

Understanding Technology Perception in Autism with Separate Analyses for Anxiety and Depression Using Quantum Circuit Simulation Approach †


 , ,
, ,  and
and
Abstract
1. Introduction
1.1. Co-Occurrence of Anxiety and Depression in ASD
1.2. Perception of Technology in ASD, Anxiety, and Depression
1.3. Challenges of Co-Morbidity: Anxiety and Depression in ASD
1.4. Technological Intervention for Emotional Regulation
1.5. The Role of Quantum Computing in Collaborative AI
2. Materials and Methods
2.1. Objective of the Study
2.2. Data Collection
2.3. Measuring Instruments
2.4. Statistical Methods
2.5. Reliability and Internal Consistency Analysis
2.6. Factor Analysis
2.7. Quantum Algorithms
3. Results
3.1. Parametric and Non-Parametric Statistical Analysis
3.2. Pearson Correlation Analysis for ASD, ASD and CA and, and ASC and CD
3.3. Reliability and Consistency Analysis
3.4. Quantum Associative Memory Algorithm
- A1. Difficulties in understanding and expressing themselves through written language;
- A2. Difficulties in learning how to do simple things when receiving personal help or assistance;
- A3. Difficulties in carrying out complex tasks when receiving personal help or assistance.
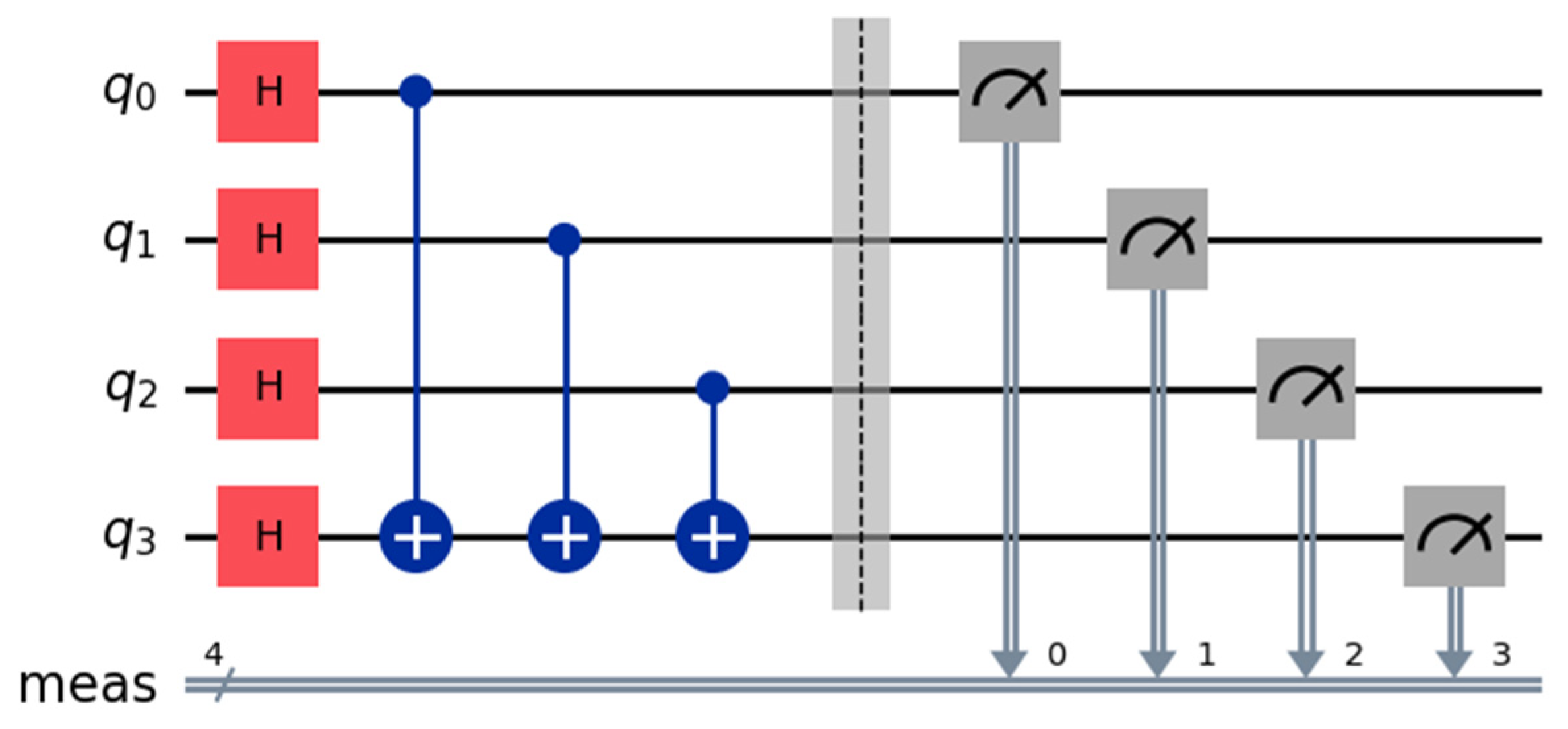
- Hadamard gates (H) initialize qubits in a superposition;
- CNOT gates (with a point) represent the interactions between the independent and dependent variables;
- Measurement gates (M) measure the final state of the qubits.
- # Create a quantum circuit with 4 qubits
- qc = QuantumCircuit(4)
- # Apply Hadamard gates to each qubit
- qc.h(0)
- qc.h(1)
- qc.h(2)
- qc.h(3)
- # Apply CNOT gates with qubits 0, 1, and 2 as controls and qubit 3 as the target
- qc.cx(0, 3)
- qc.cx(1, 3)
- qc.cx(2, 3)
- # Add measurement to all qubits
- qc.measure_all()
- # Draw the circuit
- qc.draw(“mpl”)
4. Discussion
4.1. Future Patterns in New and Emerging Technologies to Treat ASD and Concomitant Developmental Conditions Such as Anxiety and Depression
4.2. Limitations of the Study
5. Conclusions
Suggestions for Future Developments
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- WHOQOL-Measuring Quality of Life|The World Health Organization. Available online: https://www.who.int/tools/whoqol (accessed on 6 December 2023).
- Martínez, V.T.P.; Montero, O.A.A. Necesidades de aprendizaje de los especialistas de Medicina General Integral sobre los trastornos del espectro autista. Rev. Cuba. Med. Gen. Integral. 2013, 29, 267–280. [Google Scholar]
- Oreskovic, N.M.; Neumeyer, A.M.; Duggan, M.P.; Kuhlthau, K.A. Assessment of Walking Routes as a Possible Approach for Promoting Physical Activity in Children with Autism Spectrum Disorder: Brief Report. Dev. Neurorehabilit. 2020, 23, 59–63. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, J.P.; Toscano, C.V.A.; Rodrigues, A.M.; Furtado, G.E.; Barros, M.G.; Wanderley, R.S.; Carvalho, H.M. Effects of a Physical Exercise Program (PEP-Aut) on Autistic Children’s Stereotyped Behavior, Metabolic and Physical Activity Profiles, Physical Fitness, and Health-Related Quality of Life: A Study Protocol. Front. Public Health 2018, 6, 47. [Google Scholar] [CrossRef]
- Huang, J.; Du, C.; Liu, J.; Tan, G. Meta-Analysis on Intervention Effects of Physical Activities on Children and Adolescents with Autism. Int. J. Environ. Res. Public. Health 2020, 17, 1950. [Google Scholar] [CrossRef]
- Majhi, S.; Kumar, S.; Singh, L. A Review on Autism Spectrum Disorder: Pathogenesis, Biomarkers, Pharmacological and Non-Pharmacological Interventions. CNS Neurol. Disord. Drug Targets 2023, 22, 659–677. [Google Scholar] [CrossRef]
- Susniene, D.; Jurkauskas, A. The Concepts of Quality of Life and Happiness–Correlation and Differences. Eng. Econ. 2009, 63. Available online: https://inzeko.ktu.lt/index.php/EE/article/view/11648 (accessed on 6 December 2023).
- Sakip, S.R.M.; Zukri, A.Z.M.; Rahim, P.R.M.A. Assessing the Relationship Between Environmental, Psychological, Physical and Social Towards the Quality of Life. Int. J. Sustain. Constr. Eng. Technol. 2023, 14, 256–265. [Google Scholar] [CrossRef]
- Happiness or Quality of Life? Or Both?|Journal of Education Culture and Society. Available online: https://jecs.pl/index.php/jecs/article/view/1408 (accessed on 16 December 2024).
- Beneytez, C. Síntomas de ansiedad en los trastornos del espectro del autismo desde un enfoque transdiagnóstico. Universidad Complutense de Madrid. 2019. Available online: https://dialnet.unirioja.es/servlet/tesis?codigo=223238 (accessed on 16 December 2024).
- Kerns, C.M.; Kendall, P.C. Autism and anxiety: Overlap, similarities, and differences. In Handbook of Autism and Anxiety; en Autism and Child Psychopathology Series; Springer International Publishing/Springer Nature: Cham, Switzerland, 2014; pp. 75–89. [Google Scholar] [CrossRef]
- Sánchez-Cueva, M.S.; Marín, F.A.; Alonso-Esteban, Y. Ansiedad y trastornos del espectro del autismo: Notas para la intervención psicoeducativa. Siglo. Cero. 2022, 53, 4930. [Google Scholar] [CrossRef]
- White, S.W.; Oswald, D.; Ollendick, T.; Scahill, L. Anxiety in children and adolescents with autism spectrum disorders. Clin. Psychol. Rev. 2009, 29, 216–229. [Google Scholar] [CrossRef]
- Jenkinson, R.; Milne, E.; Thompson, A. The relationship between intolerance of uncertainty and anxiety in autism: A systematic literature review and meta-analysis. Autism Int. J. Res. Pract. 2020, 24, 1933–1944. [Google Scholar] [CrossRef]
- Ghaziuddin, M.; Ghaziuddin, N.; Greden, J. Depression in persons with autism: Implications for research and clinical care. J. Autism Dev. Disord. 2002, 32, 299–306. [Google Scholar] [CrossRef]
- Hofvander, B.; Delorme, R.; Chaste, P.; Nydén, A.; Wentz, E.; Ståhlberg, O.; Herbrecht, E.; Stopin, A.; Anckarsäter, H.; Gillberg, C.; et al. Psychiatric and psychosocial problems in adults with normal-intelligence autism spectrum disorders. BMC Psychiatry 2009, 9, 35. [Google Scholar] [CrossRef] [PubMed]
- Lever, A.G.; Geurts, H.M. Psychiatric Co-occurring Symptoms and Disorders in Young, Middle-Aged, and Older Adults with Autism Spectrum Disorder. J. Autism Dev. Disord. 2016, 46, 1916–1930. [Google Scholar] [CrossRef] [PubMed]
- van Heijst, B.F.; Deserno, M.K.; Rhebergen, D.; Geurts, H.M. Autism and depression are connected: A report of two complimentary network studies. Autism 2020, 24, 680–692. [Google Scholar] [CrossRef] [PubMed]
- Hopkins, K.; Crosland, P.; Elliott, N.; Bewley, S.; On behalf of the Clinical Guidelines Update Committee B. Diagnosis and management of depression in children and young people: Summary of updated NICE guidance. BMJ 2015, 350, h824. [Google Scholar] [CrossRef]
- Kelvin, R. Depression in children and young people. Paediatr. Child Health 2016, 26, 540–547. [Google Scholar] [CrossRef]
- Zenebe, Y.; Akele, B.; W/Selassie, M.; Necho, M. Prevalence and determinants of depression among old age: A systematic review and meta-analysis. Ann. Gen. Psychiatry 2021, 20, 55. [Google Scholar] [CrossRef]
- Hudson, C.C.; Hall, L.; Harkness, K.L. Prevalence of Depressive Disorders in Individuals with Autism Spectrum Disorder: A Meta-Analysis. J. Abnorm. Child Psychol. 2019, 47, 165–175. [Google Scholar] [CrossRef]
- Menezes, M.; Harkins, C.; Robinson, M.F.; Mazurek, M.O. Treatment of Depression in Individuals with Autism Spectrum Disorder: A Systematic Review. Res. Autism Spectr. Disord. 2020, 78, 101639. [Google Scholar] [CrossRef]
- Hollocks, M.J.; Lerh, J.W.; Magiati, I.; Meiser-Stedman, R.; Brugha, T.S. Anxiety and depression in adults with autism spectrum disorder: A systematic review and meta-analysis. Psychol. Med. 2019, 49, 559–572. [Google Scholar] [CrossRef]
- Earls, F. The epidemiology of depression in children and adolescents. Pediatr. Ann. 1984, 13, 23–31. [Google Scholar]
- Fernández, F.C.; Martínez, Á.M.; Martín, A.B.B.; Pérez-Fuentes, M.D.C.; Jurado, M.D.M.M.; Linares, J.J.G. Prevalencia de la depresión en España: Análisis de los últimos 15 años. Eur. J. Investig. Health Psychol. Educ. 2015, 5, 267. [Google Scholar] [CrossRef]
- Pardo, G.; Sandoval, A.; Umbarila, D. ADOLESCENCIA Y DEPRESIÓN. Rev. Colomb. Psicol. 2004, 13, 13–28. [Google Scholar]
- Nabeshima, T.; Kim, H.-C. Involvement of Genetic and Environmental Factors in the Onset of Depression. Exp. Neurobiol. 2013, 22, 235–243. [Google Scholar] [CrossRef] [PubMed]
- Álvaro-Estramiana, J.L.; Garrido-Luque, A.; Schweiger-Gallo, I. Causas sociales de la depresión. Una revisión crítica del modelo atributivo de la depresión. Rev. Int. Sociol. 2010, 68, 333–348. [Google Scholar] [CrossRef]
- Moscoso, D.R.B.; Narvaez, L.C.V.; Ortiz, L.F.A.; Ramos, R.A.; Gonzalez, E.M.V. Ansiedad y depresión en adolescentes. Rev. Bol. Redipe 2021, 10. [Google Scholar] [CrossRef]
- Theoharides, T.C.; Kavalioti, M.; Tsilioni, I. Mast Cells, Stress, Fear and Autism Spectrum Disorder. Int. J. Mol. Sci. 2019, 20, 3611. [Google Scholar] [CrossRef]
- Espada, J.P.; Orgilés, M.; Méndez, X.; Morales, A. Problemas relacionados con la regulación emocional: Depresión y problemas de ansiedad. Libro Blanco Salud Ment. Infanto-Juv. 2021, 1, 18–31. [Google Scholar]
- Charlton, R.A.; McQuaid, G.A.; Wallace, G.L. Social support and links to quality of life among middle-aged and older autistic adults. Autism Int. J. Res. Pract. 2023, 27, 92–104. [Google Scholar] [CrossRef]
- MacKenzie, K.T.; Theodat, A.; Beck, K.B.; Conner, C.M.; Mazefsky, C.A.; Eack, S.M. Correlates of Quality of Life in Autistic Individuals. Res. Autism Spectr. Disord. 2024, 115, 102401. [Google Scholar] [CrossRef]
- Kouroupa, A.; Laws, K.R.; Irvine, K.; Mengoni, S.E.; Baird, A.; Sharma, S. The use of social robots with children and young people on the autism spectrum: A systematic review and meta-analysis. PLoS ONE 2022, 17, e0269800. [Google Scholar] [CrossRef] [PubMed]
- Health Quality Ontario. Internet-Delivered Cognitive Behavioural Therapy for Major Depression and Anxiety Disorders: A Health Technology Assessment. Ont. Health Technol. Assess. Ser. 2019, 19, 1–199. [Google Scholar]
- Jamwal, R.; Jarman, H.K.; Roseingrave, E.; Douglas, J.; Winkler, D. Smart home and communication technology for people with disability: A scoping review. Disabil. Rehabil. Assist. Technol. 2022, 17, 624–644. [Google Scholar] [CrossRef] [PubMed]
- Fellinghauer, B.; Reinhardt, J.D.; Stucki, G.; Bickenbach, J. Explaining the disability paradox: A cross-sectional analysis of the Swiss general population. BMC Public Health 2012, 12, 655. [Google Scholar] [CrossRef]
- Niero, M. Disability paradox: I disabili e la felicità. SALUTE E Soc 2005, 32–46. Available online: https://www.francoangeli.it/riviste/articolo@Model.IDArticolo (accessed on 6 December 2023).
- Cruceanu, G.L.; Clemente-Belmonte, S.; Herrero-Sanz, R.; Ayala, A.; Zorrilla-Muñoz, V.; Agulló-Tomás, M.S.; Martínez-Miguelez, C.; Fernández-Mayoralas, G. Evaluation of Older People Digital Images: Representations from a Land, Gender and Anti-ageist Perspective. Land 2023, 12, 18. [Google Scholar] [CrossRef]
- Van Dooren, M.; De Croon, R.; Swillen, A.; Verbert, K. Bridging the Communication Gap Between People With Cognitive Impairments and Their Caregivers Using mHealth Apps: User-Centered Design and Evaluation Study With People With 22q11 Deletion Syndrome. JMIR Hum. Factors 2023, 10, e44290. [Google Scholar] [CrossRef] [PubMed]
- Zannat, N.; Mahmud, M. Exploring mindmend: An innovative mental health support app for autistic adolescents and their caregivers. J. Digit. Syst. Dev. 2024, 2, 1–16. [Google Scholar] [CrossRef]
- Terranova, N.; Renard, D.; Shahin, M.H.; Menon, S.; Cao, Y.; Hop, C.E.C.A.; Hayes, S.; Madrasi, K.; Stodtmann, S.; Tensfeldt, T.; et al. Artificial Intelligence for Quantitative Modeling in Drug Discovery and Development: An Innovation and Quality Consortium Perspective on Use Cases and Best Practices. Clin. Pharmacol. Ther. 2024, 115, 658–672. [Google Scholar] [CrossRef]
- Blaurock, M.; Büttgen, M.; Schepers, J. Designing Collaborative Intelligence Systems for Employee-AI Service Co-Production. J. Serv. Res. 2024, 10946705241238751. [Google Scholar] [CrossRef]
- Benedicto-Rodriguez, G.; Zorrilla-Muñoz, V.; Fernandez, E.; Ferrandez, J.M. Technological Influence on the Measurement of Quality of Life in Persons with Autism Spectrum Disorder. In Proceedings of the Third International Conference on Innovations in Computing Research (ICR’24), Athens, Greece, 12–14 August 2024; Daimi, K., Al Sadoon, A., Eds.; Springer Nature: Cham, Switzerland, 2024; pp. 691–698. [Google Scholar] [CrossRef]
- Hong, J.; Bishop-Fitzpatrick, L.; Smith, L.E.; Greenberg, J.S.; Mailick, M.R. Factors Associated with Subjective Quality of Life of Adults with Autism Spectrum Disorder: Self-Report Versus Maternal Reports. J. Autism Dev. Disord. 2016, 46, 1368–1378. [Google Scholar] [CrossRef] [PubMed]
- Jariwala, K.; Khanna, R.; West-Strum, D.; Bentley, J.P.; Banahan, B.F.I.; Holmes, E.R.; Barnard, M. Psychometric properties of the world health organization’s quality of life-bref instrument (WHOQOL-BREF) among adults with autism. Value Health 2014, 17, A194. [Google Scholar] [CrossRef]
- Mason, D.; Rodgers, J.; Garland, D.; Wilson, C.; Parr, J.; McConachie, H. Measuring quality of life in autistic adults: The reliability and validity of the Brief Version of the World Health Organization Quality of Life scal. AMRC Open Res. 2022, 4, 3. [Google Scholar] [CrossRef]
- Mouelhi, Y.; Jouve, E.; Castelli, C.; Gentile, S. How is the minimal clinically important difference established in health-related quality of life instruments? Review of anchors and methods. Health Qual. Life Outcomes 2020, 18, 136. [Google Scholar] [CrossRef]
- Klefbeck, K. Educational Approaches to Improve Communication Skills of Learners with Autism Spectrum Disorder and Comorbid Intellectual Disability: An Integrative Systematic Review. Scand. J. Educ. Res. 2023, 67, 51–68. [Google Scholar] [CrossRef]
- De Houwer, J.; Barnes-Holmes, D.; Moors, A. What is learning? On the nature and merits of a functional definition of learning. Psychon. Bull. Rev. 2013, 20, 631–642. [Google Scholar] [CrossRef]
- Metz, D.H. Mobility of older people and their quality of life. Transp. Policy 2000, 7, 149–152. [Google Scholar] [CrossRef]
- Jordan, M. The power of connection: Self-care strategies of social wellbeing. J. Interprof. Educ. Pract. 2023, 31, 100586. [Google Scholar] [CrossRef]
- Savari, K.; Naseri, M.; Savari, Y. Evaluating the Role of Perceived Stress, Social Support, and Resilience in Predicting the Quality of Life among the Parents of Disabled Children. Int. J. Disabil. Dev. Educ. 2023, 70, 644–658. [Google Scholar] [CrossRef]
- Dainton, M.; Conville, R.L.; Rogers, L.E. The Meaning of “Relationship” in Interpersonal Communication. J. Marriage Fam. 1999, 61, 546. [Google Scholar] [CrossRef]
- Bogolyubov, N.N. A Method for Studying Model Hamiltonians: A Minimax Principle for Problems in Statistical Physics; Elsevier: Amsterdam, The Netherlands, 2013. [Google Scholar]
- Chabane, L.; Lazarescu, A.; Verley, G. Effective Hamiltonians and Lagrangians for Conditioned Markov Processes at Large Volume. J. Stat. Phys. 2022, 187, 6. [Google Scholar] [CrossRef]
- Cervera-Lierta, A.; Kottmann, J.S.; Aspuru-Guzik, A. Meta-Variational Quantum Eigensolver: Learning Energy Profiles of Parameterized Hamiltonians for Quantum Simulation. PRX Quantum 2021, 2, 020329. [Google Scholar] [CrossRef]
- Wilde, F.; Kshetrimayum, A.; Roth, I.; Hangleiter, D.; Sweke, R.; Eisert, J. Scalably learning quantum many-body Hamiltonians from dynamical data. arXiv 2022, arXiv:2209.14328. [Google Scholar] [CrossRef]
- Altman, E.; Brown, K.R.; Carleo, G.; Carr, L.D.; Demler, E.; Chin, C.; DeMarco, B.; Economou, S.E.; Eriksson, M.A. Quantum Simulators: Architectures and Opportunities. PRX Quantum 2021, 2, 017003. [Google Scholar] [CrossRef]
- O’Neill, M.; Jones, R.S. Sensory-perceptual abnormalities in autism: A case for more research? J. Autism Dev. Disord. 1997, 27, 283–293. [Google Scholar] [CrossRef]
- Kinnaird, E.; Stewart, C.; Tchanturia, K. Investigating alexithymia in autism: A systematic review and meta-analysis. Eur. Psychiatry J. Assoc. Eur. Psychiatr. 2019, 55, 80–89. [Google Scholar] [CrossRef]
- Alberdi-Fernández, A. Habilidades Comunicativas en Trastornos del Espectro Autista. Bachelor’s Thesis, Universidad Internacional de la Rioja, Logroño, Spain, 2015. Available online: https://reunir.unir.net/handle/123456789/3219 (accessed on 16 December 2024).
- Guerrero, L.C.; Padilla, E.M. Habilidades sociales y comunicativas a través del arte en jóvenes con trastorno del espectro autista (TEA). Estud. Pedagógicos Valdivia 2017, 43, 47–64. [Google Scholar] [CrossRef]
- Coryell, W. Trastornos Depresivos-Trastornos Psiquiátricos. Manual MSD Versión Para Profesionales. Available online: https://www.msdmanuals.com/es/professional/trastornos-psiquiátricos/trastornos-del-estado-de-ánimo/trastornos-depresivos (accessed on 16 December 2024).
- González-Blanch, C.; Umaran-Alfageme, O.; Cordero-Andrés, P.; Muñoz-Navarro, R.; Ruiz-Rodríguez, P.; Medrano, L.A.; Ruiz-Torres, M.; Collado, E.D.; Cano-Vindel, A. Grupo de Investigación PsicAP. Tratamiento psicológico de los trastornos emocionales en Atención Primaria: El manual de tratamiento transdiagnóstico del estudio PsicAP. Ansiedad Estrés 2018, 24, 1–11. [Google Scholar] [CrossRef]
- Hernandez, J.; Riobo, I.; Rozga, A.; Abowd, G.D.; Picard, R.W. Using electrodermal activity to recognize ease of engagement in children during social interactions. MIT Web Domain. 2014. Available online: https://dspace.mit.edu/handle/1721.1/107809 (accessed on 16 December 2024).
- Fong, T.; Nourbakhsh, I.; Dautenhahn, K. A survey of socially interactive robots. Robot. Auton. Syst. 2023, 42, 143–166. [Google Scholar] [CrossRef]
- Shigemi, S. ASIMO and Humanoid Robot Research at Honda. In Humanoid Robotics: A Reference; Goswami, A., Vadakkepat, P., Eds.; Springer: Dordrecht, The Netherlands, 2019; pp. 55–90. [Google Scholar] [CrossRef]
- O’Reilly, Z.; Navare, U.P.; Marchesi, S.; Wykowska, A. Does Embodiment and Interaction Affect the Adoption of the Intentional Stance Towards a Humanoid Robot? In Social Robotics: 14th International Conference, ICSR 2022, Florence, Italy, December 13–16, 2022, Proceedings, Part I; Springer: Berlin/Heidelberg, Germany, 2023; pp. 357–366. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| People Diagnosed with… | Med. Age ± SD | Total | Freq. Total (%) | Total ASD | Freq. ASD (%) |
|---|---|---|---|---|---|
| Autism Spectrum Disorder (ASD) | 36.34 ± 2.71 | 241 | 2.07 | ||
| Chronic Anxiety (CA) | 63.06 ± 0.37 | 2070 | 17.77 | 61 | 0.52 |
| Chronic Depression (CD) | 43.56 ± 6.16 | 2179 | 18.70 | 29 | 0.25 |
| Domains | Description of Variables | Number of Variables that Make up the Index |
|---|---|---|
| Communication | Some variables are related to the definition of communication [43], including the following: Difficulties in speaking in an understandable way or saying meaningful sentences; speaking comprehensively or saying meaningful sentences when using the assistive device; understanding the meaning of what others say to you; understanding the meaning of what others say to you when you receive help | 11 |
| Learning | Some variables are related with the definition of learning [44]. Included are those variables that determine the level of difficulty in paying attention with the gaze or maintaining attention with the ear; learning how to do simple things; learning to do simple things when you receive personal help or assistance; carrying out simple tasks | 7 |
| Mobility | Some variables are related with the definition of mobility [45]. Difficulty is measured in variables such as changing posture; changing posture when receiving personal help or assistance; keeping the body in the same position; keeping the body in the same position when receiving personal help or assistance; walking or moving around your home; walking or moving around your home when you receive personal help or assistance. | 16 |
| Self-care | Some variables are related with the definition of self-care [46]. These include variables that measure the level of difficulty when washing and drying different parts of the body; washing and drying different parts of the body when receiving personal help or assistance; performing basic body care; performing basic care of the body when receiving personal help or assistance | 14 |
| Domestic life or social support | Some variables are related with the definition of cosmetic life or social support [47]. These include variables that measure difficulties in managing the household budget, planning expenses, or organizing purchases; managing the household budget, planning expenses, or organizing shopping when you receive personal help or assistance; preparing meals; preparing meals when you receive personal help or assistance; taking care of other household chores | 6 |
| Interpersonal relationships | Some variables are related with the definition of interpersonal relationships [48]. These inlcude those that measure aspects related to the display of affection; respect or feelings, relationships with strangers, creating and maintaining relationships with friends and neighbors, acquaintances, and colleagues; starting a family or maintaining family relationships; creating and maintaining romantic or sexual relationships. | 5 |
| Shaphiro–Wilk and Skewness–Kurtosis tests | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Domain | Difficulty Level for… | Mean | ± | S.D. | Bartlett’s Test Chi2(2) * | Pr (Skewness) * | Pr (Kurtosis) * | Adj Chi2(2) * | ANOVA (F) * | Spearman (rho) * | Kruskal–Wallis (Chi Squared with Ties) |
| COMMUNICATION | …speak in an understandable way or say sentences that make sense | 1.959184 | ± | 0.0709385 | 0.6257 * | 0.8103 * | 0.0009 | 9.60 | 3.63 * | 0.6242 | 6.806 |
| …speak in an understandable way or say meaningful sentences when using the assistive device | 2.606061 | ± | 0.1439394 | 2.4316 * | 0.6348 * | 0.7915 * | 0.30 * | 0.58 | −0.0904 | 2.568 | |
| …understand the meaning of what others say | 1.815534 | ± | 0.0658057 | 0.7495 * | 0.3253 | 0.0189 | 6.13 | 1.69 | 0.0000 | 4.080 | |
| …understand the meaning of what others say to you when you receive help | 2.481481 | ± | 0.0897718 | 0.9155 * | 0.4246 | 0.4305 * | 1.29 * | 2.06 | −0.1286 | 7.303 | |
| …understand and express themselves through written language | 2.245.614 | ± | 0.0677463 | 4.1487 * | 0.0704 | 0.0000 | 16.31 | 2.49 | 0.3952 | 9953 * | |
| …understand and express themselves through gestures, symbols, drawings or sounds | 1.922078 | ± | 0.0842445 | 2.9057 * | 0.6355 * | 0.0000 | 14.27 | 6.69 * | −0.2020 | 9755 * | |
| …hold a dialogue and exchange ideas with one or more people | 2.117117 | ± | 0.0649308 | 2.5252 * | 0.4960 | 0.0035 | 8.07 | 2.47 | 0.3984 | 5.238 | |
| …use the telephone (landline or mobile) or other communication devices or techniques | 2.2 | ± | 0.0758348 | 0.8640 * | 0.1182 | 0.0000 | 35.46 | 1.50 | 0.3582 | 7.824 | |
| …use the telephone or other communication devices or techniques when receiving help | 2.612903 | ± | 0.1111329 | 1.2219 | 0.7389 * | 0.1064 * | 2.84 * | 1.01 | 0.3984 | 7.783 | |
| …use remote written communication systems | 2.42268 | ± | 0.0715487 | 0.9242 * | 0.0019 | 0.1429 * | 3.29 * | 2.68 | 0.4166 | 3.741 | |
| …use remote written communication systems when receiving help | 2.653846 | ± | 0.1313712 | 2.7316 | 0.4364 | 0.1133 * | 1.68 * | 2.09 | 0.1444 | 5.878 | |
| LEARNING | …pay attention with your eyes or keep your attention with your ears | 1.791667 | ± | 0.0626825 | 4.5721 | 0.5265 | 0.2657 * | 22.65 | 5.01 * | −0.1306 | 10.570 * |
| …learn to do simple things | 2.044944 | ± | 0.0797566 | 0.4567 | 0.7632 * | 0.0000 | 0.27 * | 5.18 * | −0.0833 | 9.213 | |
| …learn to do simple things when receiving personal help or assistance | 2.5 | ± | 0.0904326 | 2.5418 | 0.7078 * | 0.7153 * | 13.85 | 1.17 | −0.0388 | 9.250 | |
| …carry out simple tasks | 2.017241 | ± | 0.0998831 | 3.5982 | 0.9225 * | 0.0000 | 5.64 * | 5.01 * | −0.2899 | 9.271 | |
| …carry out simple tasks when receiving personal help or assistance | 2.5 | ± | 0.140698 | 0.5132 | 0.6868 * | 0.0163 | 6.91 | 0.47 | 0.0596 | 3.678 | |
| …carry out complex tasks | 2.293103 | ± | 0.0692834 | 1.6118 | 0.0194 | 0.0000 | 4.26 * | 4.94 * | −0.2145 | 12.600 * | |
| …carry out complex tasks when receiving personal help or assistance | 2.621053 | ± | 0.1005906 | 3.9635 | 0.7766 * | 0.0000 | 9.60 | 2.23 | −0.2332 | 7.793 | |
| MOBILITY | …change position | 2.038462 | ± | 0.141212 | 0.6533 | 0.8930 * | 0.1679 * | 8.06 | 0.80 | . | 4.832 |
| …change posture when receiving personal help or assistance | 2.590909 | ± | 0.2246603 | 0.6855 | 0.7807 * | 0.1128 * | 31.22 | 0.87 | . | 1.755 | |
| …keep the body in the same position | 2.034483 | ± | 0.1263621 | 3.2550 | 0.9187 * | 0.3872 * | . | 1.78 | . | 6.666 | |
| …keep the body in the same position when receiving help or personal assistance | 2.565217 | ± | 0.1867772 | 2.4995 | 0.6384 * | 0.6510 * | 2.80 * | 0.60 | . | 5.328 | |
| …walk or move around your home | 2.130435 | ± | 0.1578555 | 1.8263 | 0.6167 * | 0.0826 * | 3.20 * | 0.20 | . | 4.201 | |
| …walk or move around in your home when you receive help or personal assistance | 2.6 | ± | 0.210263 | 1.6960 | 0.5093 * | 0.6103 * | 4.62 * | 0.43 | . | 3.899 | |
| …walk or move outside your home | 2.541667 | ± | 0.0891167 | 0.0137 | 0.0060 | 0.7536 * | 6.58 | 1.96 | . | 3.318 | |
| …walk or move outside your home when you receive help or personal assistance | 2.414634 | ± | 0.1560785 | 1.2133 | 0.6326 * | 0.0482 | 18.79 | 1.99 | . | 1.915 | |
| …move using means of transport as a passenger | 2.538462 | ± | 0.1007571 | 0.4217 | 0.0008 | 0.6935 * | 18.40 | 0.36 | . | 1.254 | |
| …move using means of transport as a passenger when receiving personal help or assistance | 2.511628 | ± | 0.1608811 | 7.4477 | 0.5180 | 0.0029 | 10.43 | 1.22 | . | 0.832 | |
| …driving vehicles without adaptations | 2.862069 | ± | 0.0957745 | . | 0.0000 | 0.0000 | 10.00 | 0.00 | . | 1.685 | |
| …driving vehicles when receiving personal help or assistance | 3.666667 | ± | 0.3333333 | . | . | . | 27.99 | . | . | . | |
| …manipulate and move objects, using hands and arms | 2.054054 | ± | 0.115898 | 1.1332 | 0.8358 * | 0.1097 * | 7.94 | 0.85 | . | 5.230 | |
| …manipulate and move objects, using hands and arms when receiving personal help or assistance | 2.862069 | ± | 0.1770318 | 9.6770 | 0.5613 * | 0.1084 * | 59.60 | 0.60 | . | 2.312 | |
| …manipulate small objects with hands and fingers | 2.212121 | ± | 0.1287879 | 14.4606 | 0.3499 | 0.0544 * | 11.56 | 2.76 | . | 11.236 * | |
| …manipulate small objects with hands and fingers when receiving personal help or assistance | 2.884615 | ± | 0.1866871 | 13.5468 | 0.8958 * | 0.0071 | 73.47 | 1.73 | 4.566 | ||
| SELF-CARE | …wash and dry the different parts of the body | 2.239437 | ± | 0.0929395 | 1.1548 | 0.1091 | 0.0000 | 4.83 * | 0.17 | −0.0425 | 1.778 |
| …wash and dry the different parts of the body when receiving help or personal assistance | 2.666667 | ± | 0.1300316 | 1.1743 | 0.5711 * | 0.0000 | 11.97 | 0.48 | −0.0065 | 2.645 | |
| …perform basic body care | 2.544118 | ± | 0.0796001 | 0.6105 | 0.0005 | 0.6149 * | 44.75 | 3.33 * | 0.2487 | 2.931 | |
| …perform basic body care when receiving personal help or assistance | 2.878788 | ± | 0.1304737 | 0.2709 | 0.1082 | 0.0023 | 7.18 | 4.04 * | 0.1744 | 2.008 | |
| …go to the toilet and relieve yourself or take care of your intimate hygiene | 2.157895 | ± | 0.1085028 | 0.0259 | 0.3216 | 0.0000 | 12.45 | 3.03 | −0.1146 | 5.903 | |
| …go to the toilet and relieve yourself or take care of your intimate hygiene when you receive help or personal assistance | 2.849057 | ± | 0.1410005 | 4.4321 | 0.2696 * | 0.0051 | 25.49 | 1.37 | −0.2387 | 7.649 | |
| …dress or undress | 2.103448 | ± | 0.1118768 | 2.4061 | 0.5013 * | 0.0000 | 21.37 | 0.86 | 0.0427 | 2.838 | |
| …dressing or undressing when receiving personal help or assistance | 2.535714 | ± | 0.141798 | 1.5484 | 0.9943 * | 0.0002 | 19.09 | 0.87 | −0.1461 | 4.665 | |
| …eat and drink | 1.977778 | ± | 0.1329118 | 0.2832 | 0.8941 * | 0.0000 | 8.26 | 2.80 | −0.2343 | 5.132 | |
| …eat and drink when receiving personal help or assistance | 2.302326 | ± | 0.1579733 | 1.3172 | 0.2263 * | 0.0653 * | 10.97 | 2.25 | −0.2100 | 4.365 | |
| …comply with medical prescriptions | 0.1579733 | ± | 0.0859398 | 0.7047 | 0.0001 | 0.9239 * | 6.65 | 1.05 | 0.2560 | 4.795 | |
| …fulfill medical prescriptions when receiving personal help or assistance | 2.726027 | ± | 0.1382929 | 2.0651 | 0.3132 * | 0.0000 | 9.22 | 0.99 | 0.0374 | 6.149 | |
| …avoid dangerous situations | 2.41791 | ± | 0.0854637 | 5.5222 | 0.0099 | 0.2554 * | 7.18 | 1.03 | −0.0526 | 7.126 | |
| …avoid dangerous situations when receiving personal help or assistance | 2.967213 | ± | 0.1440386 | 1.5263 | 0.0571 | 0.0006 | 12.45 | 0.36 | −0.0823 | 2.638 | |
| DOMESTIC LIFE | …manage the household budget, plan expenses or organize purchases | 2.681319 | ± | 0.0622711 | 3.9341 | 0.0000 | 0.0108 | 25.49 | 2.20 | −0.1464 | 7.544 |
| …manage the household budget, plan expenses or organize purchases when you receive personal help or assistance | 3.567164 | ± | 0.0979756 | 1.6465 | 0.0000 | 0.0128 | 21.37 | 0.42 | −0.0330 | 8.239 | |
| …prepare meals | 2.630435 | ± | 0.0631953 | 4.8575 | 0.0000 | 0.0853 * | 19.09 | 2.83 | −0.2279 | 7.243 | |
| …prepare meals when receiving personal help or assistance | 3.131579 | ± | 0.1144661 | 5.5536 | 0.0081 | 0.1230 * | 8.26 | 1.83 | −0.0186 | 7.257 | |
| …take care of other chores around the house | 2.494382 | ± | 0.0734451 | 4.3456 | 0.0003 | 0.7782 * | 10.97 | 1.44 | −0.0997 | 4.225 | |
| …take care of other chores around the house when you receive personal help or assistance | 3.04 | ± | 0.1114038 | 8.7014 | 0.0249 * | 0.1397 * | 6.65 | 2.16 | −0.1224 | 3.370 | |
| INDIVIDUAL RELATIONSHIPS | …show affection, respect or feelings | 1.891304 | ± | 0.0732439 | 2.2537 | 0.5269 * | 0.0014 | 9.22 | 1.87 | −0.1925 | 8.445 |
| …associating with unknown people | 2.131148 | ± | 0.059295 | 0.9925 | 0.5114 * | 0.0355 | 4.87 * | 3.77 * | −0.1927 | 7.782 | |
| …create and maintain relationships with friends, neighbors, acquaintances, subordinates, superiors or colleagues | 2 | ± | 0.0636778 | 0.9231 | 1.000 | 0.0000 | 22.70 | 2.22 | −0.1633 | 6.626 | |
| …form a family or maintain family relationships | 2.5 | ± | 0.0832816 | 2.6687 | 0.0009 | 0.9094 * | 9.46 | 1.91 | −0.0392 | 6.463 | |
| …create and maintain sentimental, partner or sexual relationships | 2.546667 | ± | 0.0742369 | 0.3646 | 0.0004 | 0.6230 * | 10.87 | 0.32 | −0.0574 | 2.151 | |
| Do you believe that the use of new technologies has improved aspects of your daily life? | 2.647059 | ± | 0.0743089 | 0.0002 | 0.6863 * | 12.27 | |||||
| Domain | Difficulty Level for… | ASD (n = 241) | ASD with CA (n = 61) | ASD with CD (n = 29) |
|---|---|---|---|---|
| COMMUNICATION | …speak in an understandable way or say sentences that make sense | −0.2053 * | −0.4067 | −0.4143 |
| …speak in an understandable way or say meaningful sentences when using the assistive device | −0.1318 | 0.7559 | . | |
| …understand the meaning of what others say | −0.1804 | −0.4446 * | −0.7354 * | |
| …understand the meaning of what others say to you when you receive help | −0.2365 * | −0.1869 | −0.4437 | |
| …understand and express themselves through written language | −0.1887 * | −0.2460 | −0.2768 | |
| …understand and express themselves through gestures, symbols, drawings or sounds | −0.3095 * | −0.5649 * | −0.4299 | |
| …hold a dialogue and exchange ideas with one or more people | −0.0496 | −0.3928 | −0.5486 | |
| …use the telephone (landline or mobile) or other communication devices or techniques | −0.1081 | −0.2764 | −0.5993 | |
| …use the telephone or other communication devices or techniques when receiving help | −0.2147 | −0.0000 | −0.5000 | |
| …use remote written communication systems | −0.0472 | −0.0475 | −0.6198 | |
| …use remote written communication systems when receiving help | −0.2489 | 0.2000 | −0.4677 | |
| LEARNING | …pay attention with your eyes or keep your attention with your ears | −0.3116 * | −0.1667 | −0.6142 |
| …learn to do simple things | −0.2994 * | −0.5765 * | −0.7385 | |
| …learn to do simple things when receiving personal help or assistance | −0.2106 | −0.0578 | . | |
| …carry out simple tasks | −0.3779 * | −0.3850 | . | |
| …carry out simple tasks when receiving personal help or assistance | −0.1201 | 0.3665 | . | |
| …carry out complex tasks | −0.2828 * | −0.2718 | −0.3543 | |
| …carry out complex tasks when receiving personal help or assistance | −0.2351 * | 0.1414 | 0.0184 | |
| MOBILITY | …change position | −0.2028 | −0.1887 | −0.2342 |
| …change posture when receiving personal help or assistance | −0.2284 | −0.0463 | −0.1766 | |
| …keep the body in the same position | −0.3374 | −0.3915 | −0.3263 | |
| …keep the body in the same position when receiving help or personal assistance | −0.2033 | 0.1942 | 0.0913 | |
| …walk or move around your home | −0.0637 | 0.1295 | −0.0425 | |
| …walk or move around in your home when you receive help or personal assistance | −0.2490 | −0.2340 | −0.4678 | |
| …walk or move outside your home | −0.1833 | −0.1970 | −0.4468 | |
| …walk or move outside your home when you receive help or personal assistance | −0.1430 | −0.2428 | −0.0778 | |
| …move using means of transport as a passenger | −0.0988 | 0.3502 | 0.7660 * | |
| …move using means of transport as a passenger when receiving personal help or assistance | −0.0996 | 0.2810 | 0.6847 | |
| …driving vehicles without adaptations | 0.0091 | . | . | |
| …driving vehicles when receiving personal help or assistance | . | . | . | |
| …manipulate and move objects, using hands and arms | −0.0613 | 0.0400 | 0.3208 | |
| …manipulate and move objects, using hands and arms when receiving personal help or assistance | −0.2310 | −0.2037 | −0.4082 | |
| …manipulate small objects with hands and fingers | −0.3429 | −0.6375 * | −0.1715 | |
| …manipulate small objects with hands and fingers when receiving personal help or assistance | −0.3015 | −0.3338 | −0.1741 | |
| SELF-CARE | …wash and dry the different parts of the body | −0.0506 | 0.0970 | 0.0000 |
| …wash and dry the different parts of the body when receiving help or personal assistance | −0.0418 | −0.0251 | 0.0000 | |
| …perform basic body care | 0.0874 | 0.0424 | −0.1291 | |
| …perform basic body care when receiving personal help or assistance | −0.0639 | −0.0807 | −0.1768 | |
| …go to the toilet and relieve yourself or take care of your intimate hygiene | −0.2954 * | −0.1874 | −0.6625 | |
| …go to the toilet and relieve yourself or take care of your intimate hygiene when you receive help or personal assistance | −0.2593 | −0.1423 | −0.3151 | |
| …dress or undress | −0.1740 | 0.1755 | 0.0000 | |
| …dressing or undressing when receiving personal help or assistance | −0.1621 | 0.0987 | 0.1291 | |
| …eat and drink | −0.3267 * | −0.4105 | −0.5571 | |
| …eat and drink when receiving personal help or assistance | −0.2102 | −0.7172 * | −0.9191 * | |
| …comply with medical prescriptions | −0.0128 | −0.2002 | −0.5130 | |
| …fulfill medical prescriptions when receiving personal help or assistance | −0.1544 | −0.1881 | −0.6198 | |
| …avoid dangerous situations | −0.1513 | −0.1015 | −0.6355 | |
| …avoid dangerous situations when receiving personal help or assistance | −0.1316 | −0.0248 | −0.3151 | |
| DOMESTIC LIFE | …manage the household budget, plan expenses or organize purchases | −0.1831 | −0.2202 | −0.4348 |
| …manage the household budget, plan expenses or organize purchases when you receive personal help or assistance | 0.0886 | 0.0696 | −0.2140 | |
| …prepare meals | −0.2307 * | −0.4367 * | −0.5433 | |
| …prepare meals when receiving personal help or assistance | −0.0543 | −0.0896 | −0.2895 | |
| …take care of other chores around the house | −0.1795 | −0.3359 | −0.5333 | |
| …take care of other chores around the house when you receive personal help or assistance | −0.1544 | −0.0791 | −0.3481 | |
| INDIVIDUAL RELATIONSHIPS | …show affection, respect or feelings | −0.0918 | 0.0262 | −0.1959 |
| …associating with unknown people | −0.1795 * | −0.0167 | 0.0669 | |
| …create and maintain relationships with friends, neighbors, acquaintances, subordinates, superiors or colleagues | −0.1587 | −0.1518 | 0.0176 | |
| …form a family or maintain family relationships | −0.1094 | 0.2160 | 0.1066 | |
| …create and maintain sentimental, partner or sexual relationships | −0.0675 | 0.1259 | 0.0449 |
| ALL VARIABLES (n = 241) | SELECTED VARIABLES ASD + CA (n = 61) | SELECTED VARIABLES ASD + CD (n = 29) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Domain | Average Interitem Correlation | Cronbach’s α | Average Interitem Correlation | Cronbach’s α | Uniqueness | KMO | Average Interitem Correlation | Cronbach’s α | |
| Difficulty Level for… | |||||||||
| COMMUNICATION | …speak in an understandable way or say sentences that make sense | 0.3114 | 0.8326 | −0.0285 | 0.1051 | −0.1626 | |||
| …speak in an understandable way or say meaningful sentences when using the assistive device | 0.3258 | 0.8417 | |||||||
| …understand the meaning of what others say | 0.3288 | 0.8435 | |||||||
| …understand the meaning of what others say to you when you receive help | 0.3124 | 0.8333 | −0.0104 | −0.1587 | |||||
| …understand and express themselves through written language | 0.3028 | 0.8269 | −0.2226 * | 0.5339 | 0.0827 * | 0.4773 | 0.0888 | 0.2804 | |
| …understand and express themselves through gestures, symbols, drawings or sounds | 0.3213 | 0.8389 | −0.0003 | −0.0380 | 0.1910 | ||||
| …hold a dialogue and exchange ideas with one or more people | 0.2905 | 0.8183 | |||||||
| …use the telephone (landline or mobile) or other communication devices or techniques | 0.2997 | 0.8248 | |||||||
| …use the telephone or other communication devices or techniques when receiving help | 0.3098 | 0.8316 | |||||||
| …use remote written communication systems | 0.3198 | 0.8380 | |||||||
| …use remote written communication systems when receiving help | 0.3153 | 0.8351 | |||||||
| Do you believe that the use of new technologies has improved aspects of your daily life? | 0.4597 | 0.9035 | −0.0590 | 0.0557 | 0.1910 | ||||
| 0.3243 | 0.8521 | 0.0328 | 0.1451 | −0.0505 | |||||
| LEARNING | …pay attention with your eyes or keep your attention with your ears | 0.4079 | 0.8283 | 0.3401 ** | 0.7204 | 0.5882 | 0.3679 | 0.4839 ** | 0.7895 |
| …learn to do simple things | 0.3883 | 0.8163 | 0.2250 | 0.5921 | 0.3057 | 0.6378 | |||
| …learn to do simple things when receiving personal help or assistance | 0.4107 | 0.8299 | 0.3294 ** | 0.7107 | 0.2864 * | 0.3047 | |||
| …carry out simple tasks | 0.3825 | 0.8126 | |||||||
| …carry out simple tasks when receiving personal help or assistance | 0.4087 | 0.8287 | |||||||
| …carry out complex tasks | 0.3961 | 0.8211 | 0.2498 * | 0.6247 | 0.3161 ** | 0.6496 | |||
| …carry out complex tasks when receiving personal help or assistance | 0.4064 | 0.8273 | 0.3585 ** | 0.7364 | 0.1763 * | 0.6243 * | 0.5467 ** | 0.8283 | |
| Do you believe that the use of new technologies has improved aspects of your daily life? | 0.4719 | 0.8622 | 0.4138 | 0.7792 | 0.4630 | 0.7752 | |||
| 0.4083 | 0.8466 | 0.3173 | 0.7361 | 0.4173 | 0.7817 | ||||
| SELF-CARE | …wash and dry the different parts of the body | 0.4127 | 0.9077 | ||||||
| …wash and dry the different parts of the body when receiving help or personal assistance | 0.4011 | 0.9036 | |||||||
| …perform basic body care | 0.4226 | 0.9111 | |||||||
| …perform basic body care when receiving personal help or assistance | 0.3975 | 0.9023 | |||||||
| …go to the toilet and relieve yourself or take care of your intimate hygiene | 0.4021 | 0.9040 | 0.4105 ** | 0.5921 | 0.5571 ** | 0.7155 | |||
| …go to the toilet and relieve yourself or take care of your intimate hygiene when you receive help or personal assistance | 0.3960 | 0.9018 | |||||||
| …dress or undress | 0.4031 | 0.9044 | |||||||
| …dressing or undressing when receiving personal help or assistance | 0.3922 | 0.9003 | |||||||
| …eat and drink | 0.4101 | 0.9068 | 0.1874 * | 0.3157 | 0.6625 ** | 0.7970 | |||
| …eat and drink when receiving personal help or assistance | 0.4055 | 0.9052 | |||||||
| …comply with medical prescriptions | 0.4229 | 0.9112 | |||||||
| …fulfill medical prescriptions when receiving personal help or assistance | 0.4036 | 0.9045 | |||||||
| …avoid dangerous situations | 0.4043 | 0.9048 | |||||||
| …avoid dangerous situations when receiving personal help or assistance | 0.4033 | 0.9044 | |||||||
| Do you believe that the use of new technologies has improved aspects of your daily life? | 0.4605 | 0.9228 | 0.5926 | 0.7442 | 0.4472 | 0.6180 | |||
| 0.4090 | 0.9121 | 0.3619 | 0.6299 | 0.5663 | 0.7596 | ||||
| DOMESTIC LIFE | …manage the household budget, plan expenses or organize purchases | 0.4512 | 0.8315 | ||||||
| …manage the household budget, plan expenses or organize purchases when you receive personal help or assistance | 0.4760 | 0.8450 | |||||||
| …prepare meals | 0.4488 | 0.8301 | 0.4367 ** | 0.6079 | 0.5433 ** | 0.7040 | |||
| …prepare meals when receiving personal help or assistance | 0.4453 | 0.8281 | |||||||
| …take care of other chores around the house | 0.4169 | 0.8110 | |||||||
| …take care of other chores around the house when you receive personal help or assistance | 0.4295 | 0.8187 | |||||||
| Do you believe that the use of new technologies has improved aspects of your daily life? | 0.6258 | 0.9094 | |||||||
| 0.4697 | 0.8611 | ||||||||
| INDIVIDUAL RELATIONSHIPS | …show affection, respect or feelings | 0.3252 | 0.7067 | ||||||
| …associating with unknown people | 0.3226 | 0.7043 | 0.0167 | 0.0328 | 0.0699 | 0.1254 | |||
| …create and maintain relationships with friends, neighbors, acquaintances, subordinates, superiors or colleagues | 0.3130 | 0.6950 | |||||||
| …form a family or maintain family relationships | 0.3232 | 0.7048 | |||||||
| …create and maintain sentimental, partner or sexual relationships | 0.3199 | 0.7016 | |||||||
| Do you believe that the use of new technologies has improved aspects of your daily life? | 0.5111 | 0.8394 | |||||||
| 0.3482 | 0.7622 | ||||||||
| Note: * Cronbach’s alpha > 0.7. * Average iteritem correlation with moderate interrelatedness: 0.15 to 0.3. ** Strong 0.3–0.5. Uniqueness * with values <0.5 indicates the variable is well represented by the factors. KMO * for values >0.6 indicates the sample is adequate for the analysis. | I_17 | 0.2072 | 0.5593 | ||||||
| Overall KMO | 0.4838 | ||||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Benedicto-Rodríguez, G.; Zorrilla-Muñoz, V.; Garcia-Aracil, N.; Fernandez, E.; Ferrández, J.M. Understanding Technology Perception in Autism with Separate Analyses for Anxiety and Depression Using Quantum Circuit Simulation Approach. Technologies 2025, 13, 165. https://doi.org/10.3390/technologies13040165
Benedicto-Rodríguez G, Zorrilla-Muñoz V, Garcia-Aracil N, Fernandez E, Ferrández JM. Understanding Technology Perception in Autism with Separate Analyses for Anxiety and Depression Using Quantum Circuit Simulation Approach. Technologies. 2025; 13(4):165. https://doi.org/10.3390/technologies13040165
Chicago/Turabian StyleBenedicto-Rodríguez, Gema, Vanessa Zorrilla-Muñoz, Nicolas Garcia-Aracil, Eduardo Fernandez, and José Manuel Ferrández. 2025. "Understanding Technology Perception in Autism with Separate Analyses for Anxiety and Depression Using Quantum Circuit Simulation Approach" Technologies 13, no. 4: 165. https://doi.org/10.3390/technologies13040165
APA StyleBenedicto-Rodríguez, G., Zorrilla-Muñoz, V., Garcia-Aracil, N., Fernandez, E., & Ferrández, J. M. (2025). Understanding Technology Perception in Autism with Separate Analyses for Anxiety and Depression Using Quantum Circuit Simulation Approach. Technologies, 13(4), 165. https://doi.org/10.3390/technologies13040165