
Parametric Frailty Analysis in Presence of Collinearity: An Application to Assessment of Infant Mortality


Abstract
:1. Introduction
2. Ridge Estimator for Parametric Frailty Model
3. Simulation Study
4. Real Life Application
5. Discussion and Conclusions
6. Future Scope
Author Contributions
Funding
Conflicts of Interest
References
- Wienke, A. Frailty Models in Survival Analysis; Chapman & Hall: London, UK, 2011; pp. 1–320. [Google Scholar]
- Beard, R.E. Note on some mathematical mortality models. In The Lifespan of Animals; Wolstenholme, G.E.W., Conner, M.O., Eds.; Ciba Foundation Colloquium on Ageing, Little, Brown: Boston, MA, USA, 1959; pp. 302–311. [Google Scholar]
- Blossfeld, H.P.; Hamerle, A. Unobserved heterogeneity in event history models. Qual. Quant. 1992, 26, 157–168. [Google Scholar] [CrossRef]
- Heckman, J.; Hotz, J.; Walker, J. New evidence on the timing and spacing of births. Am. Econ. Rev. Pap. Proc. 1985, 75, 179–184. [Google Scholar]
- Sastry, N. A nested frailty model for survival data, with an application to the study of child survival in Northeast Brazil. J. Am. Stat. Assoc. 1997, 92, 426–435. [Google Scholar] [CrossRef]
- Magadi, M.A.; Diamond, I.; Rodrigues, R.N. The determinants of delivery care in Kenya. Soc. Biol. 2001, 47, 164–188. [Google Scholar] [CrossRef]
- Omariba, D.; Beaujot, R.; Rajulton, F. Determinants of infant and child mortality in Kenya: An analysis controlling for frailty effects. Popul. Res. Policy Rev. 2007, 26, 299–321. [Google Scholar] [CrossRef]
- Pebley, A.R.; Goldman, N.; Rodriguez, G. Prenatal and delivery care and childhood immunization in Guatemala: Do family and community matter? Demography 1996, 33, 231–247. [Google Scholar] [CrossRef]
- Singh, K.K.; Pandey, N.; Gautam, A. Effect of Breastfeeding and Maternal Health Care programme on infant mortality. Demogr. India 2007, 36, 253–266. [Google Scholar]
- Hoerl, A.E.; Kennard, R.W. Ridge regression: Biased estimation for nonorthogonal problems. Technometrics 1970, 12, 55–67. [Google Scholar] [CrossRef]
- Hoerl, A.E.; Kennard, R.W. Ridge regression: Some simulations. Commun. Stat. 1970, 4, 1105–1123. [Google Scholar] [CrossRef]
- Schafer, R.L.; Roi, L.D.; Wolfe, R.A. A ridge logistic estimator. Commun. Stat. Theory Methods 1984, 13, 99–113. [Google Scholar] [CrossRef]
- Duffy, D.E.; Santner, T.J. On the small sample properties of norm-restricted maximum likelihood estimators for logistic regression models. Commun. Stat. Theory Methods 1989, 18, 959–980. [Google Scholar] [CrossRef]
- Cessie, S.L.; Houwelingen, J.C.V. Ridge estimators in logistic regression. Appl. Stat. 1992, 41, 191–201. [Google Scholar] [CrossRef]
- Vaupel, J.; Manton, K.; Stallard, E. Impact of heterogeneity in individual frailty on the dynamics of mortality. Demography 1979, 16, 439–454. [Google Scholar] [CrossRef] [PubMed]
- Oakes, D. A model for association in bivariate survival data. J. R. Stat. Soc. (B) 1982, 44, 414–422. [Google Scholar] [CrossRef]
- Sastry, N. Community characteristics, individual and household attributes, and child survival in Brazil. Demography 1996, 33, 211–229. [Google Scholar] [CrossRef] [PubMed]
- Smith, K.R.; Slattery, M.L.; French, T.K. Collinear nutrients and the risk of colon cancer. J. Clin. Epidemiol. 1991, 44, 715–723. [Google Scholar] [CrossRef]
- Xue, X.; Kim, M.Y.; Roy, E.S. Cox regression analysis in presence of collinearity: An application to assessment of health risks associated with occupational radiation exposure. Lifetime Data Anal. 2007, 12, 333–350. [Google Scholar] [CrossRef] [PubMed]
- Cox, D.R.; Hinkley, D.V. Theoretical Statistics; Chapman and Hall: London, UK, 1974. [Google Scholar]
- Ozkale, M.R. The red indicator and corrected VIFs in generalizedlinear models. Commun. Stat. Simul. Comput. 2021, 50, 4144–4170. [Google Scholar] [CrossRef]
- Mackinnon, M.J.; Puterman, A.L. Collinearity in generalized linear models. Commun. Stat. Theory Methods 1989, 18, 3463–3472. [Google Scholar] [CrossRef]
- Weissfeld, L.A.; Sereika, S.M. A multicollinearity diagnostic for generalized linear modelsy. Commun. Stat. Theory Methods 1991, 20, 1183–1198. [Google Scholar] [CrossRef]

{kind=link}
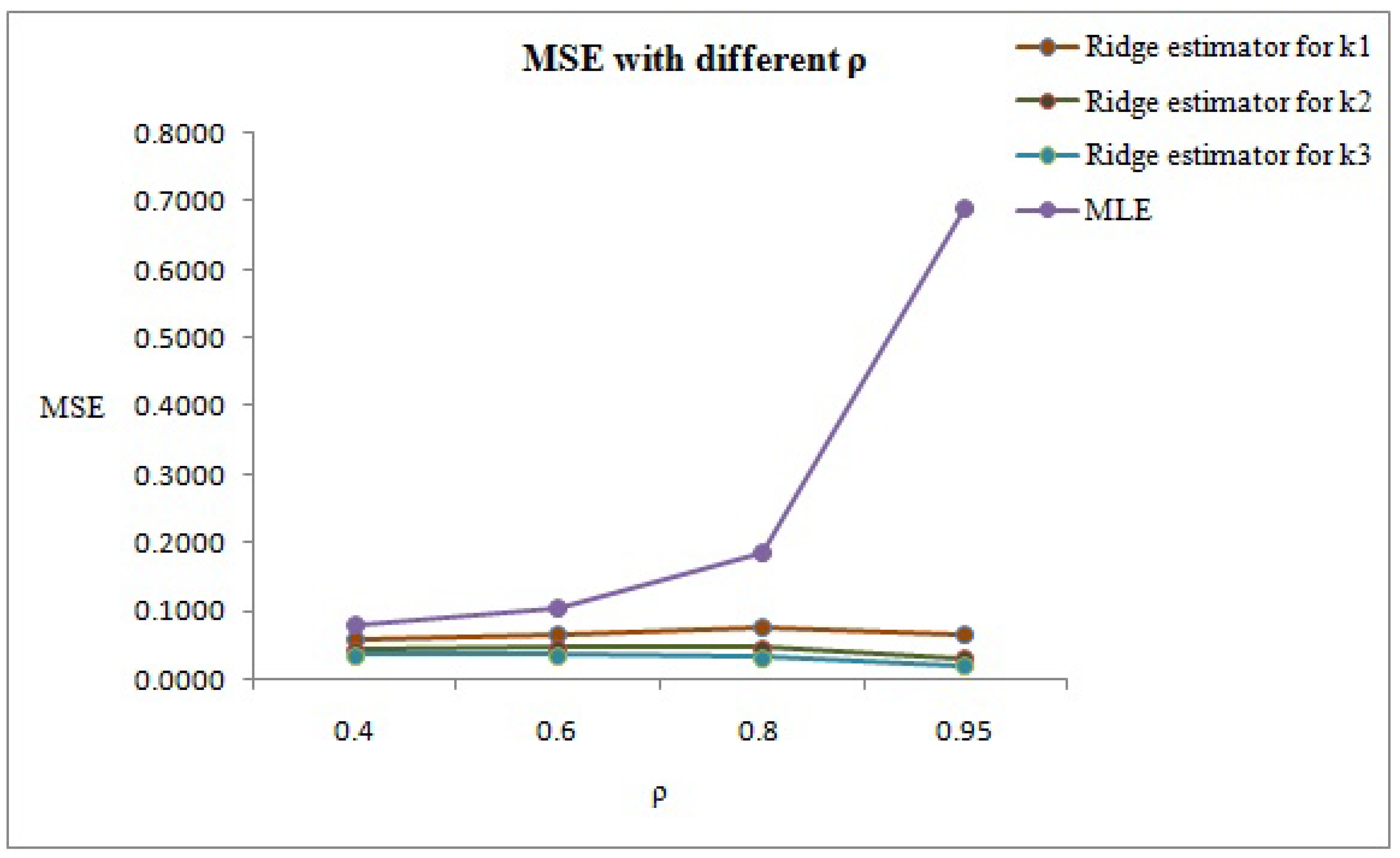
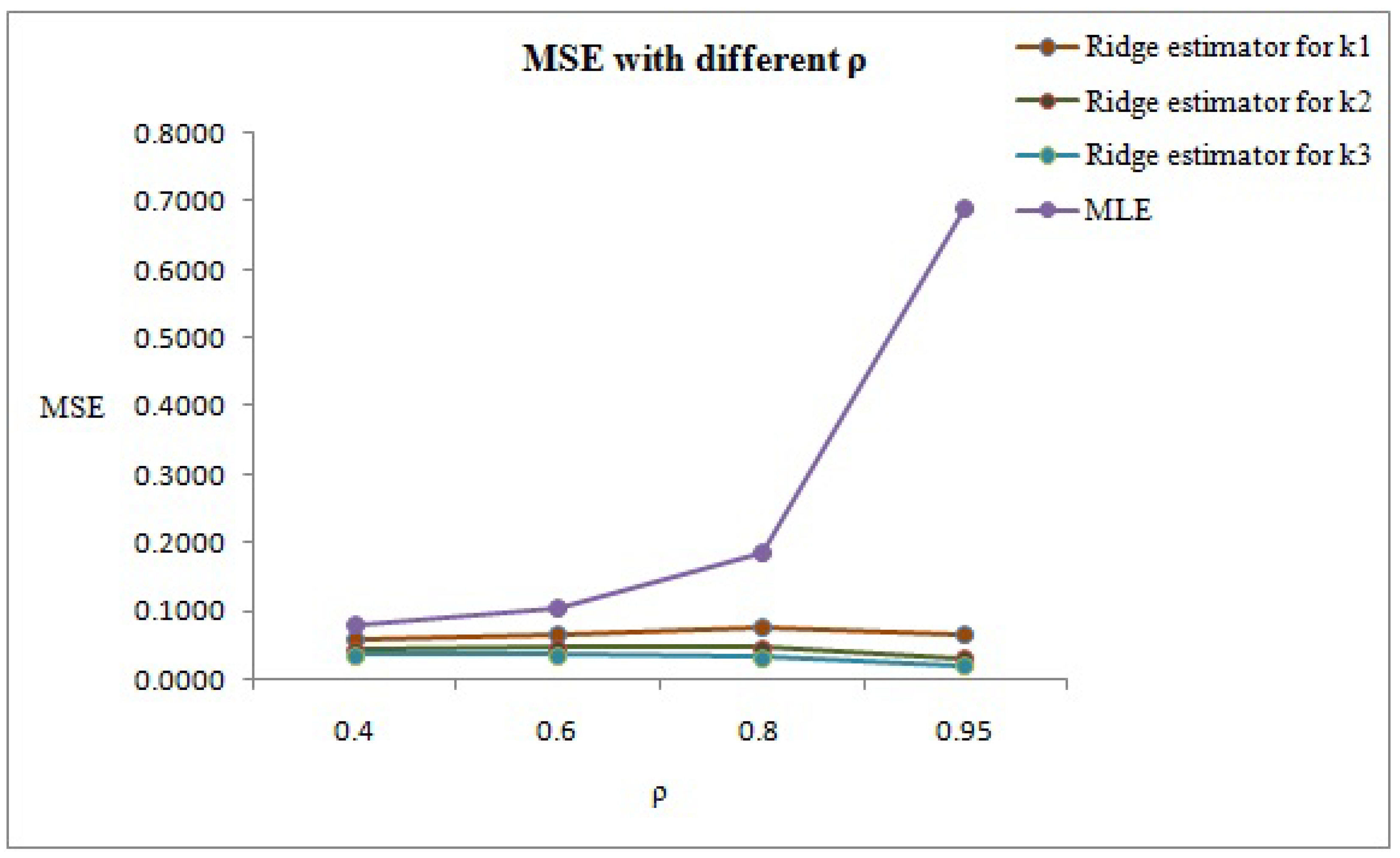
| Method | MSE () | % Reduction of MSE () | |
|---|---|---|---|
| 0.4 | MLE | 0.0801 | |
| Ridge estimator for | 0.0579 | 27.72 | |
| Ridge estimator for | 0.0444 | 44.57 | |
| Ridge estimator for | 0.0356 | 55.56 | |
| 0.6 | MLE | 0.1056 | |
| Ridge estimator for | 0.0658 | 37.69 | |
| Ridge estimator for | 0.0465 | 55.97 | |
| Ridge estimator for | 0.0355 | 66.38 | |
| 0.8 | MLE | 0.1871 | |
| Ridge estimator for | 0.0772 | 55.74 | |
| Ridge estimator for | 0.0457 | 75.57 | |
| Ridge estimator for | 0.0319 | 82.95 | |
| 0.95 | MLE | 0.6908 | |
| Ridge estimator for | 0.0654 | 90.55 | |
| Ridge estimator for | 0.0304 | 95.60 | |
| Ridge estimator for | 0.0206 | 97.02 |
| Method | MSE () | % Reduction of MSE () | |
|---|---|---|---|
| 0.4 | MLE | 0.0197 | |
| Ridge estimator for | 0.0181 | 8.12 | |
| Ridge estimator for | 0.0167 | 15.23 | |
| Ridge estimator for | 0.0155 | 21.32 | |
| 0.6 | MLE | 0.0259 | |
| Ridge estimator for | 0.0227 | 12.35 | |
| Ridge estimator for | 0.0202 | 22 | |
| Ridge estimator for | 0.0181 | 30.11 | |
| 0.8 | MLE | 0.0459 | |
| Ridge estimator for | 0.0350 | 23.74 | |
| Ridge estimator for | 0.0279 | 39.22 | |
| Ridge estimator for | 0.0230 | 49.89 | |
| 0.95 | MLE | 0.1693 | |
| Ridge estimator for | 0.0643 | 62.02 | |
| Ridge estimator for | 0.0350 | 79.33 | |
| Ridge estimator for | 0.0227 | 86.59 |
| Method | MSE () | % Reduction of MSE () | |
|---|---|---|---|
| 0.4 | MLE | 0.00196 | |
| Ridge estimator for | 0.00194 | 1.02 | |
| Ridge estimator for | 0.00193 | 1.5 | |
| Ridge estimator for | 0.00192 | 2.04 | |
| 0.6 | MLE | 0.00257 | |
| Ridge estimator for | 0.00254 | 1.16 | |
| Ridge estimator for | 0.00251 | 2.33 | |
| Ridge estimator for | 0.00247 | 3.89 | |
| 0.8 | MLE | 0.00458 | |
| Ridge estimator for | 0.00444 | 3.05 | |
| Ridge estimator for | 0.00432 | 5.60 | |
| Ridge estimator for | 0.00421 | 8.07 | |
| 0.95 | MLE | 0.01687 | |
| Ridge estimator for | 0.01492 | 1.15 | |
| Ridge estimator for | 0.01333 | 20.98 | |
| Ridge estimator for | 0.01200 | 40.58 |
| Variables | Birth | Death | ||
|---|---|---|---|---|
| Number | Percentage | Number | Percentage | |
| Place of residence | ||||
| Rural | 7348 | 63.4 | 776 | 68.49 |
| Urban | 4233 | 36.6 | 357 | 31.51 |
| Breastfeeding | ||||
| No | 925 | 8.0 | 766 | 67.61 |
| Yes | 10,656 | 92.0 | 367 | 32.39 |
| Sex | ||||
| Female | 5644 | 48.7 | 523 | 46.16 |
| Male | 5937 | 51.3 | 610 | 53.84 |
| Birth order | ||||
| 1 | 3809 | 32.9 | 315 | 27.80 |
| 2 | 3259 | 28.1 | 268 | 23.65 |
| 3 | 1799 | 15.5 | 158 | 13.95 |
| 4 | 2714 | 23.4 | 392 | 34.60 |
| Place of delivery | ||||
| Home | 6110 | 52.8 | 699 | 61.69 |
| Govt. hospital | 2802 | 24.2 | 204 | 18.01 |
| Prvt. Hospital | 2648 | 22.9 | 224 | 19.77 |
| Other | 21 | 0.2 | 6 | 0.53 |
| Marital status | ||||
| Unmarried | 11 | 0.1 | 1 | 0.09 |
| 0–4 Years | 4964 | 42.9 | 324 | 28.60 |
| 5–9 Years | 3850 | 33.2 | 357 | 31.51 |
| 10 Years | 2756 | 23.8 | 451 | 39.81 |
| ANC | ||||
| No | 2165 | 18.7 | 311 | 27.45 |
| 1–2 | 2687 | 23.2 | 303 | 26.74 |
| 3 | 6729 | 58.1 | 519 | 45.81 |
| Age of mother | ||||
| < 18 Years | 739 | 6.4 | 76 | 6.71 |
| 18–24 Years | 5075 | 43.8 | 390 | 34.42 |
| 25–29 Years | 3453 | 29.8 | 316 | 27.89 |
| 30–34 Years | 1537 | 13.3 | 206 | 18.18 |
| 35 Years | 777 | 6.7 | 145 | 12.80 |
| Mother education | ||||
| No | 4512 | 39 | 598 | 52.78 |
| Primary | 1687 | 14.6 | 196 | 17.30 |
| Secondary | 4436 | 38.3 | 309 | 27.27 |
| Higher | 946 | 8.2 | 30 | 2.65 |
| IFA | ||||
| No | 3708 | 32.0 | 484 | 42.72 |
| Yes | 7873 | 68.0 | 649 | 57.28 |
| Family size | ||||
| 1–3 | 1071 | 9.2 | 260 | 22.95 |
| 4–6 | 5214 | 45.0 | 514 | 45.37 |
| 7 | 5296 | 45.7 | 359 | 31.69 |
| Category | MLE | Ridge Estimator | ||
|---|---|---|---|---|
| S.E. | S.E. | |||
| Place of residence | ||||
| Urban | - | - | - | - |
| Rural | 1.156 | 0.104 | 1.162 | 0.103 |
| Breastfeeding | ||||
| No | - | - | - | - |
| Yes | 8.28 × 10 * | 0.093 | 8.49 × 10 * | 0.092 |
| Sex | ||||
| Male | - | - | - | - |
| Female | 1.044 | 0.089 | 1.047 | 0.089 |
| Birth order | ||||
| 1 | 1.176 | 0.176 | 1.209 | 0.171 |
| 2 | 1.243 | 0.150 | 1.265 | 0.147 |
| 3 | 1.087 | 0.154 | 1.099 | 0.151 |
| 4 | - | - | - | - |
| Place of delivery | ||||
| Home | 1.149 | 0.134 | 1.162 | 0.133 |
| Govt. hospital | 0.935 | 0.145 | 0.947 | 0.143 |
| Prvt. Hospital | - | - | - | - |
| Other | 1.350 | 0.688 | 1.336 | 0.614 |
| Marital status | ||||
| Unmarried | 0.507 | 1.652 | 0.674 | 0.985 |
| 0–4 Years | - | - | - | - |
| 5–9 Years | 1.546 * | 0.137 | 1.568 * | 0.134 |
| 10 Years | 1.939 * | 0.192 | 1.988 * | 0.187 |
| TT | ||||
| No | 1.246 | 0.153 | 1.253 | 0.151 |
| 1 | 1.077 | 0.162 | 1.079 | 0.160 |
| 2 | - | - | - | - |
| ANC | ||||
| No | 0.987 | 0.161 | 0.995 | 0.159 |
| 1–2 | 1.162 | 0.118 | 1.169 | 0.117 |
| 3 | - | - | - | - |
| Age of mother | ||||
| <18 Years | 1.459 | 0.193 | 1.461 * | 0.191 |
| 18–24 Years | - | - | - | - |
| 25–29 Years | 1.316 * | 0.125 | 1.317 * | 0.123 |
| 30–34 Years | 1.723 * | 0.170 | 1.717 * | 0.167 |
| 35 Years | 1.545 * | 0.206 | 1.543 * | 0.201 |
| Mother education | ||||
| No | 10.592 * | 0.232 | 9.821 * | 0.221 |
| Primary | 10.430 * | 0.242 | 9.639 * | 0.231 |
| Secondary | 7.560 * | 0.223 | 7.036 * | 0.213 |
| Higher | - | - | - | - |
| IFA | ||||
| No | - | - | - | - |
| Yes | 1.052 | 0.112 | 1.063 | 0.111 |
| Family size | ||||
| 1–3 | 2.175 * | 0.138 | 2.175 * | 0.137 |
| 4–6 | - | - | - | - |
| 7 | 0.715 * | 0.099 | 0.720 * | 0.098 |
| Method | MSE () | Percentage Reduction of MSE () |
|---|---|---|
| MLE | 3.819 | |
| Ridge estimator for | 3.553 | 6.97 |
| Ridge estimator for | 2.110 | 44.75 |
| Ridge estimator for | 2.048 | 46.37 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Albalawi, O.; Sirohi, A.; Rai, P.K.; Alanzi, A.R.A. Parametric Frailty Analysis in Presence of Collinearity: An Application to Assessment of Infant Mortality. Mathematics 2022, 10, 2255. https://doi.org/10.3390/math10132255
Albalawi O, Sirohi A, Rai PK, Alanzi ARA. Parametric Frailty Analysis in Presence of Collinearity: An Application to Assessment of Infant Mortality. Mathematics. 2022; 10(13):2255. https://doi.org/10.3390/math10132255
Chicago/Turabian StyleAlbalawi, Olayan, Anu Sirohi, Piyush Kant Rai, and Ayed R. A. Alanzi. 2022. "Parametric Frailty Analysis in Presence of Collinearity: An Application to Assessment of Infant Mortality" Mathematics 10, no. 13: 2255. https://doi.org/10.3390/math10132255
APA StyleAlbalawi, O., Sirohi, A., Rai, P. K., & Alanzi, A. R. A. (2022). Parametric Frailty Analysis in Presence of Collinearity: An Application to Assessment of Infant Mortality. Mathematics, 10(13), 2255. https://doi.org/10.3390/math10132255