1. Introduction
University students face new demands in their adult life, assuming new responsibilities and challenges typical of this stage, such as living outside the family residence and having to buy and cook their own food [
1]. In relation to food, they do not always select healthy options—diets of low nutritional quality, far from the Mediterranean diet (frequently considered very natural or healthy), are frequent [
2].
Students endure long hours of physical and mental effort, and, in many cases, go to the study center having eaten incomplete or very light meals [
3], which can contribute to lower academic performance [
4]. During the university stage, habits are consolidated, and in most cases, last over time. Therefore, we considered university students as a population sensitive to health promotion and prevention activities, since their lifestyles have a direct impact on their physical, psychological and mental development [
5].
College settings are often places with a high availability of refined foods high in simple sugars and fats; where there is a greater restructuring of eating habits; where the use of ICT and social networks favor the consolidation of sedentary activities; with great ignorance regarding eating habits. This context favors the proliferation of restrictive and unbalanced diets, which increase the risk of developing eating behavior disorders, more frequently seen in women [
6].
Carlos Ríos, the creator of the Realfooding movement, points out that there are many problems with having an unhealthy diet. It is dangerous living in a society in which we do not eat real food, and even more so when the brands sold to us in supermarkets are predominantly unhealthy ultra-processed foods. Within an environment controlled by the food industry, which keeps the population continually buying its products against their health [
7], real food proposes a lifestyle that seeks to banish ultra-processed foods. The real food movement is a way of trying to educate people about a healthy diet and fight against processed food, which is considered negative. Real food refers to minimally processed foods whose industrial processing has not worsened the quality of the composition or negatively interfered with its naturally present healthy properties. Within real food, we can find minimally processed foods, whole foods, and unprocessed raw materials, and good processed foods or real foods with beneficial, harmless industrial or artisanal processing with respect to their health properties.
Ultra-processed foods are the opposite of real food; edible industrial preparations are made from different synthetic substances or products, with different processing techniques. They usually have five or more ingredients, and among them are added sugars, refined flours, refined vegetable oils, additives, and salt. Industrially processed ingredients achieve more durable, attractive, tasty, and highly profitable business, thus, they are sold and consumed above the rest of the options. Ultra-processed foods are usually dense in calories per unit of weight, poor in nutrients, widely available throughout our environment, and are promoted with strong marketing and advertising campaigns. They are marketed through large multinationals, covering almost 80% of the groceries sold in supermarkets. All this explains why ultra-processed foods are more successful than unprocessed or minimally processed foods [
8]. This classification, according to Realfooding, is necessary to facilitate healthy food choices (real food) over unhealthy ones (ultra-processed), leaving behind the obsolete classification of many dietitians that is based solely on the chemical composition of the food, which spreads on social networks [
9].
The classification of the Realfooding movement is based on a system developed a decade ago by researchers at the School of Public Health at the University of São Paulo. The system, called NOVA, qualifies foods according to their degree of processing [
10].
Ultra-processed foods predominate in the food systems of the most industrialized countries [
11]. Their consumption is indicated as a risk factor by the increase in obesity, measured by BMI, both in adolescents and adults [
12], and is also associated with body fat in childhood and adolescence [
13]. In addition, several studies show the relationship between ultra-processed foods and the risk of cardiovascular, coronary, cerebrovascular diseases, and cancer [
14,
15]. A recent study, carried out on 139 healthy adolescents between the ages of 13 and 19, revealed that a higher intake of ultra-processed foods was associated with greater oxidative DNA damage [
16]. Other studies show the existence of a direct relationship between the consumption of ultra-processed foods and increased mortality [
17,
18,
19].
The prevalence of obesity has increased in recent decades. In the first major health survey, conducted in Spain (ENS, 1987), obesity prevalence was 7.7% within the adult group, and in 2001 it doubled; in 2006, it reached 15.6%; in 2012 it stood at 15.5%; in 2014 at 16.9%; in 2017 at 17.4%. In 30 years, it has multiplied by 2.3. Men show greater obesity and being overweight than women [
20].
Jaume Marrugat, head of the group of the Center for Biomedical Research in the Cardiovascular Diseases Network at the Hospital del Mar Institute, speaks of a pandemic of being overweight and obese, which has exploded since the year 2000 with a gradual and massive irruption of carbohydrates, sugary drinks, industrial pastries, and the abandonment of customs close to the Mediterranean lifestyle [
21].
A possible cause of being overweight and obese is the imbalance between energy intake and expenditure. Thus, physical activity, together with good eating habits, are the main factors. Several observations in some countries showed that humans can consume recommended daily calories (i.e., not in excess) and become overweight. Obesity does not fully obey a linear and quantitative relationship between ingested and spent calories. Frequent physical activity—more than 2 times per week—is associated with a reduction in excess weight [
20].
The Ministry of Spain, at the end of 2018, announced the adoption of the Nutri-Score nutritional front label, created by the French Public Health Agency, with the aim of helping consumers to judge the nutritional quality of packaged foods [
22].
Frontal packaging labeling (EFE) systems characterize the nutritional quality of food, can reduce the time and cognitive effort in processing the labels, and identify the healthiest food options [
23]. There are two major systems in front labeling:
(a) Nutrient-focused systems. These provide information on certain critical nutrients for health, whose excess intake increases the risk of obesity or other non-communicable diseases. In general, they report on kilocalories, fats, saturated fats, trans fats, salt/sodium, and/or sugars. Examples of this system would be nutritional traffic light labeling and warning labeling, among others.
(b) Summary systems. These are where information arises from an algorithm, based on a global evaluation of the product, in relation to its nutritional content, by synthesizing its nutritional quality in a symbol, icon, or score. In this second group, the Nutri-Score label would be present.
In this context, the Nutri-Score is a way to communicate to the consumers directly related to the real food movement. However, it has been recently shown that around 57% of industrial foods with Nutri-Score A/B are ultra-processed foods [
24], and there is a study that blames industrial foods for childhood obesity [
25,
26]. Australian studies of the health star rating system [
27] showed how the HSR is simple, uncluttered, easy to understand, and useful for a quick comparison across products. The nutrition information is positive, however, there is a perceived lack of transparency in the criteria used to determine the number of stars. Thus, numerous well-rated industrial foods by Nutri-Score are absolutely not “healthy” at all. Nutri-Score summarizes, therefore, a set of unintelligible numbers and terms of nutritional values, located on the back of the packaging, based on a colored logo that is easily understood by consumers. It informs consumers about the nutritional quality of food, facilitating the ability to identify and contrast its nutritional quality, and the choice of options with better nutritional quality [
28]. The adoption of Nutri-Score by public health authorities is justified by studies that show the authenticity and effectiveness of its algorithm, as well as its superiority compared to other existing front-end labeling [
28]. It is debatable, however, that there is a scientific reason for justifying the adoption of this score. The only scientific justification would be that the adoption of such scores worldwide would be really associated with decreased risks of chronic disease prevalence. A study of Spanish consumers indicated that Nutri-Score was well perceived and the characterization of nutritional quality was easy to understand [
29], which allows consumers the possibility of making a better choice of products and verifying the nutritional levels [
30].
In practice, Nutri-Score allows consumers, at a glance, to compare the nutritional quality at the time of purchase:
- -
Foods belonging to different “families” (categories): for example, comparing the quality of yogurts with dessert creams; or foods consumed for breakfast, such as cereals with alternatives, such as sliced bread, cookies, biscuits, industrial pastries, etc.
- -
Food of the same category: for example, cereals, such as mueslis versus chocolate cereals; fruit cookies versus chocolate cookies; different types of pizza with each other; types of drinks (water, fruit juice or soft drinks).
- -
The same type of food, but different brands: for example, canned sardines of different brands.
The Nutri-Score nutritional logo (also known as 5C for its five colors—see
Figure 1) details five types of nutritional quality, going from green (associated with the letter A) to red (associated with the letter E), based on the calculation of an algorithm according to scientifically validated public health criteria [
23]. The algorithm underlying Nutri-Score is a system that was developed in Great Britain in 2005 by a team of Oxford researchers to regulate advertising aimed at children and was validated by the UK Food Standards Agency (FSA) [
31,
32]. In 2015, the Higher Council of Public Health of France [
33] was in charge of delimiting a frontal labeling adaptation of the Anglo-Saxon algorithm that led to the FSAm/HCSP score (initials of the agencies of both countries).
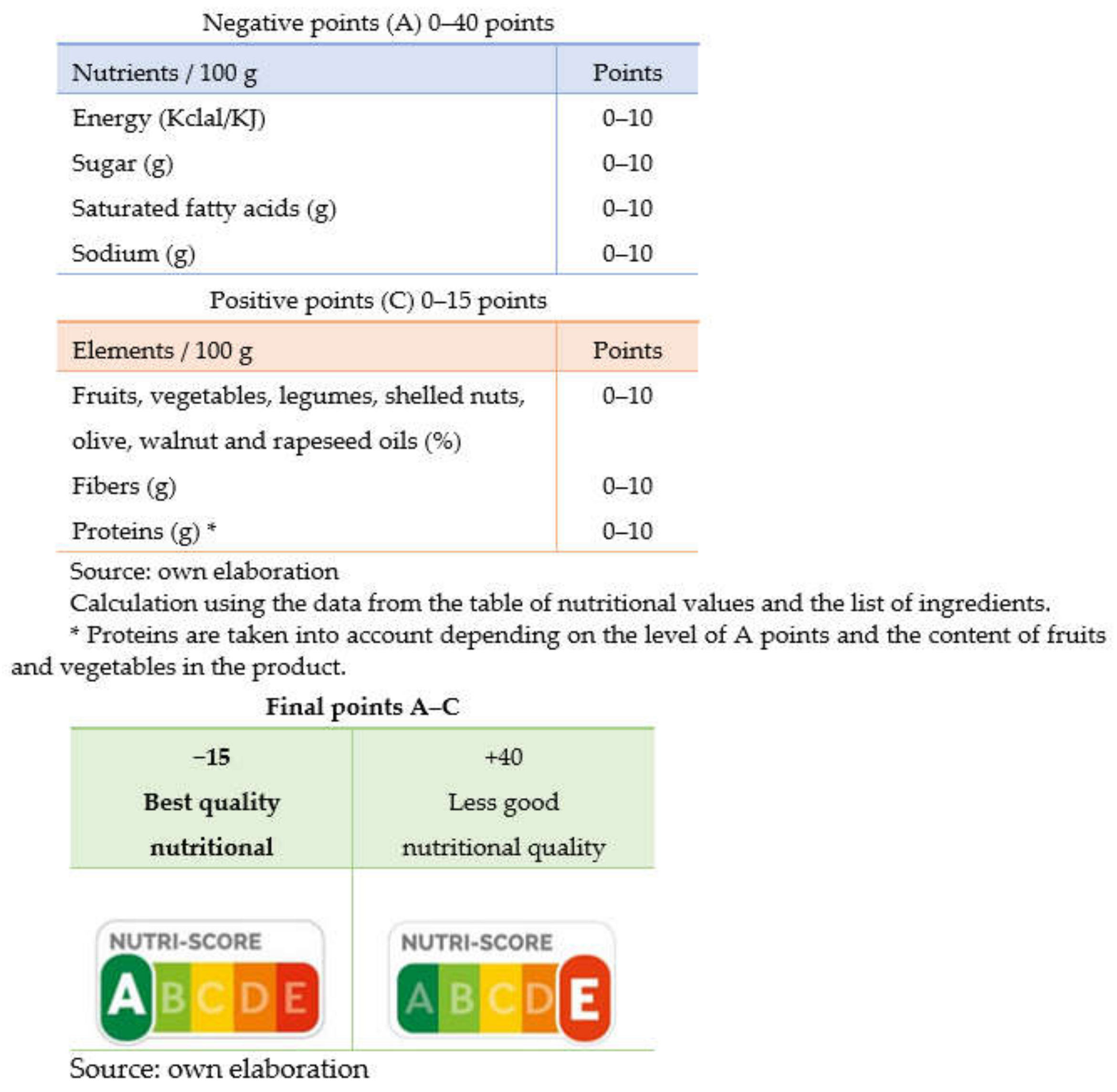
This system is based on the attribution of points based on the nutritional composition per 100 g or 100 mL of a product (
Figure 2).
On the one hand, a calculation is based on the content of nutrients considered “unfavourable” or critical from a nutritional point of view, to which a score of 0 to 10 points is attributed according to their content in kilocalories, simple sugars, saturated fatty acids and sodium (points A). On the other hand, “favorable” nutrients or ingredients (proteins, dietary fiber, and the percentage of fruits, vegetables, legumes, oleaginous fruits, olives, walnuts, and rapeseed oils) are considered and are assigned a score from 0 to 5 points (C points). The first sum of points corresponding to nutrients, points A, is made, and based on these, the total points of C are subtracted, without taking proteins into account.
The final score falls within the range of −15 to +40. Based on four predefined limits, the result is classified into five categories according to nutritional quality, and is represented in five colored circles, ranging from dark green to red, from the best to the worst nutritional quality. The largest circle, oversized, indicates the overall nutritional quality of the product. The association of colors and letters (A/B/C/D/E) seeks to guarantee greater understanding. All the elements used to calculate the Nutri-Score (which has received some critics) appear in the table of the mandatory nutritional declaration and in the list of ingredients located on the back of the packages, which guarantees transparency in the calculation and in the possibility of verifying the representation of the color attributed by Nutri-Score.
In the present study, we analyzed the perception of a group of university students, as a particularly sensitive group from the point of view of nutritional habits [
34,
35] with a low interest in reading nutritional labeling [
30], who submit to information sources that prioritize instantaneity [
36] a natural effect in the context of the broadband society and cloud journalism [
37]. We surveyed their knowledge of nutrition, their degree of understanding of the Nutri-Score nutritional front labeling, their perceptions about food, and their level of knowledge of nutrition issues. An indirect effect of the study and the survey method used was to inform the participants of nutritional aspects and the function of the Nutri-Score label.
This observational cross-sectional study focuses on analyzing eating habits and nutritional knowledge in a sample of university students, as well as the Nutri-Score labeling system. We considered this sample as attending to the problems of leaving home, isolation, and new relationships, and the stress produced by a stronger level of university studies.
4. Discussion and Conclusions
We observed that 87.5% of the students participating in the study have a BMI within the normal weight range. A total of 11.2% of students are overweight or obese; this is soothing to note due to the relationship between the consumption of ultra-processed foods and mortality [
17,
18,
19].
It is striking, however, that most of those who are overweight or obese perceive their diet in a distorted way, qualifying it as normal or even very healthy. Neither sex nor age, the type of university, studies, or branches of knowledge influences how the study participants perceived their diet. A total of 86.9% of the participants (university students) considered their diet as normal, very healthy, or quite healthy. Only 11.8% admitted to having an unhealthy diet—the rest did not know. However, the results showed that this perception is wrong. Despite the fact that university students (70.8%) claim to know how to differentiate the foods that are within the NOVA food classification system, the data collected shows just the opposite.
The consumption of ultra-processed foods by the respondents is too high to consider that they have a normal or healthy diet. Weekly, 71% admitted to consuming soft drinks, 83% for snacks, 83% for nuggets, 67% for pastries, and 68% for alcohol. A total of 25.5% did not know the adequate or optimal amount of the daily consumption for salt and sugar. More information, however, is considered to be positive, granting people a better choice of products, and checking nutritional levels [
30].
A total of 20.2% acknowledge not knowing how to differentiate between unprocessed, processed, or ultra-processed products. This was confirmed in the product classification test, where 50% misclassified Nocilla/Nutella, 70% for oat flakes, 71% for canned lentils, and 68% for ham. Our data demonstrate the great lack of knowledge that exists about what is eaten.
An alarming fact, which reflects the lack of information and awareness about what is eaten, is that 64% declared that they sometimes or never read the nutritional information of the products. A total of 33% did not know what the Nutri-Score label indicates, although some studies indicated that Nutri-Score is well perceived and the characterization of nutritional quality is easy to understand [
28].
Those who perceive their diet as healthier are participants with a lower BMI, exercise regularly and read product labels—especially nutritional information, expiration dates, and ingredients.
Women show a better knowledge of processed products, in addition to the fact that they tend to consume less ultra-processed products than men, especially alcohol, bars, and energy drinks. Therefore, some did seem to manage their new responsibilities and greater autonomy more effectively, without the quality of their diet being conditioned by their new circumstances (more sedentary life and availability of less healthy products), thus, ceasing to be a vulnerable group from a nutritional point of view [
3].
Being overweight, in the participants, is associated with no physical activity and a lack of nutritional information—94% of those who are overweight say they did not know the recommended daily amounts of salt and sugar.
Of the mandatory food information that is reflected in the labeling [
30], the students’ focus was mainly on nutritional information (49.1%), being the most consulted element by almost half of the students, and was higher in the case of women. However, there is a greater interest in the expiration date or preferential consumption than in the ingredients, the latter being essential for the identification of healthy products.
The participants, in general, do not read the labels—their nutritional information. A total of 64% only sometimes or never read the labels, mainly due to the excess of information, not considering it important, and the difficulty of understanding the symbols. A total of 33% did not know the meaning of the Nutri-Score label. It was difficult for them to know the degree of the healthiness of the products, to identify the healthiest, and 25% considered that it was quite or very difficult to determine if they were healthy. They recognized that labels such as the Nutri-Score would help them to better choose the products they consume. Those who live outside the family home consume more alcohol and soft drinks.
A total of 72% of students admit to having bought food products due to the influence of the information displayed on the front of the package. Men seem somewhat more easily influenced (77% compared to 69% for women).
A total of 65.8% of the people surveyed admit having seen the Nutri-Score nutritional label on the front, being the highest level of recognition in the case of women. The majority (49.1%) correctly affirmed that its meaning is the degree of nutritional quality of a product. When comparing the labels of two products, one with the Nutri-Score scheme and the other with the CDO label, it was observed that 88.8% of the participating university students say they better interpreted the product labeled with Nutri-Score; therefore, it seems to be an easy-to-use system for understanding [
23]. Likewise, for 88.8% of those surveyed, this label would help them to introduce more healthy foods into their diet, more so in the group of women. Therefore, due to the easy interpretation of the Nutri-Score logo and the lack of other tools that help participants make healthier decisions, Nutri-Score is postulated as a good guidance system for healthier food purchase decisions.
Previous research studies on the understanding of the Nutri-Score labeling, or other nutritional labels that help people make healthy food choices in the university population, are scarce.
The sample is somewhat small (161 individuals) and the non-probabilistic sampling prevents making generalizations from the data collected. Therefore, we are dealing with an exploratory study. A larger, probabilistic sample would allow broader and more robust generalizations to be made.
Some relevant information could not be verified, such as the self-reported data on weight, height, or the perception of food, thus, certain variables may contain bias or inaccuracy to a certain degree.
For subsequent lines of research, it is recommended to carry out a new survey on a larger, probabilistic sample of university students about the Nutri-Score logo, and its influence on the purchase decision. In addition to this, exploring and analyzing new trends and habits, such as the influence and consumption of certain channels and influencers, as well as some apps to analyze the food barcode in situ, is recommended. Currently, there are few brands that include the Nutri-Score label, as it is not required. However, it is being adopted by more products every day, and awareness of proper nutrition is increasing.


 ,
, 


{kind=link}
{kind=link}