
Immediate Effects of Foam Roller and Stretching to the Lead Hip on Golfers Swing: A Randomized Crossover Trial

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
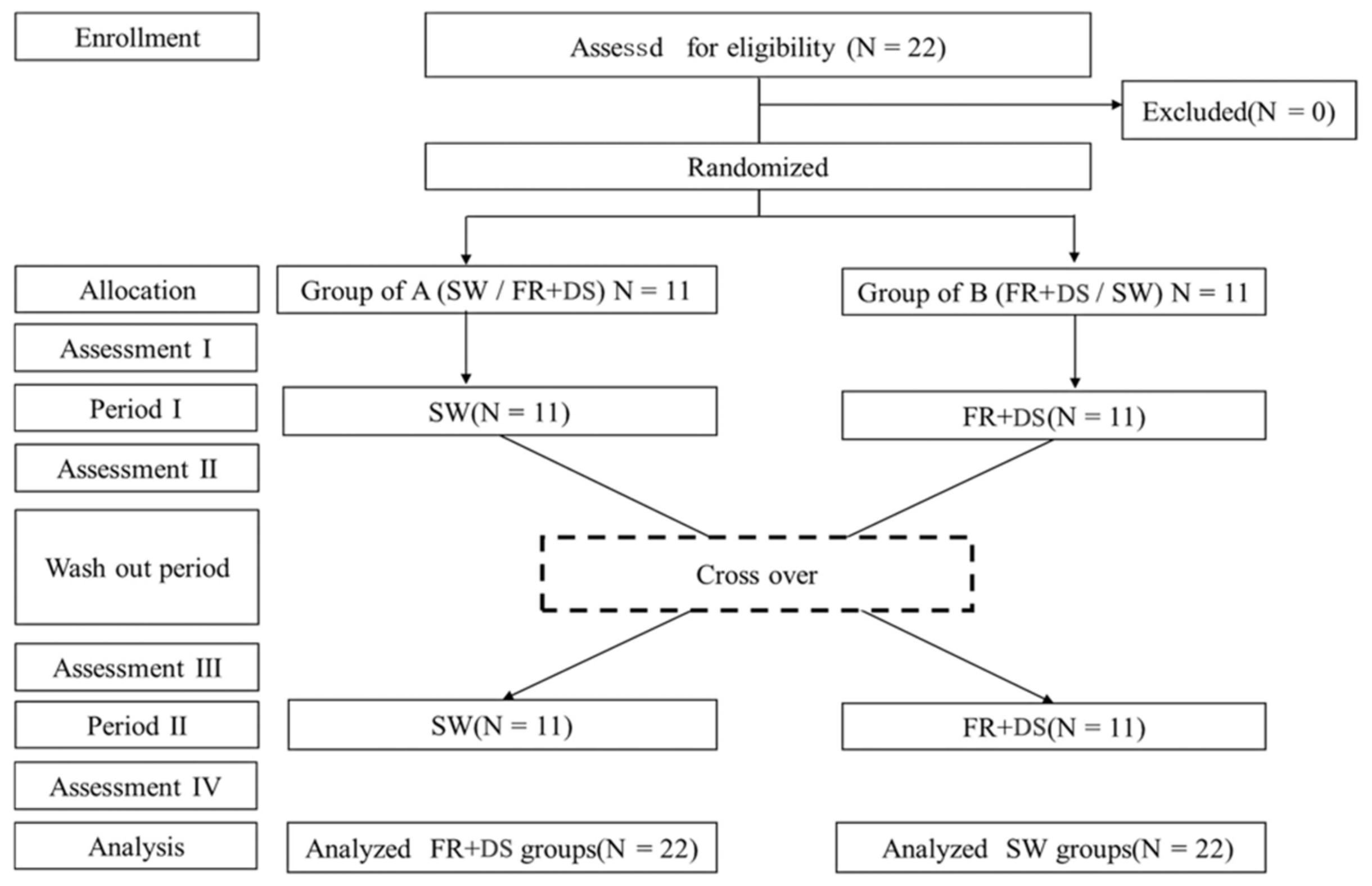
2.1. Study Design and Ethical Considerations
2.2. Participants
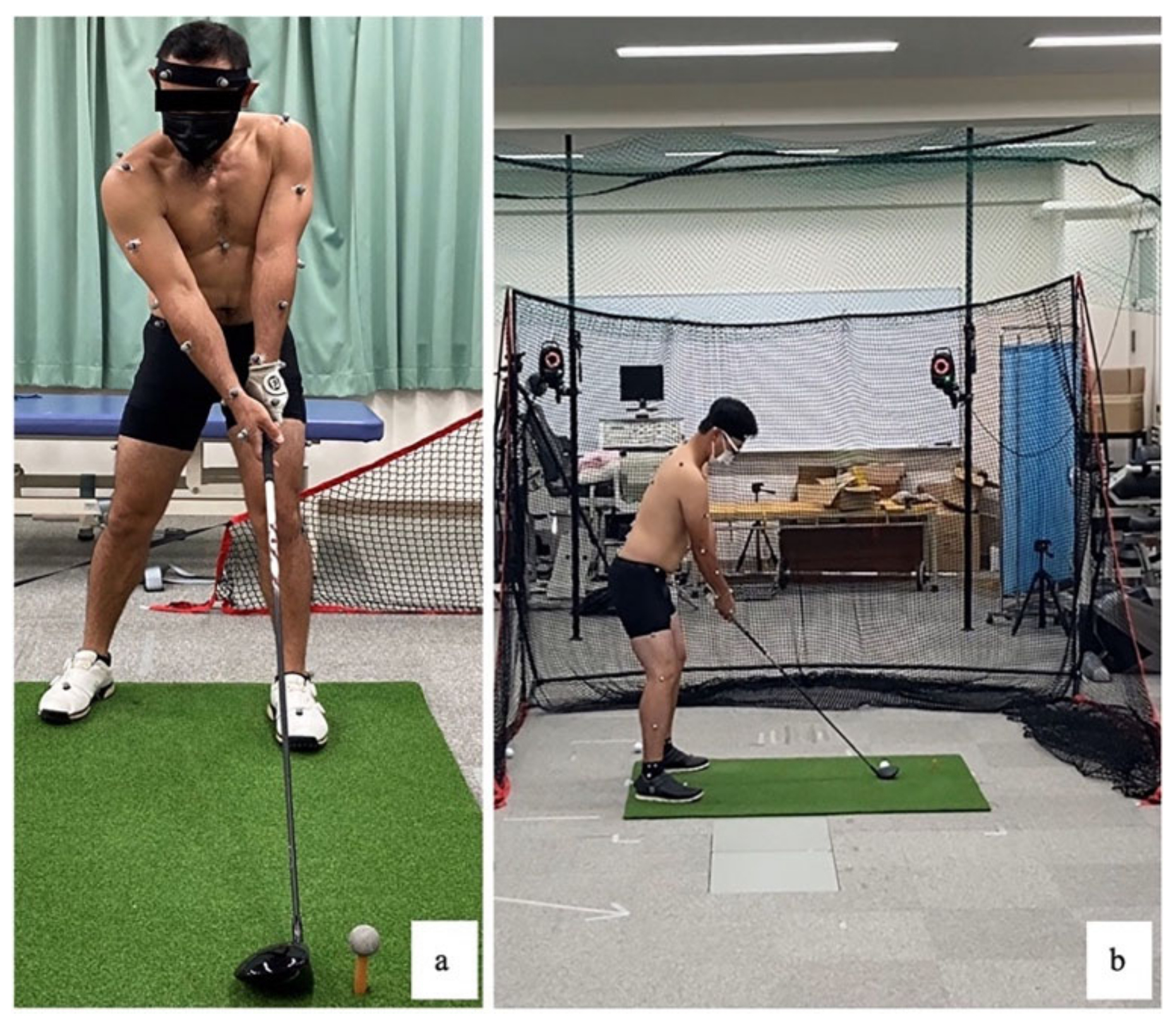
2.3. Motion Analysis as Primary Outcome
2.4. Clinical Test as Secondary Outcomes
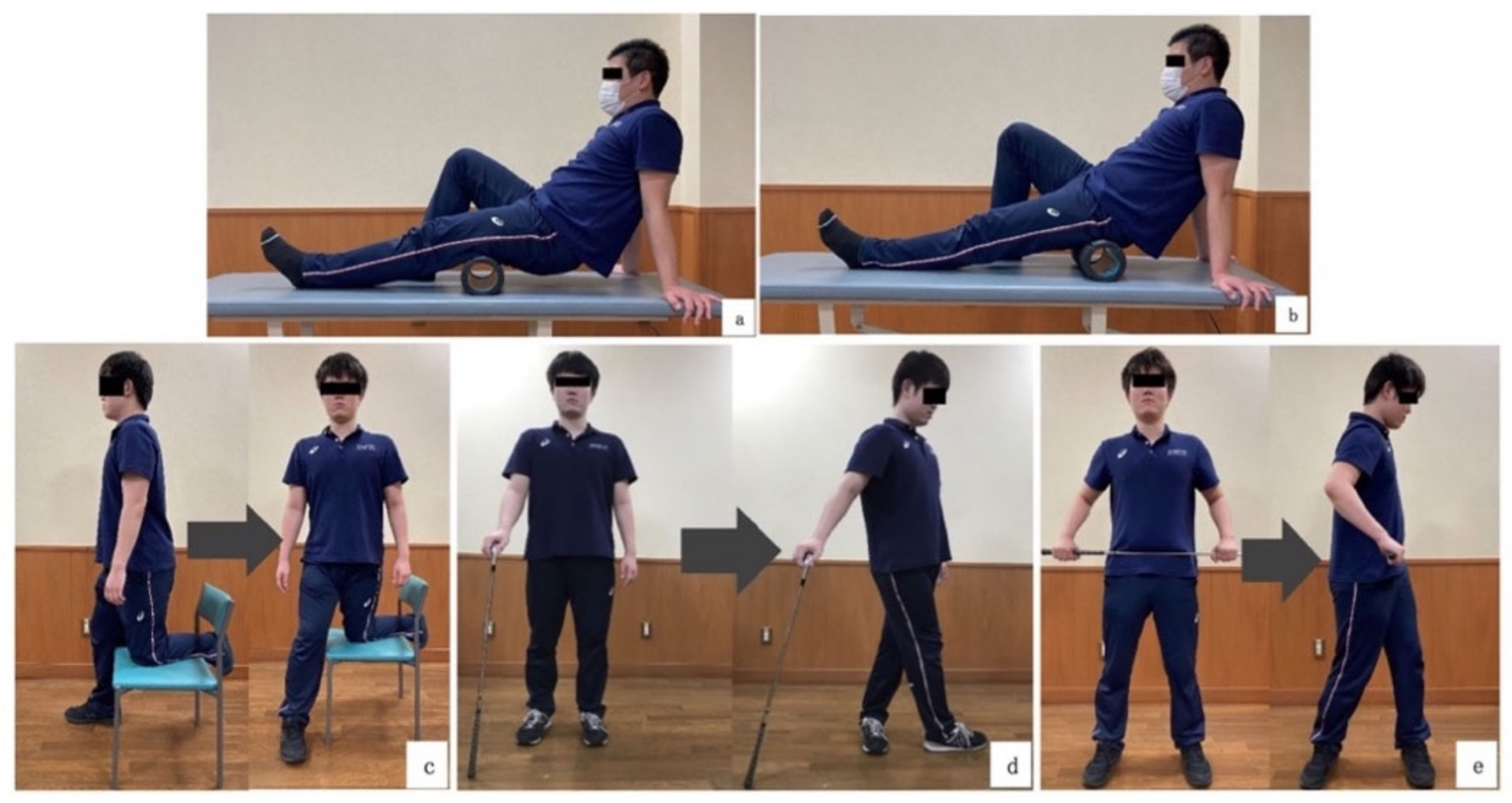
2.5. Intervention Program
2.6. Sample Size
2.7. Data Processing
3. Results
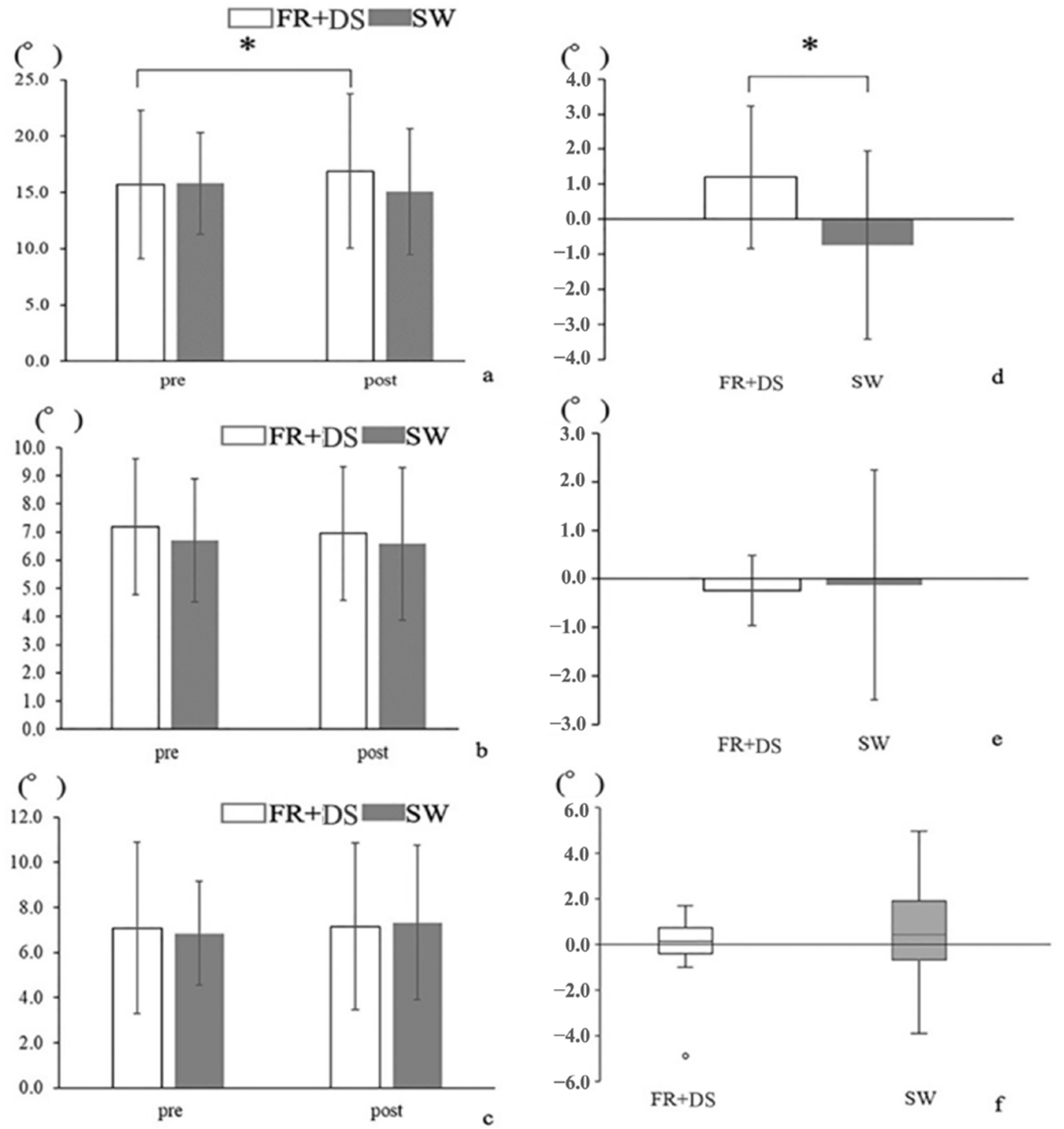
3.1. Differences in Hip and Lumbar Spine ROM before and after Intervention
3.2. Correlation between Lead Hip IR Angle and Lower Lumbar Lrot Angle Changes during the Golf Swing
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gosheger, G.; Liem, D.; Ludwig, K.; Greshake, O.; Winkelmann, W. Injuries and Overuse Syndromes in Golf. Am. J. Sports Med. 2003, 31, 438–443. [Google Scholar] [CrossRef] [PubMed]
- Sahrmann, S.; Azevedo, D.C.; Dillen, L. Van Diagnosis and Treatment of Movement System Impairment Syndromes. Braz. J. Phys. Ther. 2017, 21, 391–399. [Google Scholar] [CrossRef]
- Adams, M.A. Biomechanics of Back Pain. Acupunct. Med. J. Br. Med. Acupunct. Soc. 2004, 22, 178–188. [Google Scholar] [CrossRef] [PubMed]
- Neumann, D.A. Kinesiology of the Musculoskeletal System; Mosby: St. Louis, MO, USA, 2009. [Google Scholar]
- Hosea, T.M.; Gatt, C.J.; Galli, K.M.; Langrana, N.A.; Zawadsky, J.P. Biochemical Analysis of the Golfer’s Back. In Science and Golf; Chapman and Hall: London, UK, 1990; pp. 43–48. [Google Scholar]
- Lindsay, D.; Horton, J. Comparison of Spine Motion in Elite Golfers with and without Low Back Pain. J. Sports Sci. 2002, 20, 599–605. [Google Scholar] [CrossRef]
- Hashimoto, K.; Miyamoto, K.; Yanagawa, T.; Hattori, R.; Aoki, T.; Matsuoka, T.; Ohno, T.; Shimizu, K. Lumbar Corsets Can Decrease Lumbar Motion in Golf Swing. J. Sports Sci. Med. 2013, 12, 80–87. [Google Scholar] [PubMed]
- Lejkowski, P.M.; Poulsen, E. Elimination of Intermittent Chronic Low Back Pain in a Recreational Golfer Following Improvement of Hip Range of Motion Impairments. J. Bodyw. Mov. Ther. 2013, 17, 448–452. [Google Scholar] [CrossRef]
- Reinhardt, G. The Role of Decreased Hip IR as a Cause of Low Back Pain in a Golfer: A Case Report. HSS J. 2013, 9, 278–283. [Google Scholar] [CrossRef] [Green Version]
- Kim, S.-B.; You, J.S.H.; Kwon, O.-Y.; Yi, C.-H. Lumbopelvic Kinematic Characteristics of Golfers with Limited Hip Rotation. Am. J. Sports Med. 2015, 43, 113–120. [Google Scholar] [CrossRef]
- Murray, E.; Birley, E.; Twycross-Lewis, R.; Morrissey, D. The Relationship between Hip Rotation Range of Movement and Low Back Pain Prevalence in Amateur Golfers: An Observational Study. Phys. Ther. Sport 2009, 10, 131–135. [Google Scholar] [CrossRef]
- Vad, V.B.; Bhat, A.L.; Basrai, D.; Gebeh, A.; Aspergren, D.D.; Andrews, J.R. Low Back Pain in Professional Golfers. Am. J. Sports Med. 2004, 32, 494–497. [Google Scholar] [CrossRef]
- Van Dillen, L.R.; Bloom, N.J.; Gombatto, S.P.; Susco, T.M. Hip Rotation Range of Motion in People with and without Low Back Pain Who Participate in Rotation-Related Sports. Phys. Ther. Sport 2008, 9, 72–81. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Behm, D.G.; Chaouachi, A. A Review of the Acute Effects of Static and Dynamic Stretching on Performance. Eur. J. Appl. Physiol. 2011, 111, 2633–2651. [Google Scholar] [CrossRef] [PubMed]
- Opplert, J.; Babault, N. Acute Effects of Dynamic Stretching on Muscle Flexibility and Performance: An Analysis of the Current Literature. Sports Med. 2018, 48, 299–325. [Google Scholar] [CrossRef]
- Gergley, J.C. Acute Effects of Passive Static Stretching during Warm-up on Driver Clubhead Speed, Distance, Accuracy, and Consistent Ball Contact in Young Male Competitive Golfers. J. Strength Cond. Res. 2009, 23, 863–867. [Google Scholar] [CrossRef] [PubMed]
- Skinner, B.; Moss, R.; Hammond, L. A Systematic Review and Meta-Analysis of the Effects of Foam Rolling on Range of Motion, Recovery and Markers of Athletic Performance. J. Bodyw. Mov. Ther. 2020, 24, 105–122. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, M.; Sato, S.; Kiyono, R.; Yoshida, R.; Murakami, Y.; Yasaka, K.; Yahata, K.; Konrad, A. Acute Effect of Vibration Roller With and Without Rolling on Various Parts of the Plantar Flexor Muscle. Front. Physiol. 2021, 12, 716668. [Google Scholar] [CrossRef]
- Alonso-Calvete, A.; Padrón-Cabo, A.; Lorenzo-Martínez, M.; Rey, E. Acute Effects of Foam Rolling on Blood Flow Measured by Ultrasonography in Soccer Players. J. Strength Cond. Res. 2021, 35, 3256–3259. [Google Scholar] [CrossRef]
- Schroeder, J.; Wilke, J.; Hollander, K. Effects of Foam Rolling Duration on Tissue Stiffness and Perfusion: A Randomized Cross-Over Trial. J. Sports Sci. Med. 2021, 20, 626–634. [Google Scholar] [CrossRef]
- Behara, B.; Jacobson, B.H. Acute Effects of Deep Tissue Foam Rolling and Dynamic Stretching on Muscular Strength, Power, and Flexibility in Division I Linemen. J. Strength Cond. Res. 2017, 31, 888–892. [Google Scholar] [CrossRef]
- Cheatham, S.W.; Stull, K.R.; Batts, W.N.; Ambler-Wright, T. Roller Massage: Comparing the Immediate Post-Treatment Effects Between an Instructional Video and a Self-Preferred Program Using Two Different Density-Type Roller Balls. J. Hum. Kinet. 2020, 71, 119–129. [Google Scholar] [CrossRef] [Green Version]
- Han, S.; Lee, Y.; Lee, D. The Influence of the Vibration Form Roller Exercise on the Pains in the Muscles around the Hip Joint and the Joint Performance. J. Phys. Ther. Sci. 2017, 29, 1844–1847. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adamczyk, J.G.; Gryko, K.; Boguszewski, D. Does the Type of Foam Roller Influence the Recovery Rate, Thermal Response and DOMS Prevention? PLoS ONE 2020, 15, e0235195. [Google Scholar] [CrossRef] [PubMed]
- Lin, W.-C.; Lee, C.-L.; Chang, N.-J. Acute Effects of Dynamic Stretching Followed by Vibration Foam Rolling on Sports Performance of Badminton Athletes. J. Sports Sci. Med. 2020, 19, 420–428. [Google Scholar] [PubMed]
- Hasebe, K.; Okubo, Y.; Kaneoka, K.; Takada, K.; Suzuki, D.; Sairyo, K. The Effect of Dynamic Stretching on Hamstrings Flexibility with Respect to the Spino-Pelvic Rhythm. J. Med. Investig. 2016, 63, 85–90. [Google Scholar] [CrossRef] [Green Version]
- Kang, M.-H.; Jung, D.-H.; An, D.-H.; Yoo, W.-G.; Oh, J.-S. Acute Effects of Hamstring-Stretching Exercises on the Kinematics of the Lumbar Spine and Hip during Stoop Lifting. J. Back Musculoskelet. Rehabil. 2013, 26, 329–336. [Google Scholar] [CrossRef]
- Tamura, A.; Akasaka, K.; Otsudo, T.; Sawada, Y.; Okubo, Y.; Shiozawa, J.; Toda, Y.; Yamada, K. Fatigue Alters Landing Shock Attenuation During a Single-Leg Vertical Drop Jump. Orthop. J. Sports Med. 2016, 4, 2325967115626412. [Google Scholar] [CrossRef]
- Gombatto, S.P.; Brock, T.; DeLork, A.; Jones, G.; Madden, E.; Rinere, C. Lumbar Spine Kinematics during Walking in People with and People without Low Back Pain. Gait Posture 2015, 42, 539–544. [Google Scholar] [CrossRef]
- Horan, S.A.; Evans, K.; Morris, N.R.; Kavanagh, J.J. Thorax and Pelvis Kinematics during the Downswing of Male and Female Skilled Golfers. J. Biomech. 2010, 43, 1456–1462. [Google Scholar] [CrossRef]
- Moran, K.; McGrath, T.; Marshall, B.; Wallace, E. Dynamic Stretching and Golf Swing Performance. Int. J. Sports Med. 2009, 30, 113–118. [Google Scholar] [CrossRef]
- Mitchell, K.; Banks, S.; Morgan, D.; Sugaya, H. Shoulder Motions During the Golf Swing in Male Amateur Golfers. J. Orthop. Sport. Phys. Ther. 2003, 33, 196–203. [Google Scholar] [CrossRef] [Green Version]
- De Souza, A.; Sanchotene, C.G.; da Silva Lopes, C.M.; Beck, J.A.; da Silva, A.C.K.; Pereira, S.M.; Ruschel, C. Acute Effect of 2 Self-Myofascial Release Protocols on Hip and Ankle Range of Motion. J. Sport Rehabil. 2019, 28, 159–164. [Google Scholar] [CrossRef] [PubMed]
- Henry, E.; Berglund, K.; Millar, L.; Locke, F. Immediate Effects of a Dynamic Rotation-Specific Warm-Up on X-Factor and X-Factor Stretch in the Amateur Golfer. Int. J. Sports Phys. Ther. 2015, 10, 998–1006. [Google Scholar] [PubMed]
- Hing, W.; Hall, T.; Rivett, D.; Vicenzino, B.; Mulligan, B. The Mulligan Concept of Manual Therapy; Elsevier: Sydney, NSW, Australia, 2015. [Google Scholar]
- Paradisis, G.P.; Pappas, P.T.; Theodorou, A.S.; Zacharogiannis, E.G.; Skordilis, E.K.; Smirniotou, A.S. Effects of Static and Dynamic Stretching on Sprint and Jump Performance in Boys and Girls. J. Strength Cond. Res. 2014, 28, 154–160. [Google Scholar] [CrossRef] [PubMed]
- Gergley, J.C. Latent Effect of Passive Static Stretching on Driver Clubhead Speed, Distance, Accuracy, and Consistent Ball Contact in Young Male Competitive Golfers. J. Strength Cond. Res. 2010, 24, 3326–3333. [Google Scholar] [CrossRef] [Green Version]
- Watt, J.R.; Jackson, K.; Franz, J.R.; Dicharry, J.; Evans, J.; Kerrigan, D.C. Effect of a Supervised Hip Flexor Stretching Program on Gait in Frail Elderly Patients. PM&R 2011, 3, 330–335. [Google Scholar] [CrossRef]
- Amiri-Khorasani, M.; Abu Osman, N.A.; Yusof, A. Acute Effect of Static and Dynamic Stretching on Hip Dynamic Range of Motion during Instep Kicking in Professional Soccer Players. J. Strength Cond. Res. 2011, 25, 1647–1652. [Google Scholar] [CrossRef]
- Iwata, M.; Yamamoto, A.; Matsuo, S.; Hatano, G.; Miyazaki, M.; Fukaya, T.; Fujiwara, M.; Asai, Y.; Suzuki, S. Dynamic Stretching Has Sustained Effects on Range of Motion and Passive Stiffness of the Hamstring Muscles. J. Sports Sci. Med. 2019, 18, 13–20. [Google Scholar]
- Diniz, K.M.A.; Resende, R.A.; de Oliveira Mascarenhas, R.; de Jesus Silva, H.; Filho, R.G.T.; Mendonça, L.D.M. Hip Passive Stiffness Is Associated with Hip Kinematics during Single-Leg Squat. J. Bodyw. Mov. Ther. 2021, 28, 68–74. [Google Scholar] [CrossRef]
- Peacock, C.A.; Krein, D.D.; Silver, T.A.; Sanders, G.J.; VON Carlowitz, K.-P.A. An Acute Bout of Self-Myofascial Release in the Form of Foam Rolling Improves Performance Testing. Int. J. Exerc. Sci. 2014, 7, 202–211. [Google Scholar]
- Mettler, J.H.; Shapiro, R.; Pohl, M.B. Effects of a Hip Flexor Stretching Program on Running Kinematics in Individuals With Limited Passive Hip Extension. J. Strength Cond. Res. 2019, 33, 3338–3344. [Google Scholar] [CrossRef] [Green Version]
- Foxworth, J.L.; Millar, A.L.; Long, B.L.; Way, M.; Vellucci, M.W.; Vogler, J.D. Hip Joint Torques During the Golf Swing of Young and Senior Healthy Males. J. Orthop. Sport. Phys. Ther. 2013, 43, 660–665. [Google Scholar] [CrossRef] [PubMed]
- Mun, F.; Suh, S.W.; Park, H.-J.; Choi, A. Kinematic Relationship between Rotation of Lumbar Spine and Hip Joints during Golf Swing in Professional Golfers. Biomed. Eng. Online 2015, 14, 41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Škarabot, J.; Beardsley, C.; Štirn, I. Comparing the Effects of Self-Myofascial Release with Static Stretching on Ankle Range-of-Motion in Adolescent Athletes. Int. J. Sports Phys. Ther. 2015, 10, 203–212. [Google Scholar] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| FR + DS Pre | SW Pre | p-Value | 95% CI | FR + DS Post | SW Post | p-Value | 95% CI | |||
|---|---|---|---|---|---|---|---|---|---|---|
| IR ROM | ||||||||||
| Lead hip passive | 28.7 ± 9.02 | 28.2 ± 9.04 | 1.000 | −0.38 | 1.23 | 35.4 ± 9.74 | 29.5 ± 7.90 | <0.000 * | 4.62 | 7.25 |
| Trail hip passive | 26.8 ± 7.66 | 27.2 ± 8.08 | 1.000 | −1.54 | 0.74 | 28.2 ± 7.49 | 27.6 ± 7.58 | 0.384 | −0.11 | 1.29 |
| Lead hip active | 27.4 ± 8.10 | 27.7 ± 8.31 | 1.000 | −1.25 | 0.54 | 34.4 ± 8.93 | 28.6 ± 7.35 | <0.000 * | 4.30 | 7.18 |
| Trail hip active | 26.8 ± 7.57 | 26.6 ± 7.51 | 1.000 | −1.32 | 1.88 | 28.2 ± 7.15 | 27.1 ± 7.34 | 0.276 | −0.09 | 2.17 |
| ER ROM | ||||||||||
| Lead hip passive | 27.8 ± 5.68 | 27.9 ± 4.95 | 1.000 | −1.42 | 1.30 | 27.3 ± 5.40 | 27.5 ± 4.05 | 1.000 | −1.62 | 1.10 |
| Trail hip passive | 29.1 ± 5.95 | 28.6 ± 5.26 | 1.000 | −0.62 | 1.53 | 28.9 ± 5.12 | 28.9 ± 5.18 | 1.000 | −1.79 | 1.68 |
| Lead hip active | 26.8 ± 6.33 | 28.2 ± 4.94 | 0.068 | −2.35 | −0.26 | 27.3 ± 5.12 | 28.3 ± 4.72 | 0.280 | −2.09 | 0.09 |
| Trail hip active | 28.5 ± 5.78 | 28.8 ± 4.79 | 1.000 | −1.41 | 0.95 | 29.0 ± 4.83 | 29.3 ± 5.27 | 1.000 | −1.76 | 1.10 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hamada, Y.; Akasaka, K.; Otsudo, T.; Sawada, Y.; Hattori, H.; Hasebe, Y.; Kikuchi, Y.; Hall, T. Immediate Effects of Foam Roller and Stretching to the Lead Hip on Golfers Swing: A Randomized Crossover Trial. Healthcare 2023, 11, 2001. https://doi.org/10.3390/healthcare11142001
Hamada Y, Akasaka K, Otsudo T, Sawada Y, Hattori H, Hasebe Y, Kikuchi Y, Hall T. Immediate Effects of Foam Roller and Stretching to the Lead Hip on Golfers Swing: A Randomized Crossover Trial. Healthcare. 2023; 11(14):2001. https://doi.org/10.3390/healthcare11142001
Chicago/Turabian StyleHamada, Yuji, Kiyokazu Akasaka, Takahiro Otsudo, Yutaka Sawada, Hiroshi Hattori, Yuki Hasebe, Yuto Kikuchi, and Toby Hall. 2023. "Immediate Effects of Foam Roller and Stretching to the Lead Hip on Golfers Swing: A Randomized Crossover Trial" Healthcare 11, no. 14: 2001. https://doi.org/10.3390/healthcare11142001