
Evaluating Changes in Trauma Epidemiology during the COVID-19 Lockdown: Insights and Implications for Public Health and Disaster Preparedness

 ,
,  , , ,
, , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Background
2.2. Statistical Analyses
3. Results
4. Discussion
4.1. Trauma Volume
4.2. Median Age
4.3. Trauma Mortality
4.4. Injury Mechanisms
4.5. Anatomic Description of Injury
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Injuries and Violence: The Facts 2014; Department for the Management of Noncommunicable Diseases, Disability, Violence and Injury Prevention; World Health Organization: Geneva, Switzerland, 2014; ISBN 978-92-4-150801-8. [Google Scholar]
- Kochanek, K.D.; Murphy, S.L.; Xu, J.; Arias, E. Deaths: Final Data for 2017. Natl. Vital Stat. Rep. 2019, 68, 1–77. [Google Scholar] [PubMed]
- Centers for Disease Control. Leading Cause of Death Reports, 1981–2018. Available online: https://www.cdc.gov/injury/wisqars/index.html (accessed on 20 March 2020).
- Zhu, N.; Zhang, D.; Wang, W.; Li, X.; Yang, B.; Song, J.; Zhao, X.; Huang, B.; Shi, W.; Lu, R.; et al. A Novel Coronavirus from Patients with Pneumonia in China, 2019. N. Engl. J. Med. 2020, 382, 727–733. [Google Scholar] [CrossRef]
- Camine, T.; Rembisz, A.; Barron, R.; Baldwin, C.; Kromer, M. Decrease in Trauma Admissions with COVID-19 Pandemic. WestJEM 2020, 21, 47780. [Google Scholar] [CrossRef] [PubMed]
- DiFazio, L.T.; Curran, T.; Bilaniuk, J.W.; Adams, J.M.; Durling-Grover, R.; Kong, K.; Nemeth, Z.H. The Impact of the COVID-19 Pandemic on Hospital Admissions for Trauma and Acute Care Surgery. Am. Surg. 2020, 86, 901–903. [Google Scholar] [CrossRef] [PubMed]
- Badach, J.M.; Platoff, R.; Rattigan, D.; Butts, C.A.; Shea, L.; Gaughan, J.P.; Hunter, K.; Sifri, Z.; Porter, J.; Egodage, T. Trauma Incidence during the New Jersey COVID-19 Stay-At-Home Order: A Multicenter Study. J. Surg. Res. 2023, 284, 264–268. [Google Scholar] [CrossRef]
- Migliorini, F.; Weber, C.D.; Pappalardo, G.; Schenker, H.; Hofmann, U.K.; Eschweiler, J.; Hildebrand, F. Orthopaedic, Trauma Surgery, and Covid-2019 Pandemic: Clinical Panorama and Future Prospective in Europe. Eur. J. Trauma Emerg. Surg. 2022, 48, 4385–4402. [Google Scholar] [CrossRef]
- Comelli, I.; Scioscioli, F.; Cervellin, G. Impact of the COVID-19 Epidemic on Census, Organization and Activity of a Large Urban Emergency Department.: COVID-19 Epidemic in a Large Emergency Department. Acta Bio Medica Atenei Parm. 2020, 91, 45–49. [Google Scholar] [CrossRef]
- Sephton, B.M.; Mahapatra, P.; Shenouda, M.; Ferran, N.; Deierl, K.; Sinnett, T.; Somashekar, N.; Sarraf, K.M.; Nathwani, D.; Bhattacharya, R. The Effect of COVID-19 on a Major Trauma Network. An Analysis of Mechanism of Injury Pattern, Referral Load and Operative Case-Mix. Injury 2021, 52, 395–401. [Google Scholar] [CrossRef] [PubMed]
- Rozenfeld, M.; Peleg, K.; Givon, A.; Bala, M.; Shaked, G.; Bahouth, H.; Bodas, M. COVID-19 Changed the Injury Patterns of Hospitalized Patients. Prehosp. Disaster Med. 2021, 36, 251–259. [Google Scholar] [CrossRef]
- Waseem, S.; Nayar, S.K.; Hull, P.; Carrothers, A.; Rawal, J.; Chou, D.; Khanduja, V. The Global Burden of Trauma during the COVID-19 Pandemic: A Scoping Review. J. Clin. Orthop. Trauma 2021, 12, 200–207. [Google Scholar] [CrossRef]
- Antonini, M.; Hinwood, M.; Paolucci, F.; Balogh, Z.J. The Epidemiology of Major Trauma during the First Wave of COVID-19 Movement Restriction Policies: A Systematic Review and Meta-Analysis of Observational Studies. World J. Surg. 2022, 46, 2045–2060. [Google Scholar] [CrossRef]
- Gujski, M.; Raciborski, F.; Jankowski, M.; Nowicka, P.M.; Rakocy, K.; Pinkas, J. Epidemiological Analysis of the First 1389 Cases of COVID-19 in Poland: A Preliminary Report. Med. Sci. Monit. 2020, 26, e924702. [Google Scholar] [CrossRef]
- Regulation of the Minister of Health, 13 March 2020. Available online: https://isap.sejm.gov.pl/isap.nsf/download.xsp/WDU20200000433/O/D20200433.pdf (accessed on 31 March 2023).
- Regulation of the Minister of Health, 24 March 2020. Available online: https://isap.sejm.gov.pl/isap.nsf/download.xsp/WDU20200000522/O/D20200522.pdf (accessed on 31 March 2023).
- Coronavirus (SARS-CoV-2) Infection Report. Available online: https://www.gov.pl/web/koronawirus/wykaz-zarazen-koronawirusem-sars-cov-2 (accessed on 18 April 2023).
- Raciborski, F.; Pinkas, J.; Jankowski, M.; Sierpiński, R.; Zgliczyński, W.S.; Szumowski, Ł.; Rakocy, K.; Wierzba, W.; Gujski, M. Dynamics of COVID-19 Outbreak in Poland: An Epidemiological Analysis of the First Two Months of the Epidemic. Pol. Arch. Intern. Med. 2020, 130, 615–621. [Google Scholar] [CrossRef] [PubMed]
- Grajek, M.; Białek-Dratwa, A. The Impact of the Epidemiological Situation Resulting From COVID-19 Pandemic on Selected Aspects of Mental Health among Patients with Cancer–Silesia Province (Poland). Front. Psychol. 2022, 13, 857326. [Google Scholar] [CrossRef]
- Karpiński, R.; Krakowski, P.; Jonak, J.; Machrowska, A.; Maciejewski, M.; Nogalski, A. Diagnostics of Articular Cartilage Damage Based on Generated Acoustic Signals Using ANN—Part I: Femoral-Tibial Joint. Sensors 2022, 22, 2176. [Google Scholar] [CrossRef]
- Karpiński, R.; Krakowski, P.; Jonak, J.; Machrowska, A.; Maciejewski, M.; Nogalski, A. Diagnostics of Articular Cartilage Damage Based on Generated Acoustic Signals Using ANN—Part II: Patellofemoral Joint. Sensors 2022, 22, 3765. [Google Scholar] [CrossRef] [PubMed]
- Karpiński, R. Knee Joint Osteoarthritis Diagnosis Based on Selected Acoustic Signal Discriminants Using Machine Learning. Appl. Comput. Sci. 2022, 18, 71–85. [Google Scholar] [CrossRef]
- Jojczuk, M.; Kamiński, P.; Gajewski, J.; Karpiński, R.; Krakowski, P.; Jonak, J.; Nogalski, A.; Głuchowski, D. Use of Neural Network Based on International Classification ICD-10 in Patients with Head and Neck Injuries in Lublin Province, Poland, between 2006–2018, as a Predictive Value of the Outcomes of Injury Sustained. Ann. Agric. Environ. Med. 2023, 30, 281–286. [Google Scholar] [CrossRef]
- Law, R.K.; Wolkin, A.F.; Patel, N.; Alic, A.; Yuan, K.; Ahmed, K.; Idaikkadar, N.; Haileyesus, T. Injury-Related Emergency Department Visits during the COVID-19 Pandemic. Am. J. Prev. Med. 2022, 63, 43–50. [Google Scholar] [CrossRef] [PubMed]
- Amick, M.; Bentivegna, K.; Hunter, A.A.; Leventhal, J.M.; Livingston, N.; Bechtel, K.; Holland, M.L. Child Maltreatment-Related Children’s Emergency Department Visits before and during the COVID-19 Pandemic in Connecticut. Child Abus. Negl. 2022, 128, 105619. [Google Scholar] [CrossRef] [PubMed]
- Al Afreed, F.M.; Lane, T.J.; Gray, S.E. Work-Related Injuries in the Australian Education Sector: A Retrospective Cohort Study. Injury 2022, 53, 3962–3969. [Google Scholar] [CrossRef]
- Boom, L.J.; Wolvius, E.B.; Rozeboom, A.V.J. Impact of COVID-19 Lockdown on Incidence of Maxillofacial Fractures: A Retrospective Analysis. Adv. Oral Maxillofac. Surg. 2022, 6, 100289. [Google Scholar] [CrossRef]
- Pidgeon, T.E.; Parthiban, S.; Malone, P.; Foster, M.; Chester, D.L. Injury Patterns of Patients with Upper Limb and Hand Trauma Sustained during the COVID-19 Pandemic Lockdown in the UK: A Retrospective Cohort Study. Hand Surg. Rehabil. 2021, 40, 235–240. [Google Scholar] [CrossRef] [PubMed]
- Ho, E.; Riordan, E.; Nicklin, S. Hand Injuries during COVID-19: Lessons from Lockdown. J. Plast. Reconstr. Aesthet. Surg. 2021, 74, 1408–1412. [Google Scholar] [CrossRef] [PubMed]
- Saini, N.; Ranjan, R.; Jain, V.K.; Shukla, A. Pooling of Neglected and Delayed Trauma Patients–Consequences of ‘Lockdown’ and ‘Unlock’ Phases of COVID-19 Pandemic- A Retrospective Cohort Analysis from a Tertiary Centre. J. Clin. Orthop. Trauma 2021, 21, 101533. [Google Scholar] [CrossRef] [PubMed]
- Główny Urząd Statystyczny/Obszary Tematyczne/Ludność/Ludność/Rezydenci (Ludność Rezydująca). Available online: Https://Stat.Gov.Pl/Obszary-Tematyczne/Ludnosc/Ludnosc/Ludnosc-Stan-i-Struktura-Ludnosci-Oraz-Ruch-Naturalny-w-Przekroju-Terytorialnym-Stan-w-Dniu-30-06-2021,6,30.Html (accessed on 21 September 2022).
- Nowicki, G.J.; Ślusarska, B.; Naylor, K.; Prystupa, A.; Rudnicka-Drożak, E.; Halyuk, U.; Pokotylo, P. The Relationship between the Metabolic Syndrome and the Place of Residence in the Local Community on the Example of the Janów Lubelski District in Eastern Poland: A Population-Based Study. Diabetes Metab. Syndr. Obes. 2021, 14, 2041–2056. [Google Scholar] [CrossRef] [PubMed]
- Poznańska, A.; Goryński, P.; Seroka, W.; Stokwiszewski, J.; Radomski, P.; Wojtyniak, B. Nationwide General Hospital Morbidity Study as a Source of Data about Polish Population Health. Prz. Epidemiol. 2019, 73, 69–80. [Google Scholar] [CrossRef]
- Kim, H.-Y. Statistical Notes for Clinical Researchers: Simple Linear Regression 3–Residual Analysis. Restor. Dent. Endod. 2019, 44, e11. [Google Scholar] [CrossRef]
- Rajput, K.; Sud, A.; Rees, M.; Rutka, O. Epidemiology of Trauma Presentations to a Major Trauma Centre in the North West of England during the COVID-19 Level 4 Lockdown. Eur. J. Trauma Emerg. Surg. 2021, 47, 631–636. [Google Scholar] [CrossRef]
- Vatsya, P.; Garika, S.S.; Mittal, S.; Trikha, V.; Sharma, V.; Malhotra, R. Lockdown Imposition Due to COVID-19 and Its Effect on Orthopedic Emergency Department in Level 1 Trauma Center in South Asia. J. Clin. Orthop. Trauma 2022, 28, 101826. [Google Scholar] [CrossRef] [PubMed]
- Kreis, C.A.; Ortmann, B.; Freistuehler, M.; Hartensuer, R.; Van Aken, H.; Raschke, M.J.; Schliemann, B. Impact of the First COVID-19 Shutdown on Patient Volumes and Surgical Procedures of a Level I Trauma Center. Eur. J. Trauma Emerg. Surg. 2021, 47, 665–675. [Google Scholar] [CrossRef] [PubMed]
- Harris, D.; Ellis, D.Y.; Gorman, D.; Foo, N.; Haustead, D. Impact of COVID-19 Social Restrictions on Trauma Presentations in South Australia. Emerg. Med. Australas. 2021, 33, 152–154. [Google Scholar] [CrossRef] [PubMed]
- Bäckström, D.; Wladis, A. A Cohort Study of Trauma Patients in Sweden during the First Months of the COVID-19 Pandemic: A Small Reduction in Trauma Admissions. Scand. J. Trauma Resusc. Emerg. Med. 2022, 30, 12. [Google Scholar] [CrossRef]
- Berg, G.M.; Wyse, R.J.; Morse, J.L.; Chipko, J.; Garland, J.M.; Slivinski, A.; Lieser, M.; Biswas, S.; Carrick, M.M.; Rhodes, H.; et al. Decreased Adult Trauma Admission Volumes and Changing Injury Patterns during the COVID-19 Pandemic at 85 Trauma Centers in a Multistate Healthcare System. Trauma Surg. Acute Care Open 2021, 6, e000642. [Google Scholar] [CrossRef]
- Moyer, J.-D.; James, A.; Gakuba, C.; Boutonnet, M.; Angles, E.; Rozenberg, E.; Bardon, J.; Clavier, T.; Legros, V.; Werner, M.; et al. Impact of the SARS-CoV-2 Outbreak on Epidemiology and Management of Major Traumain France: A Registry-Based Study (the COVITRAUMA Study). Scand. J. Trauma Resusc. Emerg. Med. 2021, 29, 51. [Google Scholar] [CrossRef]
- Ohm, E.; Hauge, L.J.; Madsen, C.; Grøholt, E.K.; Evensen, M.; Reneflot, A. Impact of the COVID-19 Pandemic on the Treatment of Injuries during Lockdown in Norway. Scand. J. Public Health 2021, 49, 689–696. [Google Scholar] [CrossRef]
- Ruzzini, L.; De Salvatore, S.; Lamberti, D.; Maglione, P.; Piergentili, I.; Crea, F.; Ossella, C.; Costici, P.F. COVID-19 Changed the Incidence and the Pattern of Pediatric Traumas: A Single-Centre Study in a Pediatric Emergency Department. Int. J. Environ. Res. Public Health 2021, 18, 6573. [Google Scholar] [CrossRef]
- Payr, S.; Schuller, A.; Dangl, T.; Scheider, P.; Sator, T.; Chocholka, B.; Jaindl, M.; Schwendenwein, E.; Tiefenboeck, T.M. Maintaining Medical Resources to Treat Paediatric Injuries during COVID-19 Lockdown Is Essential—An Epidemiological Analysis of a Level 1 Trauma Centre in Central Europe. Int. J. Environ. Res. Public Health 2021, 18, 5829. [Google Scholar] [CrossRef]
- Verdoni, F.; Ricci, M.; Di Grigoli, C.; Rossi, N.; Lombardo, M.D.M.; Curci, D.; Accetta, R.; Viganò, M.; Peretti, G.M.; Mangiavini, L. Effect of the COVID-19 Outbreak on Pediatric Patients’ Admissions to the Emergency Department in an Italian Orthopedic Trauma Hub. Children 2021, 8, 645. [Google Scholar] [CrossRef]
- Adiamah, A.; Thompson, A.; Lewis-Lloyd, C.; Dickson, E.; Blackburn, L.; Moody, N.; Gida, S.; La Valle, A.; Reilly, J.-J.; Saunders, J.; et al. The ICON Trauma Study: The Impact of the COVID-19 Lockdown on Major Trauma Workload in the UK. Eur. J. Trauma Emerg. Surg. 2021, 47, 637–645. [Google Scholar] [CrossRef] [PubMed]
- Riuttanen, A.; Ponkilainen, V.; Kuitunen, I.; Reito, A.; Sirola, J.; Mattila, V.M. Severely Injured Patients Do Not Disappear in a Pandemic: Incidence and Characteristics of Severe Injuries during COVID-19 Lockdown in Finland. Acta Orthop. 2021, 92, 249–253. [Google Scholar] [CrossRef]
- Ojima, M.; Ishida, K.; Katayama, Y.; Hirose, T.; Nakao, S.; Tachino, J.; Noda, T.; Umemura, Y.; Kiguchi, T.; Kiyohara, K.; et al. Impact of the COVID-19 Pandemic on Epidemiology, Treatment, and Outcome of Major Trauma in Japan in 2020: A Retrospective Observational Nationwide Registry-based Study. Acute Med. Surg. 2023, 10, e817. [Google Scholar] [CrossRef] [PubMed]
- Hakkenbrak, N.A.G.; Loggers, S.A.I.; Lubbers, E.; De Geus, J.; Van Wonderen, S.F.; Berkeveld, E.; Mikdad, S.; Giannakopoulos, G.F.; Ponsen, K.J.; Bloemers, F.W.; et al. Trauma Care during the COVID-19 Pandemic in The Netherlands: A Level 1 Trauma Multicenter Cohort Study. Scand. J. Trauma Resusc. Emerg. Med. 2021, 29, 130. [Google Scholar] [CrossRef] [PubMed]
- Chiba, H.; Lewis, M.; Benjamin, E.R.; Jakob, D.A.; Liasidis, P.; Wong, M.D.; Navarrete, S.; Carreon, R.; Demetriades, D. “Safer at Home”: The Effect of the COVID-19 Lockdown on Epidemiology, Resource Utilization, and Outcomes at a Large Urban Trauma Center. J. Trauma Acute Care Surg. 2021, 90, 708–713. [Google Scholar] [CrossRef] [PubMed]
- Ghafil, C.; Matsushima, K.; Ding, L.; Henry, R.; Inaba, K. Trends in Trauma Admissions during the COVID-19 Pandemic in Los Angeles County, California. JAMA Netw. Open 2021, 4, e211320. [Google Scholar] [CrossRef]
- Colcuc, C.; Fischer, S.; Leimkühler, P.; Miersbach, M.; Lefering, R.; Dgu, T.; Wähnert, D.; Vordemvenne, T.; Grüneweller, N. Impact of the First and Second Wave of the SARS-CoV-2 Pandemic on Severe Trauma and the Care Structures in the German TraumaNetzwerk DGU®. J. Clin. Med. 2022, 11, 7036. [Google Scholar] [CrossRef]
- Mucha, B.; Mucha, M. Aktywność fizyczna w dobie pandemii COVID-19; University of Wroclaw: Wrocław, Poland, 2021. [Google Scholar] [CrossRef]
- Miękisiak, G.; Szarek, D.; Pettersson, S.D.; Pezowicz, C.; Morasiewicz, P.; Kubaszewski, Ł.; Szmuda, T. The Increased Mortality Rate with Lower Incidence of Traumatic Brain Injury during the COVID-19 Pandemic: A National Study. Healthcare 2022, 10, 1954. [Google Scholar] [CrossRef]
- Pinggera, D.; Klein, B.; Thomé, C.; Grassner, L. The Influence of the COVID-19 Pandemic on Traumatic Brain Injuries in Tyrol: Experiences from a State under Lockdown. Eur. J. Trauma Emerg. Surg. 2021, 47, 653–658. [Google Scholar] [CrossRef]
- Grassner, L.; Petr, O.; Warner, F.M.; Dedeciusova, M.; Mathis, A.M.; Pinggera, D.; Gsellmann, S.; Meiners, L.C.; Freigang, S.; Mokry, M.; et al. Trends and Outcomes for Non-Elective Neurosurgical Procedures in Central Europe during the COVID-19 Pandemic. Sci. Rep. 2021, 11, 6171. [Google Scholar] [CrossRef]
- Santing, J.A.L.; Van Den Brand, C.L.; Jellema, K. Traumatic Brain Injury during the SARS-CoV-2 Pandemic. Neurotrauma Rep. 2020, 1, 5–7. [Google Scholar] [CrossRef] [PubMed]
- Manivannan, S.; Sharouf, F.; Mayo, I.; Albaqer, H.; Mehrez, M.; Jaber, H.; Nicholls, Z.; Woodward, B.O.; Watkins, W.J.; Zaben, M. Management of Neurotrauma during COVID-19: A Single Centre Experience and Lessons for the Future. Brain Inj. 2021, 35, 957–963. [Google Scholar] [CrossRef] [PubMed]
- Jayakumar, N.; Kennion, O.; Villabona, A.R.; Paranathala, M.; Holliman, D. Neurosurgical Referral Patterns during the Coronavirus Disease 2019 Pandemic: A United Kingdom Experience. World Neurosurg. 2020, 144, e414–e420. [Google Scholar] [CrossRef]
- Dolci, A.; Marongiu, G.; Leinardi, L.; Lombardo, M.; Dessì, G.; Capone, A. The Epidemiology of Fractures and Muskulo-Skeletal Traumas during COVID-19 Lockdown: A Detailed Survey of 17.591 Patients in a Wide Italian Metropolitan Area. Geriatr. Orthop. Surg. Rehabil. 2020, 11, 215145932097267. [Google Scholar] [CrossRef] [PubMed]
- Malige, A.; Deemer, A.; Sobel, A.D. The Effect of COVID-19 on Adult Traumatic Orthopedic Injuries: A Database Study. Eur. J. Trauma Emerg. Surg. 2022, 48, 2813–2822. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.-J.; Cho, Y.J.; Lee, D. The Impact of COVID-19 on the Epidemiologic Characteristics of Traumatic Fractures: A Systematic Review of Recent Literature. Acta Orthop. Traumatol. Turc. 2021, 55, 439–443. [Google Scholar] [CrossRef] [PubMed]
- MacDonald, D.R.W.; Neilly, D.W.; Davies, P.S.E.; Crome, C.R.; Jamal, B.; Gill, S.L.; Jariwala, A.C.; Stevenson, I.M.; Ashcroft, G.P. SCORE authors Effects of the COVID-19 Lockdown on Orthopaedic Trauma: A Multicentre Study across Scotland. Bone Jt. Open 2020, 1, 541–548. [Google Scholar] [CrossRef]
- Nuñez, J.H.; Sallent, A.; Lakhani, K.; Guerra-Farfan, E.; Vidal, N.; Ekhtiari, S.; Minguell, J. Impact of the COVID-19 Pandemic on an Emergency Traumatology Service: Experience at a Tertiary Trauma Centre in Spain. Injury 2020, 51, 1414–1418. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| Area of Injury | ICD-10 Code |
|---|---|
| Injury of head | S00–S11.9, S15–S19.9, T06.0–T06.1, T90.0–T91.9 |
| Injury of thorax | S20–S21.9, S22.2–S22.9, S23.2–S23.5, S24.3–S29.9 |
| Injury of abdomen | S30–S31.8, S34.4–S39.9 |
| Injury of spine and pelvis | S12–S14.6, S22.0–S22.1, S23.0–S23.1, S24.0–S24.2, S32.0–S34.3, T08, T09.3, T09.4 |
| Injury of upper limbs | S40–S69.9, T05.0–T05.2, T10–T11.9, T92.0–T92.9 |
| Injury of lower limbs | S70–S99.9, T05.3–T05.5, T12–T13.9, T93.0–T93.9 |
| External injuries | T00–T01.9, T14.0, T20–T35.7, T66–T68, T95.0–T98.3 |
| Others | S00.0–T87 not included above |
| Injury Mechanism | ICD-10 Code |
|---|---|
| Communication injuries | |
| Pedestrian injured in collision | V01–V09 |
| Pedal cyclist injured in collision | V10–V19 |
| Motorcycle rider injured in collision | V20–V29 |
| Car occupant injured in collision with pedestrian or animal | V40–V49 |
| Occupant of pick-up truck or van injured in collision with pedestrian or animal | V50–V79 |
| Other communication injuries. | V30–V39, V80–V99, Y85 |
| Non-communication injuries | |
| Falls from same level | W00–W09, W18 |
| Fall on and from height | W10–W17, Y30 |
| Assaulted by another person | W32–W34, W50–W52, X88–Y05, Y07–Y09, Y20, Y22–Y23 |
| Intentional self-harm | X70–X84, Y87 |
| Attacked by an animal | W53–W59, X20–X29 |
| Contact with lifting and transmission devices | W24, W28–W31 |
| Struck by thrown, projected, or falling object | W20–W23, W25–W27, W44–W45, W60, Y28–Y29 |
| Exposure to high or low temperature, high or low pressure, electric current, forces of nature | W35–W41, W85–W92, X00–X19, X30–X33, Y25–Y27 |
| Other causes | V00–Y87 not included above |
| Variable | 2019 | 2020 | p | RR | 95% CI | |||
|---|---|---|---|---|---|---|---|---|
| n | % | n | % | LL | UL | |||
| Total admissions | 10,806 | 67.5 | 5212 | 32.5 | <0.001 | 2.07 | 2.02 | 2.13 |
| Admissions by age | ||||||||
| 1–17 | 1754 | 16.3 | 540 | 10.4 | <0.001 | 1.57 | 1.43 | 1.72 |
| 18–45 | 4354 | 40.4 | 2056 | 39.5 | 1.02 | 0.98 | 1.07 | |
| 46–65 | 3157 | 23.8 | 1339 | 25.7 | 0.93 | 0.88 | 0.98 | |
| 65+ | 1513 | 19.5 | 1271 | 24.4 | 0.80 | 0.75 | 0.85 | |
| Mortality | 83 | 0.77 | 87 | 1.67 | <0.001 | 0.46 | 0.34 | 0.62 |
| Mortality by sex | ||||||||
| Male | 52 | 0.78 | 52 | 1.63 | <0.001 | 0.48 | 0.33 | 0.70 |
| Female | 31 | 0.75 | 35 | 1.73 | <0.001 | 0.43 | 0.27 | 0.70 |
| Mortality by age | ||||||||
| 1–17 | 0 | 0 | 3 | 0.56 | 0.013 a | n/a | n/a | n/a |
| 18–45 | 6 | 0.14 | 5 | 0.24 | 0.346 a | 0.57 | 0.17 | 1.85 |
| 46–65 | 21 | 0.82 | 17 | 1.27 | 0.173 b | 0.64 | 0.34 | 1.22 |
| 65+ | 56 | 2.67 | 61 | 4.80 | 0.001 b | 0.56 | 0.39 | 0.79 |
| Variable | 2019 (n = 10,806) | 2020 (n = 5212) | Z | p | r | ||
|---|---|---|---|---|---|---|---|
| Mdn | IQR | Mdn | IQR | ||||
| Age of patients | 40 | 39 | 46 | 35 | −11.44 | <0.001 | 0.11 |
| Variable | 2019 | 2020 | RR | 95% CI | |||
|---|---|---|---|---|---|---|---|
| n | % | n | % | LL | UL | ||
| Mechanism of injury | |||||||
| Pedestrian injured in collision | 52 | 2.3 | 24 | 2.2 | 1.24 | 0.76 | 2.00 |
| Pedal cyclist injured in collision | 96 | 1.1 | 54 | 1.0 | 1.02 | 0.73 | 1.41 |
| Motorcycle rider injured in collision | 46 | 2.5 | 25 | 2.0 | 1.05 | 0.65 | 1.71 |
| Car occupant injured in collision with pedestrian or animal | 105 | 0.2 | 49 | 0.2 | 1.22 | 0.88 | 1.71 |
| Occupant of pick-up truck or van injured in collision with pedestrian or animal | 7 | 0.0 | 5 | 0.0 | 0.80 | 0.25 | 2.52 |
| Other communication injuries. | 2 | 39.5 | 1 | 37.0 | 1.14 | 0.10 | 12.59 |
| Fall on same level | 1674 | 6.2 | 895 | 7.0 | 1.07 | 1.00 | 1.14 |
| Fall on and from height | 264 | 2.4 | 169 | 2.0 | 0.89 | 0.74 | 1.07 |
| Assaulted by another person | 101 | 0.2 | 49 | 0.3 | 1.18 | 0.84 | 1.65 |
| Intentional self-harm | 7 | 1.6 | 7 | 1.0 | 0.57 | 0.20 | 1.63 |
| Attacked by an animal | 66 | 3.0 | 25 | 3.1 | 1.51 | 0.95 | 2.38 |
| Contact with lifting and transmission devices | 126 | 11.1 | 76 | 10.4 | 0.95 | 0.72 | 1.25 |
| Struck by thrown, projected, or falling object | 471 | 1.1 | 251 | 1.5 | 1.07 | 0.93 | 1.24 |
| Exposure to high or low temperature, high or low pressure, electric current, forces of nature | 47 | 27.7 | 37 | 31.1 | 0.73 | 0.47 | 1.11 |
| Other causes | 1172 | 1.2 | 752 | 1.0 | 0.89 | 0.82 | 0.96 |
| Mechanism of injury—general category | |||||||
| Communication injuries | 308 | 10.1 | 158 | 9.5 | 1.06 | 0.88 | 1.27 |
| Non-communication injuries | 2756 | 89.9 | 1509 | 90.5 | 0.99 | 0.97 | 1.01 |
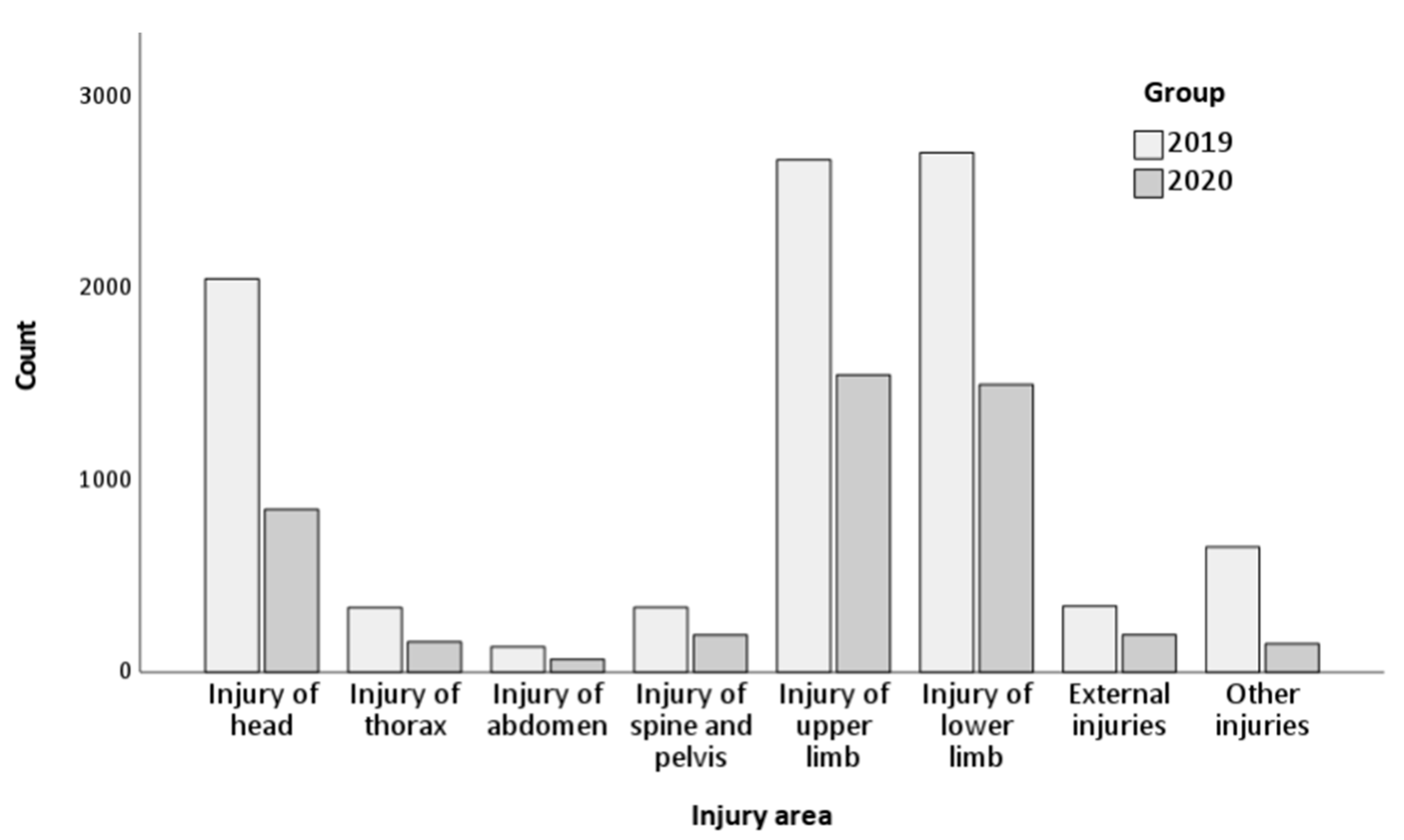
| Variable | 2019 | 2020 | RR | 95% CI | |||
|---|---|---|---|---|---|---|---|
| n | % | n | % | LL | UL | ||
| Area of injury | |||||||
| Injury of head | 2048 | 22.2 | 847 | 18.2 | 1.22 | 1.14 | 1.31 |
| Injury of thorax | 336 | 3.6 | 158 | 3.4 | 1.07 | 0.89 | 1.29 |
| Injury of abdomen | 132 | 1.4 | 67 | 1.4 | 0.99 | 0.74 | 1.33 |
| Injury of spine and pelvis | 337 | 3.7 | 194 | 4.2 | 0.88 | 0.74 | 1.04 |
| Injury of upper limb | 2669 | 28.9 | 1547 | 33.2 | 0.87 | 0.83 | 0.92 |
| Injury of lower limb | 2706 | 29.3 | 1498 | 32.2 | 0.91 | 0.87 | 0.96 |
| External injuries | 344 | 3.7 | 195 | 4.2 | 0.89 | 0.75 | 1.06 |
| Other injuries | 651 | 7.1 | 148 | 3.2 | 2.22 | 1.86 | 2.64 |
| Variable | 2019 | 2020 | RR | 95% CI | |||
|---|---|---|---|---|---|---|---|
| n | % | n | % | LL | UL | ||
| Primary diagnosis | |||||||
| Superficial injury of head | 225 | 6.62 | 16 | 1.06 | 6.25 | 3.78 | 10.35 |
| Superficial injury of scalp | 256 | 7.53 | 118 | 7.80 | 0.96 | 0.78 | 1.19 |
| Superficial injury of head, part unspecified | 117 | 3.44 | 36 | 2.38 | 1.45 | 1.00 | 2.09 |
| Open wound of scalp | 196 | 5.76 | 125 | 8.27 | 0.70 | 0.56 | 0.87 |
| Fracture of nasal bones | 146 | 4.29 | 47 | 3.11 | 1.38 | 1.00 | 1.91 |
| Dislocation of shoulder joint | 87 | 2.56 | 63 | 4.17 | 0.61 | 0.45 | 0.84 |
| Fracture of lower end of radius | 280 | 8.24 | 164 | 10.85 | 0.76 | 0.63 | 0.91 |
| Fracture of lower end of both ulna and radius | 84 | 2.47 | 59 | 3.90 | 0.63 | 0.46 | 0.88 |
| Open wound of finger(s) w/o damage to nail | 215 | 6.32 | 102 | 6.75 | 0.94 | 0.75 | 1.18 |
| Open wound of other parts of wrist and hand | 97 | 2.85 | 64 | 4.23 | 0.67 | 0.49 | 0.92 |
| Fracture of other finger | 124 | 3.65 | 69 | 4.56 | 0.80 | 0.60 | 1.07 |
| Fracture of neck of femur | 224 | 6.59 | 164 | 10.85 | 0.61 | 0.50 | 0.74 |
| Pertrochanteric fracture | 179 | 5.26 | 137 | 9.06 | 0.58 | 0.47 | 0.72 |
| Multiple fractures of lower leg | 141 | 4.15 | 74 | 4.89 | 0.85 | 0.64 | 1.12 |
| Sprain and strain of other and unspec. Parts of knee | 115 | 3.38 | 43 | 2.84 | 1.19 | 0.84 | 1.68 |
| Sprain and strain of ankle | 230 | 6.76 | 116 | 7.67 | 0.88 | 0.71 | 1.09 |
| Foreign body in cornea | 215 | 6.32 | 7 | 0.46 | 13.66 | 6.45 | 28.93 |
| Foreign body in conjunctival sac | 144 | 4.24 | 0 | 0.00 | n/a | n/a | n/a |
| Toxic effect of alcohol | 133 | 3.91 | 79 | 5.22 | 0.75 | 0.57 | 0.98 |
| Sequelae of other fractures of lower limb | 192 | 5.65 | 29 | 1.92 | 2.94 | 2.00 | 4.33 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jojczuk, M.; Pawlikowski, J.; Kamiński, P.; Głuchowski, D.; Naylor, K.; Gajewski, J.; Karpiński, R.; Krakowski, P.; Jonak, J.; Nogalski, A.; et al. Evaluating Changes in Trauma Epidemiology during the COVID-19 Lockdown: Insights and Implications for Public Health and Disaster Preparedness. Healthcare 2023, 11, 2436. https://doi.org/10.3390/healthcare11172436
Jojczuk M, Pawlikowski J, Kamiński P, Głuchowski D, Naylor K, Gajewski J, Karpiński R, Krakowski P, Jonak J, Nogalski A, et al. Evaluating Changes in Trauma Epidemiology during the COVID-19 Lockdown: Insights and Implications for Public Health and Disaster Preparedness. Healthcare. 2023; 11(17):2436. https://doi.org/10.3390/healthcare11172436
Chicago/Turabian StyleJojczuk, Mariusz, Jakub Pawlikowski, Piotr Kamiński, Dariusz Głuchowski, Katarzyna Naylor, Jakub Gajewski, Robert Karpiński, Przemysław Krakowski, Józef Jonak, Adam Nogalski, and et al. 2023. "Evaluating Changes in Trauma Epidemiology during the COVID-19 Lockdown: Insights and Implications for Public Health and Disaster Preparedness" Healthcare 11, no. 17: 2436. https://doi.org/10.3390/healthcare11172436
APA StyleJojczuk, M., Pawlikowski, J., Kamiński, P., Głuchowski, D., Naylor, K., Gajewski, J., Karpiński, R., Krakowski, P., Jonak, J., Nogalski, A., & Czerwiński, D. (2023). Evaluating Changes in Trauma Epidemiology during the COVID-19 Lockdown: Insights and Implications for Public Health and Disaster Preparedness. Healthcare, 11(17), 2436. https://doi.org/10.3390/healthcare11172436