

Assistive and Emerging Technologies to Detect and Reduce Neurophysiological Stress and Anxiety in Children and Adolescents with Autism and Sensory Processing Disorders: A Systematic Review

 ,
,  ,
, 
 ,
, 


Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
- P: Children and young people from birth to 21 years of age with ASD.
- I: Assistive technologies (low-high) and emerging technologies.
- C: ASD, with typical development and other neurodevelopmental disorders; other types of interventions.
- O: Reduction in stress and anxiety, improvement in ASD behavioral traits, reduction in aggressive behavior, and better concentration and focus.
- RQ1. What assistive and emerging technologies are used to combat stress in people with ASD?
- RQ2. Can assistive and emerging technologies help people with ASD reduce stress?
- RQ3. What are the measurements used to detect the outcomes?
- RQ4. What are the effect sizes of the studies?
2.2. Inclusion/Exclusion Criteria
- IC1: Research conducted between January 2014 and 30 March 2024 will be included.
- IC2: Experimental studies, observational studies, and original research will be included.
- IC3: Research and studies that are published in English only will be included.
- IC4: The use of new, assistive, and emerging technologies exclusively for the management of neurophysiological stress and anxiety will be included.
- IC5: Populations that have research inclusion criteria that are relevant to ASD and may include comorbidities with other conditions will be included.
- IC6: Research samples of children and adolescents up to 21 years of age will be included.
- EC1: Studies conducted before 2014 and after March 2024 will not be included.
- EC2: Studies of literature, systematic reviews, and meta-analyses of other studies will not be included.
- EC3: Studies published in a language other than English will not be included.
- EC4: Studies that include the use of new technologies or assistive technologies that do not include at least stress and anxiety in the outcome measures will not be used.
- EC5: Studies that include other populations of neurodevelopmental disorders will not be used unless they involve a comorbidity with ASD or suggest a corresponding study in that population.
- EC6: Included studies will not contain a sample of subjects older than 21 years of age.
2.3. Databases Screened and Selection Process
2.4. Data Extraction
2.5. Included Studies
3. Theoretical Knowledge
3.1. Neurophysiological Stress and Anxiety
3.2. Gut–Brain Axis
3.3. Structural and Functional Differences Caused by Stress in Early Development
3.4. ASD, Sensory Modulation Disorder (SMD), and Stress Due to Hyperreactivity to Stimuli
3.5. Stress Measurements
- -
- Through GSR (galvanic skin response) by using changes in skin conductance. When stress is present, skin resistance decreases due to increased sweat secretion.
- -
- Electromyography (EMG) measures the electrical activity of muscles. Stress causes differences in muscle contraction, which can be used to determine stress levels.
- -
- Skin temperature changes that correlate to an increase in stress levels.
- -
- Measurement of heart rate and heart rate variability.
- -
- Electrocardiogram (ECG), from which the heart rate and heart rate variability are measured. (Calculation of the variability of heart rate variability [52].
3.6. Measurement of Stress in Individuals with ASD
4. Results
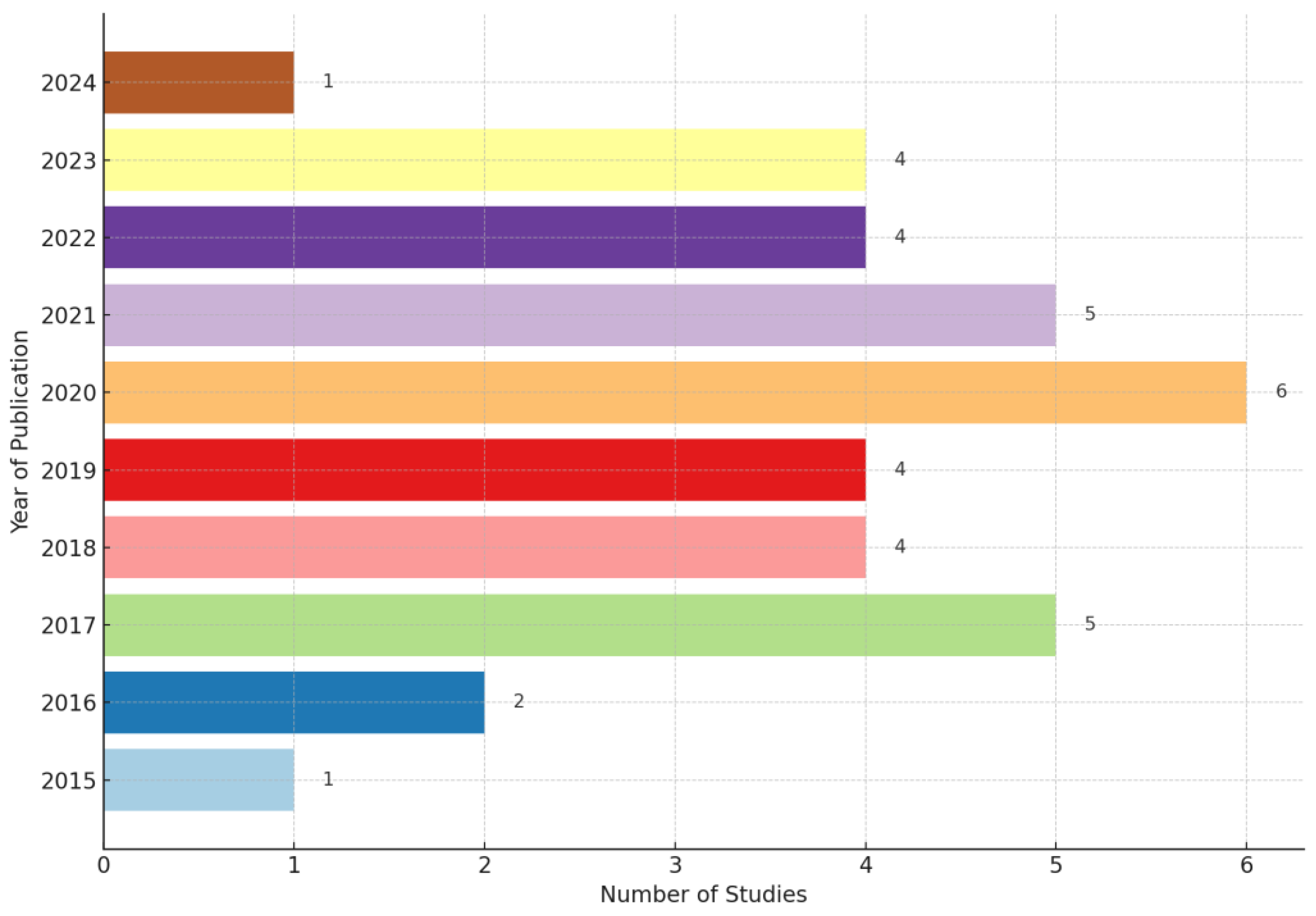
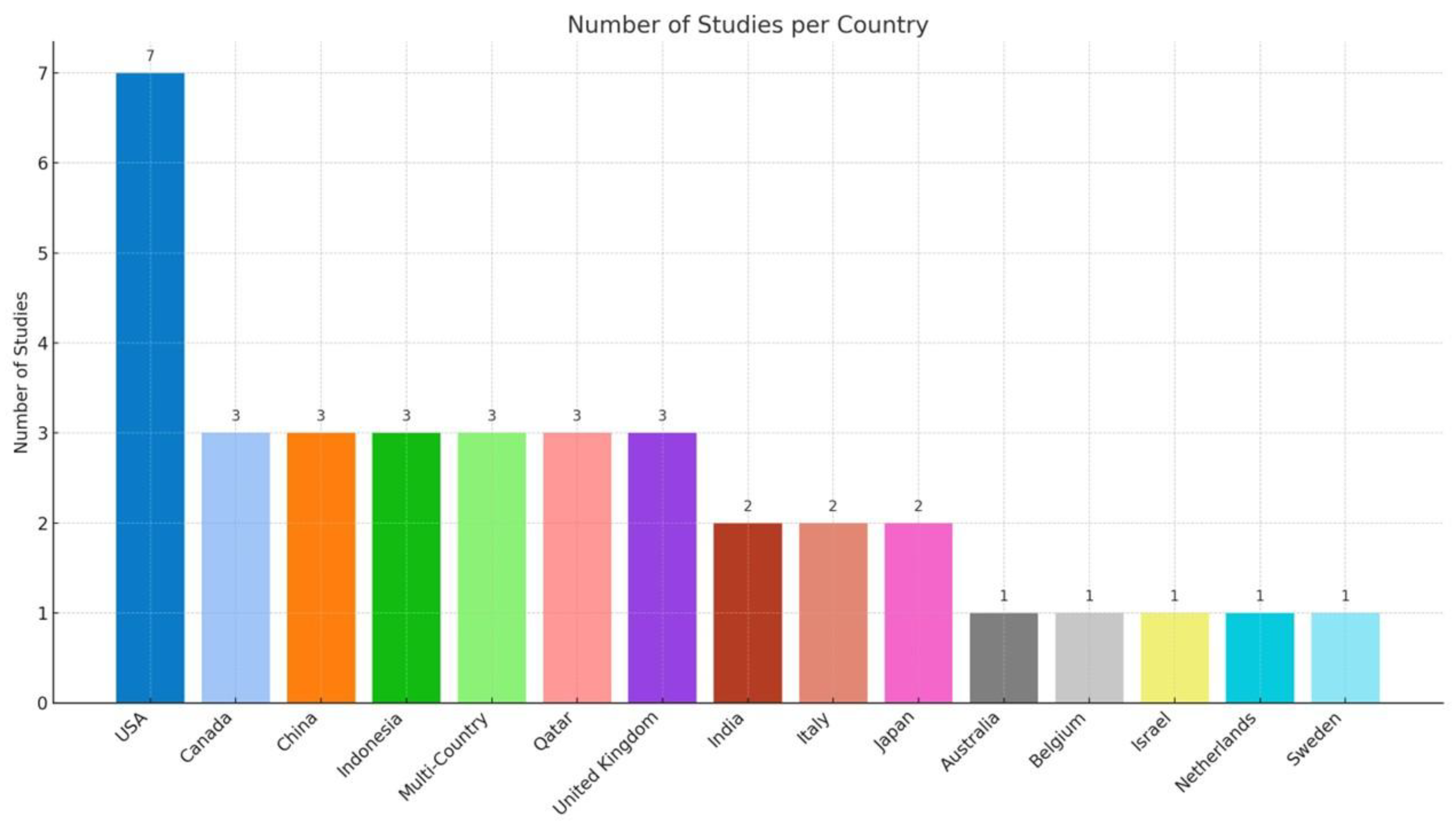
4.1. Studies Characteristics
4.2. Assistive and Emerging Technologies for Children and Adolescents with ASD on Stress Management (Low Technology)
4.2.1. Visual Programs/Schedules
4.2.2. Sensory Modalities and Wearables
4.3. Assistive and Emerging Technologies for Children and Adolescents with ASD on Stress Management (High-Tech and Emerging Technologies)
4.3.1. High-Tech Wearables
4.3.2. AI Machine Learning Predictors
4.3.3. Mobile Apps
4.3.4. Social Robots
4.3.5. Serious Games
4.3.6. Virtual Reality
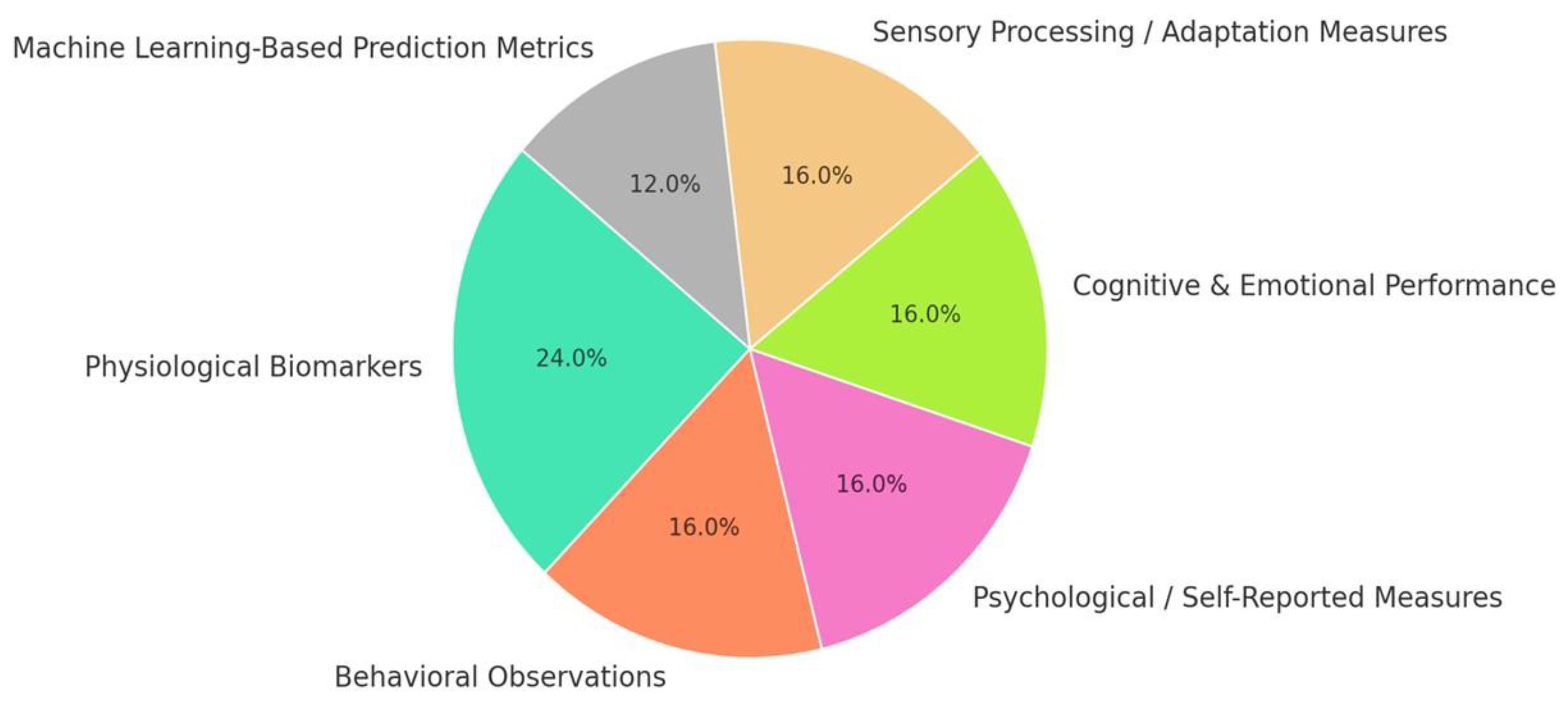
4.4. Measurement Tools Used
4.5. Effect Sizes Among Technologies
5. Discussion
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Thomaidis, L.; Mavroeidi, N.; Richardson, C.; Choleva, A.; Damianos, G.; Bolias, K.; Tsolia, M. Autism Spectrum Disorders in Greece: Nationwide Prevalence in 10–11 Year-Old Children and Regional Disparities. J. Clin. Med. 2020, 9, 2163. [Google Scholar] [CrossRef] [PubMed]
- Qin, L.; Wang, H.; Ning, W.; Cui, M.; Wang, Q. New advances in the diagnosis and treatment of autism spectrum disorders. Eur. J. Med. Res. 2024, 29, 322. [Google Scholar] [CrossRef] [PubMed]
- Okoye, C.; Obialo-Ibeawuchi, C.M.; Obajeun, O.A.; Sarwar, S.; Tawfik, C.; Waleed, M.S.; Wasim, A.U.; Mohamoud, I.; Afolayan, A.Y.; Mbaezue, R.N. Early diagnosis of Autism Spectrum Disorder: A review and analysis of the risks and benefits. Cureus 2023, 15, e43226. [Google Scholar] [CrossRef] [PubMed]
- Lord, C.; Brugha, T.S.; Charman, T.; Cusack, J.C.; Dumas, G.; Frazier, T.W.; Jones, E.; Jones, R.; Pickles, A.; State, M.W.; et al. Autism spectrum disorder. Nat. Rev. Dis. Primers 2020, 6, 1–23. [Google Scholar] [CrossRef]
- Hollocks, M.J.; Lerh, J.W.; Magiati, I.; Meiser-Stedman, R.; Brugha, T.S. Anxiety and depression in adults with autism spectrum disorder: A systematic review and meta-analysis. Psychol. Med. 2019, 49, 559–572. [Google Scholar] [CrossRef]
- Hodges, H.; Fealko, C.; Soares, N. Autism spectrum disorder: Definition, epidemiology, causes, and clinical evaluation. J. Clin. Med. 2020, 9 (Suppl. S1), S55–S65. [Google Scholar] [CrossRef]
- Grzadzinski, R.; Huerta, M.; Lord, C. DSM-5 and autism spectrum disorders (ASDs): An opportunity for identifying ASD subtypes. Mol. Autism 2013, 4, 12. [Google Scholar] [CrossRef]
- Johnson, C.P.; Myers, S.M. Identification and evaluation of children with autism spectrum disorders. Pediatrics 2007, 120, 1183–1215. [Google Scholar] [CrossRef]
- Van ’t Hof, M.; Tisseur, C.; van Berckelear-Onnes, I.; van Nieuwenhuyzen, A.; Daniels, A.M.; Deen, M.; Hoek, H.W.; Ester, W.A. Age at autism spectrum disorder diagnosis: A systematic review and meta-analysis from 2012 to 2019. Autism 2020, 25, 862–873. [Google Scholar] [CrossRef]
- Miller, L.J.; Anzalone, M.E.; Lane, S.J.; Cermak, S.A.; Osten, E.T. Concept Evolution in Sensory Integration: A Proposed Nosology for Diagnosis. Am. J. Occup. Ther. 2007, 61, 135–140. [Google Scholar] [CrossRef]
- Diagnostic and Statistical Manual of Mental Disorders; American Psychiatric Association: Washington, DC, USA, 2013.
- Christensen, J.; Wild, H.; Kenzie, E.S.; Wakeland, W.W.; Budding, D.; Lillas, C. Diverse Autonomic Nervous System Stress Response Patterns in Childhood Sensory Modulation. Frontiers in Integrative. Front. Integr. Neurosci. 2020, 14, 6. [Google Scholar] [CrossRef] [PubMed]
- Bar-Shalita, T.; Vatine, J.J.; Parush, S. Sensory modulation disorder: A risk factor for participation in daily life activities. Dev. Med. Child Neurol. 2008, 50, 932–937. [Google Scholar] [CrossRef] [PubMed]
- Schoen, S.A. Physiological and behavioral differences in sensory processing: A comparison of children with Autism Spectrum Disorder and Sensory Processing Disorder. Front. Integr. Neurosci. 2009, 3, 29. [Google Scholar] [CrossRef] [PubMed]
- Sayers, J.V. The World Health Report 2001—Mental Health: New Understanding, New Hope. Bull. World Health Organ. 2001, 79, 1085. [Google Scholar]
- Fernández-Batanero, J.M.; Montenegro-Rueda, M.; Fernández-Cerero, J. Access and Participation of Students with Disabilities: The Challenge for Higher Education. Int. J. Environ. Res. Public Health 2022, 19, 11918. [Google Scholar] [CrossRef]
- Mcculloch, G. Documentary research. In Routledge eBooks; CRC Press: Boca Raton, FL, USA, 2004. [Google Scholar] [CrossRef]
- Cook, A.M.; Hussey, S.M. Assistive Technologies: Principles and Practice; Mosby: St. Louis, MO, USA, 1995. [Google Scholar]
- Cañete, R.; Peralta, M.E. ASDesign: A User-Centered Method for the Design of Assistive Technology That Helps Children with Autism Spectrum Disorders Be More Independent in Their Daily Routines. Sustainability 2022, 14, 516. [Google Scholar] [CrossRef]
- Boon, W.; Moors, E. Exploring emerging technologies using metaphors—A study of orphan drugs and pharmacogenomics. Soc. Sci. Med. 2008, 66, 1915–1927. [Google Scholar] [CrossRef]
- Stahl, B.C. What does the future hold? A critical view of emerging information and communication technologies and their social consequences. In IFIP Advances in Information and Communication Technology; Springer: Berlin/Heidelberg, Germany, 2011; pp. 59–76. [Google Scholar] [CrossRef]
- Rotolo, D.; Hicks, D.; Martin, B.R. What is an emerging technology? Res. Policy 2015, 44, 1827–1843. [Google Scholar] [CrossRef]
- Hostinar, C.E.; Johnson, A.E.; Gunnar, M.R. Parent Support Is Less Effective in Buffering Cortisol Stress Reactivity for Adolescents Compared to Children. Dev. Sci. 2015, 18, 281–297. [Google Scholar] [CrossRef]
- Drigas, A.; Mitsea, E. Metacognition, Stress–Relaxation Balance & Related Hormones. Int. J. Recent Contrib. Eng. Sci. IT 2021, 9, 4. [Google Scholar] [CrossRef]
- Bravou, V.; Driga, A.M.S.; Drigas, A. Emotion Regulation, the Function of Stress Hormones & Digital Technologies. Tech. BioChemMed 2022, 3, 27–33. [Google Scholar] [CrossRef]
- McEwen, B.S. Neurobiological and Systemic Effects of Chronic Stress. Chronic Stress 2017, 1, 247054701769232. [Google Scholar] [CrossRef] [PubMed]
- Makris, G.; Eleftheriades, A.; Pervanidou, P. Early Life Stress, Hormones, and Neurodevelopmental Disorders. Horm. Res. Paediatr. 2023, 96, 17–24. [Google Scholar] [CrossRef] [PubMed]
- Cryan, J.F.; O’Mahony, S.M. The microbiome-gut-brain axis: From bowel to behavior. Neurogastroenterol. Motil. 2011, 23, 187–192. [Google Scholar] [CrossRef]
- Chen, X.; D’Souza, R.; Hong, S. The role of gut microbiota in the gut-brain axis: Current challenges and perspectives. Protein Cell 2013, 4, 403–414. [Google Scholar] [CrossRef]
- Mayer, E.A. Gut Feelings: The Emerging Biology of Gut–Brain Communication. Nat. Rev. Neurosci. 2011, 12, 453–466. [Google Scholar] [CrossRef]
- Foster, J.A.; Rinaman, L.; Cryan, J.F. Stress & the gut-brain axis: Regulation by the microbiome. Neurobiol. Stress 2017, 7, 124–136. [Google Scholar] [CrossRef]
- Stilling, R.M.; Ryan, F.J.; Hoban, A.E.; Shanahan, F.; Clarke, G.; Claesson, M.J.; Dinan, T.G.; Cryan, J.F. Microbes & Neurodevelopment—Absence of Microbiota during Early Life Increases Activity-Related Transcriptional Pathways in the Amygdala. Brain Behav. Immun. 2015, 50, 209–220. [Google Scholar] [CrossRef]
- Puricelli, C.; Rolla, R.; Gigliotti, C.L.; Boggio, E.; Beltrami, E.; Dianzani, U.; Keller, R. The Gut-Brain-Immune axis in Autism Spectrum Disorders: A State-of-Art Report. Front. Psychiatry 2022, 12, 755171. [Google Scholar] [CrossRef]
- Bamicha, V.; Pergantis, P.; Drigas, A. The Effect of Gut Microbiome, Neurotransmitters, and Digital Insights in Autism. Appl. Microbiol. 2024, 4, 1677–1701. [Google Scholar] [CrossRef]
- Banqueri, M.; Méndez, M.; Arias, J. Impact of Stress in Childhood: Psychobiological Alterations. Psicothema 2017, 1, 18–22. [Google Scholar] [CrossRef]
- Seckfort, D.L.; Paul, R.; Grieve, S.M.; Vandenberg, B.; Bryant, R.A.; Williams, L.M.; Clark, C.R.; Cohen, R.A.; Bruce, S.; Gordon, E. Early life stress on brain structure and function across the lifespan: A preliminary study. Brain Imaging Behav. 2008, 2, 49–58. [Google Scholar] [CrossRef]
- Frodl, T.; O’Keane, V. How does the brain deal with cumulative stress? A review with focus on developmental stress, HPA axis function and hippocampal structure in humans. Neurobiol. Dis. 2013, 52, 24–37. [Google Scholar] [CrossRef] [PubMed]
- Hanson, J.L.; Chung, M.K.; Avants, B.B.; Rudolph, K.D.; Shirtcliff, E.A.; Gee, J.C.; Davidson, R.J.; Pollak, S.D. Structural Variations in Prefrontal Cortex Mediate the Relationship between Early Childhood Stress and Spatial Working Memory. J. Neurosci. 2012, 32, 7917–7925. [Google Scholar] [CrossRef]
- Niehaus, C.E.; Chaplin, T.M.; Goncalves, S.F.; Semelsberger, R.; Thompson, J.C. Maternal stress and adolescent brain structure and function. Brain Behav. 2019, 9, e01311. [Google Scholar] [CrossRef]
- Milani, A.C.C.; Hoffmann, E.V.; Fossaluza, V.; Jackowski, A.P.; Mello, M.F. Does pediatric post-traumatic stress disorder alter the brain? Systematic review and meta-analysis of structural and functional magnetic resonance imaging studies. Psychiatry Clin. Neurosci. 2017, 71, 154–169. [Google Scholar] [CrossRef]
- Heyn, S.A.; Keding, T.J.; Ross, M.C.; Cisler, J.M.; Mumford, J.A.; Herringa, R.J. Abnormal prefrontal development in Pediatric posttraumatic stress Disorder: A Longitudinal structural and functional magnetic resonance Imaging study. Biol. Psychiatry Cogn. Neurosci. Neuroimaging 2019, 4, 171–179. [Google Scholar] [CrossRef]
- Fernández-Andrés, M.I.; Pastor-Cerezuela, G.; Sanz-Cervera, P.; Tárraga-Mínguez, R. A Comparative Study of Sensory Processing in Children with and without Autism Spectrum Disorder in the Home and Classroom Environments. Res. Dev. Disabil. 2015, 38, 202–212. [Google Scholar] [CrossRef]
- Chistol, L.T.; Bandini, L.G.; Must, A.; Phillips, S.; Cermak, S.A.; Curtin, C. Sensory Sensitivity and Food Selectivity in Children with Autism Spectrum Disorder. J. Autism Dev. Disord. 2018, 48, 583–591. [Google Scholar] [CrossRef]
- Kojovic, N.; Ben Hadid, L.; Franchini, M.; Schaer, M. Sensory Processing Issues and Their Association with Social Difficulties in Children with Autism Spectrum Disorders. J. Clin. Med. 2019, 8, 1508. [Google Scholar] [CrossRef]
- Loh, S.Y.; Ee, S.I.; Marret, M.J. Sensory processing and its relationship to participation among childhood occupations in children with autism spectrum disorder: Exploring the profile of differences. Int. J. Dev. Disabil. 2021, 69, 226–237. [Google Scholar] [CrossRef] [PubMed]
- Narzisi, A.; Fabbri-Destro, M.; Crifaci, G.; Scatigna, S.; Maugeri, F.; Berloffa, S.; Fantozzi, P.; Prato, A.; Muccio, R.; Valente, E.; et al. Sensory Profiles in School-Aged Children with Autism Spectrum Disorder: A Descriptive Study Using the Sensory Processing Measure-2 (SPM-2). J. Clin. Med. 2022, 11, 1668. [Google Scholar] [CrossRef] [PubMed]
- Crosswell, A.D.; Lockwood, K.G. Best practices for stress measurement: How to measure psychological stress in health research. Health Psychol. Open 2020, 7, 205510292093307. [Google Scholar] [CrossRef] [PubMed]
- Cohen, S.; Gianaros, P.J.; Manuck, S.B. A stage model of stress and disease. Perspect. Psychol. Sci. 2016, 11, 456–463. [Google Scholar] [CrossRef]
- Bravou, V.; Oikonomidou, D.; Drigas, A. Applications of Virtual Reality for Autism Inclusion. A Review. Retos 2022, 45, 779–785. [Google Scholar] [CrossRef]
- Pergantis, P.; Drigas, A. Assistive Technology for Autism Spectrum Disorder Children That Experiences Stress and Anxiety. Braz. J. Sci. 2023, 2, 77–93. [Google Scholar] [CrossRef]
- Moraiti, I.; Drigas, A. Measuring the stress of autistic people with the help of a smartwatch, Internet of Things Technology. Braz. J. Sci. 2024, 3, 45–56. [Google Scholar] [CrossRef]
- Moraiti, I. Examining the stress level of autistic people using a smartwatch integrated with the internet of things technology. World J. Adv. Res. Rev. 2023, 19, 1372–1389. [Google Scholar] [CrossRef]
- Tomczak, M.T. Employees with Autism Spectrum Disorders in the Digitized Work Environment: Perspectives for the Future. J. Disabil. Policy Stud. 2021, 31, 195–205. [Google Scholar] [CrossRef]
- Spratt, E.G.; Nicholas, J.S.; Brady, K.T.; Carpenter, L.A.; Hatcher, C.R.; Meekins, K.A.; Furlanetto, R.W.; Charles, J.M. Enhanced cortisol response to stress in children in autism. J. Autism Dev. Disord. 2011, 42, 75–81. [Google Scholar] [CrossRef]
- Levine, T.P.; Sheinkopf, S.J.; Pescosolido, M.; Rodino, A.; Elia, G.; Lester, B. Physiologic Arousal to Social Stress in Children with Autism Spectrum Disorders: A Pilot Study. Res. Autism Spectr. Disord. 2011, 6, 177–183. [Google Scholar] [CrossRef]
- Kushki, A.; Drumm, E.; Mobarak, M.P.; Tanel, N.; Dupuis, A.; Chau, T.; Anagnostou, E. Investigating the Autonomic Nervous System Response to Anxiety in Children with Autism Spectrum Disorders. PLoS ONE 2013, 8, e59730. [Google Scholar] [CrossRef]
- Stein, L.I.; Lane, C.J.; Williams, M.E.; Dawson, M.E.; Polido, J.C.; Cermak, S.A. Physiological and Behavioral Stress and Anxiety in Children with Autism Spectrum Disorders during Routine Oral Care. BioMed Res. Int. 2014, 2014, 694876. [Google Scholar] [CrossRef] [PubMed]
- Burke, A. Zen shiatsu: A longitudinal case study measuring stress reduction in a child with autism spectrum disorder. Int. J. Ther. Massage Bodyw. 2014, 7, 23–28. [Google Scholar] [PubMed] [PubMed Central]
- Varni, J.W.; Seid, M.; Kurtin, P.S. PEDSQLTM 4.0: Reliability and Validity of the Pediatric Quality of Life InventoryTM Version 4.0 Generic core scales in healthy and patient populations. Med. Care 2001, 39, 800–812. [Google Scholar] [CrossRef]
- Corbett, B.A.; Muscatello, R.A.; Baldinger, C. Comparing stress and arousal systems in response to different social contexts in children with ASD. Biol. Psychol. 2019, 140, 119–130. [Google Scholar] [CrossRef]
- Bloeming-Wolbrink, K.A.; Janssen, M.J.; de Weerth, C.; Ruijssenaars, W.A.; Sweep, F.C.; Eijsbouts, A.; Schuengel, C. Stress in Adults with Congenital Deafblindness and an Intellectual Disability: Information from Their Cortisol Curves. Br. J. Vis. Impair. 2012, 30, 149–159. [Google Scholar] [CrossRef]
- Thoen, A.; Steyaert, J.; Alaerts, K.; Evers, K.; Van Damme, T. A Systematic Review of Self-Reported Stress Questionnaires in People on the Autism Spectrum. Rev. J. Autism Dev. Disord. 2021, 10, 295–318. [Google Scholar] [CrossRef]
- Groden, J.; Diller, A.; Bausman, M.; Velicer, W.; Norman, G.; Cautela, J. The Development of a Stress Survey Schedule for Persons with Autism and Other Developmental Disabilities. J. Autism Dev. Disord. 2001, 31, 207–217. [Google Scholar] [CrossRef]
- Chiu, H.T.; Ip, I.N.; Ching, F.N.Y.; Wong, B.P.-H.; Lui, W.-H.; Tse, C.-S.; Wong, S.W.H. Resting Heart Rate Variability and Emotion Dysregulation in Adolescents with Autism Spectrum Disorder. J. Autism Dev. Disord. 2023, 54, 1482–1493. [Google Scholar] [CrossRef]
- Ip, H.H.; Wong, S.W.; Chan, D.F.; Byrne, J.; Li, C.; Yuan, V.S.; Lau, K.S.; Wong, J.Y. Enhance emotional and social adaptation skills for children with autism spectrum disorder: A virtual reality enabled approach. Comput. Educ. Comput. Educ. 2018, 117, 1–15. [Google Scholar] [CrossRef]
- Nguyen, J.; Cardy, R.E.; Anagnostou, E.; Brian, J.; Kushki, A. Examining the effect of a wearable, anxiety detection technology on improving the awareness of anxiety signs in autism spectrum disorder: A pilot randomized controlled trial. Mol. Autism 2021, 12, 72. [Google Scholar] [CrossRef] [PubMed]
- Fridenson-Hayo, S.; Berggren, S.; Lassalle, A.; Tal, S.; Pigat, D.; Meir-Goren, N.; O’Reilly, H.; Ben-Zur, S.; Bölte, S.; Baron-Cohen, S.; et al. ‘Emotiplay’: A serious game for learning about emotions in children with autism: Results of a cross-cultural evaluation. Eur. Child Adolesc. Psychiatry 2017, 26, 979–992. [Google Scholar] [CrossRef] [PubMed]
- Rachmani, M.; Rizal, M.F.; Sutadi, H.; Suharsini, M. Comparison of Two Visual Techniques in Decreasing Stress Levels in Children with Autism Spectrum Disorder. J. Int. Dent. Med. Res. 2020, 13, 1136–1139. [Google Scholar]
- Tamany, I.; Rizal, M.F.; Suharsini, M. Comparison of the Effectiveness of Two Intervention Methods in Reducing Stress Levels in Children with Autism. J. Int. Dent. Med. Res. 2020, 13, 1117–1120. [Google Scholar]
- Johnston, D.; Egermann, H.; Kearney, G. SoundFields: A Virtual Reality Game Designed to Address Auditory Hypersensitivity in Individuals with Autism Spectrum Disorder. Appl. Sci. 2020, 10, 2996. [Google Scholar] [CrossRef]
- Lussier-Desrochers, D.; Massé, L.; Simonato, I.; Lachapelle, Y.; Godin-Tremblay, V.; Lemieux, A. Evaluation of the effect of a serious game on the performance of daily routines by autistic and ADHD children. Adv. Neurodev. Disord. 2023, 7, 566–578. [Google Scholar] [CrossRef]
- Yuan, S.N.V.; Ip, H.H.S. Using virtual reality to train emotional and social skills in children with autism spectrum disorder. Lond. J. Prim. Care 2018, 10, 110–112. [Google Scholar] [CrossRef]
- Vallefuoco, E.; Bravaccio, C.; Gison, G.; Pecchia, L.; Pepino, A. Personalized Training via Serious Game to Improve Daily Living Skills in Pediatric Patients with Autism Spectrum Disorder. IEEE J. Biomed. Health Inform. 2022, 26, 3312–3321. [Google Scholar] [CrossRef]
- Baric, V.B.; Skuthälla, S.; Pettersson, M.; Gustafsson, P.A.; Kjellberg, A. The effectiveness of weighted blankets on sleep and everyday activities—A retrospective follow-up study of children and adults with attention deficit hyperactivity disorder and/or autism spectrum disorder. Scand. J. Occup. Ther. 2021, 30, 1357–1367. [Google Scholar] [CrossRef]
- Pfeiffer, B.; Duker, L.S.; Murphy, A.; Shui, C. Effectiveness of Noise-Attenuating headphones on physiological responses for children with autism spectrum disorders. Front. Integr. Neurosci. 2019, 13, 65. [Google Scholar] [CrossRef]
- Mah, J.W.T.; Tsang, P. Visual Schedule System in Dental Care for Patients with Autism: A Pilot Study. J. Clin. Pediatr. Dent. 2016, 40, 393–399. [Google Scholar] [CrossRef] [PubMed]
- Kwong, T.C.; Yuan, H.-L.; Mung, S.W.Y.; Chu, H.K.H.; Chan, C.C.H.; Lun, D.P.K.; Yu, H.M.; Cheng, L.; Choy, Y.S. Healthcare headset with tuneable auditory characteristics control for children with Autism spectrum disorder. Appl. Acoust. 2024, 218, 109876. [Google Scholar] [CrossRef]
- Jouen, A.-L.; Narzisi, A.; Xavier, J.; Tilmont, E.; Bodeau, N.; Bono, V.; Ketem-Premel, N.; Anzalone, S.; Maharatna, K.; Chetouani, M.; et al. GOLIAH (Gaming Open Library for Intervention in Autism at Home): A 6-Month Single Blind Matched Controlled Exploratory Study. Child Adolesc. Psychiatry Ment. Health 2017, 11, 17. [Google Scholar] [CrossRef]
- Yu, Z.; Sherpa, M.T.; Iadarola, S.; Shamlian, K.; Daley, S.; Levine, G.; Bajorski, P.; Zheng, Z. Understanding Stress in Children with ASD and Their Caregivers in Daily Life: A Feasibility Study Using Mobile Devices. In Proceedings of the MobileHCI ’23 Companion: 25th International Conference on Mobile Human-Computer Interaction, Athens, Greece, 26–29 September 2023. [Google Scholar] [CrossRef]
- Masino, A.J.; Forsyth, D.; Nuske, H.; Herrington, J.; Pennington, J.; Kushleyeva, Y.; Bonafide, C.P. m-Health and Autism: Recognizing Stress and Anxiety with Machine Learning and Wearables Data. In Proceedings of the 2019 IEEE 32nd International Symposium on Computer-Based Medical Systems (CBMS), Cordoba, Spain, 5–7 June 2019; pp. 714–719. [Google Scholar] [CrossRef]
- Alban, A.Q.; Alhaddad, A.Y.; Al-Ali, A.; So, W.; Connor, O.; Ayesh, M.; Qidwai, U.A.; Cabibihan, J. Heart Rate as a Predictor of Challenging Behaviours among Children with Autism from Wearable Sensors in Social Robot Interactions. Robotics 2023, 12, 55. [Google Scholar] [CrossRef]
- Afif, I.Y.; Farkhan, M.; Kurdi, O.; Maula, M.I.; Ammarullah, M.I.; Setiyana, B.; Jamari, J.; Winarni, T.I. Effect of Short-Term Deep-Pressure Portable Seat on Behavioral and Biological Stress in Children with Autism Spectrum Disorders: A Pilot Study. Bioengineering 2022, 9, 48. [Google Scholar] [CrossRef]
- Carlier, S.; Van Der Paelt, S.; Ongenae, F.; De Backere, F.; De Turck, F. Empowering Children with ASD and Their Parents: Design of a Serious Game for Anxiety and Stress Reduction. Sensors 2020, 20, 966. [Google Scholar] [CrossRef]
- Nakadoi, Y. Usefulness of Animal Type Robot Assisted Therapy for Autism Spectrum Disorder in the Child and Adolescent Psychiatric Ward. In Lecture Notes in Computer Science; Springer Science+Business Media: Berlin/Heidelberg, Germany, 2015; pp. 478–482. [Google Scholar] [CrossRef]
- Gee, B.M.; Lloyd, K.; Sutton, J.; McOmber, T. Weighted Blankets and Sleep Quality in Children with Autism Spectrum Disorders: A Single-Subject Design. Children 2020, 8, 10. [Google Scholar] [CrossRef]
- Bharatharaj, J.; Huang, L.; Mohan, R.E.; Al-Jumaily, A.; Krägeloh, C. Robot-Assisted Therapy for Learning and Social Interaction of Children with Autism Spectrum Disorder. Robotics 2017, 6, 4. [Google Scholar] [CrossRef]
- Zimmerman, K.N.; Ledford, J.R.; Severini, K.E. Brief Report: The effects of a weighted blanket on engagement for a student with ASD. Focus Autism Other Dev. Disabil. 2018, 34, 15–19. [Google Scholar] [CrossRef]
- Macdonald, L.; Trembath, D.; Ashburner, J.; Costley, D.; Keen, D. The use of visual schedules and work systems to increase the on-task behaviour of students on the autism spectrum in mainstream classrooms. J. Res. Spec. Educ. Needs 2018, 18, 254–266. [Google Scholar] [CrossRef]
- Alban, A.Q.; Ayesh, M.; Alhaddad, A.Y.; Al-Ali, A.K.; So, W.C.; Connor, O.; Cabibihan, J. Detection of Challenging Behaviours of Children with Autism Using Wearable Sensors during Interactions with Social Robots. In Proceedings of the 2021 30th IEEE International Conference on Robot & Human Interactive Communication (RO-MAN), Vancouver, BC, Canada, 8–12 August 2021. [Google Scholar] [CrossRef]
- Keshav, N.U.; Vahabzadeh, A.; Abdus-Sabur, R.; Huey, K.; Salisbury, J.; Liu, R.; Sahin, N.T. Longitudinal Socio-Emotional Learning Intervention for Autism via Smartglasses: Qualitative School Teacher Descriptions of Practicality, Usability, and Efficacy in General and Special Education Classroom Settings. Educ. Sci. 2018, 8, 107. [Google Scholar] [CrossRef]
- Cabibihan, J.; Chellali, R.; So CW, C.; Aldosari, M.; Connor, O.; Alhaddad, A.Y.; Javed, H. Social robots and wearable sensors for mitigating meltdowns in autism—A pilot test. In Lecture Notes in Computer Science; Springer: Berlin/Heidelberg, Germany, 2018; pp. 103–114. [Google Scholar] [CrossRef]
- Huijnen, C.A.G.J.; Verreussel-Willen, H.A.M.D.; Lexis, M.A.S.; De Witte, L.P. Robot KASPAR as Mediator in Making Contact with Children with Autism: A Pilot Study. Int. J. Soc. Robot. 2021, 13, 237–249. [Google Scholar] [CrossRef]
- Coskun, B.; Uluer, P.; Toprak, E.; Barkana, D.E.; Kose, H.; Zorcec, T.; Robins, B.; Landowska, A. Stress Detection of Children with Autism using Physiological Signals in Kaspar Robot-Based Intervention Studies. In Proceedings of the 2022 9th IEEE RAS/EMBS International Conference for Biomedical Robotics and Biomechatronics (BioRob), Seoul, Republic of Korea, 21–24 August 2022. [Google Scholar] [CrossRef]
- Zwilling, M.; Romano, A.; Hoffman, H.; Lotan, M.; Tesler, R. Development and validation of a system for the prediction of challenging behaviors of people with autism spectrum disorder based on a smart wearable shirt: A mixed-methods design. Front. Behav. Neurosci. 2022, 16, 948184. [Google Scholar] [CrossRef]
- Fioriello, F.; Maugeri, A.; D’Alvia, L.; Pittella, E.; Piuzzi, E.; Rizzuto, E.; Del Prete, Z.; Manti, F.; Sogos, C. A wearable heart rate measurement device for children with autism spectrum disorder. Sci. Rep. 2020, 10, 18659. [Google Scholar] [CrossRef]
- Newbutt, N.; Bradley, R.; Conley, I. Using virtual reality head-mounted displays in schools with autistic children: Views, experiences, and future directions. Cyberpsychology Behav. Soc. Netw. 2020, 23, 23–33. [Google Scholar]
- Roche, M.A.; Back, E.; Van Herwegen, J. Parental perspectives on the use of fidget toys and sensory-seeking profiles in autistic and neurotypical children. Curr. Psychol. 2023, 43, 15872–15882. [Google Scholar] [CrossRef]
- Suresh, L.R.; George, C.A. Virtual Reality Distraction on Dental Anxiety and Behavior in Children with Autism Spectrum Disorder. J. Int. Dent. Med. Res. 2019, 12, 1004–1010. [Google Scholar]
- Ikuta, N.; Iwanaga, R.; Tokunaga, A.; Nakane, H.; Tanaka, K.; Tanaka, G. Effectiveness of Earmuffs and Noise-cancelling Headphones for Coping with Hyper-reactivity to Auditory Stimuli in Children with Autism Spectrum Disorder: A Preliminary Study. Hong Kong J. Occup. Ther. 2016, 28, 24–32. [Google Scholar] [CrossRef]
- Miller, I.T.; Wiederhold, B.K.; Miller, C.S.; Wiederhold, M.D. Virtual Reality Air Travel Training with Children on the Autism Spectrum: A Preliminary Report. Cyberpsychology Behav. Soc. Netw. 2020, 23, 10–15. [Google Scholar] [CrossRef]
- Hirano, S.H.; Yeganyan, M.T.; Marcu, G.; Nguyen, D.H.; Boyd, L.A.; Hayes, G.R. vSked: Evaluation of a System to Support Classroom Activities for Children with Autism. In Proceedings of the SIGCHI Conference on Human Factors in Computing Systems, Atlanta, GA, USA, 10–15 April 2010; pp. 1633–1642. [Google Scholar] [CrossRef]
- Pergantis, P.; Drigas, A. Sensory Integration Therapy as Enabler for Developing Emotional Intelligence in Children with Autism Spectrum Disorder and the ICT’s Role. Braz. J. Sci. 2023, 2, 53–65. [Google Scholar] [CrossRef]
- Milstein, N.; Gordon, I. Validating Measures of Electrodermal Activity and Heart Rate Variability Derived From the Empatica E4 Utilized in Research Settings That Involve Interactive Dyadic States. Front. Behav. Neurosci. 2020, 14, 148. [Google Scholar] [CrossRef] [PubMed]
- Cavallo, F.; Brubaker, H.; Brown, T. Utilizing Individual Z-Scores to Measure Efficacy of the World’s First Augmented Reality Glasses for Autism: A Single Case Study. J. Soc. Sci. Res. 2020, 1, 54–71. [Google Scholar]
- Guemghar, I.; Pires de Oliveira Padilha, P.; Abdel-Baki, A.; Jutras-Aswad, D.; Paquette, J.; Pomey, M.-P. Social Robot Interventions in Mental Health Care and Their Outcomes, Barriers, and Facilitators: Scoping Review. JMIR Ment. Health 2022, 9, e36094. [Google Scholar] [CrossRef]
- Rasouli, S.; Gupta, G.; Nilsen, E.; Dautenhahn, K. Potential Applications of Social Robots in Robot-Assisted Interventions for Social Anxiety. Int. J. Soc. Robot. 2022, 14, 1–32. [Google Scholar] [CrossRef]
- Dautenhahn, K.; Nehaniv, C.L.; Walters, M.L.; Robins, B.; Kose-Bagci, H.; Mirza, N.A.; Blow, M. KASPAR—A Minimally Expressive Humanoid Robot for Human–Robot Interaction Research. Appl. Bionics Biomech. 2009, 6, 369–397. [Google Scholar] [CrossRef]
- Aminuddin, R.; Sharkey, A.; Levita, L. Interaction with the Paro Robot May Reduce Psychophysiological Stress Responses. In Proceedings of the 11th ACM/IEEE International Conference on Human-Robot Interaction, Christchurch, New Zealand, 7–10 March 2016; pp. 593–594. [Google Scholar] [CrossRef]
- Law, M.; Jarrett, P.; Simpson, M.C.; Holtkamp, H.U.; Giglio, C.; Broadbent, E. The Effects of Interacting with a Paro Robot After a Stressor in Patients with Psoriasis: A Randomised Pilot Study. Front. Psychol. 2022, 13, 871295. [Google Scholar] [CrossRef]
- Doulou, A.; Pergantis, P.; Drigas, A.; Skianis, C. Managing ADHD Symptoms in Children Through the Use of Various Technology-Driven Serious Games: A Systematic Review. Multimodal Technol. Interact. 2025, 9, 8. [Google Scholar] [CrossRef]
- Maskey, M.; Lowry, J.; Rodgers, J.; McConachie, H.; Parr, J.R. Reducing Specific Phobia/Fear in Young People with Autism Spectrum Disorders (ASDs) through a Virtual Reality Environment Intervention. PLoS ONE 2014, 9, e100374. [Google Scholar] [CrossRef]
- Pergantis, P.; Bamicha, V.; Skianis, C.; Drigas, A. AI Chatbots and Cognitive Control: Enhancing Executive Functions Through Chatbot Interactions: A Systematic Review. Brain Sci. 2025, 15, 47. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| “Autism Spectrum Disorder” OR “ASD” OR “Assistive Technologies” OR “AT” OR “Emerging Technologies” OR “Stress” OR “Neurophysiological Stress” OR “Anxiety” AND “Autism Spectrum Disorder” AND (“Assistive Technologies” OR “AT”) AND (“Emerging Technologies”) AND (“Stress” OR “Neurophysiological Stress”) AND (“Anxiety”) AND “ASD” AND (“Assistive Technologies” OR “AT”) AND (“Emerging Technologies”) AND (“Stress” OR “Neurophysiological Stress”) AND (“Anxiety”) AND “Autism Spectrum Disorder” AND (“Assistive Technologies” OR “AT”) AND (“Emerging Technologies”) AND (“Neurophysiological Stress” OR “Physiological Stress” OR “Cortisol Levels” OR “Heart Rate Variability”) AND (“Anxiety” OR “Emotional Dysregulation” OR “Mental Health”) |
| Name | Type of Study | Subjects (Age, Gender, Diagnosis) | Intervention | Type of Technology | Measure | Results | Limitations | Effect Sizes | Longitudinal Effects | Country |
|---|---|---|---|---|---|---|---|---|---|---|
| [99] | Preliminary Study | 21 children with ASD, aged 4–16 years (16 boys, 5 girls) | Use of earmuffs and noise-canceling (NC) headphones | Earmuffs, NC headphones | Goal Attainment Scaling (GAS) T-scores | Earmuffs significantly improved Goal Attainment Scaling (GAS) T-scores compared to baseline. NC headphones showed improvement in some children but not significantly overall. Earmuffs were effective in reducing behavioral problems related to hyperreactivity to auditory stimuli. NC headphones were effective for some children but less consistent. | Small sample size; refusal of some participants to wear earmuffs or noise-canceling headphones; limited behavioral data for noise-canceling headphones; lack of control over variables like age, sex, general intelligence, functional level, and frequency of intervention; no examination of adverse or long-term effects; and exclusion of other sound isolation devices like earplugs. | Effect size was calculated with an alpha value of 0.05 and power of 80% for the Goal Attainment Scaling T-score; improvement was set to 1 for the sample size estimation. | No longitudinal effects were assessed; the study primarily focused on immediate behavioral changes using earmuffs and noise-canceling headphones. | Japan |
| [76] | Pilot Study | 14 boys, 3–8 years old, autism spectrum disorder (ASD) | Tell-show-do method + Visual Schedule System (test group) vs. Tell-show-do method (control group) | Visual Schedule System using picture communication symbols | Number of dental steps attempted, completion time per step, behavioral distress levels, physiological arousal (EDA) | Test group completed 1.38 more steps, 35.52 s faster per step, and 18.7% lower distress than the control group. | Small sample size (14 boys). Lack of statistical power to detect significant differences; intervention limited to a single method (visual pedagogy); potential rater bias, as intervention was clearly noticeable; children were not informed about upcoming appointments, which might have influenced anxiety levels. | Patients in the visual pedagogy group completed 1.38 more steps on average, completed steps 35.52 s faster per step, and displayed 18.7% lower levels of behavioral distress. Cohen’s d is not explicitly provided, but results indicate a notable clinical effect. | Limited by short study duration. No follow-up to assess long-term retention of improvements. Future research aims to explore more sensitive physiological stress indicators and broader participant demographics. | Canada |
| [88] | Multiple-Baseline, Single-Case Design | 4 students, aged 8–11 years, diagnosed with ASD | Use of visual schedules and work systems to increase on-task behavior in mainstream classrooms | low | Observations within a natural classroom environment | Visual schedules and work systems increased on-task behavior in all four students. Mixed results for secondary variables, with some showing reduced off-task behavior and increased productivity. On-task behavior increased from a baseline mean of 20–61% to 53–86% during intervention. Off-task behaviors showed moderate improvement but were not statistically significant. Productivity increased significantly in some students. | Small sample size (4 students); individual variability in teacher implementation of visual schedules and work systems; variability in baseline behaviors due to external classroom factors; limited generalizability due to specific participant demographics; fidelity of implementation was not consistent across all sessions; no follow-up sessions to confirm maintenance of behavior improvements. | Statistically significant improvements in on-task behaviors for three of the four students (Tau-U values ranging from 0.6458 to 1.25; p < 0.05); moderate improvements in productivity for two students (Tau-U = 0.7857, p = 0.0184 and Tau-U = 1.5, p = 0.0015). | A single maintenance probe was conducted for one student, showing decreased on-task behavior after intervention cessation. No broader longitudinal effects were assessed. | Australia |
| [87] | Alternating Treatments Single Case Research Design | 5-year-old male diagnosed with ASD | Weighted blanket and structured work boxes | low | Percentage of 10 s intervals of engagement | SWB resulted in consistently higher levels of engagement. Weighted blanket resulted in lower engagement, often similar to or less than baseline levels. | Single-subject design limits generalizability; short intervention duration (10 min sessions); possible novelty effect of weighted blanket intervention; lack of comparison to other evidence-based sensory interventions; limited reliability of teacher-reported engagement data; and no formal assessment of potential long-term benefits or harms of using weighted blankets. | No effect size was explicitly reported; visual analysis indicates structured work boxes (SWB) showed significant improvements in engagement, while the weighted blanket intervention demonstrated levels of engagement similar to or lower than the baseline. | No longitudinal effects were assessed; outcomes were limited to immediate responses during and after the short intervention period. | USA |
| [85] | Single-Subject Design | Two 4-year-old participants were diagnosed with autism | Weighted blanket intervention for 14 days | Weighted blankets | Objective sleep measures; caregiver surveys | Minimal changes in sleep patterns as a result of the weighted blanket intervention. Enhanced morning mood and significantly decreased time to fall asleep for participants. Findings suggest minimal changes in sleep patterns, enhanced morning mood, and decreased time to fall asleep. Not strong enough to recommend for clinical use. | Very small sample size (2 participants); convenience sampling from a medically underserved region; lack of blinding for caregivers; limited reliability of the Hello Sense Sleep app; potential for caregiver bias in self-reported measures; short intervention duration (14 days); and inability to generalize findings due to the single-subject design. | Effectiveness evaluated using Percentage of Non-Overlapping Data (PND). For participant 1 (John), PND for morning mood was 84% (effective); for participant 2 (Katie), PND for time to fall asleep and night wakings was 84% and 100%, respectively (effective). | No longitudinal effects were assessed; the study focused solely on immediate sleep behavior outcomes during the intervention period. | USA |
| [75] | Single-Subject Multi-Treatment Design | 6 children, aged 8–16 years, diagnosed with ASD | Use of in-ear (IE) and over-ear (OE) noise-attenuating headphones | In-ear (IE) and over-ear (OE) noise-attenuating headphones, Empatica E4 wristbands | Skin conductance levels (SCL), nonspecific skin conductance responses (NS-SCRs) | Noise-attenuating headphones led to a significant decrease in skin conductance levels (SCL) and frequency of nonspecific skin conductance responses (NS-SCRs). SCL and NS-SCR frequency significantly decreased between baseline and the first intervention phase. The intervention provided protection against the negative effects of environmental noise. | Small sample size (6 children); high dropout rate (50%); individual variability in electrodermal activity (EDA) responses; no tracking of ‘aware mode’ use in in-ear headphones; inability to generalize findings due to single-subject design; and limited data on broader environmental variables like specific noise types or frequencies. | Effect size not directly calculated; intervention showed significant reductions in skin conductance level (SCL) and nonspecific skin conductance responses (NS-SCR) frequency in the intervention phases compared to baseline (p < 0.05). | No longitudinal effects were assessed; the study focused on short-term outcomes during and immediately after the intervention. | USA |
| [68] | Clinical and Laboratory Experimental Study | 20 children, 6–10 years old, autism spectrum disorder (ASD) | Video Modeling Berkunjung ke Dokter Gigi (VM-BDG) vs. Visual Pedagogy Module Berkunjung ke Dokter Gigi (VPM-BDG) | Video Modeling (VM-BDG), Visual Pedagogy Module (VPM-BDG) | Delta salivary cortisol levels before and after intervention | Both VM-BDG and VPM-BDG effectively reduced stress levels; no significant difference between the interventions. | Small sample size (20 children); no control group without intervention; limited generalizability due to strict inclusion criteria; salivary cortisol measurement may be influenced by external factors; short duration between pre- and post-intervention saliva collection. | Delta salivary cortisol values showed a reduction in stress for both interventions; no statistically significant differences between VM-BDG and VPM-BDG. Both interventions were equally effective in reducing stress but lacked a control comparison for baseline reference. | Short study duration with no long-term follow-up. No assessment of sustained stress reduction over multiple visits. Future research should explore broader demographics and extended data collection periods. | Indonesia |
| [69] | Clinical Experimental Study | 20 children, 6–10 years old, Autism Spectrum Disorder (ASD) | Video Modeling vs. Visual Pedagogical Module | Video Modeling, Visual Pedagogical Module (PV-BDG) | Salivary Immunoglobulin A (sIgA) levels before and after intervention | Both methods reduced stress levels as measured by sIgA; no significant difference between the groups. | Small sample size (20 children); no significant difference in stress reduction between the two interventions; limited generalizability due to specific participant criteria; no control group without intervention; external factors influencing saliva IgA levels were not controlled. | sIgA levels increased after video modeling but decreased with the PV-BDG module; no significant difference in ΔsIgA levels between the two groups; clinical effectiveness was observed but lacks strong statistical significance. | Short study duration with no long-term follow-up; further research is needed to assess sustained stress reduction effects. Future studies should include broader demographics and additional physiological stress markers. | Indonesia |
| [74] | Retrospective Follow-up Study | 85 individuals: 48 children aged ≤17 (57%), 37 adults ≥ 18 years (44%), diagnosed with ADHD and/or ASD | Use of weighted blankets | Weighted blankets (chain-weighted and ball-weighted) | Self-reports via telephone interviews | Weighted blankets improved falling asleep, sleeping through the night, and relaxing during the day. They also improved morning and evening routines, including preparing/going to sleep and waking up. Also, 59% reported improved ability to fall asleep, 81% reported improved sleeping through the night, and 45.8% reported improved daily routines. | Small sample size (8 families); non-randomized design; data collection interruptions due to technological issues; limited diversity in family demographics; inability to capture nuanced stress triggers beyond predefined survey options; and no assessment of real-world generalizability of findings. | Medium to large effect sizes were observed for SCR features (Cohen’s d ranging from 0.59 to 2.67) during stress episodes, indicating strong associations between physiological signals and self-reported stress. | No longitudinal effects were assessed; the study focused solely on immediate stress patterns during a short data collection period. | Sweden |
| [77] | Experimental Study | 83 children (75 males; 8 females), 7–12 years old, autism spectrum disorder (ASD) | Development and validation of noise-canceling headphones with aural perception tuning | Hybrid Active Noise Cancelation (ANC) system with EEG-based sound perception tuning | Subjective aural perception ratings, EEG signals for neural responses | Headset effectively reduced auditory hyperreactivity; unpleasant frequencies (250 Hz, 8 kHz) were identified, and noise cancelation improved participants’ aural comfort. | Small sample size (83 ASD and 50 TD children); subjective aural perception ratings may introduce bias; external noise factors could impact ANC effectiveness; study limited to specific frequencies (250 Hz–8 kHz); lack of long-term usability testing in real-world environments. | Significant reduction in unpleasant sound perception with ANC headset; frequencies of 250 Hz and 8 kHz were rated as most unpleasant; aural perception ratings significantly correlated with EEG neural responses; different ASD clusters exhibited unique auditory response profiles. | No long-term follow-up on adaptation and behavioral impact; ANC effectiveness in daily settings remains uncertain. Future studies should assess sustained benefits and individual long-term auditory adaptation. | China |
| [84] | Observational Study | 9 patients with ASD (4 boys; 5 girls), aged 8–19 years | Interaction with PARO, a baby harp seal-type therapeutic robot | PARO, baby harp seal-type therapeutic robot | Observation of patient interactions with PARO | Effective for some patients in developing good communication and reducing impulsive behaviors or anxiety. Some patients did not like PARO due to its features, like big eyes or drive noise. Some patients treated PARO like a real animal, which helped in communication and reducing anxiety. Other patients disliked PARO for its features. | Small sample size (9 patients); lack of objective indices for measuring effectiveness; potential influence of other concurrent treatments; results may be due to temporary changes in emotional state rather than PARO itself; limited generalizability due to narrow demographic diversity. | Effect size not calculated; observational data indicated some positive changes but lacked quantitative analysis. | No longitudinal effects were assessed; the study focused on short-term behavioral and emotional changes observed during interaction with PARO. | Japan |
| [86] | Pilot Study with Mixed Methods (Quantitative-Qualitative) | 9 children, aged 6–16 years, diagnosed with ASD | Interaction with semi-autonomous parrot-inspired robot KiliRo using the Adapted Model-Rival Method (AMRM) Semi-autonomous parrot-inspired robot | Semi-autonomous parrot-inspired robot (KiliRo) | Facial expressions (Oxford emotion API), informal and semi-formal interviews, closed-format questionnaire | Children appeared attracted and happy to interact with KiliRo. AMRM may help improve learning and social interaction abilities. Participants showed increased happiness and engagement over the study period. Positive feedback from parents, pediatricians, and psychologists on robot’s potential. | Small sample size (9 children); short duration of intervention (5 days); simulated autonomy of the robot limits ecological validity; potential bias in qualitative interviews due to group settings; limited diversity in participant demographics; absence of control group for comparison. | Effect size was not explicitly calculated; qualitative and descriptive analyses provided positive indications of emotional engagement and social interaction. | No longitudinal effects were assessed; the focus was on immediate responses and interaction patterns during the short intervention period. | India |
| [67] | Cross-cultural Evaluation with Randomized Controlled Trial | 89 children with high-functioning ASC, aged 6–9 years (Israel: 38, Sweden: 36, UK: 15) | Use of Emotiplay serious game for emotion recognition training | Internet-based serious game (Emotiplay) | Emotion recognition tasks (face, voice, body, integrative), SRS-2, VABS-II Socialization scale | Significant improvements in emotion recognition across face, voice, body, and integrative tasks. Parents reported reduced autism symptoms and improved socialization in Israel and Sweden. Children using Emotiplay showed significant improvements in emotion recognition and social skills compared to controls. Parents in Israel reported reduced autism symptoms. | Variation in intervention protocols across countries (UK, Israel, Sweden); inconsistent parental involvement; dropout rates due to lack of motivation and technical issues; potential cultural biases in emotion recognition tasks; short duration of intervention (8 weeks); reliance on parental reporting for generalization and socialization outcomes; and lack of active control groups in certain study sites. | Significant effect sizes were reported for emotion recognition improvements in the intervention group: η2 = 0.20 for body tasks, 0.40 for integrative tasks, and 0.30 for country-level differences (MANOVA results). | No longitudinal effects were assessed; improvements were only measured immediately post-intervention with no follow-up period. | UK, Israel, Sweden |
| [78] | Matched Controlled Exploratory Study | 24 children (14 experimental group, 10 control group), 5–8 years old, autism spectrum disorder (ASD), IQ ≥ 60 | GOLIAH (Gaming Open Library for Intervention in Autism at Home) platform combined with Treatment As Usual (TAU) for 6 months | Automated serious gaming platform (GOLIAH) targeting joint attention and imitation tasks | Performance metrics in imitation and joint attention games; ADOS scores, Vineland socialization, Parenting Stress Index (PSI), Child Behavior Checklist (CBCL) | Improvement in imitation and joint attention performance within GOLIAH games; no significant differences in core ASD symptoms compared to the control group (TAU alone); no increase in parental stress. | Small sample size (14 experimental, 10 control); no randomization due to parental motivation selection; observance rate lower than expected; limited generalizability due to strict inclusion criteria; no web-based version of GOLIAH available at the time of the study. | Significant improvement in 4 out of 6 imitation games; 3 out of 4 joint attention games showed reduced reaction times; no significant group × time interaction for clinical measures; improvements in Vineland socialization, CBCL scores, and parental stress observed in both groups. | No long-term follow-up conducted; study suggests potential for larger randomized controlled trials; future research to focus on younger children and web-based implementation of GOLIAH. | France, Italy |
| [91] | Pilot Study | 10-year-old boy with mild autism, 6-year-old neurotypical boy | Use of wearable sensors and social robots for detecting and mitigating meltdowns | Wearable sensors (Empatica E4 wristband), social robots (PARO, toy train) | Physiological signals (HR, EDA, movement), video observations | Wearable sensors effectively detected physiological changes correlating with meltdowns. Sensors on the wrist and ankle showed similar responses. Social robots helped in calming the child. Effective detection of physiological changes during meltdowns. Social robots were effective in calming the child. | Small sample size; pilot study design limits generalizability; sensor placement (wrist vs. ankle) needs further investigation; no long-term data on effectiveness; limited diversity in participant demographics; challenges in controlling for external variables like environmental stimuli. | Effect size not directly calculated; study focused on the correlation of physiological signals (EDA, BVP, accelerometer) with challenging behaviors. | No longitudinal effects were assessed; the focus was on real-time detection of challenging behaviors and immediate intervention possibilities. | Qatar |
| [65] | Controlled Trial | 94 children, 6–12 years old (86 males; 8 females), autism spectrum disorder (ASD) with IQ ≥ 60 | 28-session virtual reality-enabled program using an immersive half-CAVE system to train emotional regulation and social adaptation | Immersive virtual reality (CAVE environment with non-intrusive motion tracking) | Emotion regulation (PEP-3 Affective Expressions), social interaction (PEP-3 Social Reciprocity), emotion recognition (Faces and Eyes Tests), adaptive skills (ABAS-II) | Significant improvement in emotion expression (p = 0.037) and social reciprocity (p = 0.007); no significant changes in emotion recognition or adaptive skills. | Small sample size (94 children); lack of randomization due to parental selection; no follow-up assessments beyond training period; limited generalizability to diverse ASD populations; no comparison with other VR-based training programs. | Significant improvements in emotion expression and regulation (p = 0.037); social reciprocity scores increased significantly (p = 0.007); no significant changes in emotion recognition (p = 0.666); mixed findings on adaptive skills improvements. | No long-term follow-up was conducted; future studies recommended to assess sustained behavioral improvements; need for broader participant demographics and comparisons with alternative training methods. | China |
| [90] | Single-Subject Study | One 13-year-old male student diagnosed with autism | Smartglasses-based socio-emotional learning intervention using the Empowered Brain system | Smartglasses (Google Glass), Empowered Brain system | Educator logs, video interviews | Educators found the intervention practical and easy to implement. The student demonstrated improved verbal and nonverbal communication skills. No adverse effects on the classroom environment. Positive impact on student’s social communication skills. Educators found the technology practical and usable without causing distractions in the classroom. | Single-subject design; limited to one 13-year-old male participant with autism; absence of quantitative validated outcome measures; short intervention period (2 weeks, 16 sessions); findings cannot be generalized due to the specificity of the sample; teacher-reported improvements lack independent verification. | Effect size was not calculated; qualitative teacher-reported improvements in social interaction, eye contact, and classroom participation were observed. | No longitudinal effects were assessed; the study focused on immediate teacher-reported outcomes during the two-week intervention. | USA |
| [72] | Waitlist Control Design | 94 children, mean age 106.3 months (88.9% boys, 11.1% girls), all diagnosed with ASD | VR-based social skills training | Virtual Reality | PEP-3 Affective Expressions and Social Reciprocity | Children showed improved emotional expression, regulation, social interaction, and adaptation post-training, indicating VR training’s effectiveness. | Large dropout rate (approximately 20%); limited diversity in demographics (primarily from Hong Kong); difficulty with logistics and scheduling due to reliance on a large, stationary CAVE VR system; some children refused initial participation due to discomfort with VR goggles; absence of long-term data to assess the sustainability of improvements. | Significant effect sizes for improvement in emotional expression and regulation (partial η2 = 0.069, p = 0.025) and social reciprocity (partial η2 = 0.100, p = 0.007). | No longitudinal effects were assessed; outcomes were measured immediately post-intervention with no follow-up. | China |
| [80] | Experimental Study | 38 children (22 with ASD, 16 without ASD), ages not specified | Machine learning models (SVM, logistic regression) trained on wearables data to differentiate stress and rest states | Consumer-grade wearable device with machine learning algorithms | Heart rate (HR) and RR interval data; accuracy of machine learning models | SVM achieved 93% accuracy; logistic regression achieved 87% accuracy in differentiating stress vs. rest states; similar performance for both ASD and non-ASD groups. | Balanced dataset (equal rest and stress samples) may not reflect real-world class imbalance; small sample size (38 participants); study conducted in a controlled setting, limiting generalizability; movement-induced physiological changes that are not fully accounted for. | The SVM model achieved 93% accuracy; the logistic regression model achieved 87% accuracy; high F1 scores (above 0.84) for stress detection in the ASD group; model performance was stable across ASD and non-ASD groups. | No long-term follow-up to assess real-world applicability. Further research is needed to test effectiveness in social settings. Future studies should address class imbalance in real-world stress exposure scenarios. | USA |
| [96] | Mixed-Methods Exploratory Study | 31 autistic children, 6–16 years old, with autism spectrum disorder (ASD) | Exploration of preferences and usability of three VR head-mounted displays (HTC Vive, ClassVR, Google Cardboard) in school settings | Virtual reality head-mounted displays (HMDs): HTC Vive, ClassVR, Google Cardboard | Questionnaire responses on device preference, enjoyment, physical comfort, and potential uses of VR in classrooms | HTC Vive was most preferred due to the immersive experience, while ClassVR was least preferred; children reported high enjoyment, comfort, and interest in VR for calming, preparing for real-world events, and learning. | Small sample size; limited diversity in participants; narrow age range (6–16 years old); diverse devices with varying functionalities potentially skewed results; lack of longitudinal assessment; only partial utilization of device capabilities; limited software comparability across devices; and subjective preference data. | Effect size not explicitly calculated; results highlighted high preference rates for interactive VR devices (e.g., HTC Vive) over lower-tech options. | No longitudinal effects were assessed; the study focused on the immediate usability and preferences of VR devices. | United Kingdom |
| [98] | Experimental Study | 40 children, 8–15 years old, with autism spectrum disorder (ASD) | Virtual reality distraction (VR) during routine non-invasive dental treatments compared to conventional behavior management | Virtual reality (VR) eyeglasses with visual and auditory stimuli | Venham’s Picture Test (anxiety), Frankel’s Behavior Rating Scale (behavior) | Significant reduction in anxiety (p = 0.037) and improvement in dental behavior (p = 0.0001) when VR distraction was used. | Small sample size (40 children completed both visits); high dropout rate (58.8%); no randomization due to practical constraints; anxiety and behavior scores may be influenced by prior exposure to dental teams; no physiological stress biomarkers were measured. | Statistically significant reduction in anxiety scores (p = 0.037); significant improvement in behavior rating (p = 0.0001); negative correlation between anxiety and behavior scores (p < 0.001), indicating VR distraction had a positive impact. | No long-term follow-up beyond the second dental visit; future studies should explore extended intervention effects; larger randomized trials are needed to validate VR distraction as a sustained behavior management tool. | India |
| [83] | Feasibility and Usability Study | 3 families, children aged 6–10 years old, autism spectrum disorder (ASD) | New Horizon Serious Game designed for stress and anxiety reduction with relaxation mini-games; parent app SpaceControl for monitoring gaming behavior | Serious Game (mobile-based), relaxation techniques (guided imagery and focused breathing), supporting parent app | Children’s mood (Likert scale), SCAS (Spence Children Anxiety Scale), SCAS-P (Parent version), gaming behavior logs | Positive feedback from parents and children. The game showed potential for reducing stress and anxiety, but the results were preliminary due to the small sample size. | Small sample size (3 families); imited generalizability due to pilot study nature; no objective stress biomarkers measured; game impact on actual stress reduction remains unclear; short testing period restricts behavioral adaptation assessment. | Preliminary positive trends were observed in SCAS and SCAS-P scores; no statistically significant effect sizes due to a small sample; parental feedback suggested potential improvements in relaxation effects; engagement levels varied among children. | No long-term follow-up was conducted; future studies aim to assess sustained use over extended periods; need for larger sample size to evaluate longitudinal effectiveness in stress management. | Belgium |
| [95] | Comparative Study | 24 children (mean age = 42.62 months; 12 with ASD, 12 with LD) | Use of a wearable heart rate measurement device during interactive activities | Wearable heart rate measurement device (thoracic belt with ECG sensors) | Heart rate (HR) monitoring | HR was significantly higher in children with ASD compared to those with LD during interactive activities. Increased HR correlated with autism severity. | Small sample size (24 children) with a high dropout rate (55.6%); potential biases in interpretation due to unbalanced gender representation; short duration of interactive activities limiting comprehensive HR analysis; reliance on ADOS-2 for stress correlation may miss nuanced non-social stressors; and technical limitations of the wearable device leading to signal inconsistencies in certain activities. | Significant effect sizes were observed for HR differences during stress-inducing activities (ADOS-2 bubble play: Cohen’s d = 0.93, p = 0.026; anticipation of routine: Cohen’s d = 1.06, p = 0.012), indicating strong stress responses in children with ASD. | No longitudinal effects were assessed; the study focused solely on short-term physiological responses to structured activities. | Italy |
| [70] | Pilot Study | 6 participants diagnosed with ASD, aged 16–19 years | Use of SoundFields, a virtual reality game with binaural-based spatial audio | Virtual reality game (SoundFields) with binaural-based spatial audio | Self-reported anxiety scores, tracked voluntary interaction time | Significant decrease in anxiety linked to target auditory stimuli after four weeks of intervention. Participants actively engaged and enjoyed the VR environment. Decreased anxiety towards target stimuli, increased voluntary interactions with target auditory stimuli, and positive engagement with the VR environment. | Small sample size (6 participants); lack of a control group to compare results; short intervention duration (4 weeks); potential biases in self-reported anxiety scores; no measures of generalization to real-world auditory hypersensitivity; and reliance on subjective outcome measures rather than physiological or objective behavioral data. | The effect size was not explicitly calculated; the Wilcoxon signed-rank test indicated a significant decrease in self-reported anxiety scores (p = 0.026). | No longitudinal effects were assessed; focus was limited to immediate post-intervention outcomes without follow-up evaluations. | UK |
| [100] | Preliminary Controlled Trial | 5 children, 4–8 years old (4 males; 1 female), autism spectrum disorder (ASD) | Virtual reality-based air travel training (VR-ATT) with social stories and real-world air travel rehearsal | Google Cardboard VR with iPhone X and narrative-based functional communication activities | Parent-rated air travel ability questionnaire (Likert scale) and clinical activity rubric during intervention | 4 out of 5 participants improved by at least 2 points in air travel ability; no significant statistical changes due to the small sample size. | Small sample size (5 children); no control group for comparison; short intervention period (3 weeks); individual differences in VR engagement levels; parent-reported improvements lack objective physiological validation. | Improvement in air travel skills reported by parents; activity completion rubric showed increases in task performance; no statistically significant differences in pre- and post-training scores (p = 0.0625). | No long-term follow-up conducted; future studies are recommended to evaluate real-world transferability; need for a larger sample size and an extended intervention period. | USA |
| [89] | Feasibility Study | One 10-year-old male child diagnosed with ASD | Use of wearable sensors and social robots to detect challenging behaviors | Wearable sensors (Empatica E4) and social robots (Nao, PARO) | Physiological signals (HR, EDA, IBI, TEMP, BVP), acceleration | Physiological signals combined with kinetic measures led to more accurate predictions of challenging behaviors. Best machine learning model achieved 97% accuracy. Heart rate and interbeat interval were significant predictors of challenging behaviors. Physiological features outperformed kinetic features in prediction accuracy. | Single-subject design (10-year-old male); limited generalizability to other populations; reliance on manually annotated challenging behaviors; absence of long-term or repeated sessions; wearable discomfort or potential harm to the child not thoroughly explored; and the model’s dependency on lab settings for data collection. | High accuracy reported for combined physiological and kinetic data (97%) using an MLP classifier; effect size not explicitly calculated, but performance metrics indicated strong model reliability. | No longitudinal effects were assessed; the study was limited to single-session outcomes in a controlled lab environment. | Qatar |
| [92] | Mixed Methods (Quantitative-Qualitative) ABAB Design | 9 children, aged 8–12 years, diagnosed with ASD | Interaction with robot KASPAR and usual care with teacher | Semi-autonomous humanoid robot (KASPAR) | Micro behaviors, attention metrics, video recall interviews | Children showed significantly more nonverbal imitation, touched the robot more often, maintained attention longer, and were less distracted during KASPAR sessions compared to teacher sessions. KASPAR was able to make contact with children, hold their attention longer, and engage them in more nonverbal interactions compared to teachers. | Small sample size (9 children); limited generalizability due to the controlled and artificial study setting; absence of long-term follow-up; potential novelty effect of KASPAR; variation in teacher engagement approaches; and limited individual customization of KASPAR for each child’s specific needs. | Significant effect sizes were reported for specific micro-behaviors: non-verbal imitation (r = 0.589), touching KASPAR (r = 0.405), and maintaining attention (r = 0.545), demonstrating moderate to large effects. | No longitudinal effects were assessed; the study was limited to immediate outcomes over four weeks with no follow-up evaluations. | Netherlands |
| [66] | Pilot Randomized Controlled Trial | 38 children with ASD, aged 8–18 years, IQ > 50 | Use of Anxiety Meter (wearable, real-time anxiety detection technology) with diaphragmatic breathing training | Wearable sensors (Shimmer2) and a tablet display | Proportion of participants initiating deep breathing, heart rate, respiration rate and amplitude, self-reported anxiety | Participants using the Anxiety Meter were more likely to initiate deep breathing and reported feeling calmer. Feedback from the Anxiety Meter increased the likelihood of initiating deep breathing in response to anxiety. | Relatively small sample size (28 children); short intervention period (4 visits); imbalances in IQ and sex between treatment and control groups; controlled-laboratory setting limits real-world generalizability; potential confounding factors such as participant familiarity with stress-eliciting tasks; and reliance on self-reported measures of anxiety reduction and relaxation initiation. | Significant group differences in initiating relaxation techniques: Odds Ratio (OR) = 2.00 (95% CI = [0.340, 1.046], p = 0.001). The effect size for physiological signal improvements was not explicitly calculated. | No longitudinal effects were assessed; study outcomes were limited to immediate responses during and after the intervention sessions. | Canada |
| [82] | Pilot Study | 20 children with ASD, aged 7–13 years (14 boys; 6 girls) | Use of autism hug machine portable seat (AHMPS) with inflatable wrap and manual pull | Autism hug machine portable seat (AHMPS) with inflatable wrap and manual pull | Conners’ Parent Rating Scale-48 (CPRS-48), Galvanic Skin Response (GSR) | Conduct problems significantly decreased in the inflatable group (p = 0.007) compared to the manual pull group. Significant reduction in sympathetic response (p = 0.01) only in the inflatable group. AHMPS with inflatable wrap effectively reduced emotional arousal and neurobiological stress in children with ASD. Conduct problems decreased more in the inflatable wrap group compared to the manual pull group. | Small sample size (20 children); short duration of intervention (3 weeks); limited demographic diversity (Javanese children only); results potentially influenced by parents’ subjective ratings; no evaluation of long-term sustainability of behavioral changes; and absence of data on the broader applicability of the portable hug machine in different environments. | Medium effect size was observed for stress reduction in the inflatable wrap group (ηp2 = 0.396), indicating moderate effectiveness; a small effect size for the manual pull group (ηp2 = 0.09). | No longitudinal effects were assessed; the study focused on immediate outcomes within the 3-week intervention period. | Indonesia |
| [93] | Experimental Study | 21 children, 2–12 years old, ASD | Robot-based intervention using the Kaspar robot combined with physiological monitoring (BVP signals) and facial emotion analysis | Empatica E4 wristband (physiological monitoring), OpenFace toolkit (facial emotion detection) | Blood volume pulse (BVP), HRV (LF and HF power), facial emotion annotations as stress verification | Overall, children were not stressed during Kaspar robot interactions; stress declined during sessions for some children, as verified by facial emotion analysis. | Small sample size (21 children); lack of real-time data processing; reliance on lab-based settings limits ecological validity; contradictory results between LF and HF stress metrics in certain sessions; no data on individual differences in stress sensitivity; and limited diversity in demographics (participants mostly from specific regions). | Effect size not explicitly calculated; descriptive and session-wise analyses showed reduced stress levels during robot-based interactions, as indicated by decreasing LF and increasing HF values in many cases. | No longitudinal effects were assessed; results were based on session-specific outcomes without follow-up evaluations or broader assessments. | Turkey, Macedonia, United Kingdom, Poland |
| [73] | Pilot Study | 10 children and teenagers, 8–16 years old, with autism spectrum disorder (ASD) | ShopAut 2.0, a 3D personalized serious game for training shopping activities with pre- and post-real-life supermarket assessments | 3D Serious Game (ShopAut 2.0) with personalized training and individualized features for ASD severity levels | ICF-CY form scores (real-life shopping tasks), Vineland Adaptive Behavior Scale II (VABS-II) | Significant improvements in daily living skills, particularly in shopping procedures, attention, self-control, and problem-solving; VABS-II scores improved in communication, daily living skills, and socialization. | Small sample size (10 ASD participants); no control group for comparison; short intervention period (10 sessions); real-world shopping environment not tested beyond one location; no assessment of long-term retention of skills. | Significant improvements (p < 0.05) in shopping procedure, attention, and problem-solving skills; VABS-II scores showed enhanced daily living skills; statistically significant differences in pre- and post-training ICF-CY scores. | Short-term follow-up (6 months) showed sustained improvements; no data on long-term generalization beyond training period; future studies to explore extended intervention and broader sample sizes. | Italy |
| [94] | Mixed-Methods Design | Phase 1: 40 adults (20 with ASD, 20 without ASD); Phase 2: 10 adults with ASD presenting CB; Phase 3: 1 adult with ASD exhibiting CB | Development and validation of smart wearable shirt (SWS) for real-time prediction of challenging behaviors (CBs) | Smart wearable shirt (Hexoskin SWS) | Physiological parameters (HR, HRV, respiratory rate), behavioral diary | Higher stress levels anticipated in adults with ASD when exposed to stressors. The system was expected to predict CBs with high accuracy using physiological parameters. Higher stress levels were detected in adults with ASD compared to typically developed peers. The system was anticipated to predict CBs with an AUC value above 0.70. | Very small sample size for proof-of-concept phase (1 participant); limited generalizability due to lab-based controlled settings; lack of validated stimuli to elicit consistent stress responses; short duration of study phases (7 days for Phase 2 and proof-of-concept); and the technology’s reliance on stable Bluetooth and internet connections may not suit all environments. | Effect size for prediction accuracy not explicitly calculated; expected AUC > 0.70 (fair sensitivity) for predicting challenging behaviors using machine learning models. | No longitudinal effects were assessed; the study focused on short-term proof-of-concept outcomes and immediate data-driven predictions of challenging behaviors. | Israel |
| [81] | Experimental Study | 5 male children, aged 7–10 years, diagnosed with ASD | Use of wearable sensors to monitor physiological and kinetic data during interactions | Wearable sensors (Empatica E4), social robots (Nao, PARP) | Heart rate, HRV (RMSSD), acceleration, electrodermal activity, temperature, blood volume pulse | The XGBoost algorithm achieved the best performance, with 99% accuracy in detecting challenging behaviors. Heart rate was the main contributing feature. RMSSD correlated with challenging behaviors. Heart rate (HR) was the most significant feature for detecting challenging behaviors. Physiological features outperformed kinetic features in prediction accuracy. | Very small sample size (5 male children); limited generalizability due to controlled lab environment; manual annotation of challenging behaviors introduces potential human error; no consideration of gender differences; limited long-term data; and reliance on a single wearable sensor, which might miss multi-modal behavioral cues. | High accuracy (99%) was achieved using the XGBoost algorithm for predicting challenging behaviors based on physiological data; effect size was not explicitly reported, but high-performance metrics indicate strong model reliability. | No longitudinal effects were assessed; the study focused on immediate data-driven predictions without long-term monitoring or evaluations. | Qatar |
| [71] | Combined 3 (intervention) × 3 (diagnosis) × 3 (time) research design with repeated measures | 201 families (parents and children), children aged 6–12 years (neurotypical, ADHD, ASD) | Serious game (Kairos) and parental support | Serious game (Kairos) on electronic tablets | Routine Achievement Assessment Tool | For ADHD participants, a significant clinical effect was observed for parental support and a combination of Serious Game and parental support. For ASD children, an effect was observed for a combination of Serious Game and parental support. For neurotypical children, a significant effect was observed for Serious Game alone. Serious Game can improve children’s routines. For ADHD and ASD children, adding parental support produces greater clinical improvements. | Significant COVID-19-related methodological adjustments (e.g., allowing parents to choose routines, inconsistent study conditions); lack of standardization in parental support implementation; sample attrition due to pandemic (10%); and variability in reported results due to differences in routines chosen by parents. | For autistic children, significant improvements in routine achievement when using combined intervention (Serious Game and parental support): huge clinical effect (Cohen’s d = 2.81) over 8 weeks. For ADHD children, parental support alone yielded a large clinical effect (Cohen’s d > 1.2) in the first 4 weeks. | Moderate persistence of effects in neurotypical children but decline observed in ADHD and ASD groups after initial improvement. No formal follow-up data to assess longer-term | Canada |
| [79] | Feasibility Study | 8 families, 8 autistic boys (mean age: 9.92 years), caregivers (mean age: 44.5 years) | Self-report stress logging and physiological signal measurement using a mobile app and wearable sensors | Mobile app (EasyConnect) and wearable physiological sensors (Empatica E4) | Self-reports, PPG, and EDA signals | Caregivers and children were able to use the mobile app and sensors effectively to report and measure stress in daily life. Stress indicators from EDA were aligned with self-reports. | Small sample size (8 families); Some families did not use the app despite training; wearable device discomfort, particularly for autistic children; limited options in the stress-reporting questionnaire; external validity concerns due to natural settings. | Medium and large effect sizes were observed in EDA SCR features; higher and wider SCR peaks were found in both autistic children and caregivers during stress-reporting periods; Cohen’s d values for stress detection in caregivers were notably high (up to 2.67). | Limited due to the short study duration; no extended follow-up was conducted; future research aims to recruit more families and expand data collection for longitudinal analysis. | USA |
| [97] | Comparative Survey Study | 129 children (53 autistic, 76 neurotypical) aged 3–16 years | Use of fidget toys and fidget spinners | Fidget toys and fidget spinners | Parental survey, Sensory Profile Questionnaire 2 (SPQ 2) | Parents of autistic children perceived fidget toys and spinners as more beneficial compared to NT parents. Higher sensory-seeking scores were associated with greater perceived benefits and reduced anxiety. Autistic children with higher sensory-seeking scores were seen to benefit more from fidget toys in terms of reduced anxiety and increased concentration. NT children with higher sensory-seeking scores also showed similar benefits. | Limited generalizability due to parent-reported data; cultural biases in sensory perception and educational environments; inconsistent frequency and type of fidget toy use between autistic and NT children; small sample sizes for certain subgroup analyses; absence of longitudinal data on sustained outcomes; and potential biases influenced by school policies or media portrayals. | Significant group differences in perceived benefits of fidget toys for anxiety reduction and concentration improvement: χ2 (4) = 17.478, p = 0.002 and χ2 (4) = 16.148, p = 0.003, respectively. | No longitudinal effects were assessed; the study focused on cross-sectional parental perceptions without follow-up data. | UK |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pergantis, P.; Bamicha, V.; Doulou, A.; Christou, A.I.; Bardis, N.; Skianis, C.; Drigas, A. Assistive and Emerging Technologies to Detect and Reduce Neurophysiological Stress and Anxiety in Children and Adolescents with Autism and Sensory Processing Disorders: A Systematic Review. Technologies 2025, 13, 144. https://doi.org/10.3390/technologies13040144
Pergantis P, Bamicha V, Doulou A, Christou AI, Bardis N, Skianis C, Drigas A. Assistive and Emerging Technologies to Detect and Reduce Neurophysiological Stress and Anxiety in Children and Adolescents with Autism and Sensory Processing Disorders: A Systematic Review. Technologies. 2025; 13(4):144. https://doi.org/10.3390/technologies13040144
Chicago/Turabian StylePergantis, Pantelis, Victoria Bamicha, Aikaterini Doulou, Antonios I. Christou, Nikolaos Bardis, Charalabos Skianis, and Athanasios Drigas. 2025. "Assistive and Emerging Technologies to Detect and Reduce Neurophysiological Stress and Anxiety in Children and Adolescents with Autism and Sensory Processing Disorders: A Systematic Review" Technologies 13, no. 4: 144. https://doi.org/10.3390/technologies13040144
APA StylePergantis, P., Bamicha, V., Doulou, A., Christou, A. I., Bardis, N., Skianis, C., & Drigas, A. (2025). Assistive and Emerging Technologies to Detect and Reduce Neurophysiological Stress and Anxiety in Children and Adolescents with Autism and Sensory Processing Disorders: A Systematic Review. Technologies, 13(4), 144. https://doi.org/10.3390/technologies13040144