
Five Qualitative Research Concepts Grounded in Anthropological Methods for Teaching Design in Healthcare



{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
1.1. The Social Turn in Design Education for Healthcare
1.2. Designing for Healthcare, a Qualitative Research Endeavor
1.3. Anthropological Methods as a Framework for Qualitative Assessment
2. Materials and Methods
2.1. A Design-Based Research Approach
2.2. An Engineering-Design Program as Context for This Research
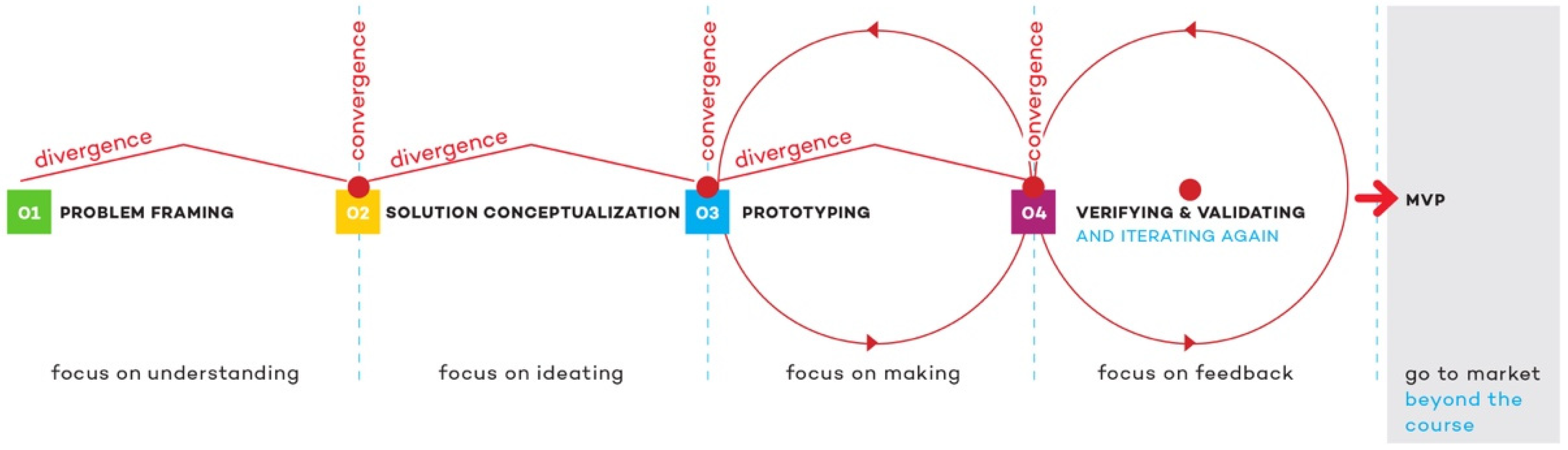
2.3. Teaching an Interactive Qualitative Research Process
2.4. Instructing Applied Qualitative Research Grounded in Anthropological Theory
2.5. Instructing Five Basic Qualitative Research Concepts
2.5.1. Informed Consent
2.5.2. Fieldnotes
2.5.3. Observation
2.5.4. Open-Ended Interviews
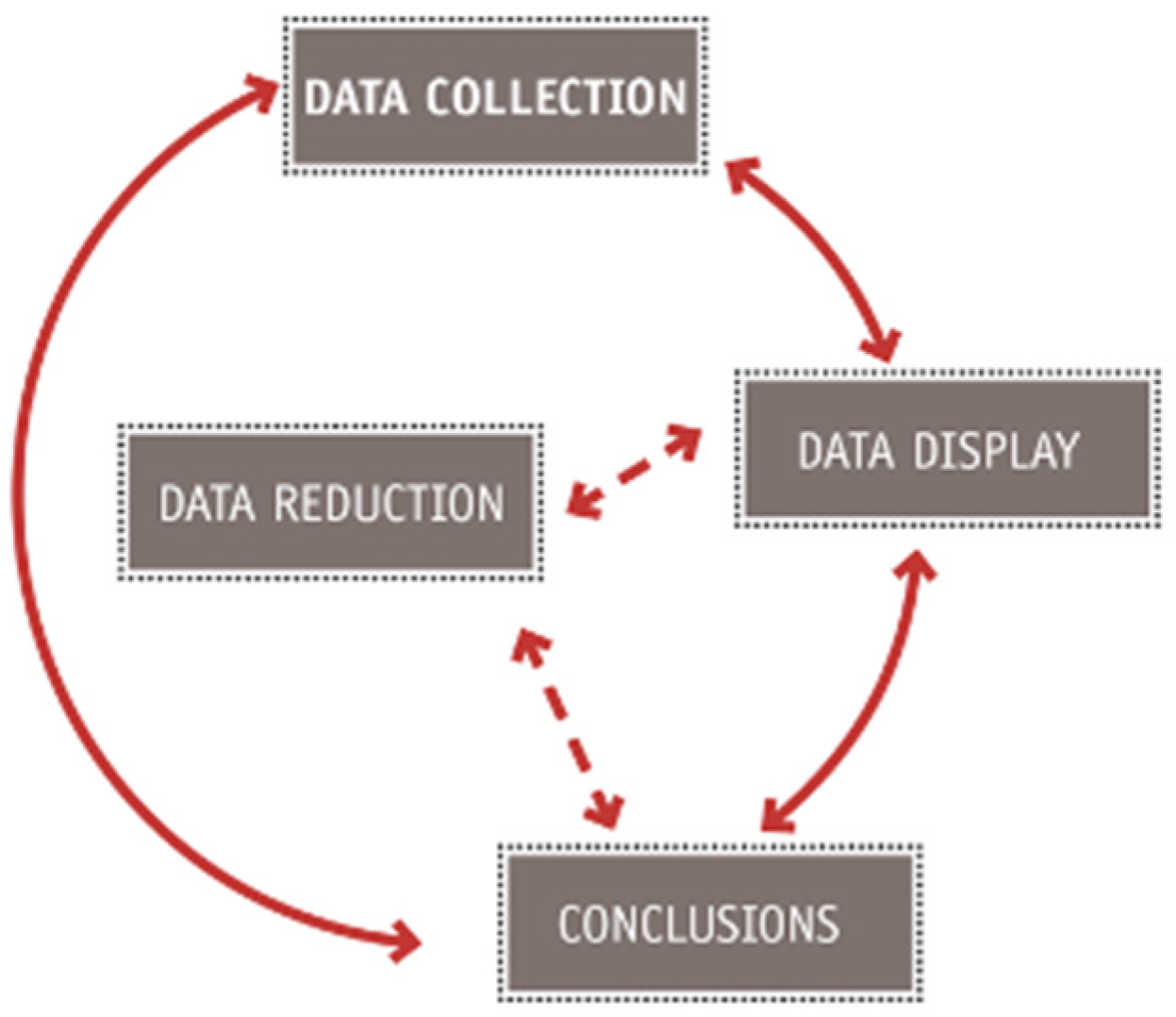
2.5.5. Qualitative Data Analysis
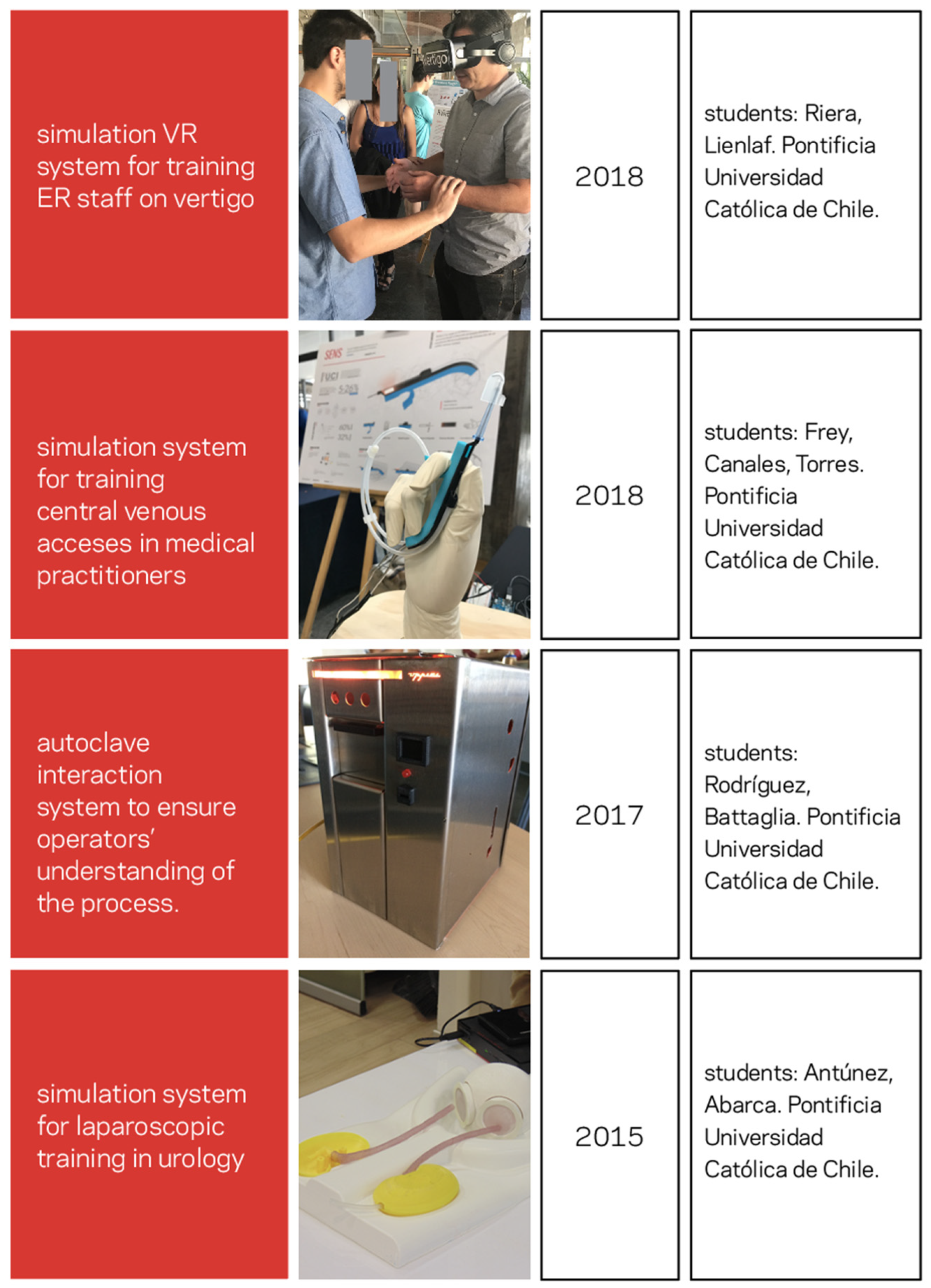
3. Results
3.1. A Simulation VR System for Training ER and UC Staff on Vertigo
3.2. Improving the Context of Operation and Communication of an Autoclave
3.3. Two Simulation Devices
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Shale, C.; Matin, S.; Durr, N.; Logsdon, E. Inclusion of Industry Professional Experts in Biomedical Engineering Design Courses At-scale. In Proceedings of the 2020 ASEE Virtual Annual Conference Content Access Proceedings, ASEE Conferences, Online, 26 June 2020. [Google Scholar]
- Manbachi, A.; Logsdon, E.A.; Yazdi, Y.; Durr, N.J. Curricular Advancement of Biomedical Engineering Undergraduate Design Projects Beyond 1 Year: A Pilot Study. Ann. Biomed. Eng. 2020, 4, 1137–1146. [Google Scholar] [CrossRef] [PubMed]
- Logsdon, E.; Allen, R.; Durr, N.; Nguyen, H. Board # 11 :A Team Leader Model for Biomedical Engineering Design Team Project-Definition Training and Scalable Clinical Observation (Work in Progress). In Proceedings of the 2017 ASEE Annual Conference & Exposition Proceedings, ASEE Conferences, Columbus, OH, USA, 24–28 June 2017. [Google Scholar]
- Eberhardt, A.W.; Johnson, O.L.; Kirkland, W.B.; Dobbs, J.H.; Moradi, L.G. Team-Based Development of Medical Devices: An Engineering-Business Collaborative. J. Biomech. Eng. 2016, 138, 708031–708035. [Google Scholar] [CrossRef] [PubMed]
- The University of Texas at Austin Master of Arts in Design focused on Health. Available online: https://designcreativetech.utexas.edu/ma-design (accessed on 29 January 2022).
- Rice University Master of Bioengineering in Global Medical Innovation. Available online: https://bioengineering.rice.edu/academics/masters-programs/mbe-global-medical-innovation (accessed on 29 January 2022).
- Stanford University Biodesign Innovation. Available online: https://med.stanford.edu/biodesign-stage/programs/stanford-courses/biodesign-innovation.html (accessed on 29 January 2022).
- Duke University BME Design Fellows. Available online: https://bme.duke.edu/undergrad/bme-design-fellows (accessed on 29 January 2022).
- Johns Hopkins University CBID Master’s Program. Available online: https://www.bme.jhu.edu/academics/graduate/masters-programs/cbid-masters-program/ (accessed on 29 January 2022).
- Kahn, C.; Peralta, E.; Langfitt, F. As U.S. Vaccine Rollout Speeds Up, Inequality Stunts Progress Worldwide; NPR: Washington, DC, USA, 2021. [Google Scholar]
- Economic and Social Council UN. Unequal Vaccine Distribution Self-Defeating, World Health Organization Chief Tells Economic and Social Council’s Special Ministerial Meeting. In Press Release UN; United Nations: New York, NY, USA, 2021. [Google Scholar]
- U.S. Food and Drug Administration. Artificial Intelligence and Machine Learning in Software as a Medical Device; U.S. Food & Drug Administration: Silver Spring, MD, USA, 2021.
- U.S. Food and Drug Administration. Proposed Regulatory Framework for Modifications to Artificial Intelligence/Machine Learning (AI/ML)-Based. In Software as a Medical Device (SaMD); U.S. Food & Drug Administration: Silver Spring, MD, USA, 2019. [Google Scholar]
- Cohen, I.G.; Mello, M.M. Big Data, Big Tech, and Protecting Patient Privacy. JAMA 2019, 322, 1141. [Google Scholar] [CrossRef] [PubMed]
- Turkle, S. Alone Together: Why We Expect More from Technology and Less from Each Other; Basic Books: New York, NY, USA, 2012; ISBN 9781459609020. [Google Scholar]
- Lauer, D. Facebook’s ethical failures are not accidental; they are part of the business model. AI Ethics 2021, 1, 395–403. [Google Scholar] [CrossRef] [PubMed]
- Duster, T. Lessons from History: Why Race and Ethnicity Have Played a Major Role in Biomedical Research. J. Law, Med. Ethics 2006, 34, 487–496. [Google Scholar] [CrossRef]
- Roberts, D. Fatal Invention: How Science, Politics, and Big Business Re-Create Race in the Twenty-First Century; The New Press: New York, NY, USA, 2011. [Google Scholar]
- Sufrin, C.; Kolbi-Molinas, A.; Roth, R. Reproductive Justice, Health Disparities And Incarcerated Women in the United States. Perspect. Sex. Reprod. Health 2015, 47, 213–219. [Google Scholar] [CrossRef]
- Bronson, J.; Sufrin, C. Pregnant Women in Prison and Jail Don’t Count: Data Gaps on Maternal Health and Incarceration. Public Health Rep. 2019, 134, 57S–62S. [Google Scholar] [CrossRef]
- Miranda, C.; Goñi, J.; Sotomayor, T. Embracing the social turn: Epistemic change in engineering students enrolled in an anthro-design course. Int. J. Technol. Des. Educ. 2021. [Google Scholar] [CrossRef]
- Brunhaver, S.R.; Korte, R.F.; Barley, S.R.; Sheppard, S.D. Bridging the Gaps between Engineering Education and Practice. In U.S. Engineering in a Global Economy; Freeman, R.B., Salzman, H., Eds.; University of Chicago Press: Chicago, IL, USA, 2018; pp. 129–164. [Google Scholar]
- Gray, C.M.; Fernandez, T.M. When world(view)s collide contested epistemologies and ontologies in transdisciplinary education. Int. J. Eng. Educ. 2018, 34, 574–589. [Google Scholar]
- Bardes, C.L. Defining “Patient-Centered Medicine”. N. Engl. J. Med. 2012, 366, 782–783. [Google Scholar] [CrossRef] [Green Version]
- Charon, R. Narrative Medicine: Form, Function, and Ethics. Ann. Intern. Med. 2001, 134, 83. [Google Scholar] [CrossRef] [PubMed]
- Charon, R. Narrative Medicine: Honoring the Stories of Illness; Oxford University Press: Oxford, UK, 2006. [Google Scholar]
- Charon, R.; DasGupta, S.; Hermann, N.; Irvine, C.; Marcus, E.R.; Rivera Colsn, E.; Spencer, D.; Spiegel, M. The Principles and Practice of Narrative Medicine; Oxford University Press: Oxford, UK, 2016; Volume 1, ISBN 9780199360192. [Google Scholar]
- Petroski, H. An Engineer’s Alphabet: Gleanings from the Softer Side of a Profession; Cambridge University Press: Cambridge, UK, 2011. [Google Scholar]
- Litzinger, T.A.; Lattuca, L.R.; Hadgraft, R.G.; Newstetter, W.C. Engineering Education and the Development of Expertise. J. Eng. Educ. 2011, 100, 123–150. [Google Scholar] [CrossRef]
- ABET. About ABET. 2019. Available online: https://www.abet.org/about-abet/ (accessed on 1 January 2022).
- Stilgoe, J. Innovation Is Not Self-Driving. In Who’s Driving Innovation? Springer International Publishing: Cham, Switzerland, 2020; pp. 7–20. [Google Scholar]
- Newell, A.; Shaw, J.; Simon, H. The Process of Creative Thinking. In Contemporary Approaches to Creative Thinking; Gruber, H., Terrel, G., Wertheimer, M., Eds.; Literary Licensing: New York, NY, USA, 1967; pp. 63–119. [Google Scholar]
- Miranda, C.; Altermatt, F.; Villagrán, I.; Goñi, J. Developing an Innovative Medical Training Simulation Device for Peripheral Venous Access: A User-Centered Design Approach. Healthcare 2020, 8, 420. [Google Scholar] [CrossRef] [PubMed]
- Miranda, C. Mapping Visual Negotiations in Innovation Driven Teams: A Peek into the Design Process Culture of Graduate Engineering Students; North Carolina State University: Raleigh, NC, USA, 2013. [Google Scholar]
- Cooper, A.; Reimann, R. About Face 2.0: The Essentials of Interaction Design; Wiley: Hoboken, NJ, USA, 2003. [Google Scholar]
- Goodwin, K. Designing for the Digital Age: How to Create Human-Centered Products and Services; Wiley: Hoboken, NJ, USA, 2011. [Google Scholar]
- Courage, C.; Baxter, K. Understanding Your Users: A Practical Guide to User Requirements Methods, Tools, and Techniques, 1st ed.; Morgan Kaufmann Publishers Inc.: San Francisco, CA, USA, 2005; ISBN 9780123750921. [Google Scholar]
- Vanderbeeken, M. Taking a broader view of the human experience. Interactions 2009, 16, 54–57. [Google Scholar] [CrossRef]
- Yock, P.G.; Zenios, S.; Makower, J.; Brinton, T.J.; Kumar, U.N.; Watkins, F.T.J.; Denend, L.; Krummel, T.M.; Kurihara, C.Q. Biodesign: The Process of Innovating Medical Technologies, 2nd ed.; Cambridge University Press: Cambridge, UK, 2015; ISBN 9781107087354. [Google Scholar]
- Miranda, C. Crash-Course de Antro-Diseño; Ediciones UC: Santiago, Chile, 2019. [Google Scholar]
- Dreyfuss, H. The Measure of Man, Human Factors in Design; Whitney Library of Design: New York, NY, USA, 1978. [Google Scholar]
- Dreyfuss, H.; Powell, A. Designing for People; Classic of industrial design; Allworth: New York, NY, USA, 2003; ISBN 9781581153125. [Google Scholar]
- Wasson, C. Ethnography in the Field of Design. Hum. Organ. 2000, 59, 377–388. [Google Scholar] [CrossRef]
- Kelly, M.P.; Barker, M. Why is changing health-related behaviour so difficult? Public Health 2016, 136, 109–116. [Google Scholar] [CrossRef] [Green Version]
- Marcus, G.E.; Fischer, M.M.J. Anthropology as Cultural Critique: An Experimental Moment in the Human Sciences; University of Chicago Press: Chicago, IL, USA, 1999; ISBN 9780226504506. [Google Scholar]
- Clifford, J.; Marcus, G.E.; Fortun, K. School of American Research. In Writing Culture: The Poetics and Politics of Ethnography; Anthropology/Literary theory; University of California Press: Berkely, CA, USA, 2010; ISBN 9780520266025. [Google Scholar]
- Mascia-Lees, F.E.; Sharpe, P.; Cohen, C.B. The Postmodernist Turn in Anthropology: Cautions from a Feminist Perspective. Signs J. Women Cult. Soc. 1989, 15, 7–33. [Google Scholar] [CrossRef]
- Reimann, P. Design-Based Research. In Methodological Choice and Design; Springer Netherlands: Dordrecht, The Netherlands, 2011; pp. 37–50. [Google Scholar]
- Wang, F.; Hannafin, M.J. Design-based research and technology-enhanced learning environments. Educ. Technol. Res. Dev. 2005, 53, 5–23. [Google Scholar] [CrossRef]
- Barab, S. Design-Based Research. In The Cambridge Handbook of the Learning Sciences; Sawyer, R.K., Ed.; Cambridge University Press: Cambridge, UK, 2014; pp. 151–170. [Google Scholar]
- Anderson, T.; Shattuck, J. Design-Based Research. Educ. Res. 2012, 41, 16–25. [Google Scholar] [CrossRef] [Green Version]
- Hilliger, I.; Miranda, C.; Pérez-Sanagustín, M. A Methodology to Involve Students in the Evaluation of an Engineering Curriculum in Design, Entrepreneurship, and Innovation. In Proceedings of the 2018 ASEE Annual Conference & Exposition Proceedings; ASEE Conferences, Salt Lake, UT, USA, 23 January–27 July 2018. [Google Scholar]
- Hilliger, I.; Pérez-Sanagustín, M.; Miranda, C.; Berner, C.; Vega, M. What is the theoretical basis of entrepreneurial learning in engineering education? A case study analysis using constructivism. In Proceedings of the Research Engineering Education Symposium, Bogotá, Colombia, 10–12 July 2019. [Google Scholar]
- Miles, M.; Huberman, A. Qualitative Data Analysis: An Expanded Sourcebook; Sage: Thousand Oaks, CA, USA, 1994. [Google Scholar]
- Geertz, C. Local Knowledge: Further Essays In Interpretive Anthropology; Basic Books: New York, NY, USA, 1985; ISBN 9780465041626. [Google Scholar]
- Geertz, C. Thick Description: Toward an Interpretive Theory of Culture; Fontana Press: Roermond, The Netherlands, 1973. [Google Scholar]
- Wolcott, H.F. On seeking, and rejecting, validity in qualitative research. In Qualitative Inquiry in Education; Eisner, E.W., Peshkin, A., Eds.; Teachers College Press: New York, NY, USA, 1990; pp. 121–152. [Google Scholar]
- Harry, F.; Wolcott, U.O. Ethnography: A Way of Seeing; AltaMira Press: Lanham, MD, USA, 2008; ISBN 9780759120600. [Google Scholar]
- Wolcott, H.F. Transforming Qualitative Data: Description, Analysis, and Interpretation; SAGE Publications: Thousand Oaks, CA, USA, 1994; ISBN 9780803952812. [Google Scholar]
- Wolcott, H.F. Ethnography Lessons: A Primer; Taylor & Francis: Milton Park, UK, 2016; ISBN 9781315428956. [Google Scholar]
- Lassiter, L.E. Invitation to Anthropology; Rowman & Littlefield Publishers: Lanham, MD, USA, 2014; ISBN 9780759122550. [Google Scholar]
- Lassiter, L.E. The Chicago Guide to Collaborative Ethnography; Chicago GDES Writing Editing and Publishing CGWEP (CHUP) Series; University of Chicago Press: Chicago, IL, USA, 2005; ISBN 9780226468907. [Google Scholar]
- Margaret, D.; LeCompte, U.C.B.; Jean, J.; Schensul, I.C.R.; Singer, M.; Trotter, R.T.; Cromley, E.K. Mapping Social Networks, Spatial Data, and Hidden Populations; Ethnographer’s Toolkit; AltaMira Press: Lanham, MD, USA, 1999; ISBN 9780759117327. [Google Scholar]
- Schensul, S.L.; Jean J. Schensul Institute for Community Research; Margaret D. LeCompte University of Colorado Boulder. Essential Ethnographic Methods: Observations, Interviews, and Questionnaires; AltaMira Press: Lanham, MD, USA, 1999; ISBN 9780761991441. [Google Scholar]
- Bernard, H.R. Research Methods in Anthropology: Qualitative and Quantitative Approaches; G—Reference; Information and Interdisciplinary Subjects Series; AltaMira Press: Lanham, MD, USA, 2011; ISBN 9780759112414. [Google Scholar]
- Bernard, H.R.; Gravlee, C.C. Handbook of Methods in Cultural Anthropology; Rowman & Littlefield Publishers: Lanham, MD, USA, 2014; ISBN 9780759120723. [Google Scholar]
- Guest, G.; Namey, E.E.; Mitchell, M.L. Collecting Qualitative Data: A Field Manual for Applied Research; SAGE Publications: Thousand Oaks, CA, USA, 2013; ISBN 9781412986847. [Google Scholar]
- Pink, S. Doing Visual Ethnography; Sage: London, UK, 2007. [Google Scholar]
- Alfonso, A.I.; Kurti, L.; Pink, S. Working Images: Visual Research and Representation in Ethnography; Taylor & Francis: Milton Park, UK, 2004; ISBN 9781134401352. [Google Scholar]
- Beebe, J. Rapid Assessment Process: An Introduction; AltaMira Press: Lanham, MD, USA, 2001; ISBN 9780759100121. [Google Scholar]
- Katz, P. The Scalpel’s Edge: The Culture of Surgeons; Allyn and Bacon: Boston, MA, USA, 1999; ISBN 9780205270064. [Google Scholar]
- Musmade, P.; Nijhawan, L.; Udupa, N.; Bairy, K.; Bhat, K.; Janodia, M.; Muddukrishna, B. Informed consent: Issues and challenges. J. Adv. Pharm. Technol. Res. 2013, 4, 134. [Google Scholar] [CrossRef]
- Zahle, J. Privacy, Informed Consent, and Participant Observation. Perspect. Sci. 2017, 25, 465–487. [Google Scholar] [CrossRef] [Green Version]
- AAA Executive Board American Anthropological Association Statement on Ethnography and Institutional Review Boards. Available online: https://www.americananthro.org/ParticipateAndAdvocate/Content.aspx?ItemNumber=1652 (accessed on 29 January 2022).
- Jackson, J.E. “I Am a Fieldnote”: Fieldnotes as a Symbol of Professional Identity. In Fieldnotes; Sanjek, R., Ed.; Cornell University Press: Ithaca, NY, USA, 2019; pp. 1–33. [Google Scholar]
- Emerson, R.M.; Fretz, R.I.; Shaw, L.L. Writing Ethnographic Fieldnotes, 2nd ed.; Chicago Guides to Writing, Editing, and Publishing; University of Chicago Press: Chicago, IL, USA, 2011; ISBN 9780226206868. [Google Scholar]
- Denzin, N.K. The Research Act: A Theoretical Introduction to Sociological Methods; Routledge: Hoboken, NJ, USA, 2017; ISBN 9781315134543. [Google Scholar]
- Adler, P.A.; Adler, P. The Promise and Pitfalls of Going into the Field. Contexts 2003, 2, 41–47. [Google Scholar] [CrossRef] [Green Version]
- Bernard, H.R.; Ryan, G.W. Analyzing Qualitative Data: Systematic Approaches; SAGE Publications: Thousand Oaks, CA, USA, 2010; ISBN 9780761924906. [Google Scholar]
- Charmaz, K. Constructing Grounded Theory: A Practical Guide through Qualitative Analysis; Sage Publications: London, UK, 2006. [Google Scholar]
- Glaser, B.; Strauss, A. The Discovery of Grounded Theory; Aldine Publishing Company: Hawthorne, NY, USA, 1967. [Google Scholar]
- Saldaña, J. The Coding Manual for Qualitative Researchers; Sage: Thousand Oaks, CA, USA, 2009; ISBN 9781847875488. [Google Scholar]
- Sipe, L. Developing Conceptual Categories in Classroom Descriptive Research: Some Problems and Possibilities. Anthropol. Educ. Q. 2004, 35, 472–485. [Google Scholar] [CrossRef]
- Owen, R.; Stilgoe, J.; Macnaghten, P.; Gorman, M.; Fisher, E.; Guston, D. A Framework for Responsible Innovation. In Responsible Innovation; John Wiley & Sons, Ltd.: Chichester, UK, 2013; pp. 27–50. [Google Scholar]
- Linsenmeier, R.A.; Saterbak, A. Fifty Years of Biomedical Engineering Undergraduate Education. Ann. Biomed. Eng. 2020, 48, 1590–1615. [Google Scholar] [CrossRef]
- Lee, J.W.; Ostrowski, A.; Daly, S.R.; Huang-Saad, A.; Seifert, C.M. Idea generation in biomedical engineering courses using Design Heuristics. Eur. J. Eng. Educ. 2019, 44, 360–378. [Google Scholar] [CrossRef]
- Grimm, M.J. Design as a Feature of Biomedical Engineering Education—Satisfying ABET and Preparing Students to Address Clinical Needs. J. Biomech. Eng. 2020, 142. [Google Scholar] [CrossRef]
- Lai, H.L.; Eaton, T. The Use of Qualitative Data Analysis for the Evaluation of Design Ethnography Training Among Undergraduate Engineering Students. In Proceedings of the Volume 5: Engineering Education; American Society of Mechanical Engineers, Salt Lake, UT, USA, 11–14 November 2020. [Google Scholar]
- Jasanoff, S. The Ethics of Invention: Technology and the Human Future; W.W. Norton & Company: New York, NY, USA, 2016. [Google Scholar]
- Tunstall, E. (Dori) The QAME of Trans-disciplinary Ethnography: Making Visible Disciplinary Theories of Ethnographic Praxis as Boundary Object. Ethnogr. Prax. Ind. Conf. Proc. 2008, 2008, 218–233. [Google Scholar] [CrossRef] [Green Version]



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Miranda, C.; Goñi, J.; Labruto, N. Five Qualitative Research Concepts Grounded in Anthropological Methods for Teaching Design in Healthcare. Healthcare 2022, 10, 360. https://doi.org/10.3390/healthcare10020360
Miranda C, Goñi J, Labruto N. Five Qualitative Research Concepts Grounded in Anthropological Methods for Teaching Design in Healthcare. Healthcare. 2022; 10(2):360. https://doi.org/10.3390/healthcare10020360
Chicago/Turabian StyleMiranda, Constanza, Julián Goñi, and Nicole Labruto. 2022. "Five Qualitative Research Concepts Grounded in Anthropological Methods for Teaching Design in Healthcare" Healthcare 10, no. 2: 360. https://doi.org/10.3390/healthcare10020360