Abstract
Empathy, the process of coming to know, understand, and care for another person, is a skill that can be learned; however, there is not a shared definition of empathy or understanding of how to operationalize empathy into practice. Healthcare worker empathy has been shown to have a beneficial effect on both patient health outcomes and the emotional wellness of healthcare workers. Empathic care is associated with more efficient, cost-effective, improved healthcare, and increased provider trust. The purpose of this rapid scoping review is to identify, compare, and contrast empathy training offered to select healthcare professional students (e.g., nurses, nurse practitioners, and pharmacists) as part of the general curriculum or as an elective. We utilized a rapid scoping review approach to identify potentially relevant peer-reviewed articles and studies for inclusion. Six electronic databases were searched, including: MEDLINE; EMBASE; PUBMed; CINAHL; EBSCOHOST; and ERIC, covering the past 10 years. A total of 4977 citations, 3480 abstracts, and 428 papers were screened. Fifty studies fulfilled the eligibility criteria. Of those, 21 primarily non-randomized experimental studies published between 2012 and 2021 were included in the final review. Over 80 percent of the training took place in the classroom setting and utilized active learning strategies. There is little consensus on how to best train future healthcare providers to provide empathic care to patients.
1. Introduction
Empathy, the process of coming to know, understand, and care for another person, is a skill that can be learned and developed over time [1,2]. Empathy involves not only feeling emotions but recognizing the emotions and putting yourself “in the shoes” of others [3]. Many individuals struggle to recognize/understand, share, and respond to social empathy cues, and this is particularly concerning in healthcare settings [4,5,6,7,8].
Healthcare worker empathy has been shown to have a beneficial effect on patient satisfaction and health outcomes, as well as the emotional wellness of healthcare workers [9,10]. The use of empathy in healthcare has been shown to have numerous benefits, including patient outcomes and increased provider trust. Additionally, empathy can help prevent medical paternalism, which continues to be a problem in the US healthcare system. A teachable and sustainable human resource, healthcare worker empathy is believed to be a necessary competency for all healthcare workers caring directly for patients (e.g., physicians, nurses, pharmacists, public health providers, etc.) and those working on interdisciplinary healthcare teams [4,11,12,13,14].
Empathic healthcare workers let patients know they are not alone and support patient self-efficacy, treatment adherence, and disease management planning, thus improving patient health outcomes and helping patients reach their health goals [15,16]. Empathic care is associated with more efficient, cost-effective healthcare (improved diagnostic accuracy) and increased provider trust [15,16,17]. Although no consensus definition of clinical empathy exists, empathy among current and future healthcare providers has been measured and the impact of both cognitive and affective elements of relationship-centered communication, a proxy for empathy, has been studied [1,18,19,20,21,22,23]. Studies suggest that healthcare worker empathy is associated with lower malpractice claims rates, job satisfaction, and reduced burnout [17].
Empathy training has been found to not only promote empathy but to prevent empathy deficits and erosion, thereby improving the ability of healthcare workers to counteract both prejudgments and stereotypes [24,25]. However, empathy training provided to healthcare workers does not appear to be standardized—it differs across healthcare worker/student groups and may erode over time, requiring additional training and support [2,20,21,22,23,26]. The purpose of this rapid scoping review is to identify, compare, and contrast empathy training offered to select healthcare professional students (e.g., nursing, pharmacy) as part of the general academic curriculum or as an elective.
2. Materials and Methods
We utilized a rapid scoping review approach in line with the methods recommended by Tricco in BMC Medicine and Arksey in Int J Soc Res Methodology to establish the scoping review protocol [27,28,29,30,31]. The protocol, search criteria, MESH terms, and inclusion criteria were revised based on feedback from a multidisciplinary research team and our medical librarian partners. Initial search terms included (empathy OR compassion OR sympathy OR humanism OR caring OR kindness) AND (curriculum OR curricula OR lesson OR program) AND (“health care”) AND (“higher education” OR school OR college OR graduate). For the search conducted in ERIC, the assessment included (empathy OR compassion OR sympathy OR humanism OR caring OR kindness) AND (curriculum OR curricula OR lesson OR program) AND (“health care”) AND (“higher education” OR school OR college OR graduate) AND “student”.
To identify potentially relevant peer-reviewed articles and studies for inclusion, six electronic databases were searched: MEDLINE; EMBASE; PUBMed; CINAHL; EBSCOHOST; and ERIC. The search was limited to the last 10 years (2012–2022) and was supplemented by a targeted literature search of relevant education journals in the identified three healthcare disciplines of interest (i.e., nurses, nurse practitioners, pharmacists). To ensure that all relevant studies were included, we reviewed the top 25 percent of articles that resulted from a Google Scholar search using the following search strategy: (empathy OR compassion OR sympathy OR humanism OR caring OR kindness) AND (curriculum OR curricula OR lesson OR program) AND (“health care”) AND (“higher education” OR school OR college OR graduate), which resulted in 3000 articles, of which the top 500 matches were reviewed. Lastly, a list of manuscripts that should be included in a “successful search” were established by the research team to confirm the appropriateness of search terms and plan.
Inclusion screening criteria were established a priori and focused on (1) empathy, the process of coming to know, understand, and care for another person [2], including the cognitive and affective elements related to communication or relationship building; (2) the population of interest (select healthcare professional students in one of the nursing and pharmacy and/or select medical providers (physician assistants, nurse practitioners); and (3) education, training, or other interventions offered to healthcare students as part of the required curriculum or as an elective, mandatory or optional lectures, and fully integrated, longitudinal, brief, or episodic curricular themes [2,16,23]. In addition, training studies outside the United States and studies that focused on post-graduate training were flagged for further review to determine if their empathy training study should be included in the scoping review.
All 3480 abstracts and 428 papers uploaded into covidence.org (an online, system review production tool for title/abstract screening, full-text screening, data abstraction, and quality assessment). While the studies varied in methodological quality and study design, they generally utilized active learning strategies in a classroom setting. This suggests that these strategies may be effective in promoting the development of empathic skills and attitudes among providers. All abstracts and full-text papers were independently reviewed by team-member pairs and all discrepancies resolved through research team discussion via Zoom (a secure, video conferencing platform). Note that all screening was completed independently using the agreed-upon data abstraction criteria within covidence.org.
3. Results
A total of 4977 citations and 428 potentially relevant full-text papers were screened for inclusion in the rapid scoping review. Fifty studies fulfilled the eligibility criteria and were included in the rapid review (Figure 1: PRISMA). A total of 20 studies, primarily non-randomized experimental studies published between 2012 and 2021, were included in the final review (Table 1 Summary Characteristics (Comprehensive Table Revised)). Training program type/intervention (e.g., lecture, simulation, theatrical performance), program length (1 h to 15 weeks in duration), empathy assessment tools employed (e.g., Pre–post Jefferson Scale of Empathy, Jefferson Scale of Physician Empathy—Health Professionals Version, Empathetic Communication Skills Scale, Empathetic Tendency Scale, Kiersma–Chen Empathy Scale, etc.) and study design (i.e., randomized controlled trial, non-randomized quasi-experimental design, pre–post survey, and qualitative assessment) varied significantly across training programs and disciplines. Several standardized self-assessment tools (e.g., Kiersma–Chen Empathy Scale and Jefferson Scale of Empathy) and program-developed empathy assessments were used to assess student empathy pre- and post-training participation.
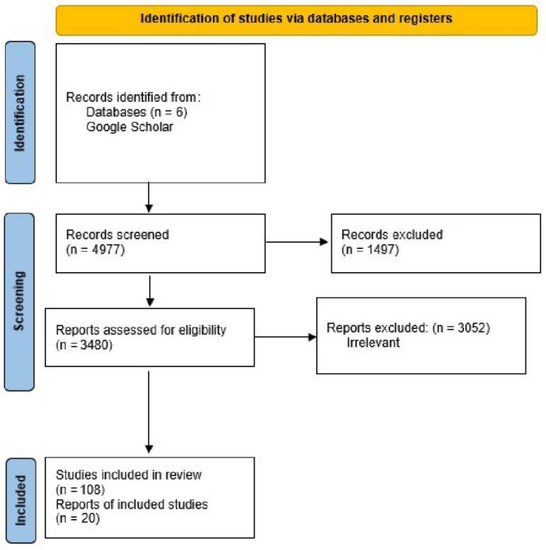
Figure 1.
PRISMA flow diagram illustrating the process of study selection for the systematic literature review.

Table 1.
Comprehensive results table.
Over 80 percent of the training took place in the classroom setting and utilized active learning strategies (e.g., case-based assessments and discussions, self-reflection activities, peer-assisted learning techniques, etc.). Less than 10% of the studies provided the training program detail necessary to replicate, utilize, and/or test the training program efficacy and impact on healthcare student empathy, irrespective of site and/or discipline. Models and theoretical frameworks for learning (e.g., behaviorism, cognitive, constructivism, etc.) were only referenced in 10% of the identified studies; however, most training interventions focused on cognitive and/or cognitive and behaviorism frameworks. Models and theoretical frameworks for communication (e.g., relationship-centered communication, motivational interviewing, self-efficacy, etc.) were explicitly described in less than 10% of studies; however, close to 90% of the training interventions provided information about the education intervention used to teach students how to better communicate with patients (e.g., role-play, simulations, group discussions, etc.). Simulation laboratories and community settings were used in 20 percent of the identified training to mimic clinical practice and patient–provider interactions.
Pharmacists and nurses were equally represented in the selected studies, with one selected trial including both pharmacy and nursing students (Table 2: Empathy Training in Pharmacy versus Nursing Students). Active learning strategies (e.g., case-based discussions, simulations, and self-reflection, etc.) of similar duration (1 h to 1 semester in duration) were used by both pharmacy and nursing programs; however, only one program within the pharmacy curriculum measured students for multiple years in the program. Both pharmacy and nursing programs utilized standardized and program-developed assessment metrics to assess student empathy, employing student self-assessment and trainer (professor or clinician) assessment of student empathy.
Table 2.
Empathy training in pharmacy versus nursing students.
Seventy percent of the included empathy training program assessments were conducted in the United States (U.S.); however, over 50% of the nursing program assessments were conducted outside of the US (e.g., Palestine, Iran, Turkey, Australia, and Spain) (Table 3: empathy training in US versus international nursing students). International study designs were similar to those conducted in the US (e.g., pre- and post-test design, etc.) and variable empathy education duration/dose (e.g., one-time simulation, empathy education integrated in curricula delivered over the course of four years).
Table 3.
Nursing student empathy training identified in countries across the globe.
4. Discussion
Our scoping review highlights the current state of empathy training in healthcare professional education and the need for more standardized approaches to training healthcare professionals in empathic care. One of the benefits of using empathy in healthcare is that it can help prevent medical paternalism, which is a problem in the healthcare system. Without appropriate training and opportunities to practice, healthcare worker behaviors can make patients feel devalued and contribute to negative emotional states, aggression, and violence toward caregivers and other patients [16,49,50]. We believe that addressing this issue through empathy training can lead to improved patient outcomes and increased provider trust.
Empathy training has been shown to reduce burnout and improve the ability of healthcare providers to care for challenging and often stigmatized populations (e.g., people who experience mental illness and those struggling with substance use disorders (MH/SUD)) [50,51,52,53,54]. However, there is little consensus on the most effective ways to train healthcare workers to provide empathic care and a wide range of instructional approaches are currently in use. Though a number of empathy training tools for healthcare students exist, it was difficult to assess the programs based on the information provided, including which tool was the most appropriate for students in specific healthcare disciplines, if the training addressed the unique needs of students providing care to individuals with mental health needs, and if the results were sustainable. There is an ongoing need to assess which educational strategies are most effective for which provider types and in which patient populations. This includes understanding which communication strategies have been most effective and best received by students and patients and assessing whether the effects of training erode over time or vary based on factors such as geography, community size, culture, or socioeconomic status.
4.1. Training Differences
In the scoping review, the authors found it difficult to assess the training programs based on the details provided. Empathy training varied significantly, from watching a one-hour video or participating in a brief three-dimensional simulation to extensive training structured into the curricula (semester-long training) [45]. Less than 10% of the studies provided the training program details required to replicate, utilize, and/or test the training program efficacy and impact of the training on healthcare student empathy, irrespective of site and/or discipline [45,47]. Models and theoretical frameworks for learning (e.g., behaviorism, cognitive, constructivism, etc.) were only referenced in 10% of the identified studies; however, the majority of training interventions focused on cognitive and/or cognitive and behaviorism [43]. In less than 10% of studies, models and theoretical frameworks for communication (e.g., relationship-centered communication, motivational interviewing, self-efficacy, etc.) were explicitly described; however, close to 90% of the training interventions provided information about the education intervention used to teach students how to better communicate with patients (e.g., role-play, simulations, group discussions, etc.), which allowed for some training program extrapolation [13,14,32,33,34,35,36,37,38,39,40,41,42,44,45,46,47,48].
Adults, in particular healthcare providers, can be taught to identify and empathically respond to a range of patient emotions (e.g., cognitive, emotional/behavioral, etc.) [4,5,7]. Cognitive empathy, understanding what another person might be feeling and thinking, allows the individual to take on their perspective in a situation. Emotional empathy, often referred to as clinical empathy, is the ability to share another person’s feelings, and focuses on understanding the patient’s feelings and using their experiences to skillfully adjust [9,10,23]. Though extrapolated in most of the identified studies, it appears that cognitive training methodologies, those most often employed in academia, were most commonly used to train pharmacy and nursing students in empathy, followed closely by emotional/behavioral frameworks [13,14,32,33,34,35,36,37,38,39,40,41,42,44,45,46,47,48]. Utilization of emotional/behavioral learning frameworks in empathy training program development may allow for improved understanding and subsequent adjustment of clinical care to better meet the needs of patients.
4.2. Differences between Training Based on Healthcare Student Type
Empathy is valued as a crucial component across all types of workplaces, from academic to corporate to the healthcare arena. Duration/intensity and training type varied significantly across nursing and pharmacy curricula, making it difficult to compare and assess the effectiveness of programs [13,13,14,16,32,33,34,35,36,38,39,41,42,43,45,46,48,55].
4.3. Differences between Training across Countries
Empathy education is delivered to health profession students occurs across the globe, although much of the published empathy education research was conducted in the United States. In this scoping review, six studies were conducted internationally, including in Palestine [32], Turkey [13,44], Australia [40], Spain [42], and Iran [43]. Simulation interventions evaluated were identified in countries across the globe [32,40], along with lectures [13,44] and workshops including role-playing, discussions, lectures, and scenarios [42,43]. There were no notable differences in the types of empathy interventions delivered internationally.
Again, the data collection tools used were identified in countries across the globe, e.g., the Kiersma–Chen Empathy Scale [32], Modified Kiersma–Chen Empathy Scale [40], Jefferson Scale of Empathy [42], and Jefferson Scale of Empathy for Health Professions Students [43]. Studies conducted in Turkey used tools that were unique to Turkey, such as the Empathic Communication Skill Scale and Empathic Tendency Scale [13,44].
Countries across the globe implemented similar study designs. For example, it was common to implement a pre–post-test design, and empathy education dose could be as short as a one-time simulation [40] as compared to empathy education integrated in curricula delivered over the course of four years [44]. All studies delivered education to nursing students and one study included nursing and medical students [13]. Findings were consistent across studies that empathy levels increased post-intervention; however, empathy appeared to erode over four years in the study that examined empathy education integrated in curricula [44].
One limitation of this scoping review is the variability in methodological quality and study design among the included studies. While efforts were made to assess the quality of each study using standardized tools, the use of primarily non-randomized experimental designs and the absence of consistent outcome measures make it difficult to draw firm conclusions about the effectiveness of different empathy training methods. In addition, while the review identified a trend towards utilizing active learning strategies in a classroom setting, there was little consensus on the specific training methods used across studies. Therefore, further research is needed to better understand the most effective approaches to training healthcare professional studies in empathic care and to develop standardized and validated methods for evaluating the effectiveness of empathy training.
5. Conclusions
Empathy training has been shown to improve the ability of healthcare providers to care for challenging and often stigmatized patients. However, there is little consensus on how to best train future healthcare providers to provide empathic care to patients and a number of questions remain. Models and theoretical frameworks for learning and communication (e.g., cognitive, behavioral/emotional, relationship-centered communication) and standardized assessment measures (e.g., Pre–post Jefferson Scale of Empathy, Jefferson Scale of Physician Empathy—Health Professionals Version, Empathetic Communication Skills Scale, Empathetic Tendency Scale, Kiersma–Chen Empathy Scale, etc.) need to be utilized in the development and testing of standardized empathy training programs across different healthcare students groups to better prepare our future healthcare providers.
Author Contributions
Conceptualization, R.R. and K.S.; methodology, R.R., K.M. and K.S.; formal analysis, R.R. and K.S.; resources, R.R; data curation, R.R., K.M., T.H. (Tracy Hellem), T.H. (Travis Hedwig), N.H., J.A., M.N. and K.S.; writing, R.R., K.M., T.H. (Tracy Hellem), T.H. (Travis Hedwig), M.N. and K.S.; writing—review and editing, R.R., K.M., T.H. (Tracy Hellem), T.H. (Travis Hedwig), N.H., J.A. and M.N.; supervision, R.R. and K.S.; project administration, R.R. and K.S. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Acknowledgments
Natalie Johansen for assistance with data collection.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Empathy: A Leader’s Greatest Skill|Bass Military Scholars|Vanderbilt University [Internet]. Available online: https://www.vanderbilt.edu/bass-military-scholars/2021/01/12/empathy-a-leaders-greatest-skill/ (accessed on 28 November 2022).
- Batson, C.D. These Things Called Empathy: Eight Related but Distinct Phenomena [Internet]. In The Social Neuroscience of Empathy; Decety, J., Ickes, W., Eds.; The MIT Press: Cambridge, MA, USA, 2009; pp. 3–16. Available online: http://mitpress.universitypressscholarship.com/view/10.7551/mitpress/9780262012973.001.0001/upso-9780262012973-chapter-2 (accessed on 1 February 2022).
- Jeffrey, D. Empathy, sympathy and compassion in healthcare: Is there a problem? Is there a difference? Does it matter? J. R. Soc. Med. 2016, 109, 446–452. [Google Scholar] [CrossRef] [PubMed]
- Moudatsou, M.; Stavropoulou, A.; Philalithis, A.; Koukouli, S. The Role of Empathy in Health and Social Care Professionals. Healthcare 2020, 8, 26. [Google Scholar] [CrossRef] [PubMed]
- Pehrson, C.; Banerjee, S.C.; Manna, R.; Shen, M.J.; Hammonds, S.; Coyle, N.; Krueger, C.A.; Maloney, E.; Zaider, T.; Bylund, C.L. Responding empathically to patients: Development, implementation, and evaluation of a communication skills training module for oncology nurses. Patient Educ. Couns. 2016, 99, 610–616. [Google Scholar] [CrossRef] [PubMed]
- Riess, H. The Science of Empathy. J. Patient Exp. 2017, 4, 74–77. [Google Scholar] [CrossRef]
- Riess, H.; Kelley, J.M.; Bailey, R.W.; Dunn, E.J.; Phillips, M. Empathy Training for Resident Physicians: A Randomized Controlled Trial of a Neuroscience-Informed Curriculum. J. Gen. Intern. Med. 2012, 27, 1280–1286. [Google Scholar] [CrossRef] [PubMed]
- Kelley, J.M.; Kraft-Todd, G.; Schapira, L.; Kossowsky, J.; Riess, H. The Influence of the Patient-Clinician Relationship on Healthcare Outcomes: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. PLoS ONE 2014, 9, e94207. [Google Scholar] [CrossRef] [PubMed]
- Anzaldua, A.; Halpern, J. Can Clinical Empathy Survive? Distress, Burnout, and Malignant Duty in the Age of COVID-19. Hastings Cent. Rep. 2021, 51, 22–27. [Google Scholar] [CrossRef] [PubMed]
- Halpern, J. What is clinical empathy? J. Gen. Intern. Med. 2003, 18, 670–674. [Google Scholar] [CrossRef]
- Bays, A.M.; Engelberg, R.A.; Back, A.L.; Ford, D.W.; Downey, L.; Shannon, S.E.; Doorenbos, A.Z.; Arnold, R.W.; Kross, E.K.; Reinke, L.F.; et al. Interprofessional Communication Skills Training for Serious Illness: Evaluation of a Small-Group, Simulated Patient Intervention. J. Palliat. Med. 2014, 17, 159–166. [Google Scholar] [CrossRef]
- Donnelly, S.; Dean, S.; Razavy, S.; Levett-Jones, T. Measuring the impact of an interdisciplinary learning project on nursing, architecture and landscape design students’ empathy. PLoS ONE 2019, 14, e0215795. [Google Scholar] [CrossRef]
- Ozcan, C.T.; Oflaz, F.; Bakir, B. The effect of a structured empathy course on the students of a medical and a nursing school: An empathy course on nursing and medical students. Int. Nurs. Rev. 2012, 59, 532–538. [Google Scholar] [CrossRef]
- Zelenski, A.B.; Saldivar, N.; Park, L.S.; Schoenleber, V.; Osman, F.; Kraemer, S. Interprofessional Improv: Using Theater Techniques to Teach Health Professions Students Empathy in Teams. Acad. Med. 2020, 95, 1210–1214. [Google Scholar] [CrossRef] [PubMed]
- Weaver, M.F.; Jarvis, M.A.E.; Schnoll, S.H. Role of the Primary Care Physician in Problems of Substance Abuse. Arch. Intern. Med. 1999, 159, 913. [Google Scholar] [CrossRef] [PubMed]
- Quinn, M.A.; Grant, L.M.; Sampene, E.; Zelenski, A.B. A Curriculum to Increase Empathy and Reduce Burnout. WMJ 2020, 119, 258–262. [Google Scholar]
- Birkhäuer, J.; Gaab, J.; Kossowsky, J.; Hasler, S.; Krummenacher, P.; Werner, C.; Gerger, H. Trust in the health care professional and health outcome: A meta-analysis. PLoS ONE 2017, 12, e0170988. [Google Scholar] [CrossRef]
- Hojat, M.; DeSantis, J.; Shannon, S.C.; Mortensen, L.H.; Speicher, M.R.; Bragan, L.; LaNoue, M.; Calabrese, L.H. The Jefferson Scale of Empathy: A nationwide study of measurement properties, underlying components, latent variable structure, and national norms in medical students. Adv. Health Sci. Educ. 2018, 23, 899–920. [Google Scholar] [CrossRef] [PubMed]
- Kane, G.C.; Gotto, J.L.; Mangione, S.; West, S.; Hojat, M. Jefferson Scale of Patient’s Perceptions of Physician Empathy: Preliminary psychometric data. Croat. Med. J. 2007, 48, 81–86. [Google Scholar]
- Hojat, M.; Louis, D.Z.; Markham, F.W.; Wender, R.; Rabinowitz, C.; Gonnella, J.S. Physicians’ Empathy and Clinical Outcomes for Diabetic Patients. Acad. Med. 2011, 86, 359–364. [Google Scholar] [CrossRef] [PubMed]
- McKenna, L.; Boyle, M.; Brown, T.; Williams, B.; Molloy, A.; Lewis, B.; Molloy, L. Levels of empathy in undergraduate nursing students: Empathy levels in nursing students. Int. J. Nurs. Pract. 2012, 18, 246–251. [Google Scholar] [CrossRef]
- Lawrence, S.A.; Cicale, C.; Wharton, T.; Chapple, R.; Stewart, C.; Burg, M.A. Empathy and attitudes about substance abuse among social work students, clinical social workers, & nurses. J. Soc. Work. Pract. Addict. 2022, 22, 40–52. [Google Scholar]
- Mirani, S.H.; Shaikh, N.A.; Tahir, A. Assessment of Clinical Empathy among Medical Students Using the Jefferson Scale of Empathy-Student Version. Cureus [Internet]. 2019. Available online: https://www.cureus.com/articles/18109-assessment-of-clinical-empathy-among-medical-students-using-the-jefferson-scale-of-empathy-student-version (accessed on 6 March 2022).
- Paulus, C.M.; Meinken, S. The effectiveness of empathy training in health care: A meta-analysis of training content and methods. Int. J. Med. Educ. 2022, 13, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Zaki, J. Moving beyond Stereotypes of Empathy. Trends Cogn. Sci. 2017, 21, 59–60. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.C.; Tan, S.R.; Tan, C.G.H.; Ng, M.S.P.; Lim, K.H.; Tan, L.H.E.; Ong, Y.T.; Cheong, C.W.S.; Chin, A.M.C.; Chiam, M.; et al. A systematic scoping review of approaches to teaching and assessing empathy in medicine. BMC Med. Educ. 2021, 21, 292. [Google Scholar] [CrossRef]
- Sucharew, H. Methods for Research Evidence Synthesis: The Scoping Review Approach. J. Hosp. Med. 2019, 14, 416. [Google Scholar] [CrossRef]
- Munn, Z.; Peters, M.D.J.; Stern, C.; Tufanaru, C.; McArthur, A.; Aromataris, E. Systematic review or scoping review? Guidance for authors when choosing between a systematic or scoping review approach. BMC Med. Res. Methodol. 2018, 18, 143. [Google Scholar] [CrossRef] [PubMed]
- Garritty, C.; Gartlehner, G.; Nussbaumer-Streit, B.; King, V.J.; Hamel, C.; Kamel, C.; Affengruber, L.; Stevens, A. Cochrane Rapid Reviews Methods Group offers evidence-informed guidance to conduct rapid reviews. J. Clin. Epidemiol. 2021, 130, 13–22. [Google Scholar] [CrossRef]
- Tricco, A.C.; Antony, J.; Zarin, W.; Strifler, L.; Ghassemi, M.; Ivory, J.; Perrier, L.; Hutton, B.; Moher, D.; Straus, S.E. A scoping review of rapid review methods. BMC Med. 2015, 13, 224. [Google Scholar] [CrossRef] [PubMed]
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef]
- Ayed, A.; Malak, M.Z.; Al-amer, R.M.; Batran, A.; Salameh, B. Effect of High-Fidelity Simulation on Perceptions of Self-Awareness, Empathy, and Patient-Centered Care among University Pediatric Nursing Classes. Clin. Simul. Nurs. 2021, 56, 84–90. [Google Scholar] [CrossRef]
- Chen, A.M.H.; Kiersma, M.E.; Yehle, K.S.; Plake, K.S. Impact of an Aging Simulation Game on Pharmacy Students’ Empathy for Older Adults. AJPE 2015, 79, 65. [Google Scholar] [CrossRef]
- Adams, S.B. Inspiring Empathy and Policy Action in Undergraduate Students: Monopoly as a Strategy. J. Nurs. Educ. 2019, 58, 298–301. [Google Scholar] [CrossRef] [PubMed]
- Miller, S.R. A curriculum focused on informed empathy improves attitudes toward persons with disabilities. Perspect. Med. Educ. 2013, 2, 114–125. [Google Scholar] [CrossRef] [PubMed]
- Ekong, G.; Kavookjian, J.; Hutchison, A. Predisposition for Empathy, Intercultural Sensitivity, and Intentions for Using Motivational Interviewing in First Year Pharmacy Students. AJPE 2017, 81, 5989. [Google Scholar] [CrossRef]
- Underwood, M.; Ronald, K. A pilot study assessing the impact of a polypharmacy mock medication simulation on student adherence and empathy. Curr. Pharm. Teach. Learn. 2020, 12, 956–962. [Google Scholar] [CrossRef] [PubMed]
- Van Winkle, L.J.; Fjortoft, N.; Hojat, M. Impact of a workshop about aging on the empathy scores of pharmacy and medical students. Am. J. Pharm. Educ. 2012, 76, 9. [Google Scholar] [CrossRef]
- Lor, K.B.; Truong, J.T.; Ip, E.J.; Barnett, M.J. A Randomized Prospective Study on Outcomes of an Empathy Intervention among Second-year Student Pharmacists. AJPE 2015, 79, 18. [Google Scholar] [CrossRef]
- Everson, N.; Levett-Jones, T.; Lapkin, S.; Pitt, V.; van der Riet, P.; Rossiter, R.; Jones, D.; Gilligan, C.; Courtney-Pratt, H. Measuring the impact of a 3D simulation experience on nursing students’ cultural empathy using a modified version of the Kiersma-Chen Empathy Scale. J. Clin. Nurs. 2015, 24, 2849–2858. [Google Scholar] [CrossRef]
- Isaacs, D.; Roberson, C.L.A.; Prasad-Reddy, L. A Chronic Disease State Simulation in an Ambulatory Care Elective Course. AJPE 2015, 79, 133. [Google Scholar] [CrossRef]
- Bas-Sarmiento, P.; Fernández-Gutiérrez, M.; Baena-Baños, M.; Romero-Sánchez, J.M. Efficacy of empathy training in nursing students: A quasi-experimental study. Nurse Educ. Today 2017, 59, 59–65. [Google Scholar] [CrossRef]
- Gholamzadeh, S.; Khastavaneh, M.; Khademian, Z.; Ghadakpour, S. The effects of empathy skills training on nursing students’ empathy and attitudes toward elderly people. BMC Med. Educ. 2018, 18, 198. [Google Scholar] [CrossRef]
- Ozcan, C.T.; Öksüz, E.; Oflaz, F. Improving Empathy in Nursing Students: A Comparative Longitudinal Study of Two Curricula. J. Korean Acad. Nurs. 2018, 48, 497. [Google Scholar] [CrossRef]
- Parker, D.; Fontem, A.; Ojong, E.; Pope, J. Impact of Diabetes Simulation on Empathy in Pharmacy Students. AJPE 2019, 83, 6432. [Google Scholar] [CrossRef] [PubMed]
- Preston, K.B.; Jean-Louis, K. A Community Service Organization Focused on the Arts to Develop Empathy in Pharmacy Students. AJPE 2020, 84, 7723. [Google Scholar] [CrossRef] [PubMed]
- Nebergall, S.; Dula, C.A.C.; King, S.A.; Matthews, D.E.; Haas-Gehres, A.; Li, J. Educating Pharmacy Students about Underserved Populations Using Patient Speakers and Simulation Activities. AJPE 2021, 85, 8461. [Google Scholar] [CrossRef] [PubMed]
- Clemens, E.J.; Reed, J.B.; Baker, E.S.; Baker, C.M. Effect of death and dying elective on student empathy and attitudes toward mortality. Curr. Pharm. Teach. Learn. 2021, 13, 1627–1633. [Google Scholar] [CrossRef]
- Janzen, S.; Arnetz, J.; Radcliffe, S.; Fitzpatrick, L.; Eden, J.; Wright, M.C. Preventing patient violence in hospitals: Applying critical decision method interviews to understand how skilled staff think and act differently. Appl. Nurs. Res. 2022, 63, 151544. [Google Scholar] [CrossRef] [PubMed]
- Brondani, M.A.; Alan, R.; Donnelly, L. Stigma of addiction and mental illness in healthcare: The case of patients’ experiences in dental settings. PLoS ONE 2017, 12, e0177388. [Google Scholar] [CrossRef] [PubMed]
- Subu, M.A.; Wati, D.F.; Netrida, N.; Priscilla, V.; Dias, J.M.; Abraham, M.S.; Slewa-Younan, S.; Al-Yateem, N. Types of stigma experienced by patients with mental illness and mental health nurses in Indonesia: A qualitative content analysis. Int. J. Ment. Health Syst. 2021, 15, 77. [Google Scholar] [CrossRef]
- Henderson, C.; Evans-Lacko, S.; Thornicroft, G. Mental illness stigma, help seeking, and public health programs. Am. J. Public Health 2013, 103, 777–780. [Google Scholar] [CrossRef]
- Clement, S.; Schauman, O.; Graham, T.; Maggioni, F.; Evans-Lacko, S.; Bezborodovs, N.; Morgan, C.; Rüsch, N.; Brown, J.S.L.; Thornicroft, G. What is the impact of mental health-related stigma on help-seeking? A systematic review of quantitative and qualitative studies. Psychol. Med. 2015, 45, 11–27. [Google Scholar] [CrossRef] [PubMed]
- Rao, H.; Mahadevappa, H.; Pillay, P.; Sessay, M.; Abraham, A.; Luty, J. A study of stigmatized attitudes towards people with mental health problems among health professionals. J. Psychiatr. Ment. Health Nurs. 2009, 16, 279–284. [Google Scholar] [CrossRef] [PubMed]
- Chen, A.; Hanna, J.J.; Manohar, A.; Tobia, A. Teaching Empathy: The Implementation of a Video Game into a Psychiatry Clerkship Curriculum. Acad. Psychiatry 2018, 42, 362–365. [Google Scholar] [CrossRef] [PubMed]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).