
A Hybrid Model with Spherical Fuzzy-AHP, PLS-SEM and ANN to Predict Vaccination Intention against COVID-19



Abstract
:1. Introduction
- (a)
- What factors influence individuals’ immunization intentions against COVID-19 in the context of Vietnam?
- (b)
- Among the significant predictors, which factor has a greater association with individuals’ vaccination intention against COVID-19 in the context of Vietnam?
- (1)
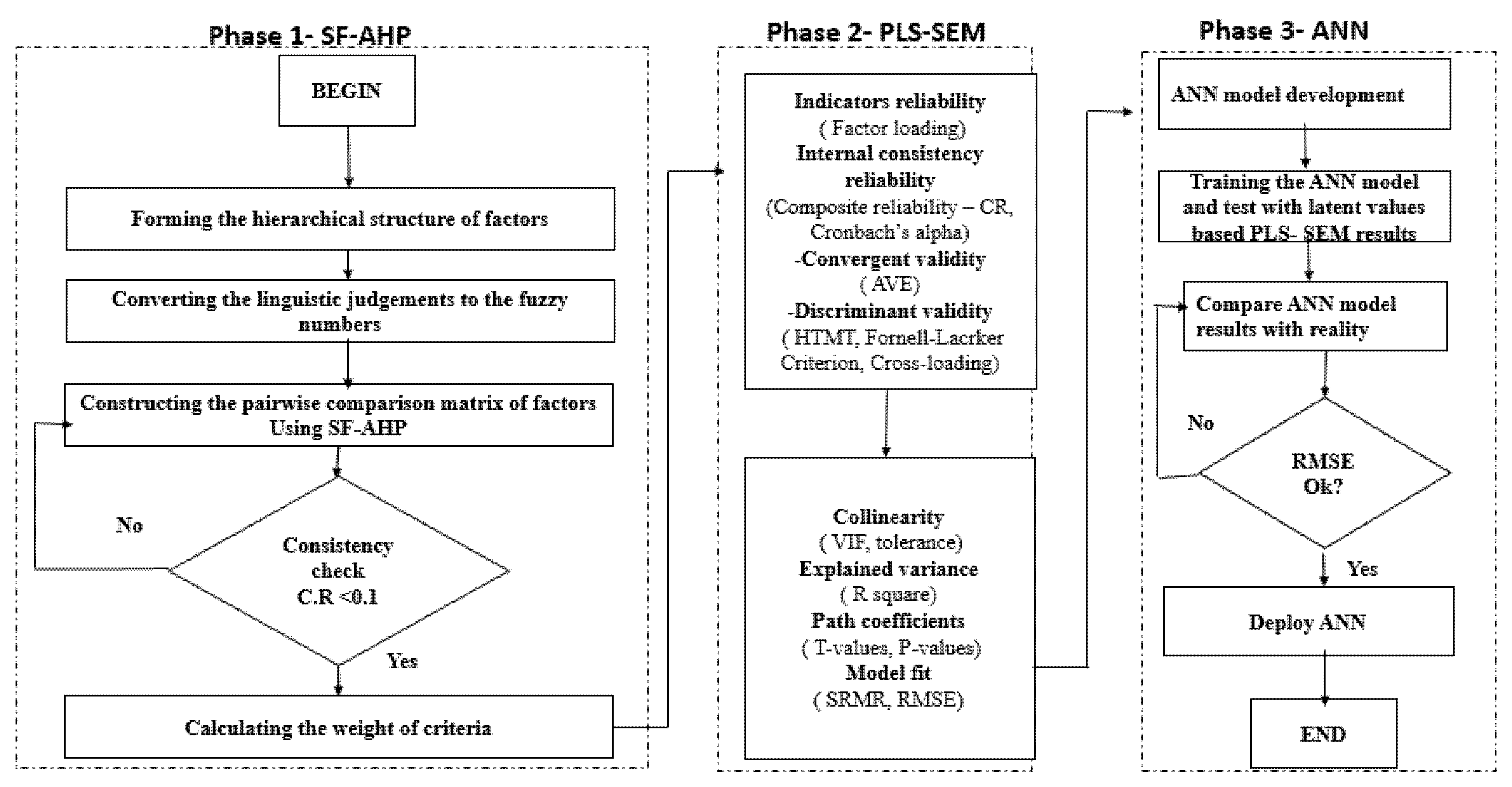
- This study is first to propose a hybrid three-staged model combining SF-AHP, PLS-SEM and ANN to analyze individuals’ behavioral intention to vaccinate.
- (2)
- The SF-AHP can identify the significant factors of individuals’ vaccination intention through relative weights based on experts’ opinion. PLS-SEM can deploy the results of SF-AHP to conduct the massive survey to collect larger sample.
- (3)
- The ANN model can detect both linear and nonlinear models and compensatory and non-compensatory models, and it can learn from deep learning training sessions. Because it employs a feed-forward-back-propagation (FFBP) algorithm, ANN is a subset of machine learning (ML). Thus, by combining the strengths of SF-AHP, PLS-SEM, and ANN, we can complement and leverage the strengths of both methods, advancing the expert systems and artificial intelligence methodologies.
- (4)
- The benefits of this research will accrue to individuals, ministries of health, and educational institutions through the provision of broad knowledge, as the results are expected to identify the factors influencing vaccination intention among Vietnamese. Understanding these factors would enable the government to optimize its intervention strategies and accelerate the massive vaccination campaigns against COVID-19.
2. Literature Review
2.1. Theoretical Foundation
2.2. Hypothesis Development
3. Research Methodology
3.1. Research Framework
3.2. Spherical Fuzzy Analytical Hierarchy Process (SF-AHP)
- (1)
- Union operation
- (2)
- Intersection operation
- (3)
- Addition operation
- (4)
- Multiplication operation
- (5)
- Multiplication by a scalar;
- (6)
- Power of
3.3. PLS-SEM Approach
3.3.1. Sampling and Collecting Data
3.3.2. Quantitative Analysis
- (1)
- Reliability test: The reliability analysis results are shown through two indexes: Cronbach’s Alpha coefficient is greater than 0.7, and Composite Reliability (CR) is greater than 0.7 [22,59]. At the same time, this study also evaluates the convergence value of the constructs through the factor loading coefficient greater than 0.5 and the Average Variance Extracted (AVE) greater than 0.5. Thus, when the constructs achieve convergence and reliability, the analytical results for the constructs by items will be reliable [22,59].
- (2)
- Discriminant validity: In addition to assessing the confidence value and the convergence value, the analysis requires the constructs to ensure distinctiveness from each other. Two commonly used evaluation methods are: AVE’s square root is greater than the corresponding correlation coefficient between the two constructs, and HTMT is less than 0.85 [22,59].
- (3)
3.4. ANN Algorithm
4. Analytical Results
4.1. A Case Study in Vietnam
4.2. SF-AHP Results
4.3. PLS-SEM Results
4.3.1. Sample Characteristics
4.3.2. Assessment of the Measurement Model
4.3.3. Multicollinearity
4.3.4. Hypothesis Testing Results
4.4. Results of ANN
4.5. Sensitivity Analysis
5. Discussions
6. Conclusions, Limitations and Future Works
6.1. Conclusions
6.2. Theoretical Implications
6.3. Practical Implications
6.4. Limitations and Future Research
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Danh sách khu vực phong tỏa và địa bàn ghi nhận ca bệnh COVID-19 trong cộng đồng từ ngày 27/4/2021 đến 17h30 ngày 12/10/2021, Centers for Disease Control and Prevention CDC COVID Data Tracker. 2021. Available online: https://vncdc.gov.vn/download-file.html?id=f16340536436165ae0bd1a1c (accessed on 1 August 2021).
- Chấn chỉnh việc thực hiện thu phí xét nghiệm COVID-19, Centers for Disease Control and Prevention CDC COVID Data Tracker. 2021. Available online: https://vncdc.gov.vn/chan-chinh-viec-thuc-hien-thu-phi-xet-nghiem-covid-19-nd16574.html (accessed on 1 August 2021).
- Pradhan, D.; Biswasroy, P.; Kumar Naik, P.; Ghosh, G.; Rath, G. A Review of Current Interventions for COVID-19 Prevention. Arch. Med. Res. 2020, 51, 363–374. [Google Scholar] [CrossRef] [PubMed]
- Pinto Neto, O.; Kennedy, D.M.; Reis, J.C.; Wang, Y.; Brizzi, A.C.B.; Zambrano, G.J.; de Souza, J.M.; Pedroso, W.; de Mello Pedreiro, R.C.; de Matos Brizzi, B.; et al. Mathematical model of COVID-19 intervention scenarios for São Paulo—Brazil. Nat. Commun. 2021, 12, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.; Lee, H.; Song, K.-H.; Kim, E.S.; Park, J.S.; Jung, J.; Ahn, S.; Jeong, E.K.; Park, H.; Kim, H. Bin Impact of Public Health Interventions on Seasonal Influenza Activity During the COVID-19 Outbreak in Korea. Clin. Infect. Dis. 2021, 73, e132–e140. [Google Scholar] [CrossRef] [PubMed]
- Doherty, F.V.; Odeyemi, O.A.; Adeola, A.; Amolegbe, O.; Ajagbe, F.E. Evaluation of knowledge, impacts and government intervention strategies during the COVID–19 pandemic in Nigeria. Data Br. 2020, 32, 106177. [Google Scholar] [CrossRef]
- Chu, D.K.W.; Gu, H.; Chang, L.D.J.; Cheuk, S.S.Y.; Gurung, S.; Krishnan, P.; Ng, D.Y.M.; Liu, G.Y.Z.; Wan, C.K.C.; Tsang, D.N.C.; et al. SARS-CoV-2 superspread in fitness center, Hong Kong, China, March 2021. Emerg. Infect. Dis. 2021, 27, 2230–2232. [Google Scholar] [CrossRef]
- Sheth, S.A.; Wu, T.C.; Sharrief, A.; Ankrom, C.; Grotta, J.C.; Fisher, M.; Savitz, S.I. Early Lessons from World War COVID Reinventing Our Stroke Systems of Care. Stroke 2020, 51, 2268–2272. [Google Scholar] [CrossRef]
- Bechtold, H.D.; Cruz, A.T.; Kaziny, B.D. From World War II to COVID-19: A Historical Perspective on the American Medical Supply Chain. Disaster Med. Public Health Prep. 2021, 1–2. [Google Scholar] [CrossRef]
- Bailey, Y.; Shankar, M.; Phillips, P. Casualties of the World War II metaphor: Women’s reproductive health fighting for narrative inclusion in COVID-19. Med. Humanit. 2021. Available online: https://mh.bmj.com/content/medhum/early/2021/06/21/medhum-2021-012152.full.pdf (accessed on 1 August 2021). [CrossRef]
- Hyland, P.; Vallières, F.; Shevlin, M.; Bentall, R.P.; McKay, R.; Hartman, T.K.; McBride, O.; Murphy, J. Resistance to COVID-19 vaccination has increased in Ireland and the United Kingdom during the pandemic. Public Health 2021, 195, 54–56. [Google Scholar] [CrossRef]
- Soares, P.; Rocha, J.V.; Moniz, M.; Gama, A.; Laires, P.A.; Pedro, A.R.; Dias, S.; Leite, A.; Nunes, C. Factors associated with COVID-19 vaccine hesitancy. Vaccines 2021, 9, 300. [Google Scholar] [CrossRef]
- Mahmood, T.; Ullah, K.; Khan, Q.; Jan, N. An approach toward decision-making and medical diagnosis problems using the concept of spherical fuzzy sets. Neural Comput. Appl. 2019, 31, 7041–7053. [Google Scholar] [CrossRef]
- Ilyas, M.; Ali, Z.; Gumaei, A. Spherical Fuzzy Sets-Based Cosine Similarity and Information Measures for Pattern Recognition and Medical Diagnosis. IEEE Access 2021, 9, 25835–25842. [Google Scholar] [CrossRef]
- Nassereddine, M.; Azar, A.; Rajabzadeh, A.; Afsar, A. Decision making application in collaborative emergency response: A new PROMETHEE preference function. Int. J. Disaster Risk Reduct. 2019, 38, 101221. [Google Scholar] [CrossRef]
- Kutlu Gündoğdu, F.; Kahraman, C. A novel spherical fuzzy analytic hierarchy process and its renewable energy application. Soft Comput. 2020, 24, 4607–4621. [Google Scholar] [CrossRef]
- Tsai, J.F.; Wang, C.P.; Chang, K.L.; Hu, Y.C. Selecting bloggers for hotels via an innovative mixed MCDM model. Mathematics 2021, 9, 1555. [Google Scholar] [CrossRef]
- Nguyen, P.H.; Tsai, J.F.; Kumar, V.A.G.; Hu, Y.C. Stock investment of agriculture companies in the Vietnam stock exchange market: An AHP integrated with GRA-TOPSIS-MOORA approaches. J. Asian Financ. Econ. Bus. 2020, 7, 113–121. [Google Scholar] [CrossRef]
- Nguyen, P.H. A Fuzzy Analytic Hierarchy Process (FAHP) Based on SERVQUAL for Hotel Service Quality Management: Evidence from Vietnam. J. Asian Financ. Econ. Bus. 2021, 8, 1101–1109. [Google Scholar] [CrossRef]
- Kahraman, C. Decision Making with Spherical Fuzzy Sets; Springer: Cham, Switzerland, 2021; Volume 392, ISBN 978-3-030-45460-9. Available online: https://www.semanticscholar.org/paper/Decision-Making-with-Spherical-Fuzzy-Sets-Kahraman-G%C3%BCndo%C4%9Fdu/8a9d9e5f310804cb809ce4f243c8c25554867580 (accessed on 1 October 2021).
- Yildiz, D.; Temur, G.T.; Beskese, A.; Bozbura, F.T. A spherical fuzzy analytic hierarchy process based approach to prioritize career management activities improving employee retention. J. Intell. Fuzzy Syst. 2020, 39, 6603–6618. [Google Scholar] [CrossRef]
- Hair, J.F.; Risher, J.J.; Sarstedt, M.; Ringle, C.M. When to use and how to report the results of PLS-SEM. Eur. Bus. Rev. 2019, 31, 2–24. [Google Scholar] [CrossRef]
- Hair, J.F.; Sarstedt, M.; Hopkins, L.; Kuppelwieser, V.G. Partial least squares structural equation modeling (PLS-SEM): An emerging tool in business research. Eur. Bus. Rev. 2014, 26, 106–121. [Google Scholar] [CrossRef]
- Nguyen, P.H.; Tsai, J.F.; Dang, T.T.; Lin, M.H.; Pham, H.A.; Nguyen, K.A. A hybrid spherical fuzzy MCDM approach to prioritize governmental intervention strategies against the COVID-19 pandemic: A case study from Vietnam. Mathematics 2021, 9, 2626. [Google Scholar] [CrossRef]
- Doornekamp, L.; Van Leeuwen, L.; Van Gorp, E.; Voeten, H. Determinants of Vaccination Uptake in Risk Populations: A Comprehensive Literature Review. Vaccines 2020, 8, 480. [Google Scholar] [CrossRef] [PubMed]
- Alyasseri, Z.A.A.; Al-Betar, M.A.; Doush, I.A.; Awadallah, M.A.; Abasi, A.K.; Makhadmeh, S.N.; Alomari, O.A.; Abdulkareem, K.H.; Adam, A.; Damasevicius, R.; et al. Review on COVID-19 diagnosis models based on machine learning and deep learning approaches. Expert Syst. 2021, e12759. [Google Scholar] [CrossRef] [PubMed]
- Sabzi, H.Z.; Abudu, S.; Alizadeh, R.; Soltanisehat, L.; Dilekli, N.; King, J.P. Environmental Effects Integration of time series forecasting in a dynamic decision support system for multiple reservoir management to conserve water sources. Energy Sources Part A Recover. Util. Environ. Eff. 2018, 40, 1398–1416. [Google Scholar] [CrossRef]
- Fei, Z.; Ryeznik, Y.; Sverdlov, A.; Tan, C.W.; Wong, W.K. An overview of healthcare data analytics with applications to the COVID-19 pandemic. IEEE Trans. Big Data 2021, 1. [Google Scholar] [CrossRef]
- Oyelade, O.N.; Ezugwu, A.E. A case-based reasoning framework for early detection and diagnosis of novel coronavirus. Inform. Med. Unlocked 2020, 20, 100395. [Google Scholar] [CrossRef]
- Kowalski, R.M.; Black, K.J. Protection Motivation and the COVID-19 Virus. Health Commun. 2021, 36, 15–22. [Google Scholar] [CrossRef]
- Prasetyo, Y.T.; Castillo, A.M.; Salonga, L.J.; Sia, J.A.; Seneta, J.A. Factors affecting perceived effectiveness of COVID-19 prevention measures among Filipinos during Enhanced Community Quarantine in Luzon, Philippines: Integrating Protection Motivation Theory and extended Theory of Planned Behavior. Int. J. Infect. Dis. 2020, 99, 312–323. [Google Scholar] [CrossRef]
- Mir, H.H.; Parveen, S.; Mullick, N.H.; Nabi, S. Using structural equation modeling to predict Indian people’s attitudes and intentions towards COVID-19 vaccination. Diabetes Metab. Syndr. Clin. Res. Rev. 2021, 15, 1017–1022. [Google Scholar] [CrossRef]
- Shmueli, L. Predicting intention to receive COVID-19 vaccine among the general population using the health belief model and the theory of planned behavior model. BMC Public Health 2021, 21, 804. [Google Scholar] [CrossRef]
- Khaled, S.M.; Petcu, C.; Bader, L.; Amro, I.; Al-Hamadi, A.M.H.A.; Al Assi, M.; Ali, A.A.M.; Le Trung, K.; Diop, A.; Bellaj, T.; et al. Prevalence and potential determinants of COVID-19 vaccine hesitancy and resistance in qatar: Results from a nationally representative survey of qatari nationals and migrants between december 2020 and january 2021. Vaccines 2021, 9, 471. [Google Scholar] [CrossRef]
- Lin, Y.; Hu, Z.; Zhao, Q.; Alias, H.; Danaee, M.; Wong, L.P. Understanding COVID-19 vaccine demand and hesitancy: A nationwide online survey in China. PLoS Negl. Trop. Dis. 2020, 14, e0008961. [Google Scholar] [CrossRef]
- Li, L.; Wang, J.; Nicholas, S.; Maitland, E.; Leng, A.; Liu, R. The intention to receive the COVID-19 vaccine in China: Insights from protection motivation theory. Vaccines 2021, 9, 445. [Google Scholar] [CrossRef]
- Reiter, P.L.; Pennell, M.L.; Katz, M.L. Acceptability of a COVID-19 vaccine among adults in the United States: How many people would get vaccinated? Vaccine 2020, 38, 6500–6507. [Google Scholar] [CrossRef]
- Kaadan, M.I.; Abdulkarim, J.; Chaar, M.; Zayegh, O.; Keblawi, M.A. Determinants of COVID-19 vaccine acceptance in the Arab world: A cross-sectional study. Glob. Health Res. Policy 2021, 6, 23. [Google Scholar] [CrossRef]
- WHO; Kementerian Kesehatan Republik Indonesia. COVID-19 Vaccine Acceptance Survey in Indonesia. Available online: https://covid19.go.id/storage/app/media/Hasil%20Kajian/2020/November/vaccine-acceptance-survey-en-12-11-2020final.pdf (accessed on 1 October 2021).
- Chen, H.; Paris, C.; Reeson, A.; Xu, W.; Li, X. Social distance and SARS memory: Impact on the public awareness of 2019 novel coronavirus (COVID-19) outbreak. Sci. Rep. 2020, 10. [Google Scholar] [CrossRef]
- Lazarus, J.V.; Ratzan, S.C.; Palayew, A.; Gostin, L.O.; Larson, H.J.; Rabin, K.; Kimball, S.; El-Mohandes, A. A global survey of potential acceptance of a COVID-19 vaccine. Nat. Med. 2021, 27, 225–228. [Google Scholar] [CrossRef]
- WHO. Report of SAGE Working Group Vaccine Hesitancy. World Health Organ. 2015. Available online: https://www.who.int/immunization/sage/meetings/2014/october/1_Report_WORKING_GROUP_vaccine_hesitancy_final.pdf (accessed on 1 August 2021).
- Lovari, A. Spreading (Dis)trust: COVID-19 misinformation and government intervention in Italy. Media Commun. 2020, 8, 458–461. [Google Scholar] [CrossRef]
- Mitchell, V. Consumer perceived risk: Conceptualisations and models. Eur. J. Mark. 1999, 33, 163–195. [Google Scholar] [CrossRef]
- Rogers, R.W.; Maddux, J.E. Protection Motivation and Self Efficacy: A Revised Theory of Fear Appeals and Attittude Change. J. Exp. Soc. Psychol. 1983, 19, 469–479. [Google Scholar]
- Ling, M.; Kothe, E.J.; Mullan, B.A. Predicting intention to receive a seasonal influenza vaccination using Protection Motivation Theory. Soc. Sci. Med. 2019, 233, 87–92. [Google Scholar] [CrossRef] [Green Version]
- Camerini, A.L.; Diviani, N.; Fadda, M.; Schulz, P.J. Using protection motivation theory to predict intention to adhere to official MMR vaccination recommendations in Switzerland. SSM Popul. Health 2019, 7, 100321. [Google Scholar] [CrossRef]
- Trent, M.; Seale, H.; Chughtai, A.A.; Salmon, D.; MacIntyre, C.R. Trust in government, intention to vaccinate and COVID-19 vaccine hesitancy: A comparative survey of five large cities in the United States, United Kingdom, and Australia. Vaccine 2021, in press. [Google Scholar] [CrossRef]
- Vergara, R.J.D.; Sarmiento, P.J.D.; Lagman, J.D.N. Building public trust: A response to COVID-19 vaccine hesitancy predicament. J. Public Health 2021, 43, e291–e292. [Google Scholar] [CrossRef]
- Nguyen, H.; Nguyen, A. Covid-19 misinformation and the social (Media) amplification of risk: A Vietnamese perspective. Media Commun. 2020, 8, 444–447. [Google Scholar] [CrossRef]
- Aloweidi, A.; Bsisu, I.; Suleiman, A.; Abu-Halaweh, S.; Almustafa, M.; Aqel, M.; Amro, A.; Radwan, N.; Assaf, D.; Abdullah, M.Z.; et al. Hesitancy towards covid-19 vaccines: An analytical cross–sectional study. Int. J. Environ. Res. Public Health 2021, 18, 5111. [Google Scholar] [CrossRef]
- Tran, H.T.T.; Lu, S.H.; Tran, H.T.T.; van Nguyen, B. Social media insights during the COVID-19 pandemic: Infodemiology study using big data. JMIR Med. Inform. 2021, 9, e27116. [Google Scholar] [CrossRef] [PubMed]
- Sassenberg, K.; Matschke, C.; Scholl, A. The impact of discrepancies from ingroup norms on group members’ well-being and motivation. Eur. J. Soc. Psychol. 2011, 41, 886–897. [Google Scholar] [CrossRef]
- Longchamps, C.; Ducarroz, S.; Crouzet, L.; Vignier, N.; Pourtau, L.; Allaire, C.; Colleville, A.C.; El Aarbaoui, T.; Melchior, M. COVID-19 vaccine hesitancy among persons living in homeless shelters in France. Vaccine 2021, 39, 3315–3318. [Google Scholar] [CrossRef]
- Icek, A. Organizational Behavior And Human Decision Processes “The Theory of Planned Behavior”. Tagl. Prax. 2012, 53, 51–58. [Google Scholar]
- Raza, A.; Ali, Q.; Hussain, T. Role of knowledge, behavior, norms, and e-guidelines in controlling the spread of COVID-19: Evidence from Pakistan. Environ. Sci. Pollut. Res. 2020, 28, 40329–40345. [Google Scholar] [CrossRef] [PubMed]
- Avkiran, N.K.; Ringle, C.M. Partial Least Squares Structural Equation Modeling: Recent Advances in Banking and Finance: International Series in Operations Research & Management Science; Springer: Cham, Switzerland, 2018; ISBN 978-3-319-71690-9. [Google Scholar]
- Binsawad, M.H. Corporate Social Responsibility in Higher Education: A PLS-SEM Neural Network Approach. IEEE Access 2020, 8, 29125–29131. [Google Scholar] [CrossRef]
- Hair, J.; Black, W.; Babin, B.; Anderson, R. Multivariate Data Analysis: Pearson New International Edition, 7th ed.; Pearson Education Limited Harlow: Essex, UK, 2014; ISBN 0007070971018. [Google Scholar]
- Alkawsi, G.A.; Ali, N.; Mustafa, A.S.; Baashar, Y.; Alhussian, H.; Alkahtani, A.; Tiong, S.K.; Ekanayake, J. A hybrid SEM-neural network method for identifying acceptance factors of the smart meters in Malaysia: Challenges perspective. Alex. Eng. J. 2021, 60, 227–240. [Google Scholar] [CrossRef]
- Leong, L.Y.; Hew, T.S.; Ooi, K.B.; Tan, G.W.H. Predicting actual spending in online group buying – An artificial neural network approach. Electron. Commer. Res. Appl. 2019, 38, 100898. [Google Scholar] [CrossRef]
- Leong, L.Y.; Hew, T.S.; Ooi, K.B.; Dwivedi, Y.K. Predicting trust in online advertising with an SEM-artificial neural network approach. Expert Syst. Appl. 2020, 162, 113849. [Google Scholar] [CrossRef]
- Foo, P.Y.; Lee, V.H.; Tan, G.W.H.; Ooi, K.B. A gateway to realising sustainability performance via green supply chain management practices: A PLS–ANN approach. Expert Syst. Appl. 2018, 107, 1–14. [Google Scholar] [CrossRef]
- Alharbi, A.; Sohaib, O. Technology Readiness and Cryptocurrency Adoption: PLS-SEM and Deep Learning Neural Network Analysis. IEEE Access 2021, 9, 21388–21394. [Google Scholar] [CrossRef]
- Sonawane, K.; Troisi, C.L.; Deshmukh, A.A. COVID-19 vaccination in the UK: Addressing vaccine hesitancy. Lancet Reg. Health Eur. 2021, 1, 100016. [Google Scholar] [CrossRef]
- Yaqub, O.; Castle-Clarke, S.; Sevdalis, N.; Chataway, J. Attitudes to vaccination: A critical review. Soc. Sci. Med. 2014, 112, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Ajzen, I.; Ajzen, I. Theory of Planned Behaviour Questionnaire. Meas. Instrum. Database Soc. Sci. 2013, 2–9. [Google Scholar]
- Maqbool, A.; Khan, N.Z. Analyzing barriers for implementation of public health and social measures to prevent the transmission of COVID-19 disease using DEMATEL method. Diabetes Metab. Syndr. Clin. Res. Rev. 2020, 14, 887–892. [Google Scholar] [CrossRef]
- Liu, P.L. COVID-19 information on social media and preventive behaviors: Managing the pandemic through personal responsibility. Soc. Sci. Med. 2021, 277, 113928. [Google Scholar] [CrossRef]
- Luo, T.; Chen, W.; Liao, Y. Social media use in China before and during COVID-19: Preliminary results from an online retrospective survey. J. Psychiatr. Res. 2021, 140, 35–38. [Google Scholar] [CrossRef]
- Puri, N.; Coomes, E.A.; Haghbayan, H.; Gunaratne, K. Social media and vaccine hesitancy: New updates for the era of COVID-19 and globalized infectious diseases. Hum. Vaccines Immunother. 2020, 16, 2586–2593. [Google Scholar] [CrossRef]
- Wang, P.W.; Ahorsu, D.K.; Lin, C.Y.; Chen, I.H.; Yen, C.F.; Kuo, Y.J.; Griffiths, M.D.; Pakpour, A.H. Motivation to have covid-19 vaccination explained using an extended protection motivation theory among university students in china: The role of information sources. Vaccines 2021, 9, 380. [Google Scholar] [CrossRef]
- Schwarzinger, M.; Watson, V.; Arwidson, P.; Alla, F.; Luchini, S. COVID-19 vaccine hesitancy in a representative working-age population in France: A survey experiment based on vaccine characteristics. Lancet Public Health 2021, 6, e210–e221. [Google Scholar] [CrossRef]
- Paul, E.; Steptoe, A.; Fancourt, D. Attitudes towards vaccines and intention to vaccinate against COVID-19: Implications for public health communications. Lancet Reg. Health Eur. 2021, 1, 100012. [Google Scholar] [CrossRef]
- Fornell, C.; Larcker, D.F. Structural Equation Models with Unobservable Variables and Measurement Error: Algebra and Statistics. J. Mark. Res. 1981, 18, 382–388. [Google Scholar] [CrossRef]
- Henseler, J.; Ringle, C.M.; Sarstedt, M. A new criterion for assessing discriminant validity in variance-based structural equation modeling. J. Acad. Mark. Sci. 2015, 43, 115–135. [Google Scholar] [CrossRef] [Green Version]
- O’Brien, R.M. A caution regarding rules of thumb for variance inflation factors. Qual. Quant. 2007, 41, 673–690. [Google Scholar] [CrossRef]
- Nguyen, P.H.; Tsai, J.F.; Kayral, I.E.; Lin, M.H. Unemployment rates forecasting with grey-based models in the post-COVID-19 period: A case study from vietnam. Sustainability 2021, 13, 7879. [Google Scholar] [CrossRef]
- Lau, A.J.; Tan, G.W.-H.; Loh, X.-M.; Leong, L.-Y.; Lee, V.-H.; Ooi, K.-B. On the way: Hailing a taxi with a smartphone? A hybrid SEM-neural network approach. Mach. Learn. Appl. 2021, 4, 100034. [Google Scholar] [CrossRef]
- Sohaib, O.; Hussain, W.; Asif, M.; Ahmad, M.; Mazzara, M. A PLS-SEM Neural Network Approach for Understanding Cryptocurrency Adoption. IEEE Access 2019, 8, 13138–13150. [Google Scholar] [CrossRef]
- Kwok, K.O.; Li, K.K.; WEI, W.I.; Tang, A.; Wong, S.Y.S.; Lee, S.S. Influenza vaccine uptake, COVID-19 vaccination intention and vaccine hesitancy among nurses: A survey. Int. J. Nurs. Stud. 2021, 114, 103854. [Google Scholar] [CrossRef]
- Dzieciolowska, S.; Hamel, D.; Gadio, S.; Dionne, M.; Gagnon, D.; Robitaille, L.; Cook, E.; Caron, I.; Talib, A.; Parkes, L.; et al. Covid-19 vaccine acceptance, hesitancy, and refusal among Canadian healthcare workers: A multicenter survey. Am. J. Infect. Control 2021, 49, 1152–1157. [Google Scholar] [CrossRef]
- Xiao, Q.; Liu, X.; Wang, R.; Mao, Y.; Chen, H.; Li, X.; Liu, X.; Dai, J.; Gao, J.; Fu, H.; et al. Predictors of willingness to receive the COVID-19 vaccine after emergency use authorization: The role of coping appraisal. Vaccines 2021, 9, 967. [Google Scholar] [CrossRef]
- Cordina, M.; Lauri, M.A.; Lauri, J. Attitudes towards covid-19 vaccination, vaccine hesitancy and intention to take the vaccine. Pharm. Pract. (Granada) 2021, 19. [Google Scholar] [CrossRef]
- Rimal, R.N.; Storey, J.D. Construction of Meaning during a Pandemic: The Forgotten Role of Social Norms. Health Commun. 2020, 35, 1732–1734. [Google Scholar] [CrossRef]
- Wong, M.C.S.; Wong, E.L.Y.; Huang, J.; Cheung, A.W.L.; Law, K.; Chong, M.K.C.; Ng, R.W.Y.; Lai, C.K.C.; Boon, S.S.; Lau, J.T.F.; et al. Acceptance of the COVID-19 vaccine based on the health belief model: A population-based survey in Hong Kong. Vaccine 2021, 39, 1148–1156. [Google Scholar] [CrossRef]
- Aydoğdu, A.; Gül, S. A novel entropy proposition for spherical fuzzy sets and its application in multiple attribute decision-making. Int. J. Intell. Syst. 2020, 35, 1354–1374. [Google Scholar] [CrossRef]
- Khan, Q.; Mahmood, T.; Hassan, N. T-Spherical Fuzzy Power Muirhead Mean Operator Based on Novel Operational Laws and Their Application in Multi-Attribute Group Decision Making. IEEE Access 2019, 7, 22613–22632. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Scales | Score Index (SI) | |
|---|---|---|
| Absolutely more Importance (AMI) | (0.9, 0.1, 0.0) | 9 |
| Very High Importance (VHI) | (0.8, 0.2, 0.1) | 7 |
| High Importance (HI) | (0.7, 0.3, 0.2) | 5 |
| Slightly More Importance (SMI) | (0.6, 0.4, 0.3) | 3 |
| Equally Importance (EI) | (0.5, 0.4, 0.4) | 1 |
| Slightly Low Importance (SLI) | (0.4, 0.6, 0.3) | 1/3 |
| Low Importance (LI) | (0.3, 0.7, 0.2) | 1/5 |
| Very Low Importance (VLI) | (0.2, 0.8, 0.1) | 1/7 |
| Absolutely Low Importance (ALI) | (0.1, 0.9, 0.0) | 1/9 |
| Factors | Left Factor Is More Important | Right Factor Is More Important | Factors | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| AMI | VHI | HI | SMI | EI | SLI | LI | VLI | ALI | ||
| PCV | 1 | 5 | 7 | 1 | 1 | TRS | ||||
| PCV | 2 | 2 | 2 | 6 | 3 | SOM | ||||
| PCV | 2 | 4 | 3 | 4 | 1 | 1 | PSC | |||
| PCV | 3 | 5 | 4 | 2 | 1 | SOI | ||||
| TRS | 3 | 5 | 3 | 4 | SOM | |||||
| TRS | 1 | 3 | 4 | 6 | 1 | PSC | ||||
| TRS | 1 | 2 | 2 | 5 | 4 | 1 | SOI | |||
| SOM | 1 | 2 | 3 | 6 | 3 | PSC | ||||
| SOM | 1 | 3 | 3 | 4 | 4 | SOI | ||||
| PSC | 1 | 1 | 4 | 2 | 5 | 2 | SOI | |||
| Factors | PCV | TRS | SOM | PSC | SOI |
|---|---|---|---|---|---|
| PCV | 1.000 | 3.021 | 3.342 | 3.871 | 5.279 |
| TRS | 0.331 | 1.000 | 1.485 | 1.957 | 2.493 |
| SOM | 0.299 | 0.674 | 1.000 | 1.411 | 1.460 |
| PSC | 0.258 | 0.511 | 0.709 | 1.000 | 2.025 |
| SOI | 0.189 | 0.401 | 0.685 | 0.494 | 1.000 |
| SUM | 2.0780 | 5.6069 | 7.2199 | 8.7327 | 12.2566 |
| Factors | PCV | TRS | SOM | PSC | SOI | MEAN | WSV | CV |
|---|---|---|---|---|---|---|---|---|
| PCV | 0.481 | 0.539 | 0.463 | 0.443 | 0.431 | 0.4714 | 2.3918 | 5.0740 |
| TRS | 0.159 | 0.178 | 0.206 | 0.224 | 0.203 | 0.1941 | 0.9826 | 5.0610 |
| SOM | 0.144 | 0.120 | 0.139 | 0.162 | 0.119 | 0.1367 | 0.6915 | 5.0596 |
| PSC | 0.124 | 0.091 | 0.098 | 0.115 | 0.165 | 0.1187 | 0.5967 | 5.0289 |
| SOI | 0.091 | 0.072 | 0.095 | 0.057 | 0.082 | 0.0791 | 0.3985 | 5.0356 |
| Factors | PCV | TRS | SOM | PSC | SOI |
|---|---|---|---|---|---|
| PCV | (0.500, 0.400, 0.400) | (0.619, 0.381, 0.275) | (0.648, 0.341, 0.283) | (0.678, 0.335, 0.238) | (0.737, 0.270, 0.201) |
| TRS | (0.357, 0.642, 0.261) | (0.500, 0.400, 0.400) | (0.535, 0.454, 0.310) | (0.571, 0.393, 0.326) | (0.606, 0.377, 0.301) |
| SOM | (0.292, 0.704, 0.242) | (0.421, 0.567, 0.303) | (0.500, 0.400, 0.400) | (0.535, 0.434, 0.330) | (0.539, 0.446, 0.311) |
| PSC | (0.268, 0.735, 0.196) | (0.370, 0.601, 0.309) | (0.399, 0.572, 0.317) | (0.500, 0.400, 0.400) | (0.584, 0.395, 0.307) |
| SOI | (0.223, 0.778, 0.160) | (0.329, 0.661, 0.268) | (0.402, 0.583, 0.296) | (0.340, 0.645, 0.275) | (0.500, 0.400, 0.400) |
| SF-AHP Weights | Calculations to Obtain Crisp Weights | Crisp Weights | |
|---|---|---|---|
| PCV | (0.647, 0.342, 0.280) | 17.988 | 0.273 |
| TRS | (0.525, 0.444, 0.326) | 14.089 | 0.214 |
| SOM | (0.471, 0.499, 0.327) | 12.465 | 0.189 |
| PSC | (0.444, 0.525, 0.320) | 11.716 | 0.178 |
| SOI | (0.374, 0.599, 0.300) | 9.713 | 0.147 |
| n | % | n | % | ||
|---|---|---|---|---|---|
| Gender | Status | ||||
| Female | 210 | 44.4 | Other | 310 | 65.3 |
| Male | 264 | 55.6 | Married | 164 | 34.7 |
| Age | Income | ||||
| Under 35 | 327 | 68.8 | <10 mil | 81 | 17.3 |
| 35 to 45 | 116 | 24.6 | From 10 mil to 15 | 211 | 44.4 |
| 46 to 65 | 31 | 6.5 | From 15 mil to 20 mil | 69 | 14.5 |
| >20 mil | 113 | 23.8 | |||
| Job | |||||
| Private office staff | 201 | 42.5 | Possibility of infection | ||
| Public Officials | 48 | 10.1 | 0–20% | 152 | 32.2 |
| Self-employed | 94 | 19.8 | 20–40% | 166 | 34.9 |
| Industrial workers | 16 | 3.4 | 40–60% | 94 | 19.8 |
| Other | 115 | 24.2 | 60–100% | 62 | 13.1 |
| Education | Whose relatives die | ||||
| High school and below | 30 | 6.5 | No | 380 | 80.2 |
| University graduate | 333 | 70.1 | Yes | 94 | 19.8 |
| Master | 61 | 12.8 | |||
| Doctor | 50 | 10.5 |
| Scales’ Items/Sources | Loading | Cronbach’s Alpha |
|---|---|---|
| Perceived Severity of COVID-19 (PSC) adapted from [37,41,47,65]; | CR = 0.890, AVE = 0.599 | |
| PSC 1_ The COVID-19 pandemic has a high mortality rate. | 0.801 | 0.867 |
| PSC 2_ Worrying about yourself, relatives, and colleagues who may be infected with COVID-19. | 0.824 | |
| PSC 3_ Recognizing the possibility of a COVID-19 pandemic breaking out in the area where you live and work. | 0.747 | |
| PSC 4_ Risk Perception of infection during concentrated isolation. | 0.775 | |
| PSC 5_ Risk Perception of infection during self-isolation | 0.728 | |
| PSC 6_ Risk perception of distance guidance during self-isolation. | 0.766 | |
| Perceived COVID-19 Vaccines (PVC) adapted from [37,65,66]; | CR = 0.952, AVE = 0.772 | |
| PVC 1_ Perceive that getting vaccinated against COVID-19 reduces the risk of the disease. | 0.849 | 0.941 |
| PVC2_ Perceive that getting vaccinated against COVID-19 reduces the severity of the disease. | 0.831 | |
| PVC 3_ Perceive that vaccination against COVID-19 is required to prevent disease outbreaks. | 0.884 | |
| PVC 4_ Perceive that vaccination against COVID-19 is good for the community. | 0.913 | |
| PVC5_ Perceive that vaccination against COVID-19 helps economic and social activities return to normal soon. | 0.929 | |
| PVC6_ Research on a COVID-19 vaccine is needed in the context of many new variants. | 0.862 | |
| Social Influence (SOI) adapted from [56,67,68]; | CR = 0.922, AVE = 0.799 | |
| SOI1_ impact of family members on your decision to get the COVID-19 vaccine. | 0.936 | 0.876 |
| SOI2_ Impact of friends and colleagues on your decision to get the COVID-19 vaccine. | 0.928 | |
| SOI3_ In general, you are easily influenced by people around you about getting the COVID-19 vaccine. | 0.811 | |
| Social Media (SOM) adapted from [69,70,71]; | CR = 0.903, AVE = 0.756 | |
| SOM1_ Regularly find out information about the COVID-19 vaccine on social networks. | 0.867 | 0.840 |
| SOM2_ Refer to the information shared from people who have received the COVID-19 vaccine on social networks. | 0.867 | |
| SOM3_ Social networks bring much helpful information to you about the COVID-19 vaccine. | 0.875 | |
| Trust in government intervention strategies (TRS) adapted from [65,72,73,74]; | CR = 0.926, AVE = 0.676 | |
| TRS1_ Trust in the government’s ability to prevent COVID-19. | 0.820 | 0.903 |
| TRS2_ Trust the vaccine being used by the Vietnamese government. | 0.877 | |
| TRS3_ Trust in the COVID-19 vaccine storage procedures. | 0.846 | |
| TRS4_ Trust in the medical team during the COVID-19 vaccination process. | 0.823 | |
| TRS5_ Trust in the ability to manage side effects after a COVID-19 vaccine. | 0.808 | |
| TRS6_ Trust that vaccines are the most effective method of disease prevention and control COVID-19. | 0.753 | |
| Behavioral intention to get vaccination (INT) adapted from [31,71,72]; | CR = 0.890, AVE = 0.733 | |
| INT1_ Registered for the COVID-19 vaccine. | 0.697 | 0.817 |
| INT2_ Expect to get a COVID-19 vaccine at any time. | 0.936 | |
| INT3_ Ready to encourage loved ones to get vaccinated against COVID-19. | 0.915 | |
| INT | PSC | PCV | SOI | SOM | TRS | |
|---|---|---|---|---|---|---|
| INT | 0.856 | |||||
| PSC | 0.539 | 0.774 | ||||
| (0.612) | ||||||
| PCV | 0.723 | 0.688 | 0.879 | |||
| (0.802) | (0.750) | |||||
| SOI | 0.423 | 0.501 | 0.469 | 0.894 | ||
| (0.480) | (0.579) | (0.503) | ||||
| SOM | 0.533 | 0.637 | 0.650 | 0.594 | 0.870 | |
| (0.615) | (0.752) | (0.719) | (0.681) | |||
| TRS | 0.621 | 0.598 | 0.658 | 0.396 | 0.527 | 0.822 |
| (0.689) | (0.659) | (0.709) | (0.431) | (0.590) |
| PVC | TRS | INT | VIF | ||
|---|---|---|---|---|---|
| H1, H2 | PSC | 0.688 a | −0.030 | 1; 2.316 | |
| (0.000) | (0.552) | ||||
| H3 | PVC | 0.523 a | 2.575 | ||
| (0.000) | |||||
| H4 | TRS | 0.244 a | 1.915 | ||
| (0.000) | |||||
| H5, H6 | SOM | 0.527 a | 0.042 | 1; 2.288 | |
| (0.000) | (0.467) | ||||
| H7 | SOI | 0.072 | 1.613 | ||
| (0.173) | |||||
| R Square | 0.474 | 0.278 | 0.566 |
| Training | Testing | ||||
|---|---|---|---|---|---|
| N | SSE | RMSE | N | SSE | RMSE |
| 437 | 4.946 | 0.106 | 37 | 0.302 | 0.090 |
| 431 | 4.273 | 0.100 | 43 | 0.296 | 0.083 |
| 417 | 3.272 | 0.089 | 57 | 0.473 | 0.091 |
| 436 | 4.661 | 0.103 | 38 | 0.474 | 0.112 |
| 427 | 3.592 | 0.092 | 47 | 0.357 | 0.087 |
| 437 | 4.467 | 0.101 | 37 | 0.300 | 0.090 |
| 432 | 5.020 | 0.108 | 42 | 0.348 | 0.091 |
| 425 | 3.722 | 0.094 | 49 | 0.352 | 0.085 |
| 431 | 3.800 | 0.094 | 43 | 0.299 | 0.083 |
| 417 | 3.927 | 0.097 | 57 | 0.338 | 0.077 |
| Mean | 4.168 | 0.098 | Mean | 0.354 | 0.089 |
| S.D | 0.596 | 0.006 | S.D | 0.067 | 0.009 |
| ANN | PVC | PSC | SOI | SOM | TRS |
|---|---|---|---|---|---|
| ANN (1) | 0.048 | 0.059 | 0.064 | 0.141 | 0.328 |
| ANN (2) | 0.559 | 0.072 | 0.108 | 0.023 | 0.238 |
| ANN (3) | 0.560 | 0.044 | 0.136 | 0.065 | 0.194 |
| ANN (4) | 0.424 | 0.058 | 0.032 | 0.054 | 0.433 |
| ANN (5) | 0.534 | 0.060 | 0.127 | 0.024 | 0.256 |
| ANN (6) | 0.500 | 0.080 | 0.034 | 0.027 | 0.359 |
| ANN (7) | 0.218 | 0.218 | 0.217 | 0.164 | 0.256 |
| ANN (8) | 0.562 | 0.040 | 0.115 | 0.019 | 0.264 |
| ANN (9) | 0.565 | 0.600 | 0.100 | 0.041 | 0.234 |
| ANN (10) | 0.516 | 0.112 | 0.117 | 0.033 | 0.223 |
| Average Importance | 0.449 | 0.134 | 0.105 | 0.059 | 0.279 |
| Normalized Importance (%) | 43.74 | 13.10 | 10.24 | 5.76 | 27.16 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nguyen, P.-H.; Tsai, J.-F.; Lin, M.-H.; Hu, Y.-C. A Hybrid Model with Spherical Fuzzy-AHP, PLS-SEM and ANN to Predict Vaccination Intention against COVID-19. Mathematics 2021, 9, 3075. https://doi.org/10.3390/math9233075
Nguyen P-H, Tsai J-F, Lin M-H, Hu Y-C. A Hybrid Model with Spherical Fuzzy-AHP, PLS-SEM and ANN to Predict Vaccination Intention against COVID-19. Mathematics. 2021; 9(23):3075. https://doi.org/10.3390/math9233075
Chicago/Turabian StyleNguyen, Phi-Hung, Jung-Fa Tsai, Ming-Hua Lin, and Yi-Chung Hu. 2021. "A Hybrid Model with Spherical Fuzzy-AHP, PLS-SEM and ANN to Predict Vaccination Intention against COVID-19" Mathematics 9, no. 23: 3075. https://doi.org/10.3390/math9233075
APA StyleNguyen, P.-H., Tsai, J.-F., Lin, M.-H., & Hu, Y.-C. (2021). A Hybrid Model with Spherical Fuzzy-AHP, PLS-SEM and ANN to Predict Vaccination Intention against COVID-19. Mathematics, 9(23), 3075. https://doi.org/10.3390/math9233075