

A Maximal Multimodal Accessibility Equality Model to Optimize the Equality of Healthcare Services

Abstract
:1. Introduction
2. Literature Review
2.1. Equality of Healthcare Accessibility
2.2. Accessibility Measures Considering Multiple Transport Modes
2.3. Models for the Optimization of the Equality of Accessibility
3. Materials and Methods
3.1. Measuring Multimodal Accessibility
3.2. The Maximal Multimodal Accessibility Equality Model
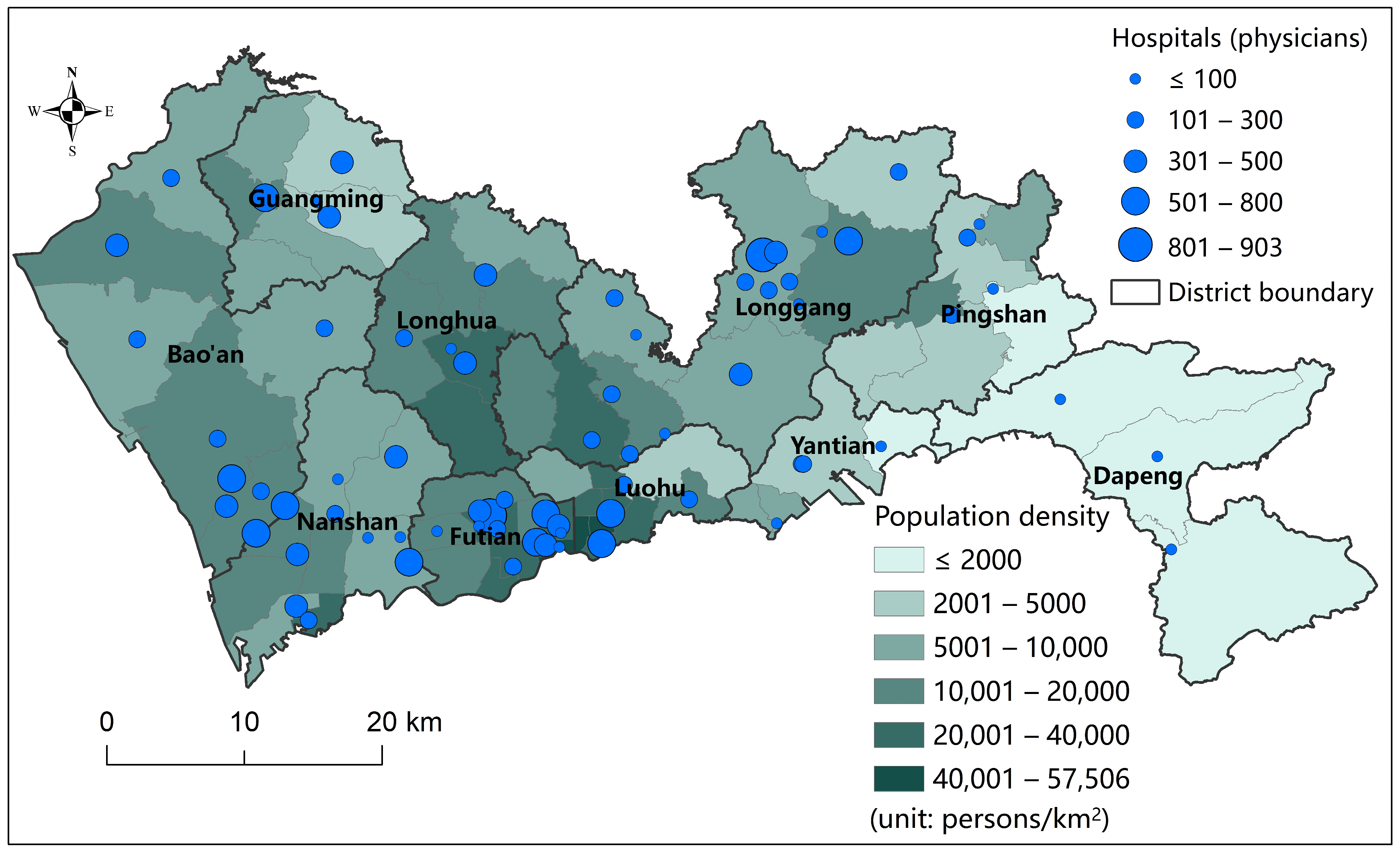
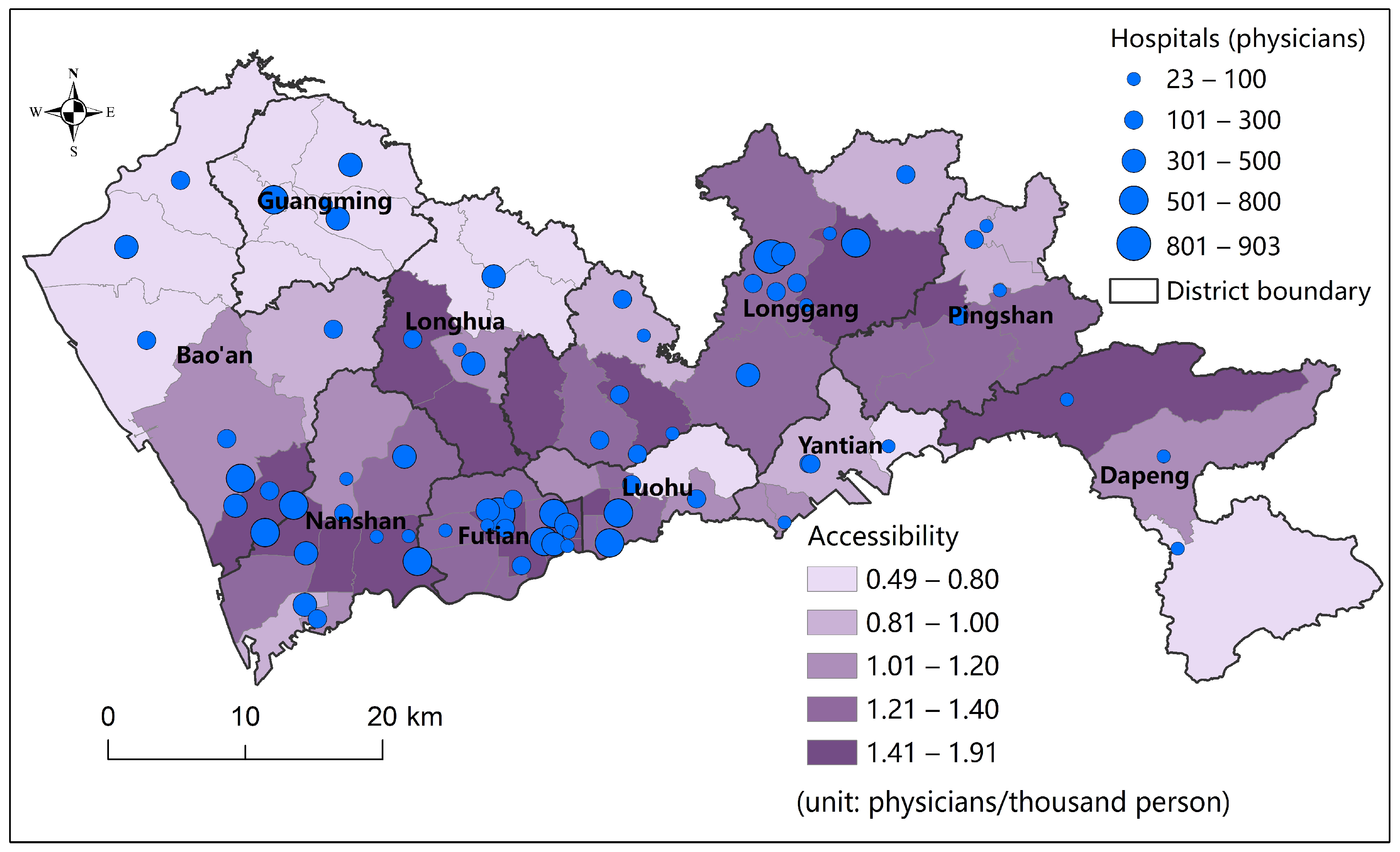
3.3. The Study Area and Data
4. Results
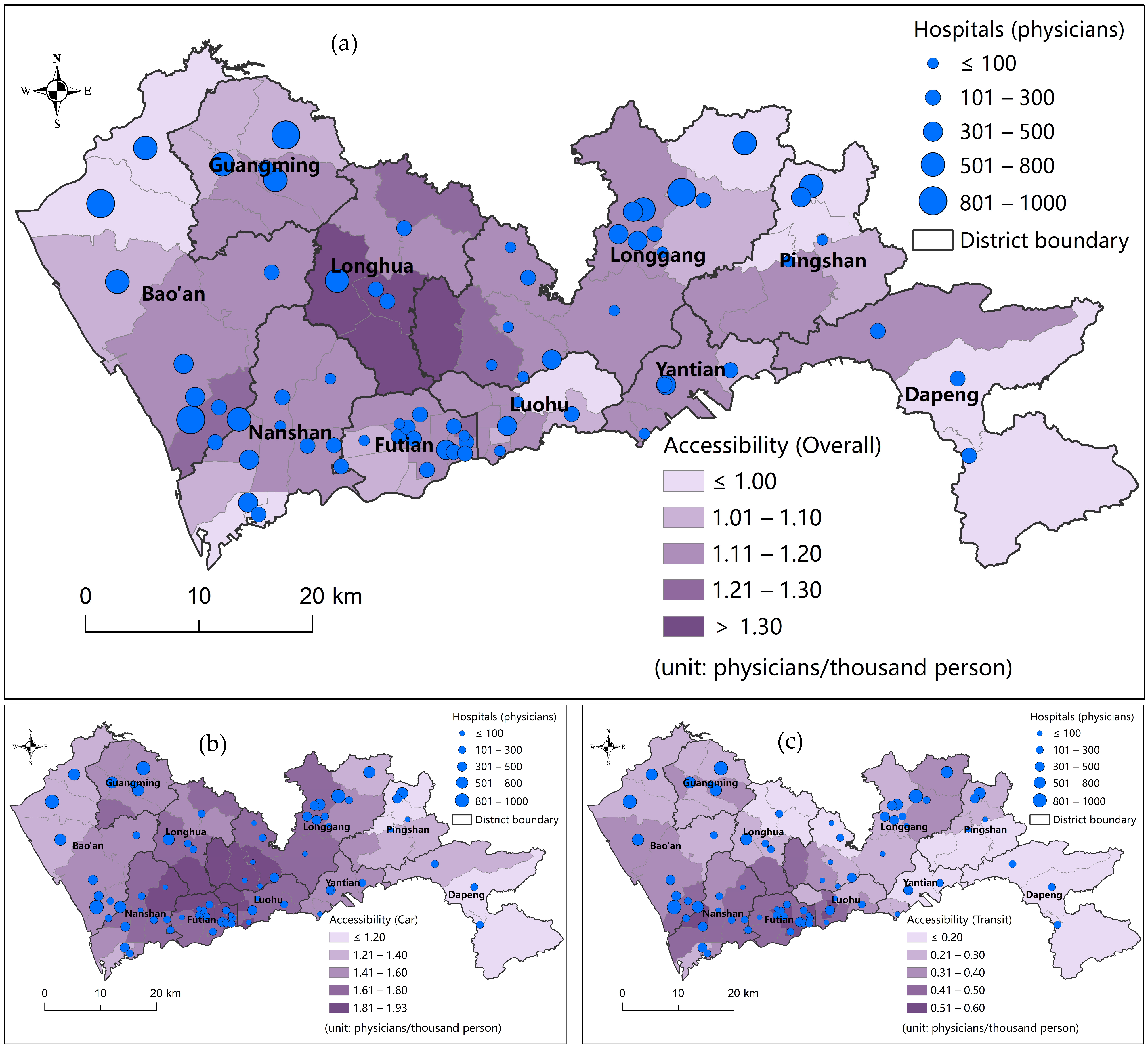
4.1. Optimization Results of the MMAE Model
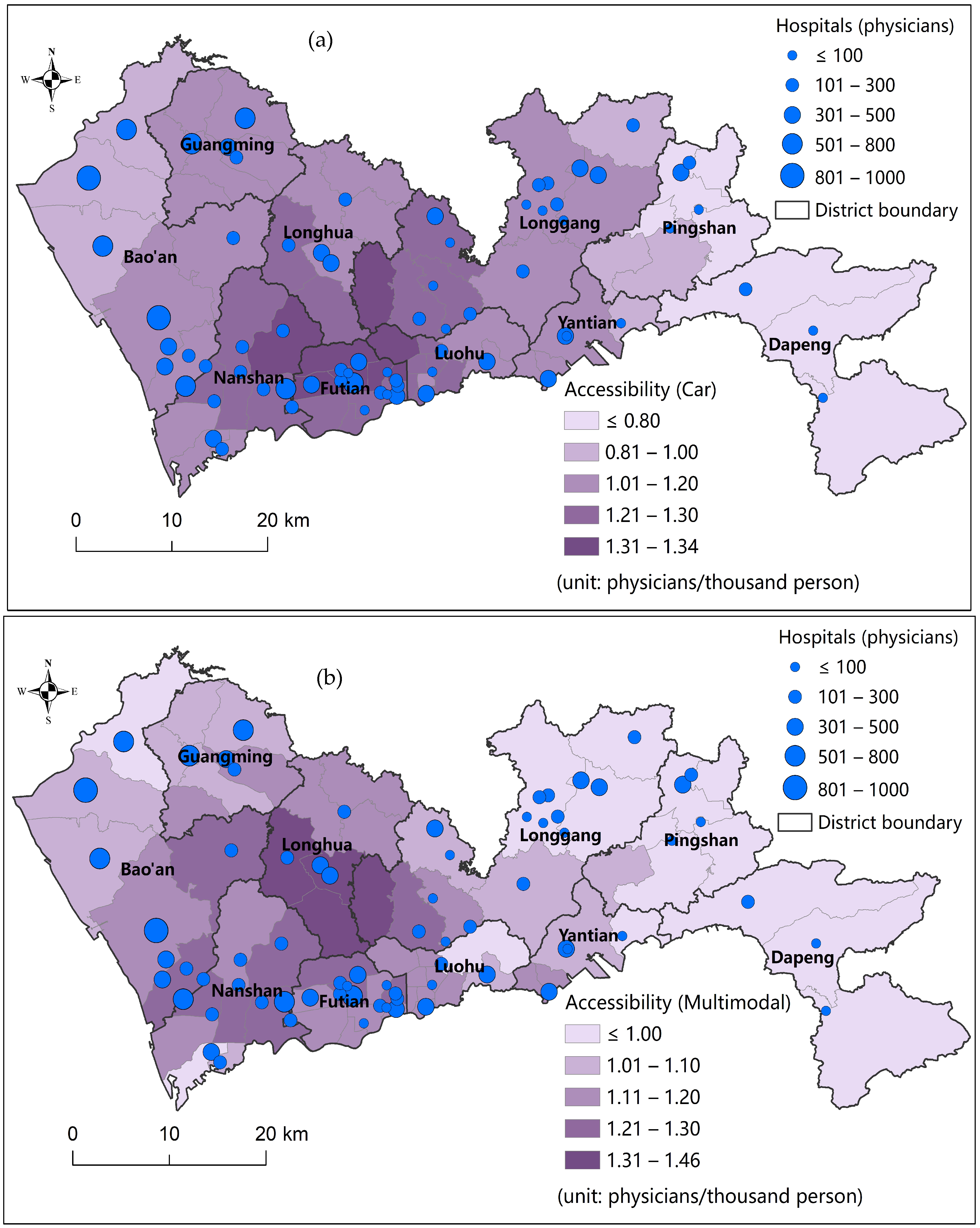
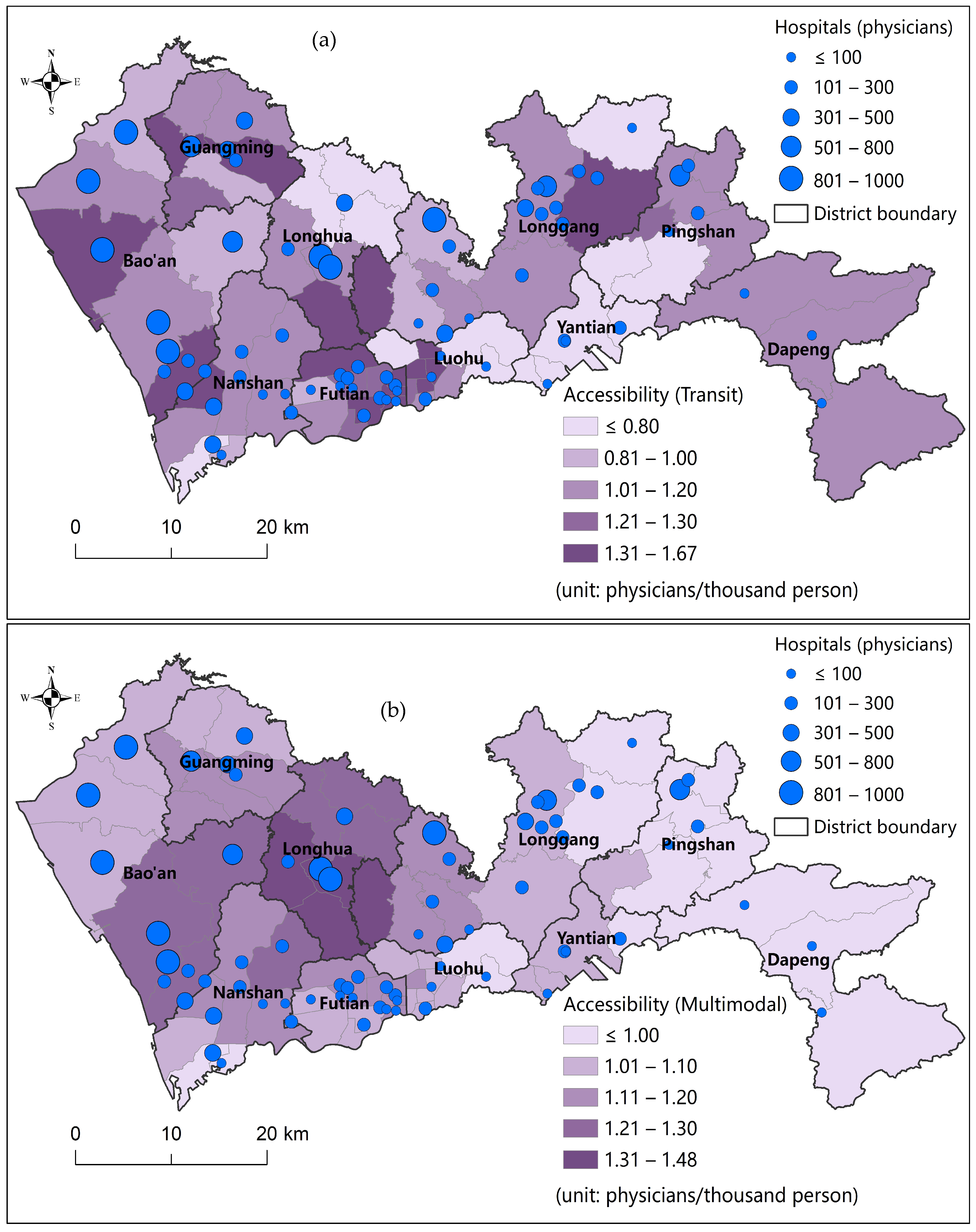
4.2. Comparisons with the Single-Modal MAE Model
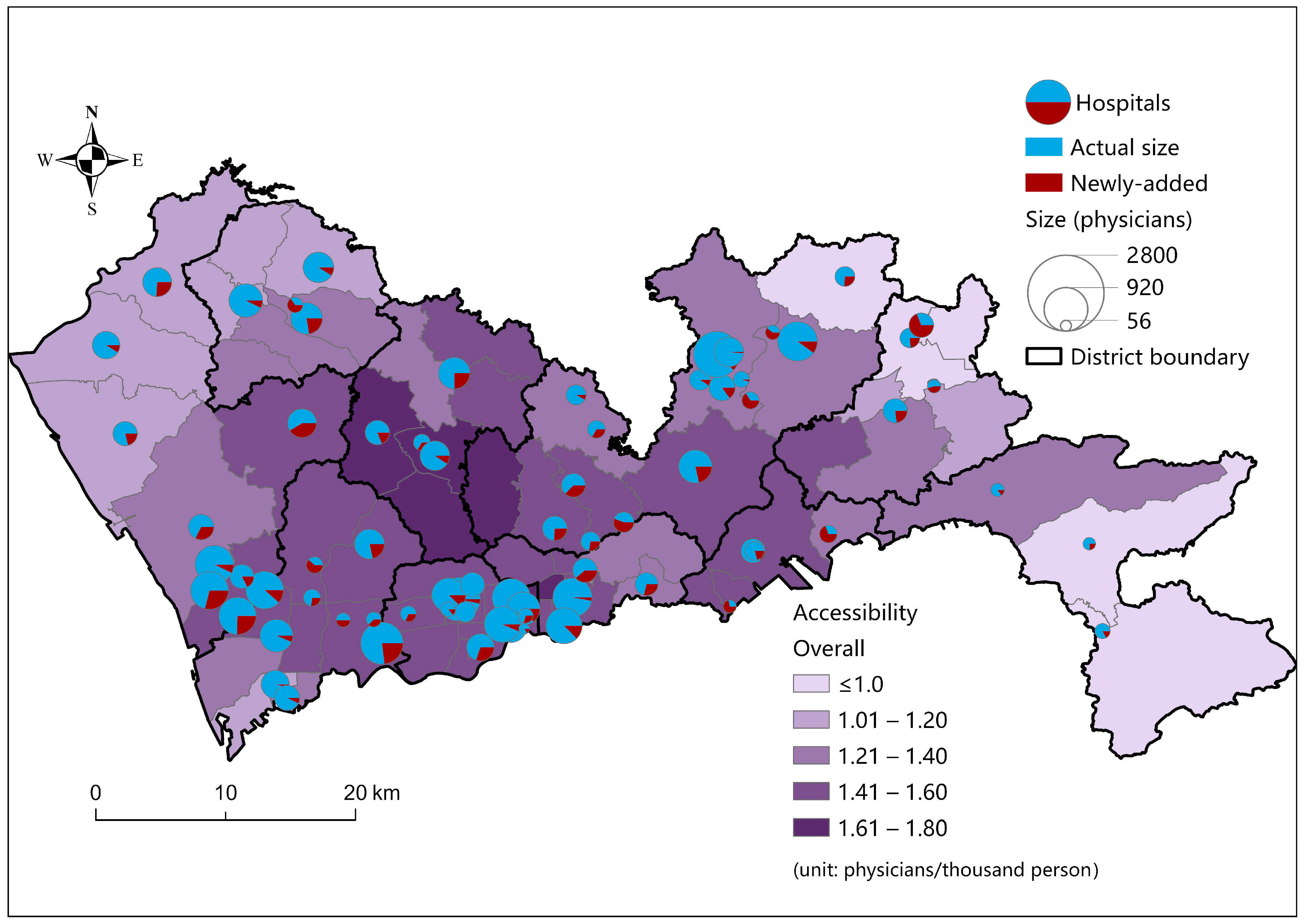
4.3. Optimal Allocation of Newly Added Resources
5. Discussion
6. Conclusions
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sen, A. Equality Reexamined; Harvard University Press: Cambridge, MA, USA, 1992. [Google Scholar]
- Krugman, P. Why Inequality Matters. New York Times, 17 December 2013; Volume 163, p. A23. [Google Scholar]
- Guagliardo, M.F. Spatial accessibility of primary care: Concepts, methods and challenges. Int. J. Health Geogr. 2004, 3, 3. [Google Scholar] [CrossRef]
- Khan, A.A. An integrated approach to measuring potential spatial access to health care services. Socio-Econ. Plan. Sci. 1992, 26, 275–287. [Google Scholar] [CrossRef]
- Neutens, T. Accessibility, equity and health care: Review and research directions for transport geographers. J. Transp. Geogr. 2015, 43, 14–27. [Google Scholar] [CrossRef]
- Wang, F. Measurement, optimization and impact of healthcare accessibility: A methodological review. Ann. Assoc. Am. Geogr. 2012, 102, 1104–1112. [Google Scholar] [CrossRef]
- Shen, Y.; Tao, Y. Associations between spatial access to medical facilities and health-seeking behaviors: A mixed geographically weighted regression analysis in Shanghai, China. Appl. Geogr. 2022, 139, 102644. [Google Scholar] [CrossRef]
- Yuan, B.; Zhang, T.; Li, J. Travel experience and health service amongst older people from the perspective of social exclusion: Policy implications of alleviating transport deprivation. Health Soc. Care Community 2022, 30, E4894–E4908. [Google Scholar] [CrossRef] [PubMed]
- Wang, F.; McLafferty, S.; Escamilla, V.; Luo, L. Late-Stage Breast Cancer Diagnosis and Health Care Access in Illinois. Prof. Geogr. 2008, 60, 54–69. [Google Scholar] [CrossRef] [PubMed]
- Hay, A.M. Concepts of Equity, Fairness and Justice in Geographical Studies. Trans. Inst. Br. Geogr. 1995, 20, 500–508. [Google Scholar] [CrossRef]
- Oliver, A.; Mossialos, E. Equity of access to health care: Outlining the foundations for action. J. Epidemiol. Community Health 2004, 58, 655–658. [Google Scholar] [CrossRef]
- Whitehead, J.; Pearson, A.L.; Lawrenson, R.; Atatoa-Carr, P. How can the spatial equity of health services be defined and measured? A systematic review of spatial equity definitions and methods. J. Health Serv. Res. Policy 2019, 24, 270–278. [Google Scholar] [CrossRef]
- Drezner, Z.; Hamacher, H.W. Facility Location: Applications and Theory; Springer: New York, NY, USA, 2002. [Google Scholar]
- Hakimi, S.L. Optimum locations of switching centers and the absolute centers and medians of a graph. Oper. Res. 1964, 12, 450–459. [Google Scholar] [CrossRef]
- Owen, S.H.; Daskin, M.S. Strategic facility location: A review. Eur. J. Oper. Res. 1998, 111, 423–447. [Google Scholar] [CrossRef]
- Wang, F.; Tang, Q. Planning toward equal accessibility to services: A quadratic programming approach. Environ. Plan. B Plan. Des. 2013, 40, 195–212. [Google Scholar] [CrossRef]
- Dai, T.; Liao, C.; Zhao, S. Optimizing the spatial assignment of schools through a random mechanism towards equal educational opportunity: A resemblance approach. Comput. Environ. Urban Syst. 2019, 76, 24–30. [Google Scholar] [CrossRef]
- Li, X.; Wang, F.; Yi, H. A two-step approach to planning new facilities towards equal accessibility. Environ. Plan. B Urban Anal. City Sci. 2017, 44, 994–1011. [Google Scholar] [CrossRef]
- Li, M.; Wang, F.; Kwan, M.-P.; Chen, J.; Wang, J. Equalizing the spatial accessibility of emergency medical services in Shanghai: A trade-off perspective. Comput. Environ. Urban Syst. 2022, 92, 101745. [Google Scholar] [CrossRef]
- Tao, Z.; Cheng, Y.; Dai, T.; Rosenberg, M.W. Spatial optimization of residential care facility locations in Beijing, China: Maximum equity in accessibility. Int. J. Health Geogr. 2014, 13, 33. [Google Scholar] [CrossRef] [PubMed]
- Dony, C.C.; Delmelle, E.M.; Delmelle, E.C. Re-conceptualizing accessibility to parks in multi-modal cities: A Variable-width Floating Catchment Area (VFCA) method. Landsc. Urban Plan. 2015, 143, 90–99. [Google Scholar] [CrossRef]
- Sharma, G.; Patil, G.R. Public transit accessibility approach to understand the equity for public healthcare services: A case study of Greater Mumbai. J. Transp. Geogr. 2021, 94, 103123. [Google Scholar] [CrossRef]
- Tahmasbi, B.; Mansourianfar, M.H.; Haghshenas, H.; Kim, I. Multimodal accessibility-based equity assessment of urban public facilities distribution. Sustain. Cities Soc. 2019, 49, 101633. [Google Scholar] [CrossRef]
- Mao, L.; Nekorchuk, D. Measuring spatial accessibility to healthcare for populations with multiple transportation modes. Health Place 2013, 24, 115–122. [Google Scholar] [CrossRef] [PubMed]
- Langford, M.; Higgs, G.; Fry, R. Multi-modal two-step floating catchment area analysis of primary health care accessibility. Health Place 2016, 38, 70–81. [Google Scholar] [CrossRef] [PubMed]
- Tao, Z.; Zhou, J.; Lin, X.; Chao, H.; Li, G. Investigating the impacts of public transport on job accessibility in Shenzhen, China: A multi-modal approach. Land Use Policy 2020, 99, 105025. [Google Scholar] [CrossRef]
- Tong, D.; Murray, A.T. Spatial Optimization in Geography. Ann. Assoc. Am. Geogr. 2012, 102, 1290–1309. [Google Scholar] [CrossRef]
- Zhang, W.; Cao, K.; Liu, S.; Huang, B. A multi-objective optimization approach for health-care facility location-allocation problems in highly developed cities such as Hong Kong. Comput. Environ. Urban Syst. 2016, 59, 220–230. [Google Scholar] [CrossRef]
- Chang, J.; Deng, Q.; Hu, P.; Guo, M.; Lu, F.; Su, Y.; Sun, J.; Qi, Y.; Long, Y.; Liu, J. Geographic Variation in Mortality of Acute Myocardial Infarction and Association with Health Care Accessibility in Beijing, 2007 to 2018. J. Am. Heart Assoc. 2023, 12, e029769. [Google Scholar] [CrossRef] [PubMed]
- Culyer, A.; Wagstaff, A. Equity and equality in health and health care. J. Health Econ. 1993, 12, 431–457. [Google Scholar] [CrossRef] [PubMed]
- Lu, C.; Zhang, Z.; Lan, X. Impact of China’s referral reform on the equity and spatial accessibility of healthcare resources: A case study of Beijing. Soc. Sci. Med. 2019, 235, 112386. [Google Scholar] [CrossRef] [PubMed]
- Harrington, D.W.; Rosenberg, M.W.; Wilson, K. Comparing health status and access to health care in Canada’s largest metropolitan areas. Urban Geogr. 2014, 35, 1156–1170. [Google Scholar] [CrossRef]
- Cheng, G.; Zeng, X.; Duan, L.; Lu, X.; Sun, H.; Jiang, T.; Li, Y. Spatial difference analysis for accessibility to high level hospitals based on travel time in Shenzhen, China. Habitat Int. 2016, 53, 485–494. [Google Scholar] [CrossRef]
- Liao, Y.; Gil, J.; Pereira, R.H.M.; Yeh, S.; Verendel, V. Disparities in travel times between car and transit: Spatiotemporal patterns in cities. Sci. Rep. 2020, 10, 4056. [Google Scholar] [CrossRef] [PubMed]
- Salonen, M.; Toivonen, T. Modelling travel time in urban networks: Comparable measures for private car and public transport. J. Transp. Geogr. 2013, 31, 143–153. [Google Scholar] [CrossRef]
- Zhang, F.; Li, D.; Ahrentzen, S.; Zhang, J. Assessing spatial disparities of accessibility to community-based service resources for Chinese older adults based on travel behavior: A city-wide study of Nanjing, China. Habitat Int. 2019, 88, 101984. [Google Scholar] [CrossRef]
- Hu, S.; Song, W.; Li, C.; Lu, J. A multi-mode Gaussian-based two-step floating catchment area method for measuring accessibility of urban parks. Cities 2020, 105, 102815. [Google Scholar] [CrossRef]
- Cheng, S.; Liao, Z.; Zhu, Y. Dynamic Changes in Community Deprivation of Access to Urban Green Spaces by Multiple Transport Modes. Front. Public Health 2021, 9, 615432. [Google Scholar] [CrossRef]
- Wang, Y.; Liu, Y.; Xing, L.; Zhang, Z. An Improved Accessibility-Based Model to Evaluate Educational Equity: A Case Study in the City of Wuhan. ISPRS Int. J. Geo-Inf. 2021, 10, 458. [Google Scholar] [CrossRef]
- White, J.A.; Case, K.E. On covering problems and the central facilities location problem. Geogr. Anal. 1974, 6, 281–294. [Google Scholar] [CrossRef]
- Church, R.; ReVelle, C.S. The maximal covering location problem. Pap. Reg. Sci. 1974, 32, 101–118. [Google Scholar] [CrossRef]
- Luo, J.; Tian, L.; Luo, L.; Yi, H.; Wang, F. Two-Step Optimization for Spatial Accessibility Improvement: A Case Study of Health Care Planning in Rural China. BioMed Res. Int. 2017, 2017, 2094654. [Google Scholar] [CrossRef]
- Liao, C.; Scheuer, B.; Dai, T.; Tian, Y. Optimizing the spatial assignment of schools to reduce both inequality of educational opportunity and potential opposition rate. Socio-Econ. Plan. Sci. 2020, 72, 100893. [Google Scholar] [CrossRef]
- Mu, L.; Xing, L.; Jing, Y.; Hu, Q. Spatial Optimization of Park Green Spaces by an Improved Two-Step Optimization Model from the Perspective of Maximizing Accessibility Equity. Land 2023, 12, 948. [Google Scholar] [CrossRef]
- Tao, Z.; Zhao, M. Planning for equal transit-based accessibility of healthcare facilities: A case study of Shenzhen, China. Socio-Econ. Plan. Sci. 2023, 88, 101666. [Google Scholar] [CrossRef]
- Shen, Q. Location Characteristics of Inner-City Neighborhoods and Employment Accessibility of Low-Wage Workers. Environ. Plan. B Plan. Des. 1998, 25, 345–365. [Google Scholar] [CrossRef]
- Du, F.; Mao, L.; Wang, J. Determinants of travel mode choice for seeking healthcare: A comparison between elderly and non-elderly patients. J. Transp. Geogr. 2021, 92, 103023. [Google Scholar] [CrossRef]
- Wang, F.; Dai, T. Spatial Optimization and Planning Practice towards Equal Access of Public Services. J. Urban Reg. Plan. 2020, 12, 28–40. [Google Scholar]
- Tao, Z.; Dai, T.; Song, C. Improving spatial equity-oriented location-allocation models of urban medical facilities. Acta Geogr. Sin. 2023, 2, 474–489. [Google Scholar]
- Kennedy, J.; Eberhart, R.C. Particle swarm optimization. In Proceedings of the IEEE International Conference on Neural Networks, Perth, Australia, 27 November–1 December 1995; Nedlands Yianni, A., Ed.; IEEE: Perth, Australia, 1996; pp. 42–48. [Google Scholar]
- Office of the Leading Group of the State Council for the Seventh National Population Census. Tabulation on 2020 China Population Census by Township; China Statistics Press: Beijing, China, 2022. [Google Scholar]
- Shenzhen Municipal Health Commission. List of Healthcare Facilities in Shenzhen. 2021. Available online: http://wjw.sz.gov.cn/bmfw/wycx/fwyl/yycx/index.html (accessed on 9 May 2024).
- Shenzhen Municipal Health Commission. The 14th Five-Year Plan of Health Development in Shenzhen. 2022. Available online: http://wjw.sz.gov.cn/gkmlpt/content/9/9713/post_9713146.html#2496 (accessed on 30 May 2024).
- The People’s Government of Shenzhen Municipality. The 14th Five-Year Plan for Shenzhen’s National Economic and Social Development and the Outline of the 2035 Long-Term Goals. 2021. Available online: http://szfb.sz.gov.cn/attachment/1/1453/1453217/11345233.pdf (accessed on 23 July 2024).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Scenario | MAD of Accessibility * | Equality Improvement ** |
|---|---|---|
| Actual allocation | 0.287 | / |
| Multimodal optimization | 0.087 | 69.7% |
| Car-modal optimization, car-modal accessibility | 0.114 | 60.3% |
| Car-modal optimization, multimodal accessibility | 0.124 | 56.8% |
| Transit-modal optimization, transit-modal accessibility | 0.188 | 34.5% |
| Transit-modal optimization, multimodal accessibility | 0.199 | 30.7% |
| New resource allocation scenario | 0.168 | 41.5% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tao, Z.; Zhong, Q.; Dang, Y. A Maximal Multimodal Accessibility Equality Model to Optimize the Equality of Healthcare Services. ISPRS Int. J. Geo-Inf. 2024, 13, 278. https://doi.org/10.3390/ijgi13080278
Tao Z, Zhong Q, Dang Y. A Maximal Multimodal Accessibility Equality Model to Optimize the Equality of Healthcare Services. ISPRS International Journal of Geo-Information. 2024; 13(8):278. https://doi.org/10.3390/ijgi13080278
Chicago/Turabian StyleTao, Zhuolin, Qianyu Zhong, and Yinuo Dang. 2024. "A Maximal Multimodal Accessibility Equality Model to Optimize the Equality of Healthcare Services" ISPRS International Journal of Geo-Information 13, no. 8: 278. https://doi.org/10.3390/ijgi13080278