin. Oncol. 2006, 24, 4914–4921. [Google Scholar] [CrossRef]
- Schrohl, A.-S.; Pedersen, H.C.; Jensen, S.S.; Nielsen, S.L.; Brünner, N. Human epidermal growth factor receptor 2 (HER2) immunoreactivity: specificity of three pharmacodiagnostic antibodies. Histopathology 2011, 59, 975–983. [Google Scholar] [CrossRef]
- Gravalos, C.; Jimeno, A. HER2 in gastric cancer: a new prognostic factor and a novel therapeutic target. Ann. Oncol. 2008, 19, 1523–1529. [Google Scholar] [CrossRef]
- Qiu, M.-Z.; Li, Q.; Wang, Z.-Q.; Liu, T.-S.; Liu, Q.; Wei, X.-L.; Jin, Y.; Wang, D.-S.; Ren, C.; Bai, L. HER2-positive patients receiving trastuzumab treatment have a comparable prognosis with HER2-negative advanced gastric cancer patients: A prospective cohort observation. Int. J. Cancer 2013, 134, 2468–2477. [Google Scholar] [CrossRef]
- Tateishi, M.; Toda, T.; Minamisono, Y.; Nagasaki, S. Clinicopathological significance of c-erbB-2 protein expression in human gastric carcinoma. J. Surg. Oncol. 1992, 49, 209–212. [Google Scholar] [CrossRef]
- Janjigian, Y.Y.; Werner, D.; Pauligk, C.; Steinmetz, K.; Kelsen, D.P.; Jäger, E.; Altmannsberger, H.-M.; Robinson, E.; Tafe, L.J.; Tang, L.H.; et al. Prognosis of metastatic gastric and gastroesophageal junction cancer by HER2 status: a European and USA International collaborative analysis. Ann. Oncol. 2012, 23, 2656–2662. [Google Scholar] [CrossRef]
- Fisher, S.B.; Fisher, K.E.; Squires, M.H.; Patel, S.H.; Kooby, D.A.; El-Rayes, B.F.; Cardona, K.; Russell, M.C.; Staley, C.A.; Farris, A.B.; et al. HER2 in resected gastric cancer: Is there prognostic value? J. Surg. Oncol. 2013, 109, 61–66. [Google Scholar] [CrossRef]
- Shitara, K.; Yatabe, Y.; Matsuo, K.; Sugano, M.; Kondo, C.; Takahari, D.; Ura, T.; Tajika, M.; Ito, S.; Muro, K. Prognosis of patients with advanced gastric cancer by HER2 status and trastuzumab treatment. Gastric Cancer 2012, 16, 261–267. [Google Scholar] [CrossRef] [Green Version]
- Bussolati, G.; Montemurro, F.; Righi, L.; Donadio, M.; Aglietta, M.; Sapino, A. A modified Trastuzumab antibody for the immunohistochemical detection of HER-2 overexpression in breast cancer. Br. J. Cancer 2005, 92, 1261–1267. [Google Scholar] [CrossRef] [Green Version]
- Dale, G.L.; Gaddy, P.; Pikul, F.J. Antibodies against biotinylated proteins are present in normal human serum. J. Lab. Clin. Med. 1994, 123, 365–371. [Google Scholar]
- Høyer-Hansen, G.; Hamers, M.J.; Pedersen, A.N.; Nielsen, H.J.; Brünner, N.; Danø, K.; Stephens, R.W. Loss of ELISA specificity due to biotinylation of monoclonal antibodies. J. Immunol. Methods 2000, 235, 91–99. [Google Scholar] [CrossRef]
- Glazyrin, A.; Shen, X.; Blanc, V.; Eliason, J.F. Direct Detection of Herceptin/Trastuzumab Binding on Breast Tissue Sections. J. Histochem. Cytochem. 2006, 55, 25–33. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| n (%) | |
|---|---|
| Age | |
| Median (range) | 63 (30–84) |
| Sex | |
| Male | 51 (73.9%) |
| Female | 18 (26.1%) |
| Specimen | |
| Biopsy | 18 (26.1%) |
| Surgical resection | 51 (73.9%) |
| Histology | |
| Intestinal | 49 (71.0%) |
| Diffuse | 15 (21.7%) |
| Mixed | 5 (7.2%) |
| Clinical stage (baseline) | |
| Early gastric cancer | 6 (8.7%) |
| Advanced gastric cancer | 63 (91.3%) |
| Metastasis (baseline) | |
| Absent | 34 (49.3%) |
| Present | 35 (50.7%) |
| HER2 IHC status | |
| 0 | 0 (0%) |
| 1+ | 2 (2.9%) a |
| 2+ | 19 (27.5%) |
| 3+ | 48 (69.6%) |
| Trastuzumab IHC status | |
| 0 | 32 (46.4%) |
| 1+ | 7 (10.1%) |
| 2+ | 5 (7.2%) |
| 3+ | 25 (36.2%) |
| PFS (months) | |
| Median (range) | 9.8 (0.1–147.4) |
| OS (months) | |
| Median (range) | 21.6 (0.1–147.4) |
| Total | 69 (100%) |
| Trastuzumab IHC | ||||||
|---|---|---|---|---|---|---|
| 0 | 1+ | 2+ | 3+ | Total | ||
| HER2 IHC | 0 | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) |
| 1+ | 2 (100%) | 0 (0%) | 0 (0%) | 0 (0%) | 2 (2.9%) | |
| 2+ | 15 (78.9%) | 3 (15.8%) | 0 (0%) | 1 (5.3%) | 19 (27.5%) | |
| 3+ | 15 (31.3%) | 4 (8.3%) | 5 (10.4%) | 24 (50.0%) | 48 (69.6%) | |
| Total | 32 (46.4%) | 7 (10.1%) | 5 (7.3%) | 25 (36.2%) | 69 (100.0%) | |
| Progression-Free Survival | Overall Survival | |||
|---|---|---|---|---|
| HR (95% CI) | p | HR (95% CI) | p | |
| Age | ||||
| <65 | 1.00 | 1.00 | ||
| ≥65 | 1.33 (0.78–2.28) | 0.291 | 1.62 (0.89–2.95) | 0.112 |
| Sex | ||||
| Male | 1.00 | 1.00 | ||
| Female | 1.12 (0.61–2.07) | 0.711 | 0.98 (0.50–1.95) | 0.964 |
| Histology | ||||
| Intestinal | 1.00 | 1.00 | ||
| Diffuse | 1.02 (0.52–2.00) | 1.18 (0.57–2.41) | ||
| Mixed | 1.79 (0.70–4.57) | 0.475 | 1.72 (0.60–4.90) | 0.576 |
| Clinical stage | ||||
| EGC | 1.00 | 1.00 | ||
| AGC | 1.62 (0.51–5.22) | 0.413 | 2.40 (0.58–9.94) | 0.226 |
| HER2 IHC | ||||
| <2+ | 1.00 | 1.00 | ||
| ≥2+ | 0.53 (0.13–2.21) | 0.383 | 0.79 (0.19–3.29) | 0.749 |
| HER2 IHC | ||||
| 1+, 2+ | 1.00 | 1.00 | ||
| 3+ | 0.23 (0.13–0.44) | < 0.001 | 0.29 (0.15–0.55) | <0.001 |
| Trastuzumab IHC | ||||
| <2+ | 1.00 | 1.00 | ||
| ≥2+ | 0.51 (0.30–0.88) | 0.016 | 0.47 (0.25–0.87) | 0.016 |
| Metastasis | ||||
| No | 1.00 | 1.00 | ||
| Yes | 1.79 (1.03–3.11) | 0.038 | 1.52 (0.83–2.79) | 0.180 |
| HER2 Negative | HER2 Positive | p-Value | |
|---|---|---|---|
| Age | |||
| <65 | 306 (61.0%) | 13 (50.0%) | 0.265 |
| ≥65 | 196 (39.0%) | 13 (50.0%) | |
| Sex | |||
| Male | 334 (66.5%) | 18 (69.2%) | 0.776 |
| Female | 168 (33.5%) | 8 (30.8%) | |
| Location | |||
| Lower | 256 (51.0%) | 15 (57.7%) | 0.444 |
| Middle | 153 (30.5%) | 7 (26.9%) | |
| Upper | 78 (15.5%) | 4 (15.4%) | |
| Entire | 15 (3.0%) | 0 (0.0%) | |
| Histology | |||
| WD | 57 (11.4%) | 11 (42.3%) | <0.001 |
| MD | 163 (32.5%) | 14 (53.8%) | |
| PD | 193 (38.4%) | 1 (3.8%) | |
| SRC | 74 (14.7%) | 0 (0.0%) | |
| Mucinous | 15 (3.0%) | 0 (0.0%) | |
| Lauren classification | |||
| Intestinal | 211 (42.0%) | 25 (96.2%) | <0.001 |
| Diffuse | 241 (48.0%) | 1 (3.8%) | |
| Mixed | 50 (10.0%) | 0 (0.0%) | |
| Lymphatic invasion | |||
| Absent | 260 (51.8%) | 15 (57.7%) | 0.557 |
| Present | 242 (48.2%) | 11 (42.3%) | |
| Vascular invasion | |||
| Absent | 445 (88.8%) | 24 (92.3%) | 0.756 |
| Present | 56 (11.2%) | 2 (7.7%) | |
| Perineural invasion | |||
| Absent | 329 (65.5%) | 23 (88.5%) | 0.017 |
| Present | 173 (34.5%) | 3 (11.5%) | |
| pTNM stage | |||
| I | 261 (52.0%) | 17 (65.4%) | 0.167 |
| II | 79 (15.7%) | 4 (15.4%) | |
| III | 139 (27.7%) | 4 (15.4%) | |
| IV | 23 (4.6%) | 1 (3.8%) | |
| Total | 502 (95.1%) | 26 (4.9%) | |
| DFS | OS | |||||||
|---|---|---|---|---|---|---|---|---|
| Univariate | Multivariate | Univariate | Multivariate | |||||
| HR (95% CI) | p | HR (95% CI) | p | HR (95% CI) | p | HR (95% CI) | p | |
| Age | ||||||||
| <65 | 1.00 | - | 1.00 | 1.00 | ||||
| ≥65 | 1.31 (0.92–1.86) | 0.139 | - | - | 2.43 (1.83–3.22) | <0.001 | 2.90 (2.18–3.87) | <0.001 |
| Sex | ||||||||
| Male | 1.00 | - | 1.00 | 1.00 | ||||
| Female | 0.79 (0.54–1.16) | 0.230 | - | - | 0.66 (0.48–0.91) | 0.010 | 0.74 (0.53–1.01) | 0.060 |
| Lymphatic invasion | ||||||||
| Absent | 1.00 | 1.00 | 1.00 | 1.00 | ||||
| Present | 9.24 (5.46–15.62) | <0.001 | 2.23 (1.23–4.03) | 0.008 | 30.07 (2.27–4.14) | <0.001 | 1.40 (0.97–2.03) | 0.076 |
| Perineural invasion | ||||||||
| Absent | 1.00 | 1.00 | 1.00 | 1.00 | ||||
| Present | 7.73 (5.16–11.58) | <0.001 | 1.45 (0.91–2.30) | 0.121 | 3.74 (2.82–4.96) | <0.001 | 1.43 (0.99–2.08) | 0.060 |
| Vascular invasion | ||||||||
| Absent | 1.00 | 1.00 | 1.00 | 1.00 | ||||
| Present | 6.49 (4.45–9.45) | <0.001 | 1.81 (1.23–2.66) | 0.003 | 4.95 (3.55–6.90) | <0.001 | 2.11 (1.47–3.03) | <0.001 |
| HER2 IHC | ||||||||
| <2+ | 1.00 | - | 1.00 | - | ||||
| ≥2+ | 0.94 (0.49–1.80) | 0.852 | - | - | 0.90 (0.54–1.51) | 0.697 | - | - |
| HER2 SISH | ||||||||
| Non-ampl | 1.00 | - | 1.00 | - | ||||
| Ampl | 0.97 (0.71–1.32) | 0.845 | - | - | 1.02 (0.61–1.70) | 0.934 | - | - |
| Trastuzumab IHC | ||||||||
| <2+ | 1.00 | 1.00 | 1.00 | 1.00 | ||||
| ≥2+ | 2.80 (1.31–6.01) | 0.008 | 1.81 (0.84–3.90) | 0.132 | 2.19 (1.08–4.44) | 0.031 | 1.68 (0.82–3.42) | 0.155 |
| Overall HER2 status | ||||||||
| Negative | 1.00 | - | 1.00 | - | ||||
| Positive | 0.94 (0.42–2.15) | 0.891 | - | - | 0.97 (0.51–1.83) | 0.926 | - | - |
| Stage | ||||||||
| I, II | 1.00 | 1.00 | 1.00 | 1.00 | ||||
| III, IV | 19.27 (11.66–31.85) | <0.001 | 8.58 (4.59–16.04) | <0.001 | 4.96 (3.73–6.60) | <0.001 | 3.11 (2.06–4.68) | <0.001 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Koh, J.; Nam, S.K.; Lee, Y.W.; Kim, J.W.; Lee, K.-W.; Ock, C.-Y.; Oh, D.-Y.; Ahn, S.-H.; Kim, H.-H.; Kang, K.-W.; et al. Trastuzumab Specific Epitope Evaluation as a Predictive and Prognostic Biomarker in Gastric Cancer Patients. Biomolecules 2019, 9, 782. https://doi.org/10.3390/biom9120782
Koh J, Nam SK, Lee YW, Kim JW, Lee K-W, Ock C-Y, Oh D-Y, Ahn S-H, Kim H-H, Kang K-W, et al. Trastuzumab Specific Epitope Evaluation as a Predictive and Prognostic Biomarker in Gastric Cancer Patients. Biomolecules. 2019; 9(12):782. https://doi.org/10.3390/biom9120782
Chicago/Turabian StyleKoh, Jiwon, Soo Kyung Nam, Youn Woo Lee, Jin Won Kim, Keun-Wook Lee, Chan-Young Ock, Do-Youn Oh, Sang-Hoon Ahn, Hyung-Ho Kim, Keon-Wook Kang, and et al. 2019. "Trastuzumab Specific Epitope Evaluation as a Predictive and Prognostic Biomarker in Gastric Cancer Patients" Biomolecules 9, no. 12: 782. https://doi.org/10.3390/biom9120782