
Trust Is for the Strong: How Health Status May Influence Generalized and Personalized Trust

 , ,
, ,  ,
, 
Abstract
:1. Introduction
1.1. The Current Landscape of Human Trust Research
1.2. Hints from Observations in Nature on the Health-to-Trust Direction
1.3. An Information-Processing Approach for Examining the Trust–Health Relationship
2. Methodology
2.1. Theoretical Foundation
2.1.1. Mindsponge Theory Overview and the Information Multi-Filtering System
- It depicts the fundamental patterns of the biosphere system.
- The procedure is one that is both dynamic and balanced.
- It uses a cost-benefit analysis and aims to maximize perceived benefits while minimizing perceived costs for the overall system.
- Because it uses energy, it follows the principle of energy conservation.
- It adheres to objectives and priorities based on the needs of the system.
- Its major function is to sustain the continued existence of the system, as manifested by survival, growth, and reproduction.
2.1.2. The Trust Mechanism in the Mindsponge Framework
2.2. Model Construction
2.2.1. Materials and Variable Selection
2.2.2. Model Formulation
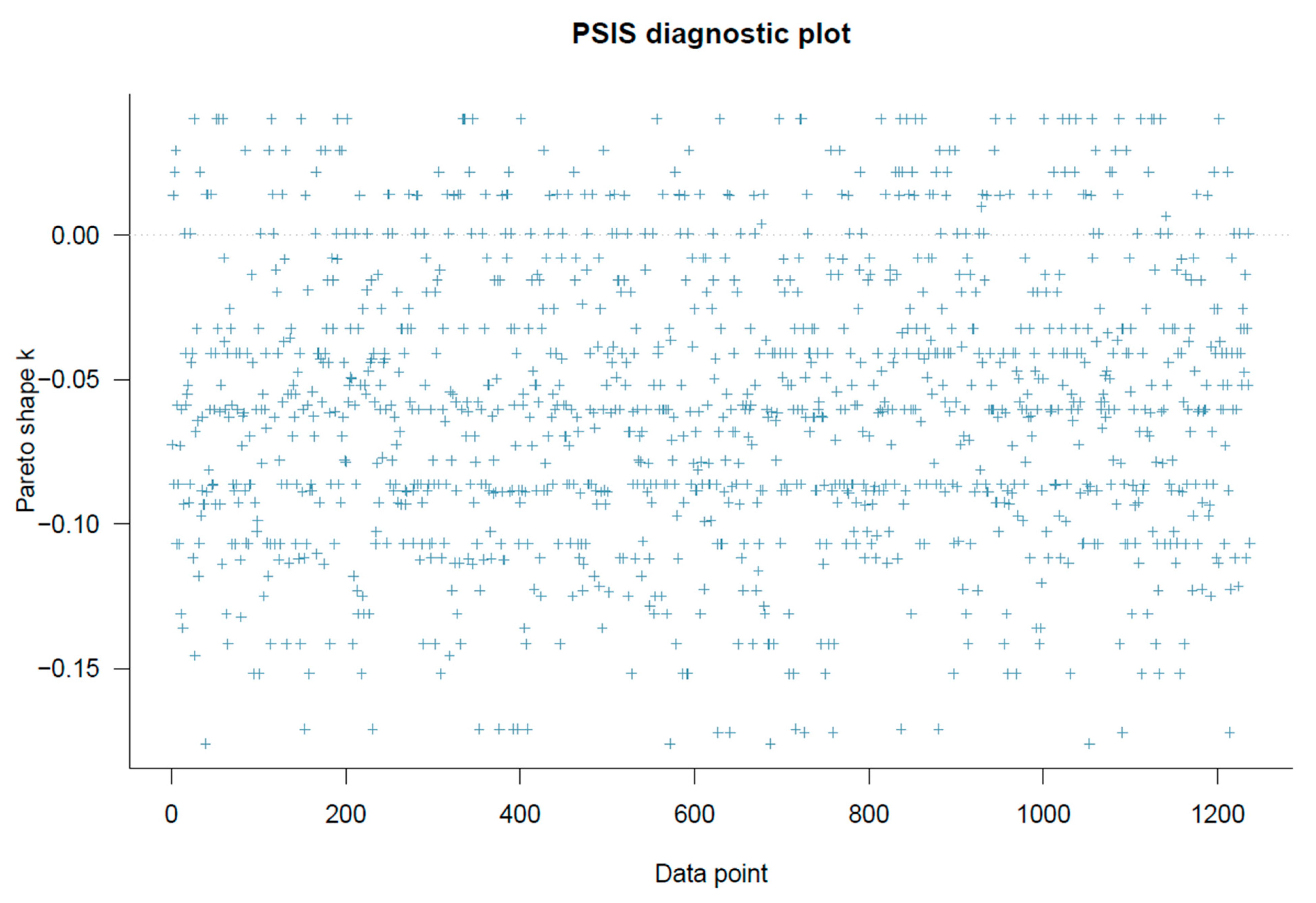
2.3. Analysis and Validation
3. Results
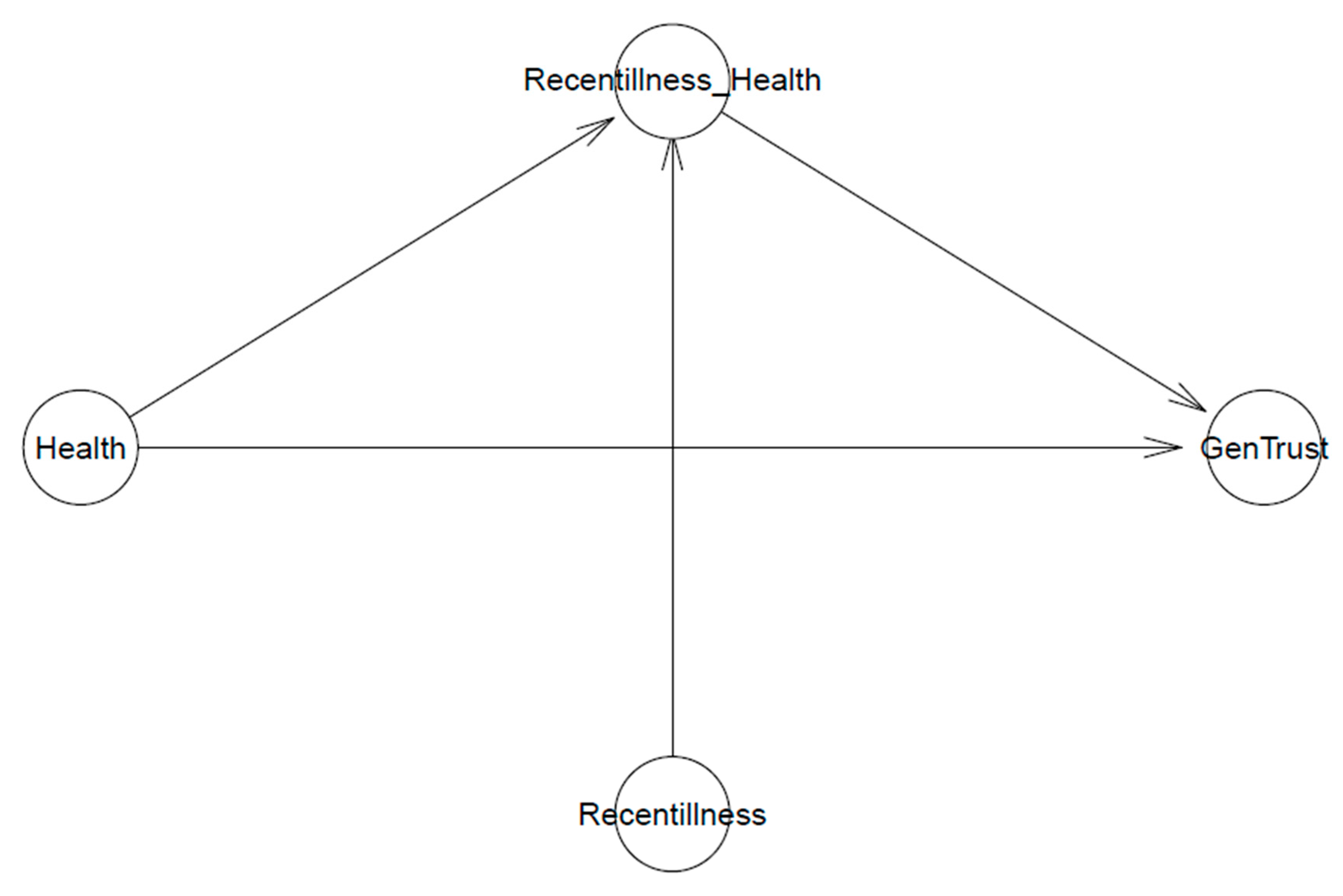
3.1. Model 1: Generalized Trust
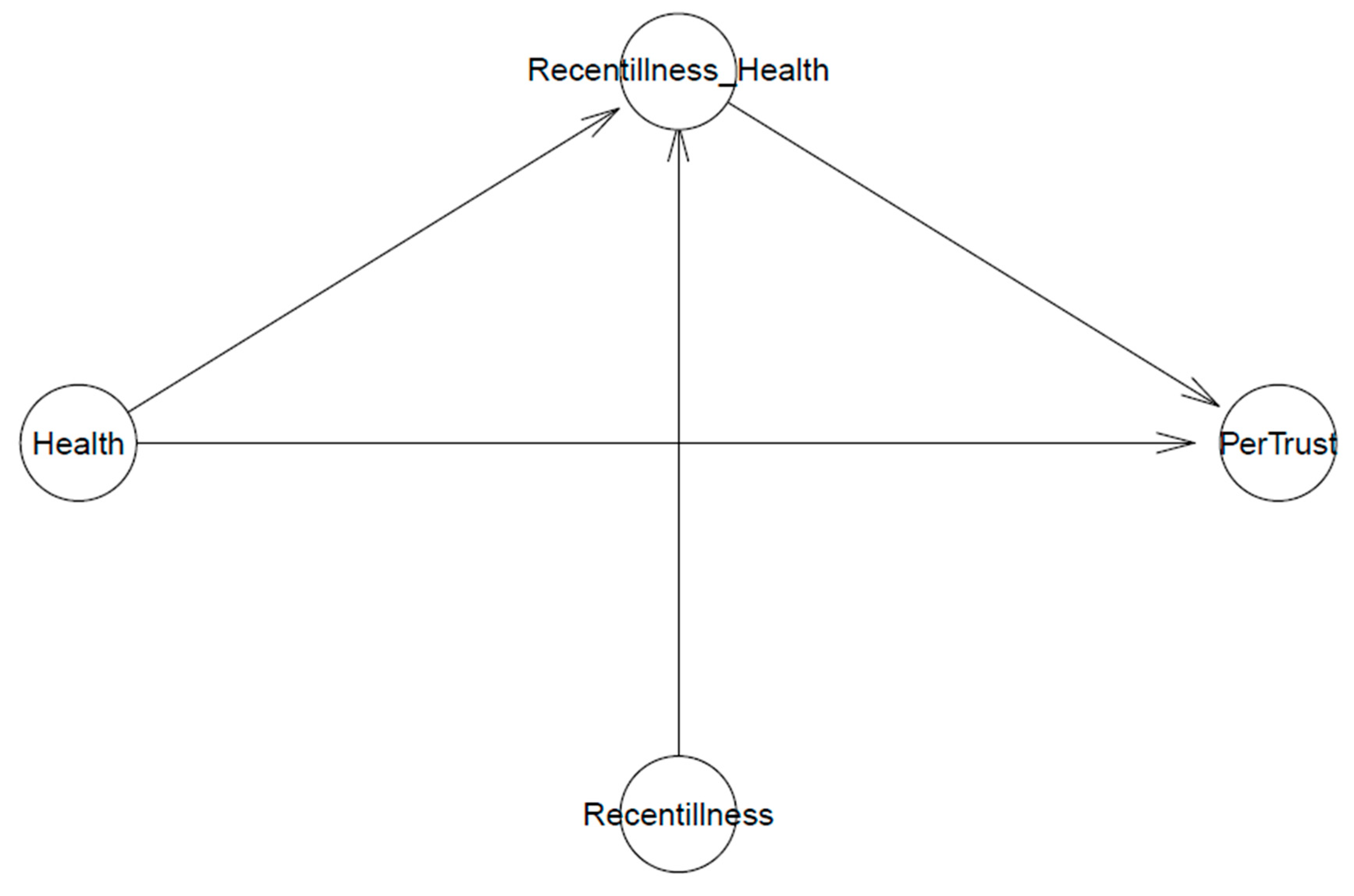
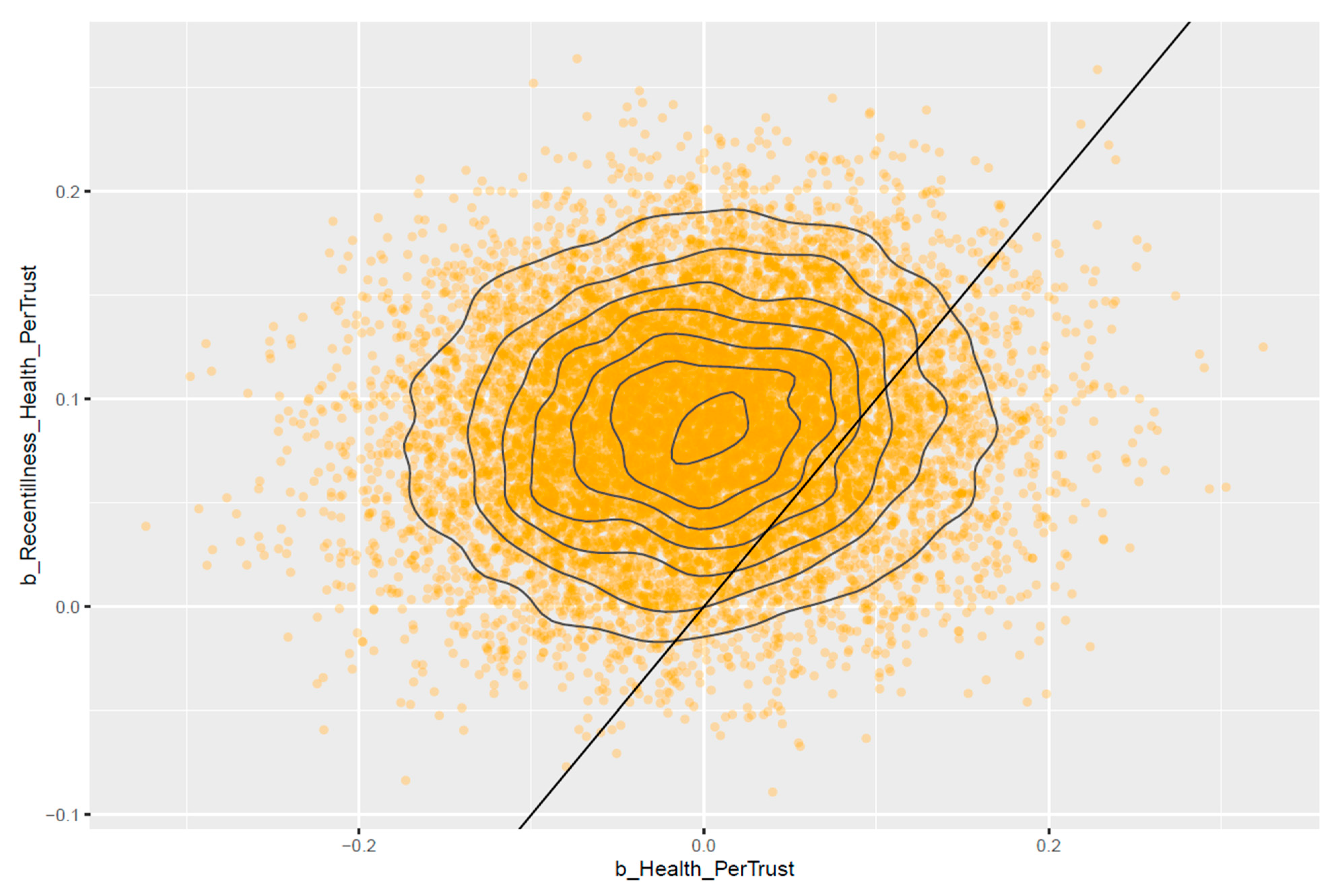
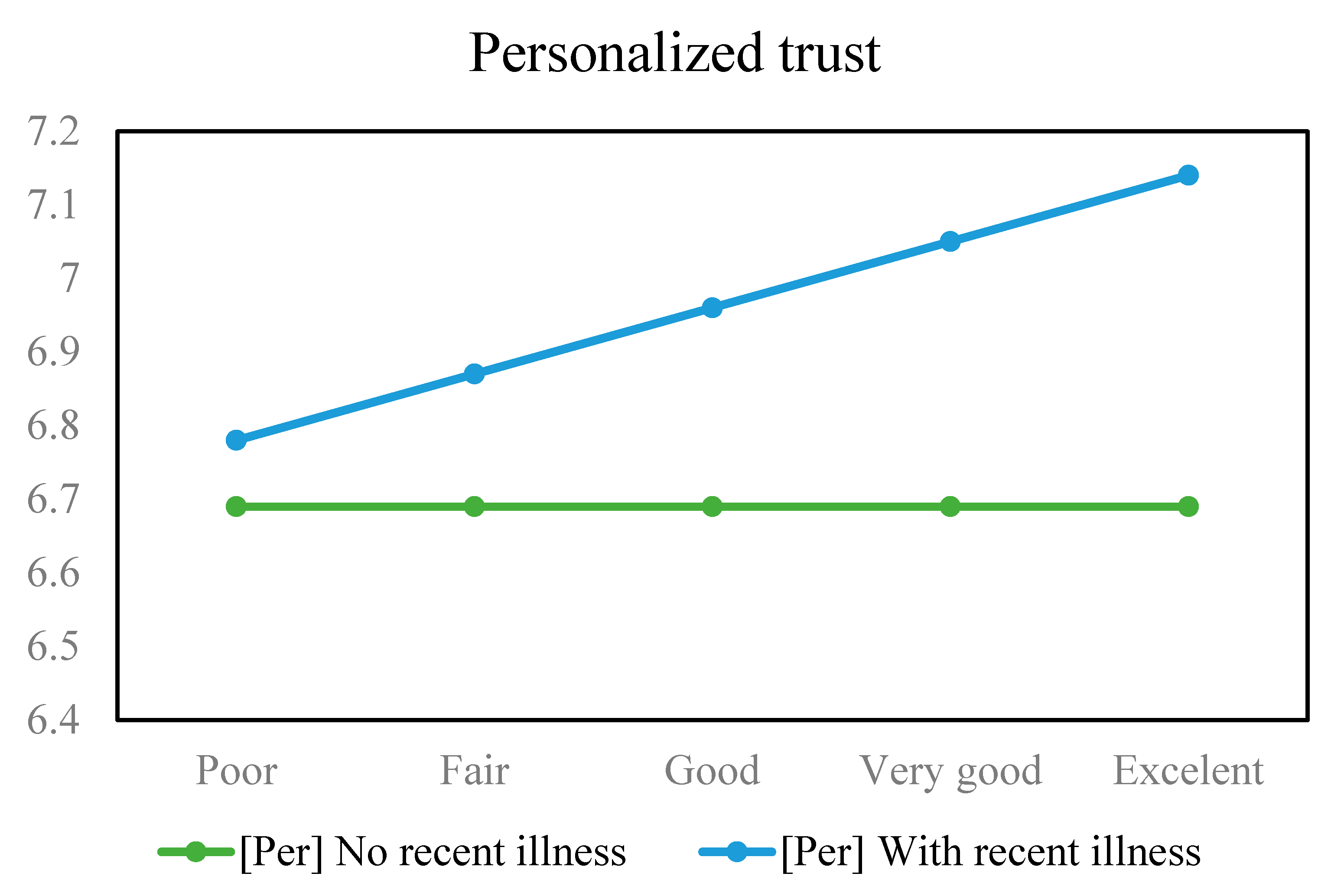
3.2. Model 2: Personalized Trust
4. Discussion
4.1. The Trust Mechanism in Relation to One’s Health
4.2. Differences between Generalized and Personalized Trust in Terms of Information Processing
4.3. Recommendations for Future Research Directions
4.4. Limitations
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kramer, R.M. Collective Trust within Organizations: Conceptual Foundations and Empirical Insights. Corp. Reput. Rev. 2010, 13, 82–97. [Google Scholar] [CrossRef]
- Baier, A. What is Trust? In Reading Onora O’Neill; Routledge: London, UK, 2013. [Google Scholar]
- Mayer, R.C.; Davis, J.H.; Schoorman, F.D. An Integrative Model of Organizational Trust. Acad. Manag. Rev. 1995, 20, 709–734. [Google Scholar] [CrossRef]
- Möllering, G. The Nature of Trust: From Georg Simmel to a Theory of Expectation, Interpretation and Suspension. Sociology 2001, 35, 403–420. [Google Scholar] [CrossRef]
- Möllering, G. The Trust/Control Duality: An Integrative Perspective on Positive Expectations of Others. Int. Sociol. 2005, 20, 283–305. [Google Scholar] [CrossRef]
- Nguyen, M.-H.; Le, T.-T.; Vuong, Q.-H. Ecomindsponge: A Novel Perspective on Human Psychology and Behavior in the Ecosystem. Urban Sci. 2023, 7, 31. [Google Scholar] [CrossRef]
- Schilke, O.; Reimann, M.; Cook, K.S. Trust in Social Relations. Annu. Rev. Sociol. 2021, 47, 239–259. [Google Scholar] [CrossRef]
- O’Neill, O. Autonomy and Trust in Bioethics; Cambridge University Press: Cambridge, UK, 2002. [Google Scholar]
- Simpson, T.W. What Is Trust? Pac. Philos. Q. 2012, 93, 550–569. [Google Scholar] [CrossRef]
- Held, V. On the Meaning of Trust. Ethics 1968, 78, 156–159. [Google Scholar] [CrossRef]
- Coleman, J. Foundations of Social Theory; Belknap Press: Cambridge, MA, USA, 1998; p. 1014. [Google Scholar]
- Le, T.-T.; Nguyen, M.-H.; Vuong, Q.-H. Chapter 4: Trust in mindsponge: A new perspective on information reliability. In The Mindsponge and BMF Analytics for Innovative Thinking in Social Sciences and Humanities; De Gruyter: Berlin, Germany, 2022; pp. 67–86. [Google Scholar]
- Barefoot, J.C.; Maynard, K.E.; Beckham, J.C.; Brummett, B.H.; Hooker, K.; Siegler, I.C. Trust, Health, and Longevity. J. Behav. Med. 1998, 21, 517–526. [Google Scholar] [CrossRef]
- Schneider, I.K.; Konijn, E.A.; Righetti, F.; Rusbult, C.E. A healthy dose of trust: The relationship between interpersonal trust and health. Pers. Relatsh. 2011, 18, 668–676. [Google Scholar] [CrossRef]
- Chan, D.K.C.; Hamamura, T.; Li, L.M.W.; Zhang, X. Effect of human development on the relationship between generalised trust and health: An international cross-sectional investigation. Lancet 2017, 390, S105. [Google Scholar] [CrossRef]
- Hamamura, T.; Li, L.M.W.; Chan, D. The Association Between Generalized Trust and Physical and Psychological Health across Societies. Soc. Indic. Res. 2017, 134, 277–286. [Google Scholar] [CrossRef]
- Jiang, J.; Li, Q.; Kang, R.; Wang, P. Social Trust and Health: A Perspective of Urban-Rural Comparison in China. Appl. Res. Qual. Life 2020, 15, 737–756. [Google Scholar] [CrossRef]
- Wang, Y.; Wai Li, L.M. Does your trust in strangers or close acquaintances promote better health? Societal residential mobility matters. J. Soc. Psychol. 2020, 160, 416–427. [Google Scholar] [CrossRef]
- Adjaye-Gbewonyo, K.; Kawachi, I.; Subramanian, S.V.; Avendano, M. High social trust associated with increased depressive symptoms in a longitudinal South African sample. Soc. Sci. Med. 2018, 197, 127–135. [Google Scholar] [CrossRef]
- Mattila, M.; Rapeli, L. Just sick of it? Health and political trust in Western Europe. Eur. J. Political Res. 2018, 57, 116–134. [Google Scholar] [CrossRef]
- Rapeli, L.; Mattila, M.; Papageorgiou, A. Breaking a habit: The impact of health on turnout and party choice. Party Politics 2020, 26, 133–142. [Google Scholar] [CrossRef]
- Duran-Nebreda, S.; Bassel, G.W. Plant behaviour in response to the environment: Information processing in the solid state. Philos. Trans. R. Soc. Lond. B Biol. Sci. 2019, 374, 20180370. [Google Scholar] [CrossRef]
- Palmer, M.S.; Gaynor, K.M.; Becker, J.A.; Abraham, J.O.; Mumma, M.A.; Pringle, R.M. Dynamic landscapes of fear: Understanding spatiotemporal risk. Trends Ecol. Evol. 2022, 37, 911–925. [Google Scholar] [CrossRef]
- Walters, E.T. Injury-Related Behavior and Neuronal Plasticity: An Evolutionary Perspective on Sensitization, Hyperalgesia, and Analgesia. In International Review of Neurobiology; Bradley, R.J., Harris, R.A., Eds.; Academic Press: Cambridge, MA, USA, 1994; Volume 36, pp. 325–427. [Google Scholar]
- Crook, R.J.; Lewis, T.; Hanlon, R.T.; Walters, E.T. Peripheral injury induces long-term sensitization of defensive responses to visual and tactile stimuli in the squid Loligo pealeii, Lesueur 1821. J. Exp. Biol. 2011, 214, 3173–3185. [Google Scholar] [CrossRef]
- Crook, R.J.; Dickson, K.; Hanlon, R.T.; Walters, E.T. Nociceptive sensitization reduces predation risk. Curr. Biol. 2014, 24, 1121–1125. [Google Scholar] [CrossRef]
- Vuong, Q.-H. Mindsponge Theory; De Gruyter: Berlin, Germany, 2023. [Google Scholar]
- Darwin, C. On the Origin of Species; Knight, D., Ed.; Routledge: London, UK, 2003; p. 502, Reprint. [Google Scholar]
- Vuong, Q.-H.; La, V.-P.; Nguyen, M.-H. The Mindsponge and BMF Analytics for Innovative Thinking in Social Sciences and Humanities; De Gruyter: Berlin, Germany, 2022. [Google Scholar]
- Nguyen, M.-H.; La, V.-P.; Le, T.-T.; Vuong, Q.-H. Introduction to Bayesian Mindsponge Framework analytics: An innovative method for social and psychological research. MethodsX 2022, 9, 101808. [Google Scholar] [CrossRef] [PubMed]
- Martínez, L.M.; Estrada, D.; Prada, S.I. Mental health, interpersonal trust and subjective well-being in a high violence context. SSM-Popul. Health 2019, 8, 100423. [Google Scholar] [CrossRef] [PubMed]
- Vuong, Q.H.; Napier, N.K. Acculturation and global mindsponge: An emerging market perspective. Int. J. Intercult. Relat. 2015, 49, 354–367. [Google Scholar] [CrossRef]
- Puderbaugh, M.; Emmady, P.D. Neuroplasticity. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Alberini, C.M.; Kandel, E.R. The regulation of transcription in memory consolidation. Cold Spring Harb. Perspect. Biol. 2015, 7, a021741. [Google Scholar] [CrossRef]
- Bernstein, C. DNA methylation and establishing memory. Epigenetics Insights 2022, 15, 25168657211072499. [Google Scholar] [CrossRef]
- Bliss, T.V.; Collingridge, G.L. A synaptic model of memory: Long-term potentiation in the hippocampus. Nature 1993, 361, 31–39. [Google Scholar] [CrossRef]
- Eagleman, D. The Brain: The Story of You; Canongate Books: Edinburgh, UK, 2015; p. 273. [Google Scholar]
- Costandi, M. Neuroplasticity; MIT Press: Cambridge, MA, USA, 2016; p. 193. [Google Scholar]
- Vuong, Q.-H.; Le, T.-T.; Jin, R.; Khuc, Q.V.; Nguyen, H.-S.; Vuong, T.-T.; Nguyen, M.-H. Near-Suicide Phenomenon: An Investigation into the Psychology of Patients with Serious Illnesses Withdrawing from Treatment. Int. J. Environ. Res. Public Health 2023, 20, 5173. [Google Scholar] [CrossRef]
- Suchow, J.W.; Bourgin, D.D.; Griffiths, T.L. Evolution in Mind: Evolutionary Dynamics, Cognitive Processes, and Bayesian Inference. Trends Cogn. Sci. 2017, 21, 522–530. [Google Scholar] [CrossRef]
- Jacobs, R.A.; Kruschke, J.K. Bayesian learning theory applied to human cognition. WIREs Cogn. Sci. 2011, 2, 8–21. [Google Scholar] [CrossRef]
- Chater, N.; Oaksford, M.; Hahn, U.; Heit, E. Bayesian models of cognition. WIREs Cogn. Sci. 2010, 1, 811–823. [Google Scholar] [CrossRef] [PubMed]
- Trenchard, H.; Perc, M. Energy saving mechanisms, collective behavior and the variation range hypothesis in biological systems: A review. Biosystems 2016, 147, 40–66. [Google Scholar] [CrossRef] [PubMed]
- Raichle, M.E.; Gusnard, D.A. Appraising the brain’s energy budget. Proc. Natl. Acad. Sci. USA 2002, 99, 10237–10239. [Google Scholar] [CrossRef] [PubMed]
- Kuzawa, C.W.; Chugani, H.T.; Grossman, L.I.; Lipovich, L.; Muzik, O.; Hof, P.R.; Wildman, D.E.; Sherwood, C.C.; Leonard, W.R.; Lange, N. Metabolic costs and evolutionary implications of human brain development. Proc. Natl. Acad. Sci. USA 2014, 111, 13010–13015. [Google Scholar] [CrossRef]
- Hofman, M. Evolution of the human brain: When bigger is better. Front. Neuroanat. 2014, 8, 15. [Google Scholar] [CrossRef]
- Haider, B.; Krause, M.R.; Duque, A.; Yu, Y.; Touryan, J.; Mazer, J.A.; McCormick, D.A. Synaptic and Network Mechanisms of Sparse and Reliable Visual Cortical Activity during Nonclassical Receptive Field Stimulation. Neuron 2010, 65, 107–121. [Google Scholar] [CrossRef]
- Vuong, Q.-H.; Le, T.-T.; La, V.-P.; Nguyen, M.-H. The psychological mechanism of Internet information processing for post-treatment evaluation. Heliyon 2022, 8, e09351. [Google Scholar] [CrossRef]
- Nickerson, R.S. Confirmation Bias: A Ubiquitous Phenomenon in Many Guises. Rev. Gen. Psychol. 1998, 2, 175–220. [Google Scholar] [CrossRef]
- Tanemura, N.; Kakizaki, M.; Kusumi, T.; Onodera, R.; Chiba, T. Levels of trust in risk-only negative health messages issued by public agencies: A quantitative research-based mindsponge framework. Humanit. Soc. Sci. Commun. 2022, 9, 388. [Google Scholar] [CrossRef]
- Tanemura, N.; Chiba, T. The usefulness of a checklist approach-based confirmation scheme in identifying unreliable COVID-19-related health information: A case study in Japan. Humanit. Soc. Sci. Commun. 2022, 9, 270. [Google Scholar] [CrossRef]
- Vuong, Q.-H.; Le, T.-T.; La, V.-P.; Nguyen, H.T.T.; Ho, M.-T.; Van Khuc, Q.; Nguyen, M.-H. COVID-19 vaccines production and societal immunization under the serendipity-mindsponge-3D knowledge management theory and conceptual framework. Humanit. Soc. Sci. Commun. 2022, 9, 22. [Google Scholar] [CrossRef]
- Robitzsch, A. Why Ordinal Variables Can (Almost) Always Be Treated as Continuous Variables: Clarifying Assumptions of Robust Continuous and Ordinal Factor Analysis Estimation Methods. Front. Educ. 2020, 5, 589965. [Google Scholar] [CrossRef]
- Wilkinson, M.D.; Dumontier, M.; Aalbersberg, I.J.; Appleton, G.; Axton, M.; Baak, A.; Blomberg, N.; Boiten, J.-W.; da Silva Santos, L.B.; Bourne, P.E.; et al. The FAIR Guiding Principles for scientific data management and stewardship. Sci. Data 2016, 3, 160018. [Google Scholar] [CrossRef]
- Martínez, L. Trust, life satisfaction and health: Population data in mid-size city in the Global South. Data Brief 2019, 27, 104639. [Google Scholar] [CrossRef]
- Nguyen, V.H.; Vuong, Q.H. On the Martingale Representation Theorem and on Approximate Hedging a Contingent Claim in the Minimum Deviation Square Criterion. In Some Topics in Industrial and Applied Mathematics; Jeltsch, R., Li, T., Sloan, I., Eds.; Series in Contemporary Applied Mathematics; World Scientific: Hackensack, NJ, USA, 2007; pp. 134–151. [Google Scholar]
- Nguyen, V.H.; Vuong, Q.H.; Tran, M.N. Central limit theorem for functional of jump Markov processes. Vietnam J. Math. 2005, 33, 443–461. [Google Scholar]
- Vehtari, A.; Gelman, A.; Gabry, J. Practical Bayesian model evaluation using leave-one-out cross-validation and WAIC. Stat. Comput. 2017, 27, 1413–1432. [Google Scholar] [CrossRef]
- La, V.-P.; Vuong, Q.-H. Package ‘bayesvl’: Visually Learning the Graphical Structure of Bayesian Networks and Performing MCMC with ‘Stan’; The Comprehensive R Archive Network (CRAN): Online, 2019. [Google Scholar]
- Vuong, Q.-H.; La, V.-P.; Nguyen, M.-H.; Ho, M.-T.; Tran, T.; Ho, M.-T. Bayesian analysis for social data: A step-by-step protocol and interpretation. MethodsX 2020, 7, 100924. [Google Scholar] [CrossRef] [PubMed]
- Vuong, Q.-H. Reform retractions to make them more transparent. Nature 2020, 582, 149. [Google Scholar] [CrossRef]
- Vuong, Q.-H. The (ir)rational consideration of the cost of science in transition economies. Nat. Hum. Behav. 2018, 2, 5. [Google Scholar] [CrossRef]
- Millan, M.J. Descending control of pain. Prog. Neurobiol. 2002, 66, 355–474. [Google Scholar] [CrossRef] [PubMed]
- Woolf, C.J.; Walters, E.T. Common patterns of plasticity contributing to nociceptive sensitization in mammals and Aplysia. Trends Neurosci. 1991, 14, 74–78. [Google Scholar] [CrossRef] [PubMed]
- Lai, V.T.; van Berkum, J.; Hagoort, P. Negative affect increases reanalysis of conflicts between discourse context and world knowledge. Front. Commun. 2022, 7, 100423. [Google Scholar] [CrossRef]
- Nguyen, M.-H. Chapter 7: Conditions for improving serendipity encounter and attainment probability. In A New Theory of Serendipity: Nature, Emergence and Mechanism; Vuong, Q.-H., Ed.; De Gruyter: Berlin, Germany, 2022; pp. 109–130. [Google Scholar]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Meaning | Type of Variable | Value |
|---|---|---|---|
| GenTrust | The respondents’ degree of generalized trust | Ordinal | From 0 (not at all) to 10 (completely) |
| PerTrust | The respondents’ degree of personalized trust | Ordinal | From 0 (not at all) to 10 (completely) |
| Health | The respondent’s general health status | Ordinal | From 1 (poor) to 5 (excellent) |
| Recentillness | Whether the respondent experienced physical illness in the past 30 days | Binary | 0 (no) or 1 (yes) |
| Parameters | Mean | SD | n_eff | Rhat |
|---|---|---|---|---|
| Constant | 3.71 | 0.33 | 4977 | 1 |
| Health | 0.21 | 0.07 | 5062 | 1 |
| Recentillness ∗ Health | −0.08 | 0.04 | 7349 | 1 |
| Parameters | Mean | SD | n_eff | Rhat |
|---|---|---|---|---|
| Constant | 6.69 | 0.39 | 5270 | 1 |
| Health | 0.00 | 0.08 | 5410 | 1 |
| Recentillness ∗ Health | 0.09 | 0.05 | 8348 | 1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vuong, Q.-H.; Nguyen, P.-L.; Jin, R.; Nguyen, M.-H.; Le, T.-T. Trust Is for the Strong: How Health Status May Influence Generalized and Personalized Trust. Healthcare 2023, 11, 2373. https://doi.org/10.3390/healthcare11172373
Vuong Q-H, Nguyen P-L, Jin R, Nguyen M-H, Le T-T. Trust Is for the Strong: How Health Status May Influence Generalized and Personalized Trust. Healthcare. 2023; 11(17):2373. https://doi.org/10.3390/healthcare11172373
Chicago/Turabian StyleVuong, Quan-Hoang, Phuong-Loan Nguyen, Ruining Jin, Minh-Hoang Nguyen, and Tam-Tri Le. 2023. "Trust Is for the Strong: How Health Status May Influence Generalized and Personalized Trust" Healthcare 11, no. 17: 2373. https://doi.org/10.3390/healthcare11172373