
Adult Normative Data for the Adaptation of the Hearing in Noise Test in European French (HINT-5 Min)

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Testing Procedure
2.3. Voice and Noise Equipment
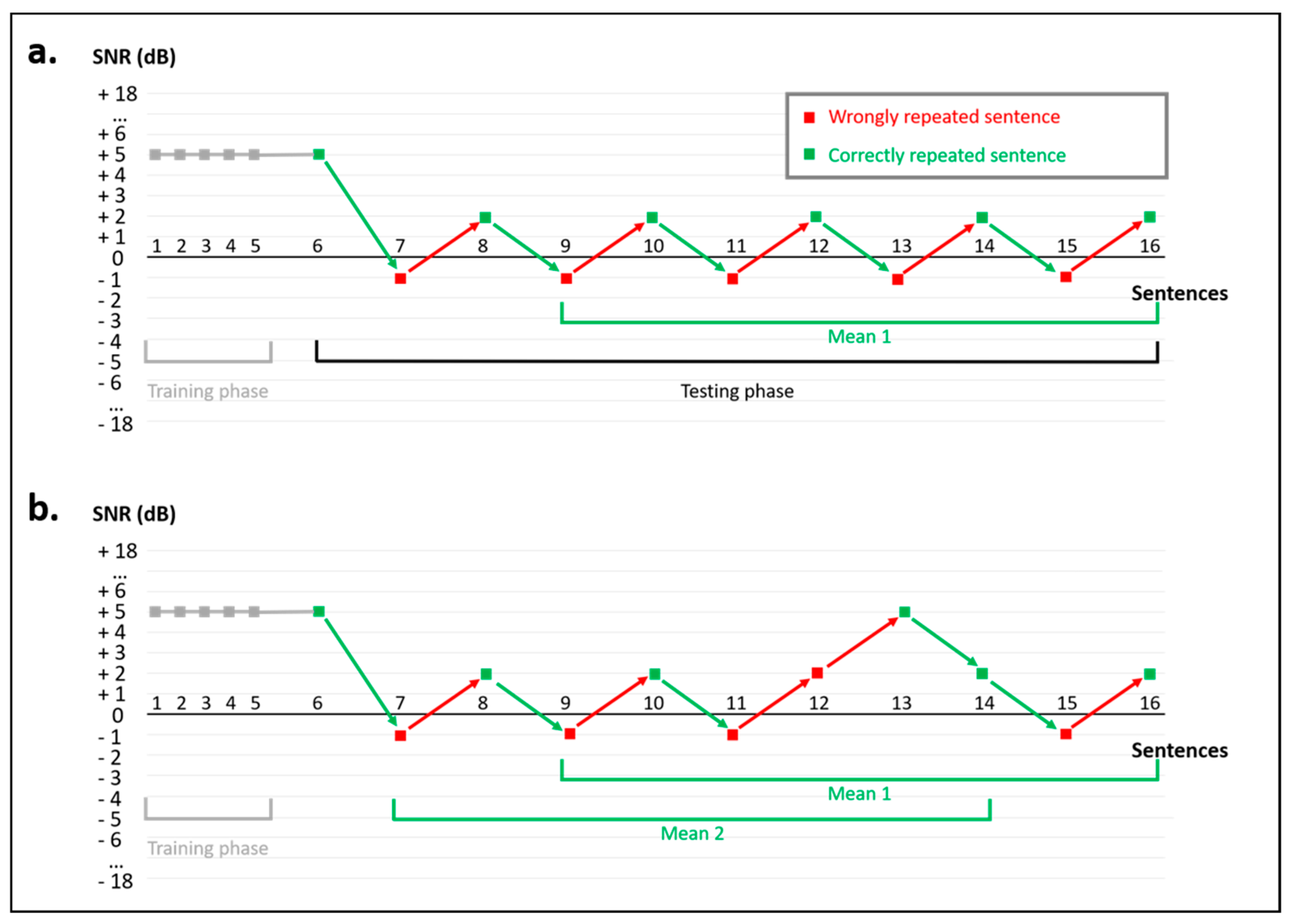
2.4. HINT-5 Min Procedure
2.5. Statistical Analyses
3. Results
3.1. Participants
3.2. Comparison of SRT50 Scores between Ears
3.3. Comparison of SRT50 Scores between the Binaural Headphone and Free-Field Conditions
3.4. Reproducibility of the HINT-5 Min
3.5. Effect of Age and Sex
3.6. Normative Values for the HINT-5 Min
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kumar, G.; Amen, F.; Roy, D. Normal Hearing Tests: Is a Further Appointment Really Necessary? J. R. Soc. Med. 2007, 100, 66. [Google Scholar] [CrossRef] [PubMed]
- Carhart, R.; Tillman, T.W. Interaction of Competing Speech Signals with Hearing Losses. Arch. Otolaryngol. Chic. Ill 1970, 91, 273–279. [Google Scholar] [CrossRef]
- Smoorenburg, G.F. Speech Reception in Quiet and in Noisy Conditions by Individuals with Noise-Induced Hearing Loss in Relation to Their Tone Audiogram. J. Acoust. Soc. Am. 1992, 91, 421–437. [Google Scholar] [CrossRef]
- Bergeron, F.; Berland, A.; Fitzpatrick, E.M.; Vincent, C.; Giasson, A.; Leung Kam, K.; Chafiq, W.; Fanouillère, T.; Demers, D. Development and Validation of the FrBio, an International French Adaptation of the AzBio Sentence Lists. Int. J. Audiol. 2019, 58, 510–515. [Google Scholar] [CrossRef] [PubMed]
- Ben-David, B.M.; Tse, V.Y.Y.; Schneider, B.A. Does It Take Older Adults Longer than Younger Adults to Perceptually Segregate a Speech Target from a Background Masker? Hear. Res. 2012, 290, 55–63. [Google Scholar] [CrossRef]
- Füllgrabe, C.; Moore, B.C.J.; Stone, M.A. Age-Group Differences in Speech Identification despite Matched Audiometrically Normal Hearing: Contributions from Auditory Temporal Processing and Cognition. Front. Aging Neurosci. 2015, 6, 347. [Google Scholar] [CrossRef] [PubMed]
- Fallon, M.; Trehub, S.E.; Schneider, B.A. Children’s Use of Semantic Cues in Degraded Listening Environments. J. Acoust. Soc. Am. 2002, 111, 2242–2249. [Google Scholar] [CrossRef] [Green Version]
- Humes, L.E. Factors Underlying Individual Differences in Speech-Recognition Threshold (SRT) in Noise Among Older Adults. Front. Aging Neurosci. 2021, 13, 702739. [Google Scholar] [CrossRef]
- Lagacé, J.; Jutras, B.; Gagné, J.-P. Auditory Processing Disorder and Speech Perception Problems in Noise: Finding the Underlying Origin. Am. J. Audiol. 2010, 19, 17–25. [Google Scholar] [CrossRef]
- Tun, P.A.; O’Kane, G.; Wingfield, A. Distraction by Competing Speech in Young and Older Adult Listeners. Psychol. Aging 2002, 17, 453–467. [Google Scholar] [CrossRef]
- Tun, P.A.; Williams, V.A.; Small, B.J.; Hafter, E.R. The Effects of Aging on Auditory Processing and Cognition. Am. J. Audiol. 2012, 21, 344–350. [Google Scholar] [CrossRef]
- Bamiou, D.-E.; Iliadou, V.V.; Zanchetta, S.; Spyridakou, C. What Can We Learn about Auditory Processing from Adult Hearing Questionnaires? J. Am. Acad. Audiol. 2015, 26, 824–837. [Google Scholar] [CrossRef] [PubMed]
- Iliadou, V.V.; Ptok, M.; Grech, H.; Pedersen, E.R.; Brechmann, A.; Deggouj, N.; Kiese-Himmel, C.; Śliwińska-Kowalska, M.; Nickisch, A.; Demanez, L.; et al. A European Perspective on Auditory Processing Disorder-Current Knowledge and Future Research Focus. Front. Neurol. 2017, 8, 622. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Glyde, H.; Hickson, L.; Cameron, S.; Dillon, H. Problems Hearing in Noise in Older Adults: A Review of Spatial Processing Disorder. Trends Amplif. 2011, 15, 116–126. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sardone, R.; Battista, P.; Donghia, R.; Lozupone, M.; Tortelli, R.; Guerra, V.; Grasso, A.; Griseta, C.; Castellana, F.; Zupo, R.; et al. Age-Related Central Auditory Processing Disorder, MCI, and Dementia in an Older Population of Southern Italy. Otolaryngol. Neck Surg. 2020, 163, 348–355. [Google Scholar] [CrossRef]
- Iliadou, V.V.; Moschopoulos, N.; Sidiras, C.; Eleftheriadou, A.; Nimatoudis, I. Over-Diagnosis of Cognitive Deficits in Psychiatric Patients May Be the Result of Not Controlling for Hearing Sensitivity and Auditory Processing: Letters to the Editor. Psychiatry Clin. Neurosci. 2018, 72, 742. [Google Scholar] [CrossRef]
- Iliadou, V.V.; Bamiou, D.-E.; Sidiras, C.; Moschopoulos, N.P.; Tsolaki, M.; Nimatoudis, I.; Chermak, G.D. The Use of the Gaps-In-Noise Test as an Index of the Enhanced Left Temporal Cortical Thinning Associated with the Transition between Mild Cognitive Impairment and Alzheimer’s Disease. J. Am. Acad. Audiol. 2017, 28, 463–471. [Google Scholar] [CrossRef]
- Iliadou, V.V.; Ptok, M.; Grech, H.; Pedersen, E.R.; Brechmann, A.; Deggouj, N.; Kiese-Himmel, C.; S’liwin’ska-Kowalska, M.; Nickisch, A.; Demanez, L.; et al. European 17 Countries Consensus Endorses More Approaches to APD than Reported in Wilson 2018. Int. J. Audiol. 2018, 57, 395–396. [Google Scholar] [CrossRef]
- Boothalingam, S.; Purcell, D.W.; Allan, C.; Allen, P.; Macpherson, E. Auditory Localization and Spatial Release From Masking in Children With Suspected Auditory Processing Disorder. Ear Hear. 2019, 40, 1187–1196. [Google Scholar] [CrossRef]
- Kumar, P.; Singh, N.K.; Hussain, R.O. Effect of Speech in Noise Training in the Auditory and Cognitive Skills in Children with Auditory Processing Disorders. Int. J. Pediatr. Otorhinolaryngol. 2021, 146, 110735. [Google Scholar] [CrossRef]
- Bamiou, D.E.; Musiek, F.E.; Luxon, L.M. Aetiology and Clinical Presentations of Auditory Processing Disorders--a Review. Arch. Dis. Child. 2001, 85, 361–365. [Google Scholar] [CrossRef] [PubMed]
- Chermak, G.D.; Bamiou, D.-E.; Iliadou, V.; Musiek, F.E. Practical Guidelines to Minimise Language and Cognitive Confounds in the Diagnosis of CAPD: A Brief Tutorial. Int. J. Audiol. 2017, 56, 499–506. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moschopoulos, N.; Nimatoudis, I.; Kaprinis, S.; Boutsikos, K.; Sidiras, C.; Iliadou, V. Implications for Early Diagnosis and Treatment in Schizophrenia Due to Correlation between Auditory Perceptual Deficits and Cognitive Impairment. J. Clin. Med. 2021, 10, 4557. [Google Scholar] [CrossRef] [PubMed]
- Stavrinos, G.; Iliadou, V.M.; Edwards, L.; Sirimanna, T.; Bamiou, D.-E. The Relationship between Types of Attention and Auditory Processing Skills: Reconsidering Auditory Processing Disorder Diagnosis. Front. Psychol. 2018, 9, 34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murphy, C.F.B.; Rabelo, C.M.; Silagi, M.L.; Mansur, L.L.; Bamiou, D.E.; Schochat, E. Auditory Processing Performance of the Middle-Aged and Elderly: Auditory or Cognitive Decline? J. Am. Acad. Audiol. 2018, 29, 005–014. [Google Scholar] [CrossRef]
- Reynard, P.; Lagacé, J.; Joly, C.A.; Dodelé, L.; Veuillet, E.; Thai-Van, H. Speech-in-Noise Audiometry in Adults: A Review of the Available Tests for French Speakers. Audiol. Neurotol. 2021; ahead of print. [Google Scholar]
- Kollmeier, B.; Warzybok, A.; Hochmuth, S.; Zokoll, M.A.; Uslar, V.; Brand, T.; Wagener, K.C. The Multilingual Matrix Test: Principles, Applications, and Comparison across Languages: A Review. Int. J. Audiol. 2015, 54, 3–16. [Google Scholar] [CrossRef]
- Spyridakou, C.; Rosen, S.; Dritsakis, G.; Bamiou, D.-E. Adult Normative Data for the Speech in Babble (SiB) Test. Int. J. Audiol. 2020, 59, 33–38. [Google Scholar] [CrossRef]
- Jansen, S.; Luts, H.; Wagener, K.C.; Kollmeier, B.; Del Rio, M.; Dauman, R.; James, C.; Fraysse, B.; Vormès, E.; Frachet, B.; et al. Comparison of Three Types of French Speech-in-Noise Tests: A Multi-Center Study. Int. J. Audiol. 2012, 51, 164–173. [Google Scholar] [CrossRef]
- Leclercq, F.; Renard, C.; Vincent, C. Speech Audiometry in Noise: Development of the French-Language VRB (Vocale Rapide Dans Le Bruit) Test. Eur. Ann. Otorhinolaryngol. Head Neck Dis. 2018, 135, 315–319. [Google Scholar] [CrossRef]
- Sidiras, C.; Iliadou, V.V.; Chermak, G.D.; Nimatoudis, I. Assessment of Functional Hearing in Greek-Speaking Children Diagnosed with Central Auditory Processing Disorder. J. Am. Acad. Audiol. 2016, 27, 395–405. [Google Scholar] [CrossRef]
- Sofokleous, V.; Marmara, M.; Panagiotopoulos, G.K.; Mouza, S.; Tsofidou, M.; Sereti, A.; Grigoriadi, I.; Petridis, Ε.; Sidiras, C.; Tsiourdas, M.; et al. Test-Retest Reliability of the Greek Speech-in-Babble Test (SinB) as a Potential Screening Tool for Auditory Processing Disorder. Int. J. Pediatr. Otorhinolaryngol. 2020, 131, 109848. [Google Scholar] [CrossRef] [PubMed]
- Joly, C.-A.; Reynard, P.; Mezzi, K.; Bakhos, D.; Bergeron, F.; Bonnard, D.; Borel, S.; Bouccara, D.; Coez, A.; Dejean, F.; et al. Guidelines of the French Society of Otorhinolaryngology-Head and Neck Surgery (SFORL) and the French Society of Audiology (SFA) for Speech-in-Noise Testing in Adults. Eur. Ann. Otorhinolaryngol. Head Neck Dis. 2021, 139, 21–27. [Google Scholar] [CrossRef] [PubMed]
- Theunissen, M.; Swanepoel, D.W.; Hanekom, J. Sentence Recognition in Noise: Variables in Compilation and Interpretation of Tests. Int. J. Audiol. 2009, 48, 743–757. [Google Scholar] [CrossRef]
- Nilsson, M.; Soli, S.D.; Sullivan, J.A. Development of the Hearing in Noise Test for the Measurement of Speech Reception Thresholds in Quiet and in Noise. J. Acoust. Soc. Am. 1994, 95, 1085–1099. [Google Scholar] [CrossRef] [PubMed]
- Myhrum, M.; Tvete, O.E.; Heldahl, M.G.; Moen, I.; Soli, S.D. The Norwegian Hearing in Noise Test for Children. Ear Hear. 2016, 37, 80–92. [Google Scholar] [CrossRef] [PubMed]
- Novelli, C.L.; de Carvalho, N.G.; Colella-Santos, M.F. Hearing in Noise Test, HINT-Brazil, in Normal-Hearing Children. Braz. J. Otorhinolaryngol. 2018, 84, 360–367. [Google Scholar] [CrossRef]
- Vaillancourt, V.; Laroche, C.; Mayer, C.; Basque, C.; Nali, M.; Eriks-Brophy, A.; Soli, S.D.; Giguère, C. Adaptation of the HINT (Hearing in Noise Test) for Adult Canadian Francophone Populations. Int. J. Audiol. 2005, 44, 358–369. [Google Scholar] [CrossRef]
- Vaillancourt, V.; Laroche, C.; Giguère, C.; Soli, S.D. Establishment of Age-Specific Normative Data for the Canadian French Version of the Hearing in Noise Test for Children. Ear Hear. 2008, 29, 453–466. [Google Scholar] [CrossRef]
- Gifford, R.H.; Shallop, J.K.; Peterson, A.M. Speech Recognition Materials and Ceiling Effects: Considerations for Cochlear Implant Programs. Audiol. Neurootol. 2008, 13, 193–205. [Google Scholar] [CrossRef]
- Massa, S.T.; Ruckenstein, M.J. Comparing the Performance Plateau in Adult Cochlear Implant Patients Using HINT and AzBio. Otol. Neurotol. 2014, 35, 598–604. [Google Scholar] [CrossRef]
- Poissant, S.F.; Bero, E.M.; Busekroos, L.; Shao, W. Determining Cochlear Implant Users’ True Noise Tolerance: Use of Speech Reception Threshold in Noise Testing. Otol. Neurotol. 2014, 35, 414–420. [Google Scholar] [CrossRef] [PubMed]
- Soli, S.D.; Wong, L.L.N. Assessment of Speech Intelligibility in Noise with the Hearing in Noise Test. Int. J. Audiol. 2008, 47, 356–361. [Google Scholar] [CrossRef] [PubMed]
- Listes-de-Phrases-Hint—Collège-National-d-Audioprothèse. Available online: https://doczz.fr/doc/626771/listes-de-phrases-hint---coll%C3%A8ge-national-d-audioproth%C3%A8se (accessed on 1 June 2022).
- Dreschler, W.A.; Verschuure, H.; Ludvigsen, C.; Westermann, S. ICRA Noises: Artificial Noise Signals with Speech-like Spectral and Temporal Properties for Hearing Instrument Assessment. International Collegium for Rehabilitative Audiology. Audiol. Off. Organ Int. Soc. Audiol. 2001, 40, 148–157. [Google Scholar] [CrossRef]
- Valente, M.; Fabry, D.A.; Potts, L.G. Recognition of Speech in Noise with Hearing Aids Using Dual Microphones. J. Am. Acad. Audiol. 1995, 6, 440–449. [Google Scholar]
- Valente, M.; Schuchman, G.; Potts, L.G.; Beck, L.B. Performance of Dual-Microphone in-the-Ear Hearing Aids. J. Am. Acad. Audiol. 2000, 11, 181–189. [Google Scholar] [CrossRef]
- Ricketts, T.; Dhar, S. Comparison of Performance across Three Directional Hearing Aids. J. Am. Acad. Audiol. 1999, 10, 180–189. [Google Scholar] [CrossRef]
- Ricketts, T.; Henry, P. Evaluation of an Adaptive, Directional-Microphone Hearing Aid. Int. J. Audiol. 2002, 41, 100–112. [Google Scholar] [CrossRef]
- Preves, D.A.; Sammeth, C.A.; Wynne, M.K. Field Trial Evaluations of a Switched Directional/Omnidirectional in-the-Ear Hearing Instrument. J. Am. Acad. Audiol. 1999, 10, 273–284. [Google Scholar] [CrossRef]
- Tran, Y.; Tang, D.; Lo, C.; McMahon, C.; Mitchell, P.; Gopinath, B. Co-Occurring Hearing Loss and Cognitive Decline in Older Adults: A Dual Group-Based Trajectory Modeling Approach. Front. Aging Neurosci. 2021, 13, 794787. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| Right Ear | Left Ear | Paired t-Test | |
|---|---|---|---|
| Test (n = 83), mean (SD) | −0.8 (±1.3) | −0.8 (±1.4) | p = 0.81 (ns) |
| Retest (n = 52), mean (SD) | −0.9 (±1.5) | −1.0 (±1.3) | p = 0.49 (ns) |
| Binaural Free Field | Binaural Headphones | Paired t-Test | |
|---|---|---|---|
| Test (n = 83), mean (SD) | −1.0 (±1.3) | −1.4 (±1.4) | p = 0.06 (ns) |
| Retest (n = 52), mean (SD) | −1.2 (±1.2) | −1.3 (±1.3) | p = 0.84 (ns) |
| Test (n = 52) | Retest (n = 52) | Paired t-Test | |
|---|---|---|---|
| Binaural free field, mean (SD) | −1.1 (±1.2) | −1.2 (±1.2) | p = 0.65 (ns) |
| Binaural headphones, mean (SD) | −1.6 (±1.5) | −1.3 (±1.3) | p = 0.14 (ns) |
| Right ear headphones, mean (SD) | −0.6 (±1.5) | −0.9 (±1.5) | p = 0.42 (ns) |
| Left ear headphones, mean (SD) | −0.7 (±1.4) | −1.0 (±1.3) | p = 0.21 (ns) |
| Female (n = 46) | Male (n = 37) | t-Test | |
|---|---|---|---|
| Mean (SD) | −1.0 (±1.2) | −1.1 (±1.4) | p = 0.58 (ns) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Buisson Savin, J.; Reynard, P.; Bailly-Masson, E.; Joseph, C.; Joly, C.-A.; Boiteux, C.; Thai-Van, H. Adult Normative Data for the Adaptation of the Hearing in Noise Test in European French (HINT-5 Min). Healthcare 2022, 10, 1306. https://doi.org/10.3390/healthcare10071306
Buisson Savin J, Reynard P, Bailly-Masson E, Joseph C, Joly C-A, Boiteux C, Thai-Van H. Adult Normative Data for the Adaptation of the Hearing in Noise Test in European French (HINT-5 Min). Healthcare. 2022; 10(7):1306. https://doi.org/10.3390/healthcare10071306
Chicago/Turabian StyleBuisson Savin, Johanna, Pierre Reynard, Eric Bailly-Masson, Célia Joseph, Charles-Alexandre Joly, Catherine Boiteux, and Hung Thai-Van. 2022. "Adult Normative Data for the Adaptation of the Hearing in Noise Test in European French (HINT-5 Min)" Healthcare 10, no. 7: 1306. https://doi.org/10.3390/healthcare10071306
APA StyleBuisson Savin, J., Reynard, P., Bailly-Masson, E., Joseph, C., Joly, C.-A., Boiteux, C., & Thai-Van, H. (2022). Adult Normative Data for the Adaptation of the Hearing in Noise Test in European French (HINT-5 Min). Healthcare, 10(7), 1306. https://doi.org/10.3390/healthcare10071306