
Exploring Equity in Healthcare Services: Spatial Accessibility Changes during Subway Expansion


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Area
2.2. Data Sources and Preprocessing
2.3. Methodology
2.3.1. Supply and Demand of Subdistricts for Healthcare Services
2.3.2. Accessibility of Population Residential Location to Healthcare Services
2.3.3. Equity Evaluation
3. Results
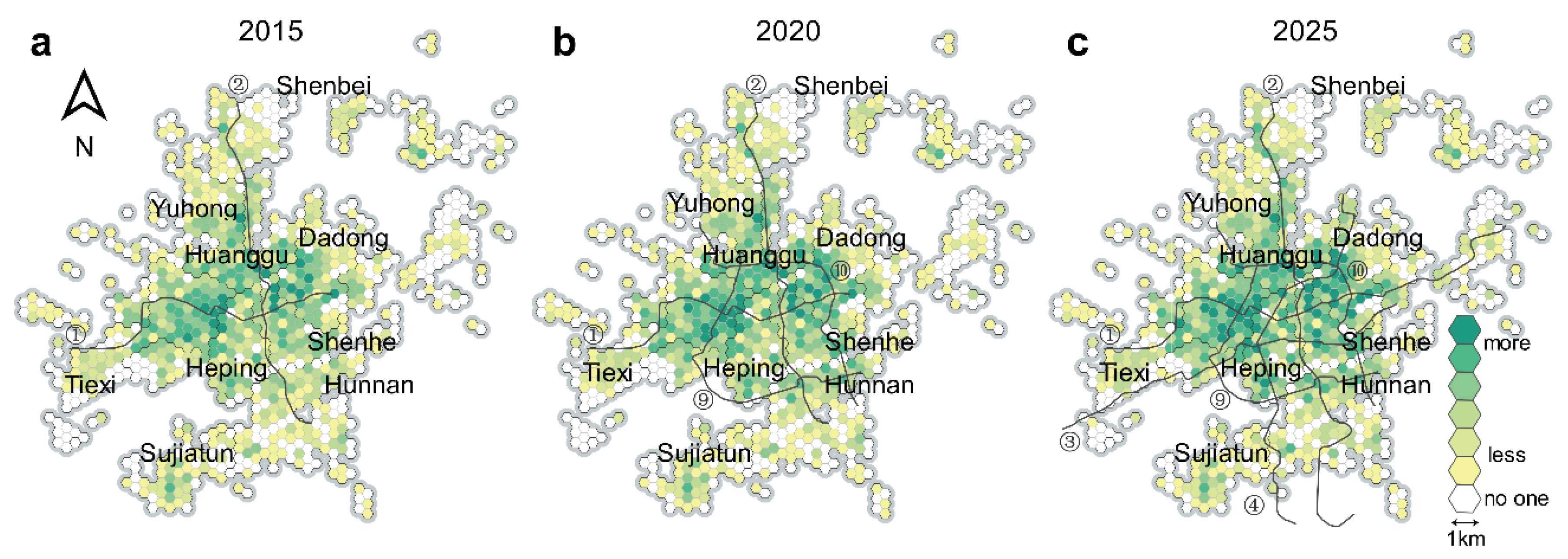
3.1. Spatial Distribution Characteristics of Healthcare Supply and Demand
3.2. Accessibility across the Central Urban Area after Introducing Subways
3.2.1. Quantity Accessibility
3.2.2. Quality Accessibility
3.2.3. Walking Accessibility
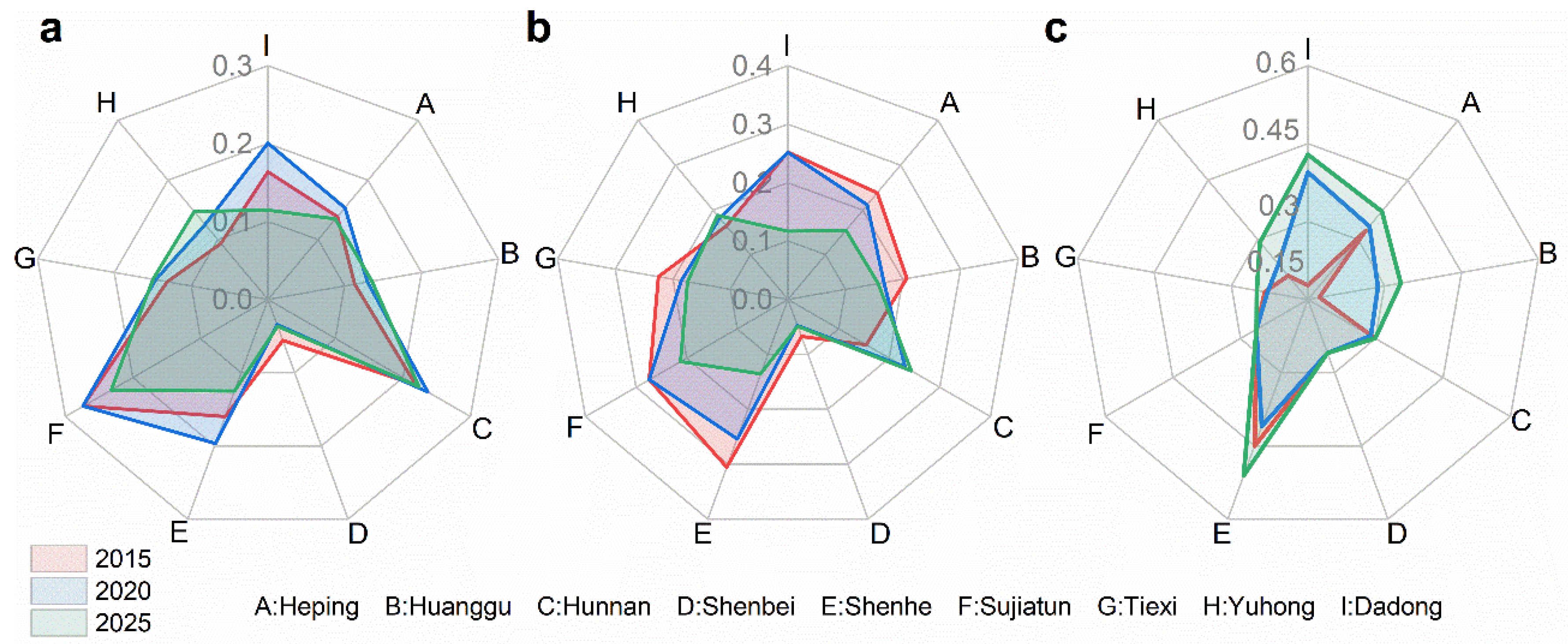
3.3. Equity Changes with Subway Line Extensions
3.3.1. Equity between Subdistricts
3.3.2. Equity between Districts
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rekha, R.S.; Wajid, S.; Radhakrishnan, N.; Mathew, S. Accessibility Analysis of Health care facility using Geospatial Techniques. Transp. Res. Procedia 2017, 27, 1163–1170. [Google Scholar] [CrossRef]
- Sanchez, T.W. Equity Analysis of Personal Transportation System Benefits. J. Urban Aff. 1998, 20, 69–86. [Google Scholar] [CrossRef]
- Borrell, L.N.; Talih, M. A symmetrized Theil index measure of health disparities: An example using dental caries in U.S. children and adolescents. Stat. Med. 2011, 30, 277–290. [Google Scholar] [CrossRef] [Green Version]
- Kain, J.F.; Meyer, J.R. Transportation and Poverty. The 100; ERIC: Online, 1970. [Google Scholar]
- Sun, Z.; Zacharias, J. Transport equity as relative accessibility in a megacity: Beijing. Transp. Policy 2020, 92, 8–19. [Google Scholar] [CrossRef]
- Mouter, N.; van Cranenburgh, S.; van Wee, B. An empirical assessment of Dutch citizens’ preferences for spatial equality in the context of a national transport investment plan. J. Transp. Geogr. 2017, 60, 217–230. [Google Scholar] [CrossRef] [Green Version]
- Pereira, R.H. Future accessibility impacts of transport policy scenarios: Equity and sensitivity to travel time thresholds for Bus Rapid Transit expansion in Rio de Janeiro. J. Transp. Geogr. 2019, 74, 321–332. [Google Scholar] [CrossRef] [Green Version]
- Rong, P.; Zheng, Z.; Kwan, M.-P.; Qin, Y. Evaluation of the spatial equity of medical facilities based on improved potential model and map service API: A case study in Zhengzhou, China. Appl. Geogr. 2020, 119, 102192. [Google Scholar] [CrossRef]
- Wang, C.-H.; Chen, N. A geographically weighted regression approach to investigating the spatially varied built-environment effects on community opportunity. J. Transp. Geogr. 2017, 62, 136–147. [Google Scholar] [CrossRef]
- Shin, K.; Lee, T. Improving the measurement of the Korean emergency medical System’s spatial accessibility. Appl. Geogr. 2018, 100, 30–38. [Google Scholar] [CrossRef]
- Siegel, M.; Koller, D.; Vogt, V.; Sundmacher, L. Developing a composite index of spatial accessibility across different health care sectors: A German example. Health Policy 2016, 120, 205–212. [Google Scholar] [CrossRef]
- Foster, A.; Dunham, I.M. Volunteered geographic information, urban forests, & environmental justice. Comput. Environ. Urban Syst. 2015, 53, 65–75. [Google Scholar] [CrossRef]
- Schultz, C.L.; Stanis, S.A.W.; Sayers, S.P.; Thombs, L.A.; Thomas, I.M. A longitudinal examination of improved access on park use and physical activity in a low-income and majority African American neighborhood park. Prev. Med. 2017, 95, S95–S100. [Google Scholar] [CrossRef]
- El-Geneidy, A.; Levinson, D.; Diab, E.; Boisjoly, G.; Verbich, D.; Loong, C. The cost of equity: Assessing transit accessibility and social disparity using total travel cost. Transp. Res. Part A Policy Pract. 2016, 91, 302–316. [Google Scholar] [CrossRef] [Green Version]
- Foth, N.; Manaugh, K.; El-Geneidy, A.M. Towards equitable transit: Examining transit accessibility and social need in Toronto, Canada, 1996–2006. J. Transp. Geogr. 2013, 29, 1–10. [Google Scholar] [CrossRef]
- Wee, G.; Geurs, K. Discussing Equity and Social Exclusion in Accessibility Evaluations. Eur. J. Transp. Infrastruct. Res. 2011, 11. [Google Scholar] [CrossRef]
- Deboosere, R.; El-Geneidy, A. Evaluating equity and accessibility to jobs by public transport across Canada. J. Transp. Geogr. 2018, 73, 54–63. [Google Scholar] [CrossRef]
- Hansen, W.G. How Accessibility Shapes Land Use. J. Am. Inst. Planners 1959, 25, 73–76. [Google Scholar] [CrossRef]
- Luo, W.; Wang, F. Measures of Spatial Accessibility to Health Care in a GIS Environment: Synthesis and a Case Study in the Chicago Region. Environ. Plan. B Plan. Des. 2003, 30, 865–884. [Google Scholar] [CrossRef] [Green Version]
- Shen, Q. Location characteristics of inner-city neighborhoods and employment accessibility of low-wage workers. Environ. Plan. B Plan. Des. 1998, 25, 345–365. [Google Scholar] [CrossRef]
- Curtis, C.; Scheurer, J. Planning for sustainable accessibility: Developing tools to aid discussion and decision-making. Prog. Plan. 2010, 74, 53–106. [Google Scholar] [CrossRef]
- Geurs, K.T.; van Eck, J.R. Accessibility measures: Review and applications. In Evaluation of Accessibility Impacts of Land-Use Transportation Scenarios, and Related Social and Economic Impact; RIVM: Bilthoven, The Netherlands, 2011. [Google Scholar]
- Kwan, M.-P.; Murray, A.T.; O’Kelly, M.E.; Tiefelsdorf, M. Recent advances in accessibility research: Representation, methodology and applications. J. Geogr. Syst. 2003, 5, 129–138. [Google Scholar] [CrossRef]
- Neutens, T. Accessibility, equity and health care: Review and research directions for transport geographers. J. Transp. Geogr. 2015, 43, 14–27. [Google Scholar] [CrossRef]
- Xia, N.; Cheng, L.; Chen, S.; Wei, X.; Zong, W.; Li, M. Accessibility based on Gravity-Radiation model and Google Maps API: A case study in Australia. J. Transp. Geogr. 2018, 72, 178–190. [Google Scholar] [CrossRef]
- Niedzielski, M.A.; Kucharski, R. Impact of commuting, time budgets, and activity durations on modal disparity in accessibility to supermarkets. Transp. Res. Part D Transp. Environ. 2019, 75, 106–120. [Google Scholar] [CrossRef]
- Widener, M.J.; Farber, S.; Neutens, T.; Horner, M. Spatiotemporal accessibility to supermarkets using public transit: An interaction potential approach in Cincinnati, Ohio. J. Transp. Geogr. 2015, 42, 72–83. [Google Scholar] [CrossRef] [Green Version]
- Herskovic, L. The Effect of Subway Access on School Choice. Econ. Educ. Rev. 2020, 78, 102021. [Google Scholar] [CrossRef]
- Islam, M.S.; Asktar, S. Measuring physical accessiblity to health facilities: A case study on Khunla City. World Health Popul. 2011, 12, 123–127. [Google Scholar] [CrossRef]
- Perry, B.; Gesler, W. Physical access to primary health care in Andean Bolivia. Soc. Sci. Med. 2000, 50, 1177–1188. [Google Scholar] [CrossRef]
- Dai, D. Black residential segregation, disparities in spatial access to health care facilities, and late-stage breast cancer diagnosis in metropolitan Detroit. Health Place 2010, 16, 1038–1052. [Google Scholar] [CrossRef] [PubMed]
- Hiscock, R.; Pearce, J.; Blakely, T.; Witten, K. Is Neighborhood Access to Health Care Provision Associated with Individual-Level Utilization and Satisfaction? Health Serv. Res. 2008, 43, 2183–2200. [Google Scholar] [CrossRef] [Green Version]
- Wan, N.; Zhan, F.B.; Zou, B.; Wilson, J.G. Spatial Access to Health Care Services and Disparities in Colorectal Cancer Stage at Diagnosis in Texas. Prof. Geogr. 2013, 65, 527–541. [Google Scholar] [CrossRef]
- McGrail, M.R.; Humphreys, J.S. Measuring spatial accessibility to primary health care services: Utilising dynamic catchment sizes. Appl. Geogr. 2014, 54, 182–188. [Google Scholar] [CrossRef]
- Wang, F. Measurement, Optimization, and Impact of Health Care Accessibility: A Methodological Review. Ann. Assoc. Am. Geogr. 2012, 102, 1104–1112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mansour, S. Spatial analysis of public health facilities in Riyadh Governorate, Saudi Arabia: A GIS-based study to assess geographic variations of service provision and accessibility. Geo-Spat. Inf. Sci. 2016, 19, 26–38. [Google Scholar] [CrossRef]
- Chang, H.-T.; Lai, H.-Y.; Hwang, I.-H.; Ho, M.-M.; Hwang, S.-J. Home healthcare services in Taiwan: A nationwide study among the older population. BMC Health Serv. Res. 2010, 10, 274. [Google Scholar] [CrossRef] [Green Version]
- Wang, Y.; Cao, M.; Liu, Y.; Ye, R.; Gao, X.; Ma, L. Public transport equity in Shenyang: Using structural equation modelling. Res. Transp. Bus. Manag. 2020, 100555. [Google Scholar] [CrossRef]
- Chen, G.; Wang, C.C.; Jin, P.; Xia, B.; Xiao, L.; Chen, S.; Luo, J. Evaluation of healthcare inequity for older adults: A spatio-temporal perspective. J. Transp. Health 2020, 19, 100911. [Google Scholar] [CrossRef]
- Boisjoly, G.; Deboosere, R.; Wasfi, R.; Orpana, H.; Manaugh, K.; Buliung, R.; El-Geneidy, A. Measuring accessibility to hospitals by public transport: An assessment of eight Canadian metropolitan regions. J. Transp. Health 2020, 18, 100916. [Google Scholar] [CrossRef]
- Rao, Y.; Lin, G. Rationality of the Geographical Distributio of Urban Education Resources from the Perspective of Balancing Supply and Demand: A Case Study of Wuhan City. J. South-Central Univ. Natl. Soc. Sci. 2021, 41, 147–152. (In Chinese) [Google Scholar]
- Giuliano, G.; Kang, S. Spatial dynamics of the logistics industry: Evidence from California. J. Transp. Geogr. 2018, 66, 248–258. [Google Scholar] [CrossRef]
- Hickman, R. Cultural perspectives on transport, urban planning and design. J. Transp. Geogr. 2017, 63, 50–52. [Google Scholar] [CrossRef]
- Sukaryavichute, E.; Prytherch, D.L. Transit planning, access, and justice: Evolving visions of bus rapid transit and the Chicago street. J. Transp. Geogr. 2018, 69, 58–72. [Google Scholar] [CrossRef]
- Duan, M.; Hang, Z.; Long, L.; Ou, R. The evaluation of allocation fairness to urban transit system service to elderly in mountainous city. J. Geo-inf. Sci. 2021, 23, 617–631. (In Chinese) [Google Scholar] [CrossRef]
- Jiang, H.; Zhang, W.; Wei, S. Public service facility accessibility as influenced by public transportation in Beijing. Prog. Geogr. 2017, 36, 1239–1249. (In Chinese) [Google Scholar] [CrossRef] [Green Version]
- Luo, X.; Yue, B.; Lin, A. The research of accessibility and fairness of pension service facilities based on multiple modes of transportation-a case study of Wuhan. J. Cent. China Norm. Univ. Sci. 2018, 52, 883–893. (In Chinese) [Google Scholar]
- Li, M.; Long, Y. The Coverage Ratio of Bus Stations and an Evaluation of Spatial Patterns of Major Chinese Cities. Urban Plan. Forum 2015, 6, 30–37. (In Chinese) [Google Scholar]
- Chen, B.Y.; Cheng, X.-P.; Kwan, M.-P.; Schwanen, T. Evaluating spatial accessibility to healthcare services under travel time uncertainty: A reliability-based floating catchment area approach. J. Transp. Geogr. 2020, 87, 102794. [Google Scholar] [CrossRef]
- Luo, J.; Chen, G.; Li, C.; Xia, B.; Sun, X.; Chen, S. Use of an E2SFCA Method to Measure and Analyse Spatial Accessibility to Medical Services for Elderly People in Wuhan, China. Int. J. Environ. Res. Public Health 2018, 15, 1503. [Google Scholar] [CrossRef] [Green Version]
- Hess, D.B. Walking to the bus: Perceived versus actual walking distance to bus stops for older adults. Transportation 2011, 39, 247–266. [Google Scholar] [CrossRef]
- Kang, J.-Y.; Michels, A.; Lyu, F.; Wang, S.; Agbodo, N.; Freeman, V.L.; Wang, S. Rapidly measuring spatial accessibility of COVID-19 healthcare resources: A case study of Illinois, USA. Int. J. Health Geogr. 2020, 19, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Jue, W.; Mei-Po, K. Hexagon-Based Adaptive Crystal Growth Voronoi Diagrams Based on Weighted Planes for Service Area Delimitation. Isprs Int. J. Geo. Inf. 2018, 7, 257. [Google Scholar]
- Caggiani, L.; Colovic, A.; Ottomanelli, M. An equality-based model for bike-sharing stations location in bicycle-public transport multimodal mobility. Transp. Res. Part A Policy Pract. 2020, 140, 251–265. [Google Scholar] [CrossRef]
- Theil, H. Economics and Information Theory; North-Holland: Amsterdam, The Netherlands, 1967. [Google Scholar]
- Liu, X.; Macedo, J.; Zhou, T.; Shen, L.; Liao, Y.; Zhou, Y. Evaluation of the utility efficiency of subway stations based on spatial information from public social media. Habitat Int. 2018, 79, 10–17. [Google Scholar] [CrossRef]
- Wang, Y.; Li, Y.; Qin, S.; Kong, Y.; Yu, X.; Guo, K.; Meng, J. The disequilibrium in the distribution of the primary health workforce among eight economic regions and between rural and urban areas in China. Int. J. Equity Health 2020, 19, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yin, C.; He, Q.; Liu, Y.; Chen, W.; Gao, Y. Inequality of public health and its role in spatial accessibility to medical facilities in China. Appl. Geogr. 2018, 92, 50–62. [Google Scholar] [CrossRef]
- Ahn, K.; Jang, H.; Song, Y. Economic impacts of being close to subway networks: A case study of Korean metropolitan areas. Res. Transp. Econ. 2020, 83, 100900. [Google Scholar] [CrossRef]
- Zhou, Q.; Dai, D.; Wang, Y.; Fan, J. Decade-Long Changes in Disparity and Distribution of Transit Opportunity in Shenzhen China: A Transportation Equity Perspective. J. Adv. Transp. 2018, 1–16. [Google Scholar] [CrossRef] [Green Version]
- Qian, T.; Chen, J.; Li, A.; Ang, L.; Shen, D. Evaluating Spatial Accessibility to General Hospitals with Navigation and Social Media Location Data: A Case Study in Nanjing. Int. J. Environ. Res. Public Health 2020, 17, 2752. [Google Scholar] [CrossRef]
- Yohan, F.; Delphine, P.; Béatrice, F.; Isabelle, R.-C.; Jean-Yves, B.; Françoise, D.; Guy, F.; Elodie, F. Beyond the map: Evidencing the spatial dimension of health inequalities. Int. J. Health Geogr 2020, 19, 46. [Google Scholar]
- Subal, J.; Paal, P.; Krisp, J.M. Quantifying spatial accessibility of general practitioners by applying a modified huff three-step floating catchment area (MH3SFCA) method. Int. J. Health Geogr. 2021, 20, 1–14. [Google Scholar] [CrossRef]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| District | Tax Value (10,000) | Number of the Elderly (10,000) | Number of Arrivals (10,000) | Mortality Rate (‰) | Vulnerability Index |
|---|---|---|---|---|---|
| Heping | 77,092 | 17.93 | 2.03 | 8.33 | 146.70 |
| Shenhe | 67,900 | 20.31 | 1.11 | 9.37 | 169.10 |
| Dadong | 29,083 | 18.97 | 0.74 | 10.34 | 129.84 |
| Huanggu | 27,022 | 21.72 | 1.65 | 8.97 | 197.85 |
| Tiexi | 44,552 | 25.15 | 1.74 | 9.82 | 269.21 |
| Sujiatun | 12,872 | 11.10 | 0.36 | 9.42 | 19.57 |
| Hunnan | 35,597 | 7.66 | 2.37 | 6.42 | 116.46 |
| Yuhong | 8498 | 10.21 | 2.25 | 7.93 | 90.50 |
| Shenbei | 9093 | 7.83 | 0.81 | 9.04 | 41.37 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liu, M.; Luo, S.; Du, X. Exploring Equity in Healthcare Services: Spatial Accessibility Changes during Subway Expansion. ISPRS Int. J. Geo-Inf. 2021, 10, 439. https://doi.org/10.3390/ijgi10070439
Liu M, Luo S, Du X. Exploring Equity in Healthcare Services: Spatial Accessibility Changes during Subway Expansion. ISPRS International Journal of Geo-Information. 2021; 10(7):439. https://doi.org/10.3390/ijgi10070439
Chicago/Turabian StyleLiu, Maohua, Siqi Luo, and Xishihui Du. 2021. "Exploring Equity in Healthcare Services: Spatial Accessibility Changes during Subway Expansion" ISPRS International Journal of Geo-Information 10, no. 7: 439. https://doi.org/10.3390/ijgi10070439
APA StyleLiu, M., Luo, S., & Du, X. (2021). Exploring Equity in Healthcare Services: Spatial Accessibility Changes during Subway Expansion. ISPRS International Journal of Geo-Information, 10(7), 439. https://doi.org/10.3390/ijgi10070439