Abstract
The current healthcare system suffers from information fragmentation. Achieving an efficient medical process necessitates coordination among healthcare institutions at different levels to enhance efficiency and reduce costs, with information synergy playing a crucial role in this endeavor. Due to concerns about information security and the costs associated with information construction, healthcare institutions are often reluctant to collaborate on information sharing. To address this issue, we propose an analytical framework for information synergy among different levels of healthcare institutions, which clarifies the impact of synergy benefits on the collaborative behavior of medical system members. We construct an evolutionary game model to study the dynamic strategy choices of the relevant participants. Our analysis reveals that general hospitals, as the main actors in the healthcare system, have a lower willingness to further invest in information construction and sharing. Their willingness is significantly influenced by the volume of information they can utilize from primary healthcare institutions. Moreover, interventions from the government and society can effectively encourage all members of the medical system to adopt collaborative information strategies. Establishing a comprehensive and unified information platform, actively promoting hierarchical diagnosis and treatment, and setting reasonable assessment indicators for the level of information available from healthcare institutions can significantly reduce the costs associated with information construction. These measures will enhance the benefits of information synergy, thereby facilitating the exchange of information within the healthcare system.
Keywords:
healthcare service coordination; information synergy; incentive mechanism; evolutionary game MSC:
91A80
1. Introduction
In recent years, and with the development of information technology, hospitals at all levels have established medical information systems. However, these systems often operate in isolation, creating severe “information silos” [1]. This lack of interoperability leads to increased treatment costs and wasted medical resources. Patients’ medical information is stored in separate systems, making it difficult to share and utilize optimally [2].
Due to a lack of access to patients’ previous medical records, patients often undergo redundant consultations and diagnostic tests when they are transferred to another hospital [3]. Moreover, the fragmented nature of this information impedes the potential for additional value to be derived from the data. The effective utilization of clinical data can significantly aid physicians in their diagnostic processes and enhance the research capabilities of hospitals. Primary healthcare institutions, being in closer contact with patients, gather more continuous and comprehensive data on patients’ daily health status and medication usage. Conversely, general hospitals possess superior research capabilities and expertise in big data analysis, thus better leveraging health data [4]. However, the information barriers between general hospitals and primary healthcare institutions obstruct efficient data sharing. Consequently, general hospitals have limited access to the necessary data for research, while primary healthcare institutions lack the clinical data and systematic knowledge required to offer personalized health management services to patients. This paper aims to explore strategies to incentivize information synergy among medical institutions.
In mature healthcare markets, the model where a single hospital provides all services to all patients is frequently being replaced, especially for patients with chronic diseases [5]. Hospitals are becoming more deeply integrated with other primary healthcare providers, such as family doctors, clinics, pharmacies, and rehabilitation centers, forming interdependent ecosystems. For instance, in the United States, leading retail pharmacies now offer a range of routine diagnostic and treatment services. Similarly, in China, the government is promoting the decentralization of healthcare services by significantly expanding family doctor services, community health centers, and third-party service providers [6]. This integration fosters a more efficient and patient-centric approach to healthcare delivery. Patients’ health is generally managed by healthcare organizations, where primary medical institutions deliver routine care and general hospitals provide complex and highly specialized treatments. General hospitals predominantly offer intricate diagnostic and treatment services, while primary medical institutions handle daily and post-acute care, along with health management services. For example, in the United States, Accountable Care Organizations (ACOs) are voluntary groups of healthcare providers, such as hospitals, physicians, and clinics, that collaborate to manage the health of specific patient populations.
Such integration necessitates information synergy across institutions, including bidirectional referral information sharing, telemedicine, and resident health records. In China, hospitals’ willingness to participate in medical information sharing remains low, resulting in patients’ diagnostic information being stored in static, fragmented forms that cannot be effectively utilized. According to the sampling survey report conducted by the China Hospital Information Management Association (CHIMA) in 2021–2022 (source: https://www.chima.org.cn/Html/News/Articles/16012.html, accessed on 10 March 2024), 69.21% of Chinese medical institutions participated in regional health information sharing. However, only about 60% of these institutions used bidirectional referrals, electronic medical record sharing, and resident health record sharing functionalities. Furthermore, less than 30% conducted collaborative examinations, highlighting a significant deficiency in information synergy among medical institutions.
Implementing information synergy between hospitals faces several obstacles. Firstly, it increases costs [3]. Verifying, storing, and synchronizing medical data are complex processes that require significant resources and time. For general hospitals, sharing knowledge through telemedicine or collaborative data analyses consumes expert resources, potentially impacting their operational efficiency and increasing costs. Secondly, there is a low level of trust in general hospitals towards information from primary healthcare institutions, as evidenced by the need for repeated tests during patient referrals [4,7]. With many countries, including China, exploring bundled payment mechanisms [8,9,10], these additional tests increase the costs for medical institutions and reduce their revenue. Given the above issues, studying the factors influencing the development of medical information infrastructure and decisions regarding data sharing incentives is of practical significance.
Game theory methods can analyze the benefits and costs associated with the decision-making behaviors of stakeholders within a system. Information collaboration in healthcare systems represents a scenario in which participants must weigh up their long-term interests. Evolutionary game theory, by modeling the imitation of behaviors among groups with bounded rationality, can dynamically reflect the evolution of strategic choices and their optimal strategies. This paper focuses on how members of healthcare systems make decisions on further information construction to maximize their own benefits, considering the synergistic effects of these decisions and the degree of mutual recognition surrounding the information. Therefore, we developed an evolutionary game model involving different levels of healthcare institutions, focusing on the impact of factors such as the information amount, information synergy benefits, information construction costs, and social and governmental incentives on the strategic choices of the participants.
Through an analysis of the evolutionary game model, this paper attempts to address the following three questions:
- (1)
- What decisions will general hospitals and medical institutions make regarding information construction?
- (2)
- What are the main factors influencing the decisions of general hospitals and primary healthcare institutions?
- (3)
- How will these influencing factors affect the evolutionary paths of general hospitals and primary healthcare institutions?
The remaining structure of this paper is as follows: Section 2 provides a brief review of the related literature. Section 3 describes the construction and analysis of the evolutionary game model. Section 4 conducts a numerical simulation using the model. Section 5 provides the results and discussions. Section 6 concludes with implications for management.
2. Literature Review
Our work involves coordination between different healthcare institutions, as well as the sharing of health information and medical knowledge for collaborative innovation.
2.1. Coordination between Different Healthcare Institutions
Our study addresses the coordination within the healthcare system, acknowledging the variance in expertise across different levels of healthcare institutions and their respective roles in patient health management. This variation implies that as patients’ health conditions change, they transition between different healthcare providers [5]. Through coordination among healthcare institutions, the quality of patient experiences can improve by 3.2%, and their 30-day readmission rate can reduce by 6.6%. However, these benefits entail additional costs [11]. Therefore, effective coordination within the healthcare system requires appropriate incentives, with payment methods being a primary focus in related research.
Traditional payment methods, such as fees-for-service (FFS), often lead to excessive care for patients and a low willingness for inter-institutional collaboration [8]. Compared to traditional payment methods, penalty contracts can align efforts with system-wide or socially optimal outcomes [5]. Bundled payments that include gainsharing can achieve a “triple win” for different levels of healthcare institutions and payers, although the specific payment schemes involved need to be carefully designed [10,12]. Research comparing four common payment methods—fee-for-service (FFS), capitation, GP fundholding, and penalty schemes—found that the latter two effectively incentivize primary medical institutions to improve the quality of health management services, even though marginal treatment costs increase [9]. Thus, effective coordination within the healthcare system necessitates intervention through appropriate mechanisms by the government and society [13]. Moreover, the allocation of medical resources can influence patient choices, necessitating the redistribution of resources to improve coordination [14]. Studies have shown that the moderate vertical integration of medical resources can enhance efficiency, although excessive integration might not yield corresponding benefits [4,7].
Existing research primarily focuses on the coordination of the capabilities of services among healthcare institutions. However, in the digital era, as patients transition between providers, the coordination of medical information could significantly enhance the quality and efficiency of the healthcare system. More attention has been given to the benefits of health information construction for the healthcare system [1,2,15]. Regarding the motivation for information coordination, studies have analyzed whether competitive private healthcare institutions should engage in information sharing [3] and the decision-making process for information exchange within healthcare alliances [6]. Nevertheless, there is a lack of research on the value creation of information coordination between different levels of healthcare institutions.
2.2. Service Coordination for Innovation and Information Synergy
Our study on medical information coordination is broadly related to information collaboration and service innovation. A mature service network, particularly a healthcare system, requires the collaboration of different participants for technological development and value creation. Collaboration between users and service providers [16,17,18], and among service providers [19,20], has been extensively studied. The heterogeneity of participants, the elasticity of outputs, and the costs influence the equilibrium level of collaborative efforts and utility, thereby affecting the decisions of each participant [16]. In the digital context, information sharing promotes collaboration, which has been widely researched in manufacturing and retail [21,22], as well as in service sectors [23,24,25,26]. Within the segmented field of healthcare services, substantial research has also been conducted [27].
Since the generation of information, such as the real-time changes in patient health data, is continuous, innovation based on this information is also a long-term dynamic decision-making process. This also makes it difficult for participants to make fully rational decisions at the outset of innovation. Instead, they often need to imitate the strategies of successful groups within the system based on the observed benefits. Evolutionary game theory models are suitable for analyzing the dynamic decisions of organizational collaborations and interactions. Information construction and coordination are revealed to be long-term strategies and dynamic processes [28,29,30]. Evolutionary game theory has been widely applied to organizational collaboration in various fields, including carbon emissions [31,32], corporate governance [33,34], digital construction [35], and healthcare services [36,37]. In the field of medical information coordination, since patient health management is a long-term process, the coordination of medical information among related healthcare institutions is also a dynamic decision-making process. Existing studies have used evolutionary game theory models to describe the process of information construction [6,27]. This paper, building on the evolutionary game models of different levels of healthcare institutions, considers the impact of information coordination benefits on members and examines the role of primary hospitals in information sharing based on the degree of mutual recognition of that information.
3. Evolutionary Game Model
3.1. Model Description and Assumptions
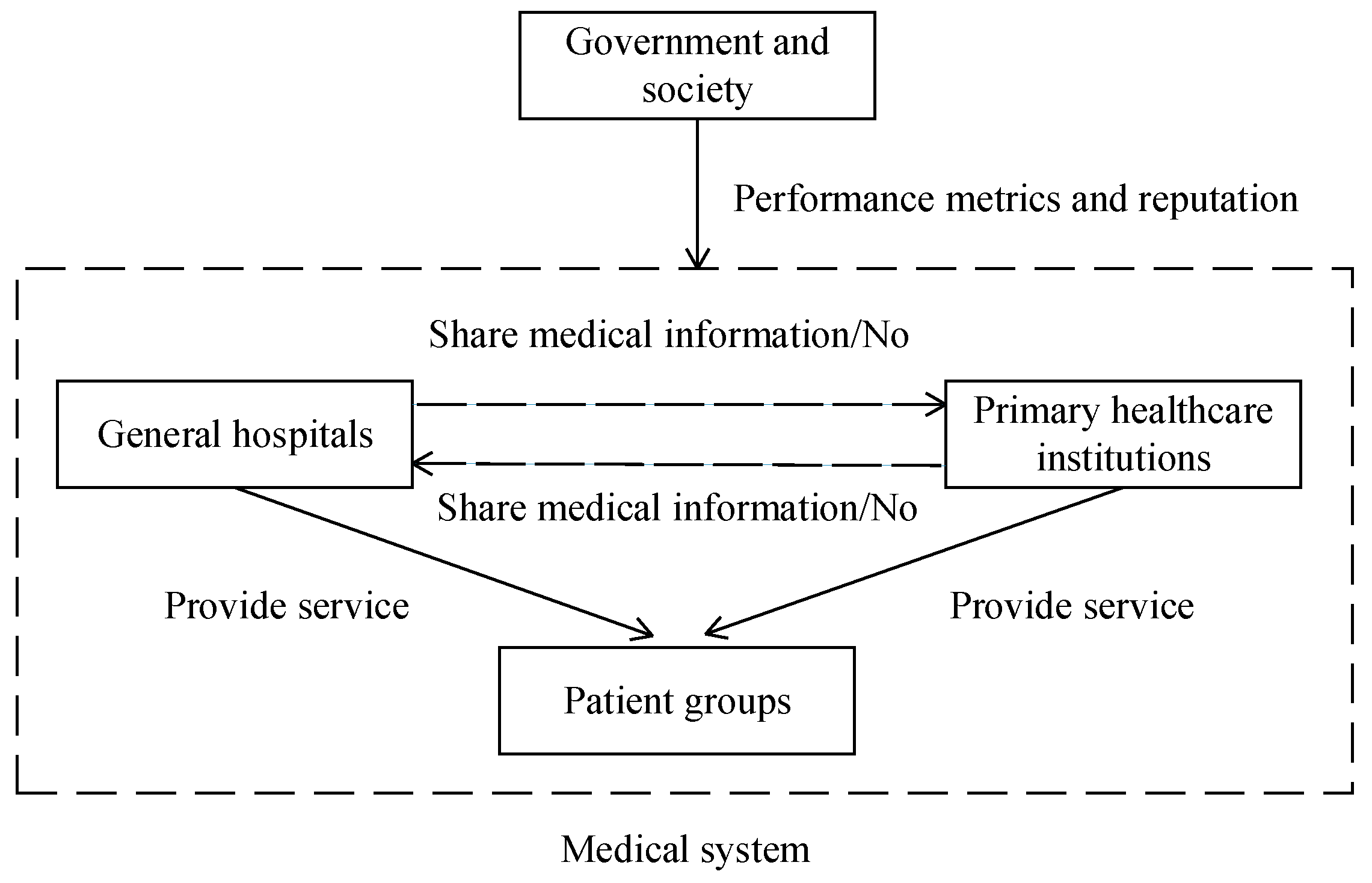
This paper examines a healthcare system composed of general hospitals and primary healthcare institutions, where each entity decides whether to implement further information construction and share medical information based on their specific circumstances. Typically, when medical institutions engage in further information construction, service providers from different institutions can access patients’ historical treatment and examination data in real time. Additionally, they can share medical knowledge through telemedicine and other methods, which enhances diagnostic efficiency while preventing redundant consultations and tests. This process reduces the costs for patients during visits and transfers between hospitals. In the context of bundled payments, hospitals can also realize substantial cost savings, thereby achieving greater benefits.
In many countries, such as China, public hospitals predominantly lead the healthcare system. The government can motivate medical institutions to implement information construction by establishing relevant performance evaluation metrics. Given that healthcare is a public service, a robust information system can elevate the social reputation of medical institutions. However, information construction requires a significant financial investment from these institutions. Consequently, they must consider the costs and benefits carefully to decide whether to proceed with information construction. The system’s structure is illustrated in Figure 1.
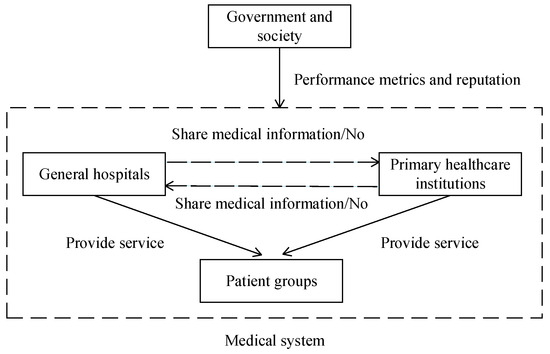
Figure 1.
The structure of a medical system with information synergy.
To develop an effective model based on evolutionary game theory, the following assumptions are put forward:
Assumption 1.
During the process of providing healthcare services, both general hospitals and primary healthcare institutions can choose whether to engage in further information construction and share medical information. Let () denote the size of the medical information database (G for general hospitals, P for primary healthcare institutions). However, for medical institutions, there exists a difference in the degree of the information’s mutual recognition; higher-level hospitals often cannot fully trust the information from lower-level institutions [7]. We assume the trust level of general hospitals towards primary healthcare institutions is (). Thus, general hospitals can utilize the information quantity .
Assumption 2.
When healthcare system members engage in further information construction, they incur direct benefits as well as costs. The direct benefits come from the direct utilization of information from other institutions, even if they themselves have not engaged in information construction. For general hospitals, information from primary healthcare institutions can help reduce consultation times and lower the costs of repeat examinations. Assuming they can obtain these benefits is denoted as for . In terms of primary healthcare institutions, they can assist in patient health management through the information platform provided by general hospitals, contingent on their own ability to collect patient health information. Assuming they can obtain this benefit is denoted as for . The cost is noted as . We assume that costs increase convexly with the amount of information gained, such that an amount of information of incurs a cost equal to , where and . Cost convexity is a common assumption in the relevant literature [16].
Assumption 3.
When both members in the healthcare system engage in information construction, they generate information synergy, which can be utilized, through methods like big data collection, for purposes such as assisting in diagnosis and treatment, thereby obtaining information synergy benefits. The synergy benefits that general hospitals and primary healthcare institutions, denoted as , can achieve are denoted as and , respectively [16,17,19].
Assumption 4.
Due to government and societal concerns regarding public health services, healthcare system members engaging in further information construction can gain reputation benefits denoted as for , such as attracting more patients who prefer hospitals with higher information levels. Additionally, a portion of the revenue for public hospitals comes from government subsidies, and the government sets related performance metrics. Members not engaging in information construction will face a potential loss of their government subsidy, denoted as .
Assumption 5.
The probability of the general hospital choosing the S strategy is , and the probability of it not choosing the S strategy is . Simultaneously, the probability of primary hospitals choosing the S strategy is , and the probability of them not choosing the S strategy is .
A description of the parameters used in this paper is given in Table 1.

Table 1.
The model’s parameters and their descriptions.
As participants in the game, members of the healthcare system decide whether to engage in further information construction and information sharing based on which strategy yields a greater profit. According to the above assumptions, the payoff matrix is shown in Table 2.
Table 2.
Payoff matrix for general hospitals and primary healthcare institutions.
3.2. Model Analysis
Let be the expected utility of a general hospital who chose the S strategy, be the expected utility of a general hospital who chose the N strategy, be the expected utility of a primary healthcare institution who chose the S strategy, and be the expected utility of a primary healthcare institution who chose the N strategy. According to Table 2, we can obtain the utilities of the general hospitals and primary healthcare institutions as follows:
Therefore, the average expected utility of the general hospitals and primary healthcare institutions can be obtained. Let and represent their average expected utility, respectively, which are presented as follows:
According to the Malthusian dynamic equation [38], the replicator dynamic equations of the general hospital and primary healthcare institution are as follows:
According to the above replication dynamic equations, when and , five evolutionary equilibrium points , , , , and can be obtained, where and . After the equilibrium points are obtained, we followed the methods of Friedman (1991) [38], determining the stability of the equilibrium point through the local stability of the Jacobian matrix.
According to the Jacobian matrix (9), the determinant (Det) and the trace (Tr) can be calculated:
If and , the equilibrium point of the replication dynamic equation is locally stable asymptotically and the equilibrium point is an evolutionarily stable strategy (ESS) [39]. Based on the equilibrium results displayed in Table 3, all nine scenarios demonstrate the existence of an evolutionarily stable strategy (ESS), which can be categorized into four distinct cases. The equilibrium outcome of the evolution is primarily influenced by the relationship between the magnitude of the payer’s penalty and the difference between the costs and benefits of information collaboration:
Table 3.
Analysis of equilibrium points.
- (1)
- When , , and at least one of or holds (Case 1), the healthcare system will eventually evolve to .
- (2)
- When , , and at least one of or holds (Case 2), the healthcare system will eventually evolve to .
- (3)
- When , , , and holds (Case 3), the healthcare system will eventually evolve to or .
- (4)
- When and holds or and holds (Case 4), the healthcare system will eventually evolve to or .
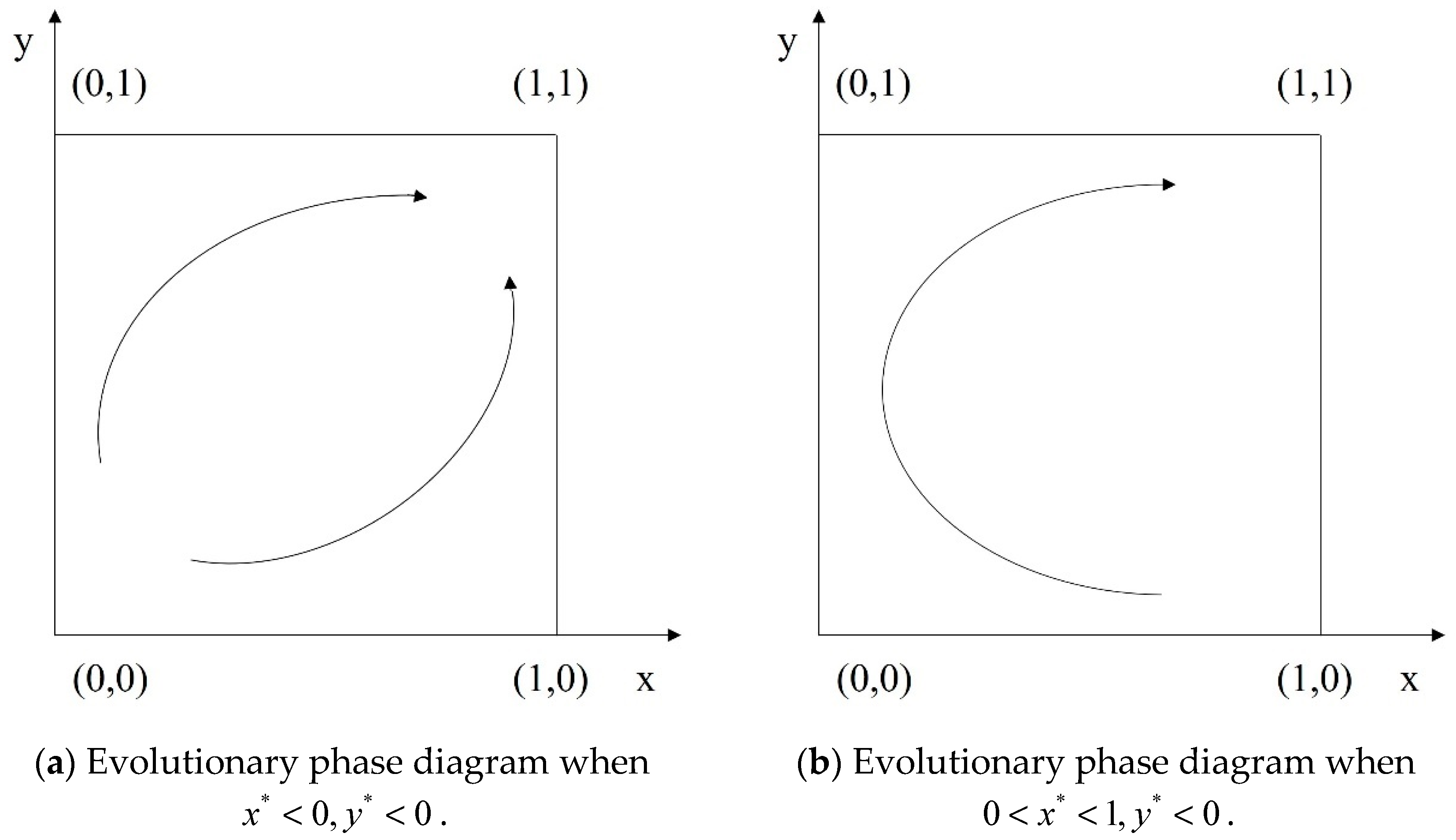
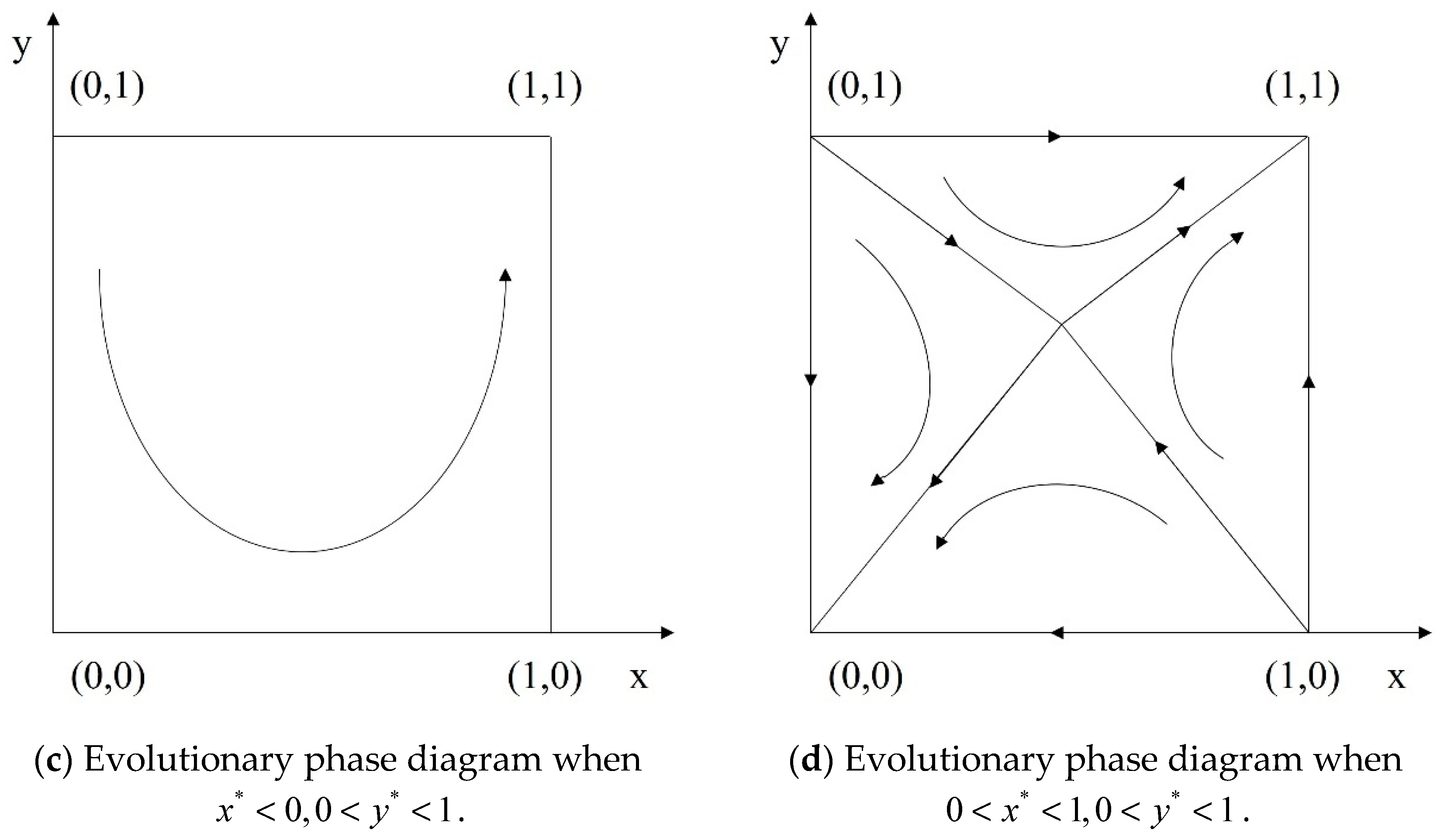
Our anticipated evolutionary equilibrium outcome is for both general hospitals and primary healthcare institutions to engage in further information construction and information sharing, thereby achieving synergy. As illustrated in Table 3, only in three scenarios under Case 2 and in Case 3 does the value of ultimately evolve to . These scenarios are of primary interest. The phase diagrams illustrating these scenarios are presented in Figure 2. Figure 2a–c correspond to scenarios 4, 5, and 6 in Case 2, where the healthcare system will eventually evolve to , meaning both general hospitals and primary healthcare institutions choose to engage in information synergy. Figure 2d corresponds to Case 3 where, depending on the initial conditions of the system, the healthcare system will eventually evolve to either or . In this case, both general hospitals and primary healthcare institutions will either both adopt information synergy or both refrain from it, indicating a consistent strategy.
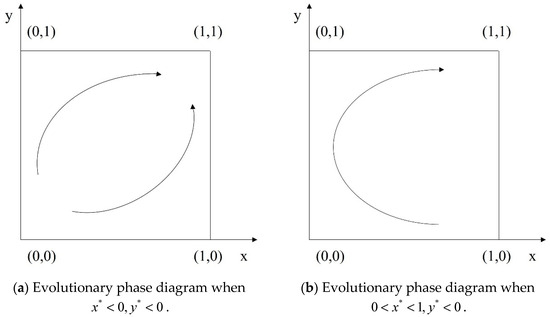
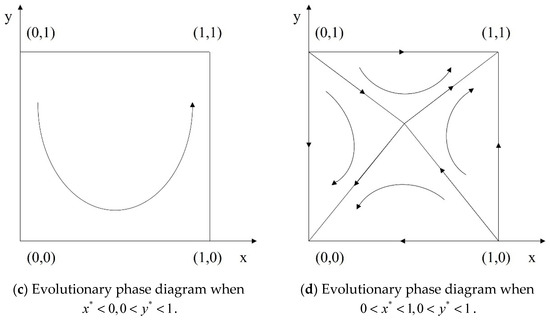
Figure 2.
Evolutionary phase diagrams of information synergy decisions.
4. Discussion
To better illustrate the process of information coordination between different levels of healthcare institutions, numerical experiments were conducted to validate the model’s effectiveness and to reveal the impact of various parameters on its evolutionary outcomes. To more appropriately set the corresponding parameters, we referred to reports published by CHIMA and data from hospitals in Zhenjiang, with some adjustments made for information security. According to dynamic replication Equations (7) and (8), the parameters that need to be set include , , , , , , , , , , , , , and . Under the conditions of Case 2 and Case 3, it is required that () and (). Detailed parameter settings are provided in Table 4.
Table 4.
Initial values of parameters.
4.1. The Impact of the Volume of Information and the Degree of Recognition
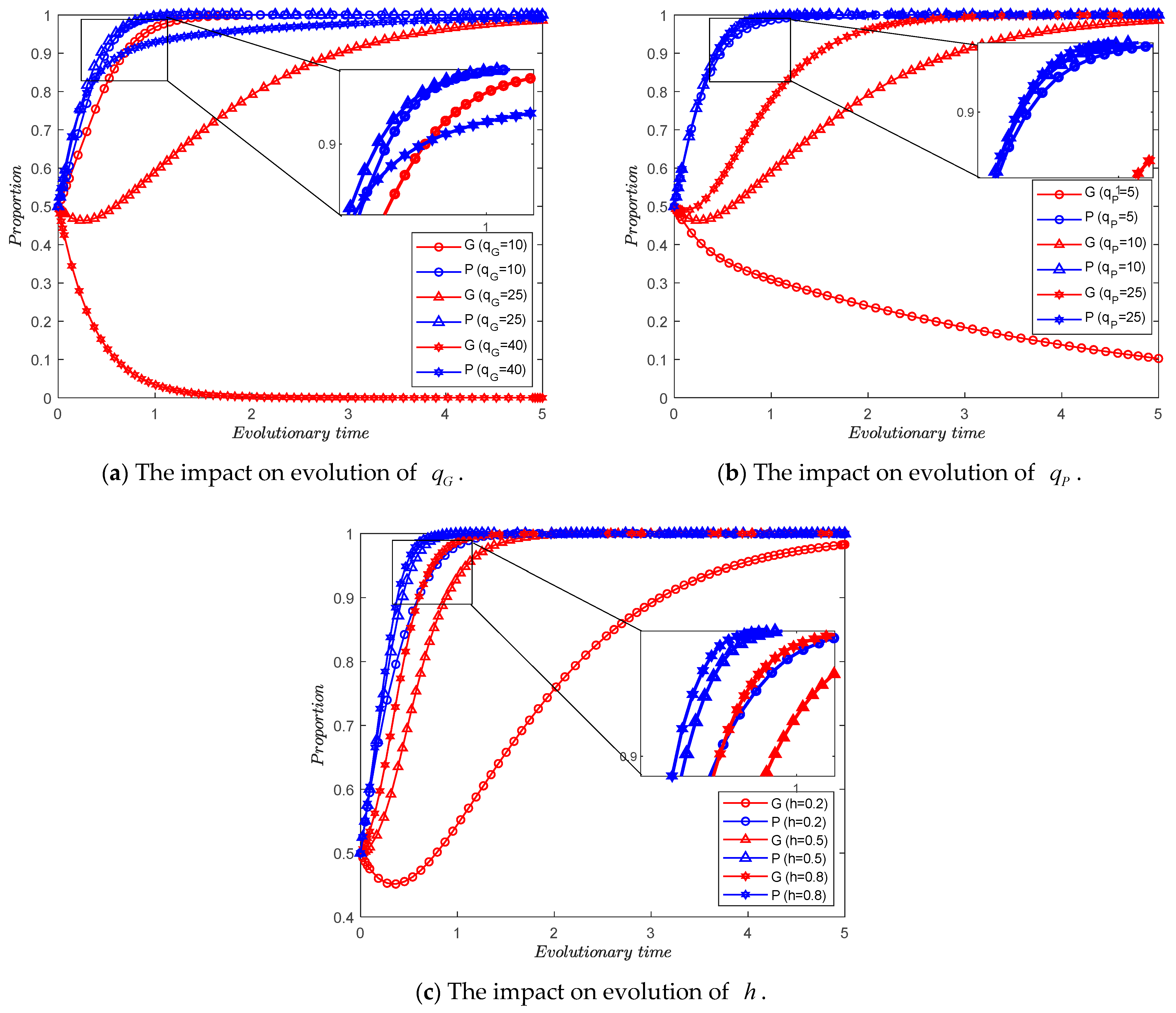
First, we analyze the impact of the basic amount of information from each medical institution and the degree of mutual recognition on the evolutionary trend of the medical system, respectively. We obtain Figure 3a by letting take values of 10, 25, and 40. By letting take values of 5, 10, and 25, respectively, we obtain Figure 3b. By letting take values of 0.2, 0.5, and 0.8, respectively, we obtain Figure 3c.
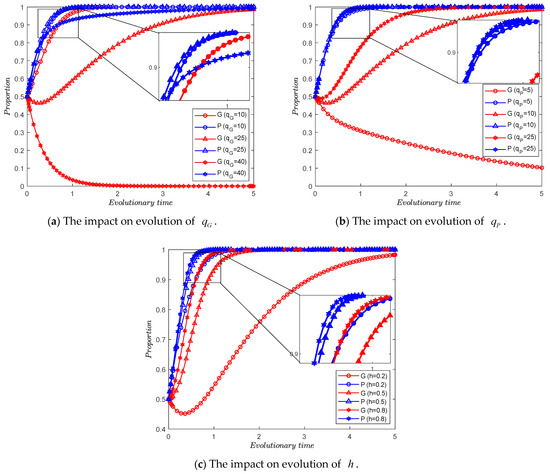
Figure 3.
The impact of the databases’ volume and the degree of mutual recognition.
Observation 1.
As the amount of information shared by general hospitals increases, the medical system evolves gradually more slowly for both sides sharing medical information.
Observation 2.
As the amount of information shared by primary healthcare institutions increases, the medical system evolves gradually faster for both sides sharing medical information.
Observation 3.
As the degree of mutual recognition increases, the medical system evolves gradually faster for both sides sharing medical information.
From Figure 3, we can obtain Observations 1 and 2. In the context of healthcare informatization, the roles and motivations of general hospitals and primary healthcare institutions differ significantly. When the information databases of general hospitals become sufficiently large, it indicates that their stored information is comprehensive and includes patients’ daily health information. In such scenarios, general hospitals can leverage this information to significantly enhance the efficiency of their medical services and reduce costs. However, maintaining this information synergy requires a higher investment and more personnel to support primary healthcare institutions, which implies higher costs. Therefore, as the information databases of general hospitals expand, their likelihood of them participating in information synergy decreases. When the repository becomes sufficiently large, general hospitals may choose not to undertake further information construction or share information.
Conversely, when the information databases of primary healthcare institutions are relatively small, the benefits that general hospitals can derive from information synergy are minimal, further reducing their likelihood of participating. Primary healthcare institutions, on the other hand, are always motivated to improve information construction and share information, as collaboration can enhance their reputation and persuade more patients to seek care there. However, as shown in Figure 3a, the participation of general hospitals in information synergy significantly influences primary healthcare institutions. When general hospitals do not participate in collaboration, the likelihood of primary healthcare institutions engaging in such collaboration also decreases.
The degree of the mutual recognition of their medical information significantly impacts the evolution of the system. This study primarily considers the extent to which general hospitals recognize information from primary healthcare institutions, reflecting the volume of information from primary healthcare institution databases that general hospitals can utilize. As the degree of mutual recognition increases, the amount of usable information available to general hospitals grows, thereby increasing their likelihood of participating in information synergy.
Additionally, as shown in Figure 3, when the amount of information or the degree of its recognition is within a certain range, the probability of general hospitals choosing information collaboration first decreases and then increases (red curve). This occurs because, in the initial stage, the participation of primary healthcare institutions is low, leading to insufficient benefits for general hospitals from information synergy. However, as the participation of primary healthcare institutions increases, the involvement of general hospitals also rises. It can be observed that an increase in the amount of information available and the degree of its recognition among participants helps mitigate this phenomenon. This is because, when these values are high, general hospitals can still obtain sufficient benefits from synergy even if the proportion of primary healthcare institutions engaging in information collaboration is not high.
4.2. The Impact of the Benefits of Information Synergy
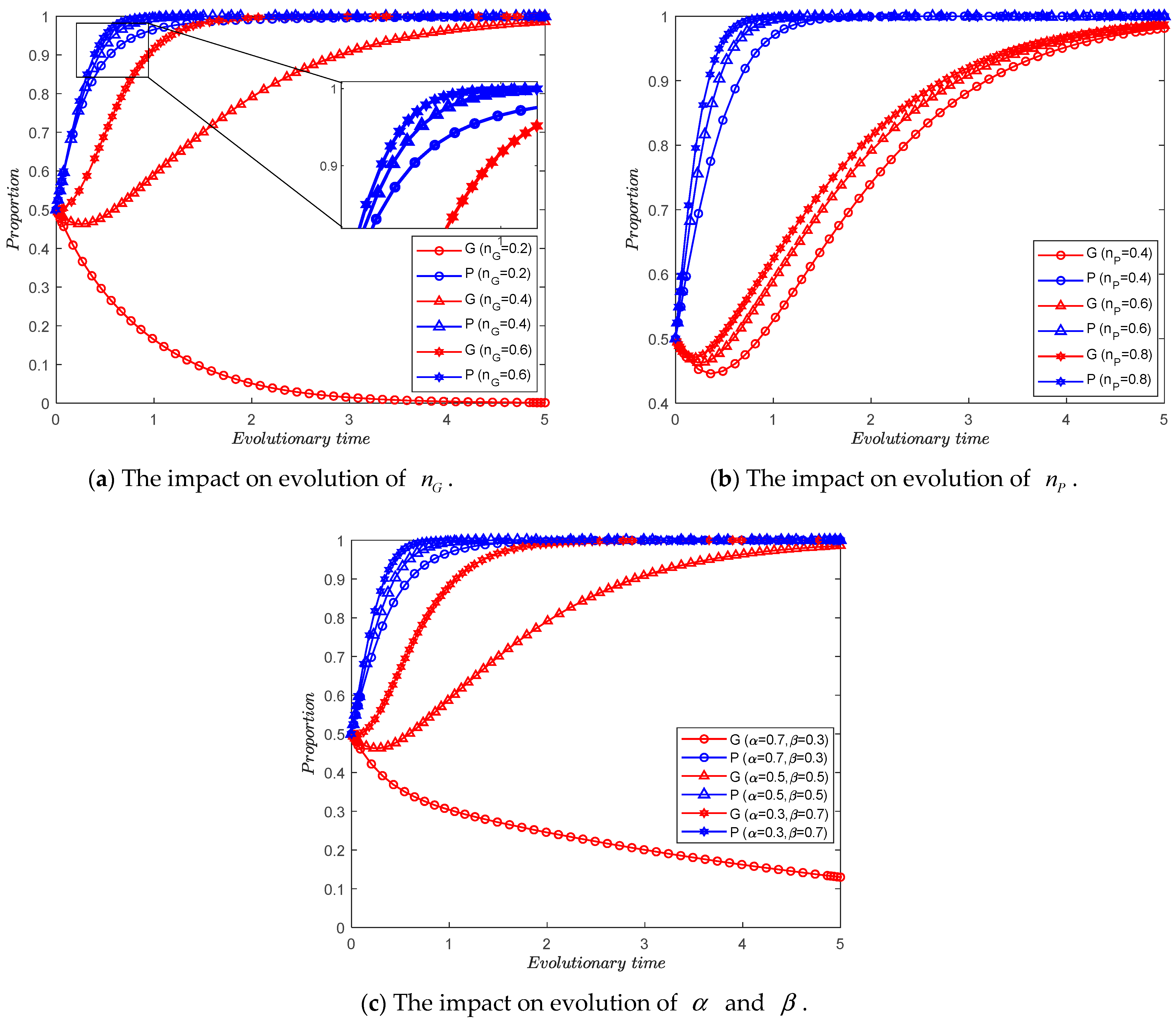
Second, we analyze the impact of the benefit of information synergy for each medical institution on the evolutionary trend of the medical system. By letting take values of 0.2, 0.4, and 0.6, respectively, we obtain Figure 4a. By letting take values of 0.4, 0.6, and 0.8, respectively, we obtain Figure 4b. By letting take values of , , and , respectively, we obtain Figure 4c.
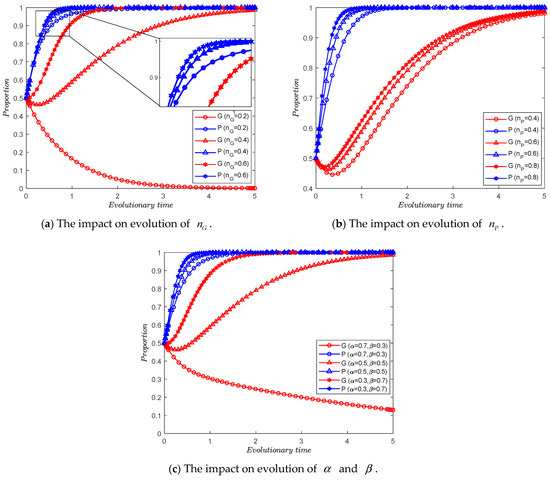
Figure 4.
The impact of the synergy benefits coefficient and the information synergy elasticity coefficient.
Observation 4.
As the synergy benefits coefficient of each medical institution increases, the medical system evolves gradually faster for both sides sharing medical information.
Observation 5.
As the information synergy elasticity coefficient of general hospitals decreases and that of primary healthcare institutions increases, the medical system evolves gradually faster for both sides sharing medical information.
Observations 4 and 5 similarly describe the impact of collaborative benefits on the decision-making of healthcare system members, but they focus more on the formation of collaborative benefits. Parameters and illustrate the dependence of different medical institutions on information synergy, while parameters and depict the contribution of different medical institutions to collaborative value. These parameters mainly vary depending on the type of diseases patients have, characterized by the severity and duration of their disease.
From the perspective of severity, when a patient’s disease is more severe, their care relies more on the guidance of general hospitals. Hence, primary healthcare institutions, through information synergy within the healthcare system, such as remote consultations, can provide services to more patients and obtain greater collaborative benefits. Consequently, the value of is higher, and the likelihood of primary healthcare institutions participating in collaboration increases. Conversely, when a patient’s condition is less severe, patients can freely choose medical institutions, and visiting general hospitals might lead to resource misallocation, thus affecting efficiency. However, examination reports from primary healthcare institutions can save time for general hospitals during diagnosis, thereby bringing collaborative benefits to general hospitals. When the value of is higher, general hospitals can effectively improve their diagnostic efficiency through collaboration, thus enhancing their willingness to participate in collaboration.
From the perspective of disease duration, when the disease has a longer course, patient care and diagnosis rely more on daily health information. Due to the convenience and proximity of primary healthcare institutions to patients, they possess more daily health information, thus playing a more significant role in information synergy (). Conversely, when the disease’s course is shorter, diagnosis and treatment rely more on technology and experience, areas where general hospitals have more advantages. In the treatment of long-term diseases, such as chronic diseases, healthcare information synergy plays a more significant role, thereby increasing the likelihood of healthcare system members participating in collaboration.
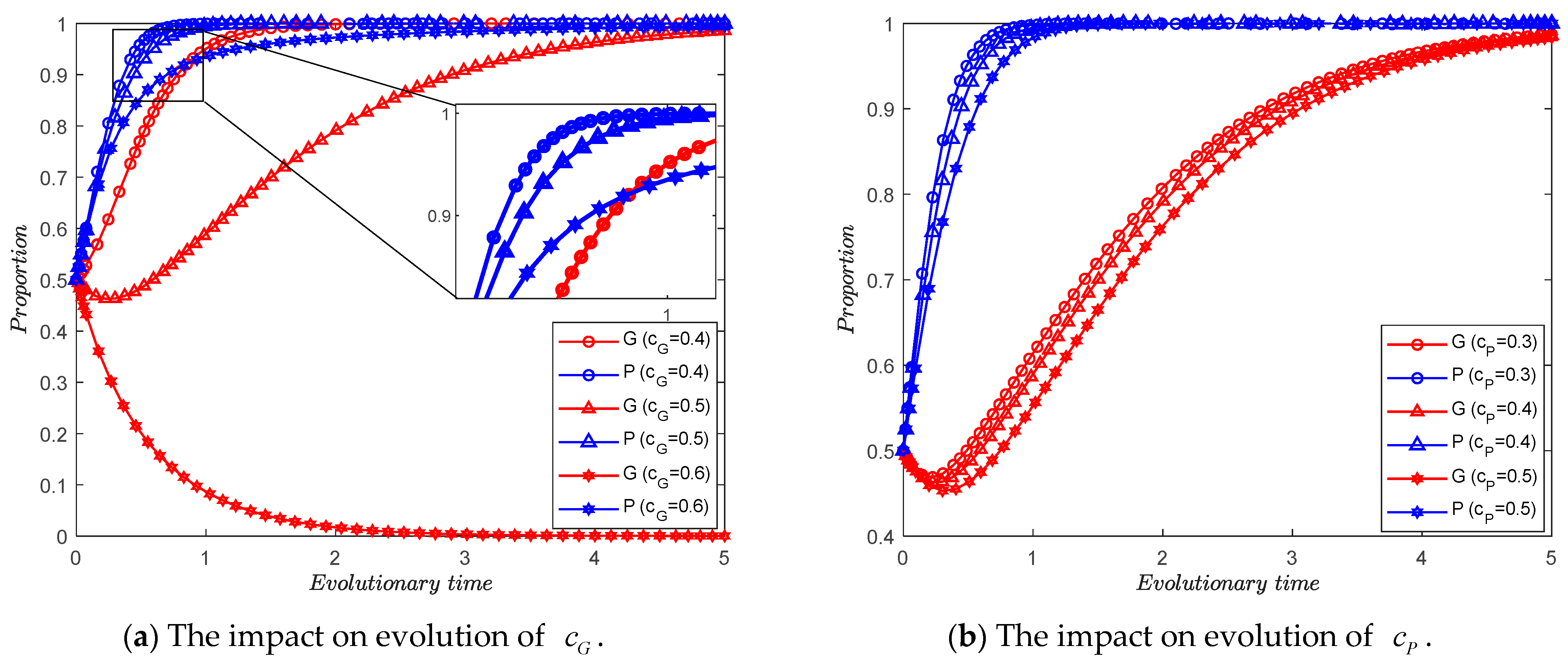
4.3. The Impact of the Cost of Information Construction
Third, we analyze the impact of the cost of information construction for each medical institution on the evolutionary trend of the medical system. By letting take values of 0.4, 0.5, and 0.6, respectively, we obtain Figure 5a. By letting take values of 0.3, 0.4, and 0.5, respectively, we obtain Figure 5b.
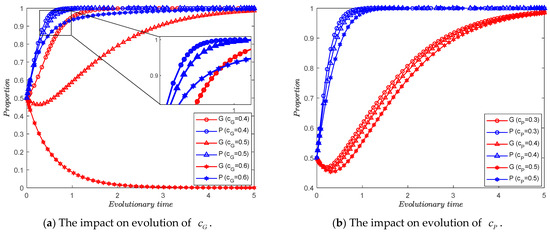
Figure 5.
The impact of the cost of information construction.
Observation 6.
As the information construction cost coefficient of each medical institution increases, the medical system evolves gradually more slowly for both sides sharing medical information.
Observation 6 can be derived from Figure 5, indicating that the higher the cost of further information construction for healthcare system members, the greater the likelihood that they will opt out of information synergy. For primary healthcare institutions, changes in costs primarily affect the speed of system evolution. However, for general hospitals, the large volume and complexity of their information mean that excessively high costs can hinder their decisions regarding information synergy. Thus, it can be observed that excessively high costs of information construction are detrimental to information synergy within the healthcare system.
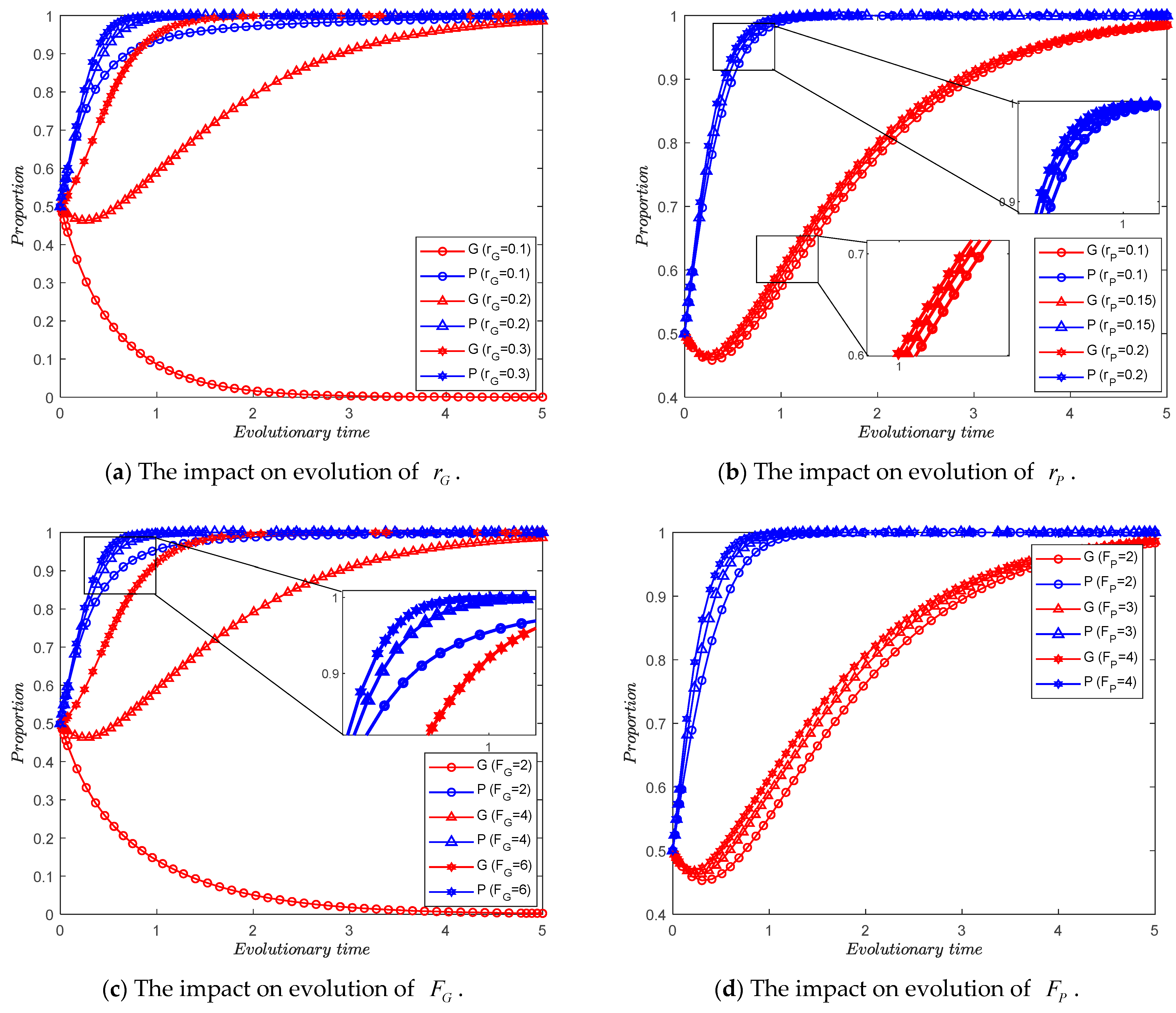
4.4. The Impact of the Societal and Government Incentives
Finally, we analyze the impact of societal and government interventions on the evolutionary trend of the medical system. By letting take values of 0.1, 0.2, and 0.3, respectively, we obtain Figure 6a. By letting take values of 0.1, 0.15, and 0.2, respectively, we obtain Figure 6b. By letting take values of 2, 4, and 6, respectively, we obtain Figure 6c. By letting take values of 2, 3, and 4, respectively, we obtain Figure 6d.
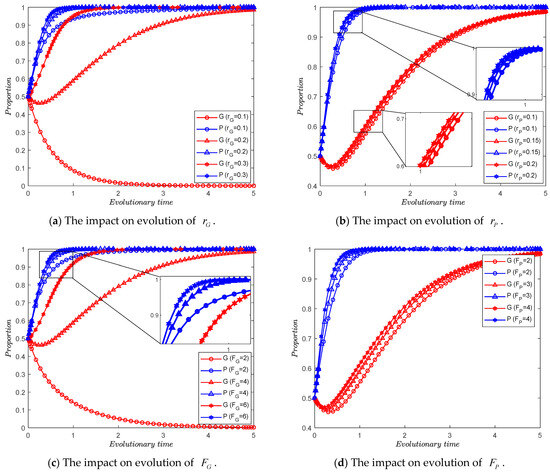
Figure 6.
The impact of the reputation of information construction and punishments from the government.
Observation 7.
As the reputation of information construction increases, the medical system evolves gradually faster for both sides sharing medical information.
Observation 8.
As the punishment for inadequate information construction increases, the medical system evolves gradually faster for both sides sharing medical information.
Observations 7 and 8 can be derived from Figure 6, indicating that when there is higher external attention paid to healthcare information collaboration—such as patients preferring medical institutions with higher levels of informatization and easier referral processes, or government-led healthcare payers establishing evaluation standards for information synergy—the resulting reputation benefits or penalties will affect the total revenue of healthcare system members, thereby influencing their decisions. Consequently, when societal attention is high, the likelihood of information synergy within the healthcare system increases.
5. Discussion and Managerial Implications
Insufficient healthcare informatization leads to inefficient medical services and the invalid diversion of patients, making information synergy within the healthcare system a focal point of academic research. Information synergy between general hospitals and primary healthcare institutions can promote the efficient division of labor within the healthcare system and enhance the service capabilities of primary healthcare institutions. Existing research primarily focuses on how policies can facilitate the allocation of resources allocation to general hospitals, often overlooking the role of primary healthcare institutions in information synergy.
This study finds that the credibility of the information from primary hospitals, their role in collaborative benefits, and the dependence of each member on information synergy significantly influence decisions regarding further information construction and sharing. By integrating evolutionary game theory, this research explores how these factors affect the speed at which the system achieves equilibrium in information synergy in terms of the long-term decisions of participants with different bounded rationalities, as well as how social and governmental interventions can improve information construction. In this paper, we propose two primary managerial implications based on the following dimensions.
5.1. Benefits of Medical Information Synergy
In the healthcare system, the ability of patients to freely choose their providers makes collaboration between general hospitals and primary healthcare institutions essential [7,40]. Information sharing in this context can greatly improve care efficiency and reduce medical costs. Consequently, various healthcare alliances have been formed to ensure an effective division of labor throughout the patient care process [5,41]. Our findings indicate that general hospitals, as leaders, play a crucial role in healthcare information collaboration. However, we also find that general hospitals are often reluctant to collaborate, especially when they do not foresee substantial benefits from such collaboration.
General hospitals possess high levels of expertise and a robust information infrastructure, making them more attractive to patients who prefer to receive services from these institutions. Consequently, general hospitals can achieve considerable revenue by independently serving patients. Their collaboration with primary healthcare institutions may introduce competition. Additionally, due to the varying nature of patient diseases, information from primary healthcare institutions does not always provide sufficient benefits to general hospitals, especially in cases of severe or short-term illnesses.
These challenges necessitate further improvements in primary healthcare institutions. First, there is a need to establish a solid health information database for patients, continuously tracking and updating their health status and medical interventions to improve the quality of information. On one hand, a larger volume of information enables more precise big data analyses, leading to greater benefits. On the other hand, patients may seek care across cities, making regional or even national databases particularly important. This often requires government-led initiatives, such as that by the National Institute of Health Data Science of China (source: http://www.mhdata.sdu.edu.cn/, accessed on 10 March 2024). Information platforms with official endorsements can attract participation from healthcare institutions. Second, it is essential to collaborate with research institutions to advance studies related to big data in healthcare, enhancing the level of diagnostic support technologies. These measures will ultimately increase the willingness of general hospitals to participate in information synergy. In the early stages of scientific research, high costs often become a barrier to further development. The government needs to implement effective incentives, such as funding support and talent development, to promote the growth of the health information industry.
5.2. Incentives for Information Synergy Behavior
In practice, the balance of benefits and costs significantly influences the information synergy decisions of healthcare system members, presenting challenges to the sustainability of such collaboration [42,43]. The process of information synergy often requires support from online systems, which can increase information security risks [44]. Additionally, the process of updating information can lead to distortions, adding extra costs for healthcare system members [3,6,43].
To address these challenges, it is crucial to build a comprehensive healthcare information synergy system and actively develop blockchain technology to ensure the efficiency and accuracy of information sharing. This involves the standardization of both office automation systems and information requirements, which needs to be driven by government policies from the top down. Additionally, encouraging patients to initially seek care at primary healthcare institutions can enhance the complementary nature of information synergy and tiered medical services, thereby increasing the patient preference for healthcare providers engaged in information synergy. The government can guide patients towards tiered medical care by implementing differentiated reimbursement systems and improving the medical standards of primary healthcare institutions.
6. Conclusions
With the application of technologies such as the Internet of Medical Things (IoMT), medical cyber–physical systems, machine learning, and big data (BD), the healthcare industry has recognized the importance of Industry 4.0. Information construction is particularly crucial for the coordination of the healthcare system, which comprises general hospitals and primary healthcare institutions. Given that participants have bounded rationality, it is necessary to consider their learning processes in their decision-making. Based on this, an evolutionary game model of information synergy in healthcare networks is proposed. Numerical simulations analyze the parameters affecting the collaborative benefits and the impact of interventions on participants’ strategy choices.
This study finds that, compared to general hospitals, primary healthcare institutions are more proactive in making decisions regarding information synergy. Furthermore, the further construction of their information databases influences general hospitals’ willingness to participate in information synergy. A well-established database can enhance collaborative benefits through the quantity and trustworthiness of its information, promoting information coordination within the healthcare system. Additionally, the decision for information synergy is influenced by the type of illness a patient has. General hospitals are more willing to engage in information synergy for patients with longer disease cycles and milder conditions. For acute or severe patients, general hospitals often need to invest more in information construction for information sharing, such as establishing remote consultation platforms and maintaining related medical staff, making them less inclined to participate in information synergy in these cases. This requires greater incentives from the government and society, the establishment of reasonable performance evaluation indicators, the active promotion of the tiered diagnosis and treatment concept, and the adjustment of medical expense subsidies to guide patients to choose hospitals with well-established information systems, thereby encouraging healthcare system members to further invest in information construction.
This study has certain limitations, which also provide directions for future research. Firstly, when establishing the evolutionary game model, some factors were not considered, such as the risks of information leakage and misdiagnosis. Including more influencing factors could make the model more realistic. Additionally, future research could analyze an evolutionary game model with optimal control, as the behavior of healthcare system members and external interventions often affect the evolutionary equilibrium. Finally, future studies could empirically test the conclusions of this research using real-world data.
Author Contributions
Conceptualization, S.Y. and H.W.; methodology, S.Y. and H.W.; software, S.Y.; validation, S.Y.; investigation, S.Y.; resources, S.Y.; data curation, S.Y.; writing—original draft preparation, S.Y.; writing—review and editing, S.Y. and H.W.; visualization, S.Y.; supervision, H.W.; project administration, H.W. All authors have read and agreed to the published version of the manuscript.
Funding
This work was supported by the Program of the National Natural Science Foundation of China [grant number: 72071042].
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
The original contributions presented in the study are included in the article, further inquiries can be directed to the corresponding author.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Núñez-Merino, M.; Maqueira-Marín, J.M.; Moyano-Fuentes, J.; Castaño-Moraga, C.A. Product development process for a new healthcare service in the Industry 4.0 context: An action research approach. Prod. Plan. Control 2024, 1–20. [Google Scholar] [CrossRef]
- Bardhan, I.R.; Thouin, M.F. Health information technology and its impact on the quality and cost of healthcare delivery. Decis. Support Syst. 2013, 55, 438–449. [Google Scholar] [CrossRef]
- Niu, B.; Xu, H.; Dai, Z. Check Only Once? Health Information Exchange between Competing Private Hospitals. Omega 2022, 107, 102556. [Google Scholar] [CrossRef]
- Li, Z.-P.; Wang, J.-J.; Chang, A.-C.; Shi, J. Capacity reallocation via sinking high-quality resource in a hierarchical healthcare system. Ann. Oper. Res. 2021, 300, 97–135. [Google Scholar] [CrossRef]
- Adida, E.; Bravo, F. Contracts for Healthcare Referral Services: Coordination via Outcome-Based Penalty Contracts. Manag. Sci. 2019, 65, 1322–1341. [Google Scholar] [CrossRef]
- Dong, C.; Liu, J.; Mi, J. Information-Driven Integrated Healthcare: An Analysis of the Cooperation Strategy of County Medical Community Based on Multi-Subject Simulation. Healthcare 2023, 11, 2019. [Google Scholar] [CrossRef]
- Wang, J.-J.; Li, Z.-P.; Shi, J.; Chang, A.-C. Hospital referral and capacity strategies in the two-tier healthcare systems. Omega 2020, 100, 102229. [Google Scholar] [CrossRef]
- Adida, E.; Mamani, H.; Nassiri, S. Bundled Payment vs. Fee-for-Service: Impact of Payment Scheme on Performance. Manag. Sci. 2017, 63, 1606–1624. [Google Scholar] [CrossRef]
- Wang, Z.; Zhou, W.; Zheng, Z. Encouraging preventive services in primary care through payment schemes. Comput. Ind. Eng. 2022, 171, 108485. [Google Scholar] [CrossRef]
- Ghamat, S.; Zaric, G.S.; Pun, H. Care-coordination: Gain-sharing agreements in bundled payment models. Prod. Oper. Manag. 2021, 30, 1457–1474. [Google Scholar] [CrossRef]
- Lan, Y.; Chandrasekaran, A.; Goradia, D.; Walker, D. Collaboration Structures in Integrated Healthcare Delivery Systems: An Exploratory Study of Accountable Care Organizations. Manuf. Serv. Oper. Manag. 2022, 24, 1796–1820. [Google Scholar] [CrossRef]
- Bravo, F.; Levi, R.; Perakis, G.; Romero, G. Care coordination for healthcare referrals under a shared-savings program. Prod. Oper. Manag. 2023, 32, 189–206. [Google Scholar] [CrossRef]
- Teymourifar, A.; Kaya, O.; Ozturk, G. Contracting models for pricing and capacity decisions in healthcare systems. Omega 2021, 100, 102232. [Google Scholar] [CrossRef]
- Cao, X.; Rajagopalan, S.; Tong, C. Impact of vertical integration in a referral-based healthcare system. Omega 2024, 123, 102998. [Google Scholar] [CrossRef]
- Tiwari, M.; Bryde, D.J.; Stavropoulou, F.; Dubey, R.; Kumari, S.; Foropon, C. Modelling supply chain Visibility, digital Technologies, environmental dynamism and healthcare supply chain Resilience: An organization information processing theory perspective. Transp. Res. Part E Logist. Transp. Rev. 2024, 188, 103613. [Google Scholar] [CrossRef]
- Liu, W.; Chai, R.; Cao, X.; Fang, X.; Yang, Y. Promoting product idea contribution of heterogeneous users for product improvement in online innovation communities. Int. J. Prod. Res. 2022, 61, 3599–3620. [Google Scholar] [CrossRef]
- Andritsos, D.A.; Tang, C.S. Incentive Programs for Reducing Readmissions when Patient Care is Co-Produced. Prod. Oper. Manag. 2018, 27, 999–1020. [Google Scholar] [CrossRef]
- Yan, L.; Yan, X.; Tan, Y.; Sun, S.X. Shared minds: How patients use collaborative information sharing via social media platforms. Prod. Oper. Manag. 2019, 28, 9–26. [Google Scholar] [CrossRef]
- Zheng, Y.; Zhou, B.; Bai, C.; Cai, Q. Differential game model of the cross-organizational cooperative r&d of general purpose technologies under two-way collaboration. Chin. J. Manag. Sci. 2023, 31, 255–265. [Google Scholar]
- Tang, Q.; Wang, C.; Feng, T. Research on the Group Innovation Information-Sharing Strategy of the Industry–University–Research Innovation Alliance Based on an Evolutionary Game. Mathematics 2023, 11, 4161. [Google Scholar] [CrossRef]
- Liu, Z.; Zhang, D.J.; Zhang, F. Information Sharing on Retail Platforms. Manuf. Serv. Oper. Manag. 2021, 23, 606–619. [Google Scholar] [CrossRef]
- Tan, Y.; Huang, X.; Li, W. Does blockchain-based traceability system guarantee information authenticity? An evolutionary game approach. Int. J. Prod. Econ. 2023, 264, 108974. [Google Scholar] [CrossRef]
- Li, K.; Liang, C. Exploring the promotion of blockchain adoption in the healthcare industry through government subsidies. Kybernetes, 2023; ahead-of-print. [Google Scholar] [CrossRef]
- Sun, M.; Chai, Q.; Ng, C.T. Managing the quality-speed tradeoff in blockchain-supported healthcare diagnostic services. Omega Int. J. Manag. Sci. 2023, 120, 102911. [Google Scholar] [CrossRef]
- Wang, G.; Li, J.; Hopp, W.J.; Fazzalari, F.L.; Bolling, S.F. Using Patient-Specific Quality Information to Unlock Hidden Healthcare Capabilities. Manuf. Serv. Oper. Manag. 2019, 21, 582–601. [Google Scholar] [CrossRef]
- Atasoy, H.; Chen, P.-Y.; Ganju, K. The Spillover Effects of Health IT Investments on Regional Healthcare Costs. Manag. Sci. 2018, 64, 2515–2534. [Google Scholar] [CrossRef]
- Gao, Y.; Zhu, Z.; Yang, J. An Evolutionary Game Analysis of Stakeholders’ Decision-Making Behavior in Medical Data Sharing. Mathematics 2023, 11, 2921. [Google Scholar] [CrossRef]
- Merrill, J.A.; Deegan, M.; Wilson, R.V.; Kaushal, R.; Fredericks, K. A system dynamics evaluation model: Implementation of health information exchange for public health reporting. J. Am. Med. Inform. Assoc. 2013, 20, e131–e138. [Google Scholar] [CrossRef]
- Eftekhari, S.; Yaraghi, N.; Gopal, R.D.; Ramesh, R. Impact of Health Information Exchange Adoption on Referral Patterns. Manag. Sci. 2023, 69, 1615–1638. [Google Scholar] [CrossRef]
- Yang, S.; Wang, H.; Lin, X. Dynamic decision of health information exchange under different hospital relationships: A differential game approach. J. Ind. Manag. Optim. 2023, 19, 6634–6663. [Google Scholar] [CrossRef]
- Kang, K.; Tan, B.Q. Carbon emission reduction investment in sustainable supply chains under cap-and-trade regulation: An evolutionary game-theoretical perspective. Expert Syst. Appl. 2023, 227, 120335. [Google Scholar] [CrossRef]
- Liu, P.; Deng, Q.; Jiang, C. Evolutionary game analysis on collaborative logistics diffusion considering diminishing marginal utility under dynamic productivity. Int. J. Syst. Sci. Oper. Logist. 2024, 11, 2339388. [Google Scholar] [CrossRef]
- Xia, P.; Liu, Z.; Qing, Q. An evolutionary game analysis of vehicle recall supervision considering the impact of public opinion. J. Oper. Res. Soc. 2022, 74, 1640–1653. [Google Scholar] [CrossRef]
- Wang, Y.; Chen, H.; Gu, X. A Two-Stage Evolutionary Game Model for Collaborative Emergency Management Between Local Governments and Enterprises. Int. J. Disaster Risk Sci. 2023, 14, 1029–1043. [Google Scholar] [CrossRef]
- Fan, W.; Wu, X.; He, Q. Digitalization drives green transformation of supply chains: A two-stage evolutionary game analysis. Ann. Oper. Res. 2024, 1–20. [Google Scholar] [CrossRef]
- Chen, Y.; Ding, S.; Zheng, H.; Zhang, Y.; Yang, S. Exploring diffusion strategies for mHealth promotion using evolutionary game model. Appl. Math. Comput. 2018, 336, 148–161. [Google Scholar] [CrossRef]
- Zhu, C.; Zhou, L.; Zhang, X.; Walsh, C.A. Tripartite Evolutionary Game and Simulation Analysis of Healthcare Fraud Supervision under the Government Reward and Punishment Mechanism. Healthcare 2023, 11, 1972. [Google Scholar] [CrossRef]
- Friedman, D. Evolutionary Games in Economics. Econometrica 1991, 59, 637–666. [Google Scholar] [CrossRef]
- Friedman, D. On economic applications of evolutionary game theory. J. Evol. Econ. 1998, 8, 15–43. [Google Scholar] [CrossRef]
- Zhou, C.; Lan, Y.; Zhao, R.; Zhang, G. Incentive schemes for readmissions reduction in coordinating reverse referral healthcare services. Comput. Ind. Eng. 2023, 176, 108938. [Google Scholar] [CrossRef]
- Thrasher, E.H.; Craighead, C.W.; Byrd, T.A. An empirical investigation of integration in healthcare alliance networks. Decis. Support Syst. 2010, 50, 116–127. [Google Scholar] [CrossRef]
- Demirezen, E.M.; Kumar, S.; Sen, A. Sustainability of Healthcare Information Exchanges: A Game-Theoretic Approach. Inf. Syst. Res. 2016, 27, 240–258. [Google Scholar] [CrossRef]
- Shabbar, R.; Sayama, H. Health information exchange network under collaboration, cooperation, and competition: A game-theoretic approach. Health Care Manag. Sci. 2023, 26, 516–532. [Google Scholar] [CrossRef]
- Choi, S.J.; Chen, M.; Tan, X. Assessing the impact of health information exchange on hospital data breach risk. Int. J. Med. Inform. 2023, 177, 105149. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).