

Characteristics of COVID-19 Patients Admitted to Intensive Care Unit in Multispecialty Hospital of Riyadh, Saudi Arabia: A Retrospective Study

 and
and
Abstract
:1. Introduction
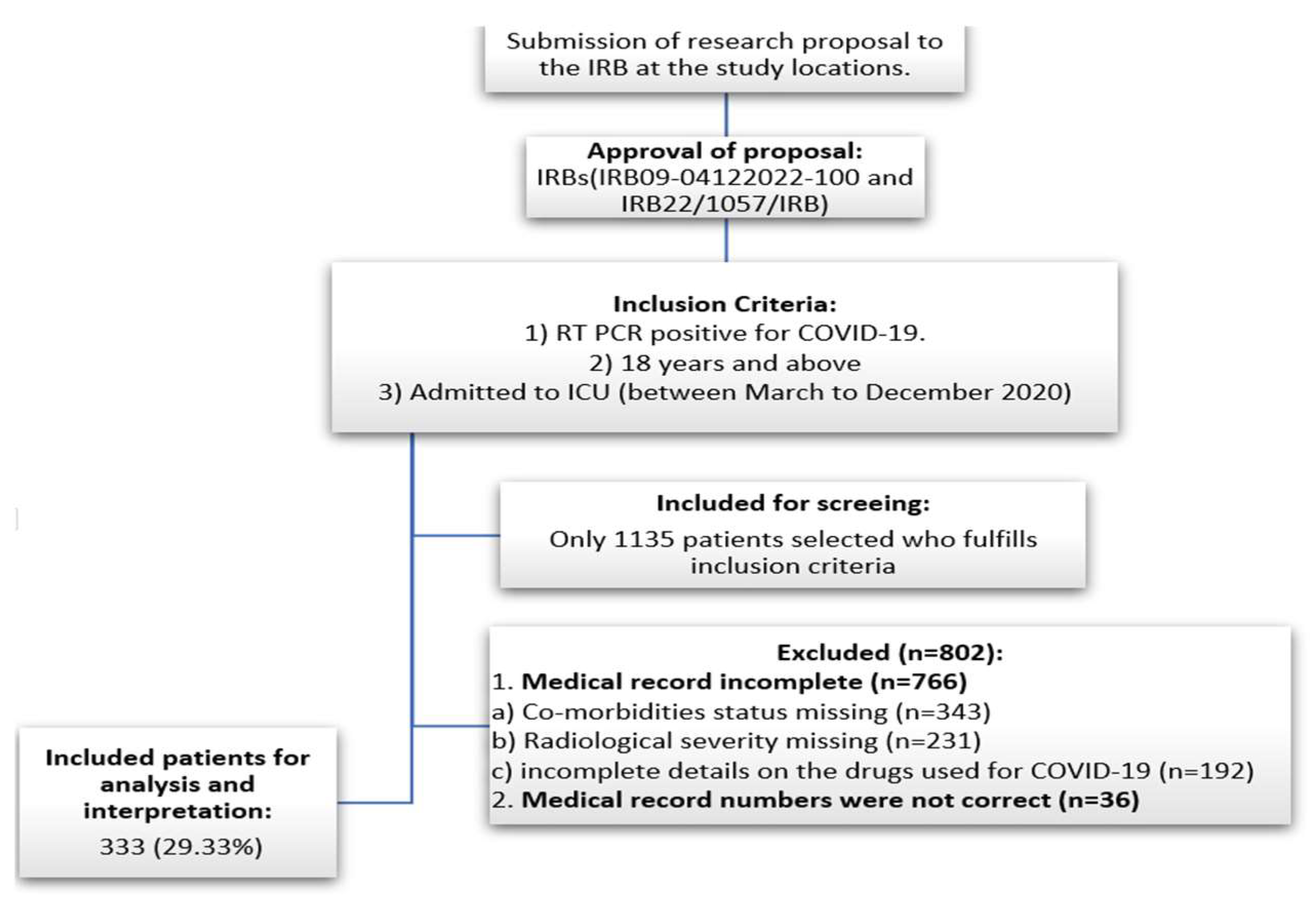
2. Materials and Methods
2.1. Study Design and Settings
2.2. Data Collection
2.3. Data Analysis
3. Results
3.1. Demographic Characteristics of the Patients
3.2. Baseline Characteristics of the Patients
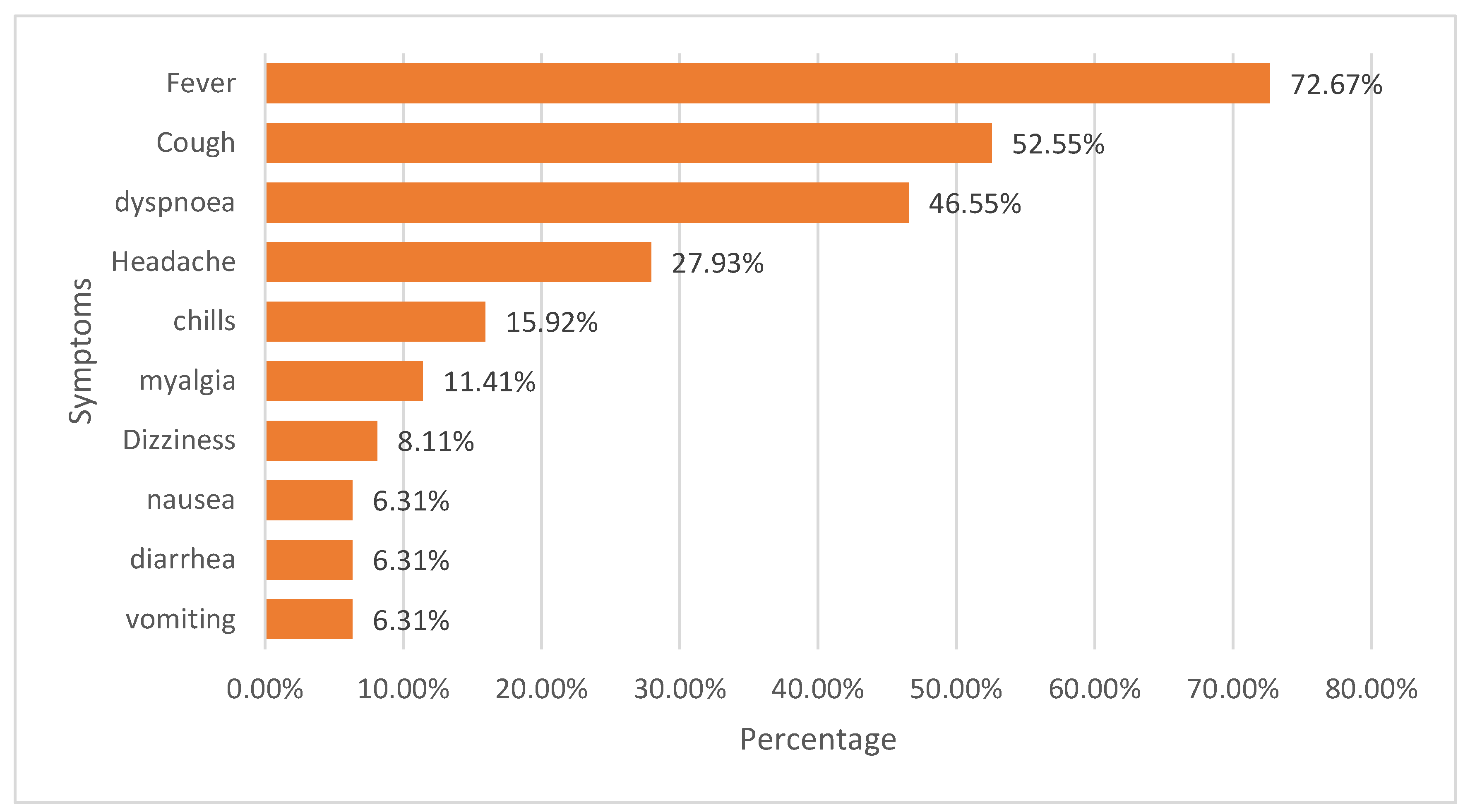
3.3. COVID-19 Symptoms of The patients
3.4. Status of Comorbidities of the Patients
3.5. Description of Medications Used for Managing Comorbidities
3.6. Description of Drugs Used for Managing COVID-19
3.7. General Observations during Hospitalization and Follow-up
3.8. Characteristics of Intubated Patients
3.9. Characteristics of Deceased Patients
3.10. Predictors for Fatality in COVID-19 Patients
3.11. Predictors for Intubation in COVID-19 Patients
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Alkhamees, A.A.; Alrashed, S.A.; Alzunaydi, A.A.; Almohimeed, A.S.; Aljohani, M.S. The psychological impact of COVID-19 pandemic on the general population of Saudi Arabia. Compr. Psychiatry 2020, 102, 152192. [Google Scholar] [CrossRef] [PubMed]
- Alanagreh, L.A.; Alzoughool, F.; Atoum, M. The Human Coronavirus Disease COVID-19: Its Origin, Characteristics, and Insights into Potential Drugs and Its Mechanisms. Pathogens 2020, 9, 331. [Google Scholar] [CrossRef] [PubMed]
- Grant, M.C.; Geoghegan, L.; Arbyn, M.; Mohammed, Z.; McGuinness, L.; Clarke, E.L.; Wade, R.G. The prevalence of symptoms in 24,410 adults infected by the novel coronavirus (SARS-CoV-2; COVID-19): A systematic review and meta-analysis of 148 studies from 9 countries. PLoS ONE 2020, 15, e0234765. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Morales, A.J.; Cardona-Ospina, J.A.; Gutiérrez-Ocampo, E.; Villamizar-Peña, R.; Holguin-Rivera, Y.; Escalera-Antezana, J.P.; Alvarado-Arnez, L.E.; Bonilla-Aldana, D.K.; Franco-Paredes, C.; Henao-Martinez, A.F.; et al. Clinical, laboratory and imaging features of COVID-19: A systematic review and meta-analysis. Travel Med. Infect. Dis. 2020, 34, 101623. [Google Scholar] [CrossRef]
- Alamer, A.; Asdaq, S.M.; Al Yamani, M.; Al Ghadeer, H.; Alnasser, Z.H.; Aljassim, Z.; Albattat, M.; Alhajji, A.; Alrashed, A.; Mohzari, Y.; et al. Characteristics of mechanically ventilated COVID-19 patients in the Al-Ahsa Region of Saudi Arabia: A retro-spective study with survival analysis. Ann. Saudi Med. 2022, 42, 165–173. [Google Scholar] [CrossRef]
- Gibson, P.G.; Qin, L.; Puah, S.H. COVID-19 acute respiratory distress syndrome (ARDS): Clinical features and differences from typical pre-COVID-19 ARDS. Med. J. Aust. 2020, 213, 54–56. [Google Scholar] [CrossRef]
- Swenson, K.E.; Swenson, E.R. Pathophysiology of Acute Respiratory Distress Syndrome and COVID-19 Lung Injury. Crit. Care Clin. 2021, 37, 749–776. [Google Scholar] [CrossRef]
- Huang, S.; Vieillard-Baron, A.; Evrard, B.; Prat, G.; Chew, M.S.; Balik, M.; Clau-Terré, F.; De Backer, D.; Dessap, A.M.; Orde, S.; et al. Echocardiography phenotypes of right ventricular involvement in COVID-19 ARDS patients and ICU mortality: Post-hoc (exploratory) analysis of repeated data from the ECHO-COVID study. Intensiv. Care Med. 2023, 49, 946–956. [Google Scholar] [CrossRef]
- La Via, L.; Dezio, V.; Santonocito, C.; Astuto, M.; Morelli, A.; Huang, S.; Vieillard-Baron, A.; Sanfilippo, F. Full and simplified assessment of left ventricular diastolic function in Covid-19 patients admitted to ICU: Feasibility, incidence, and association with mortality. Echocardiography 2022, 39, 1391–1400. [Google Scholar] [CrossRef]
- Hilton, J.; Boyer, N.; Nadim, M.K.; Forni, L.G.; Kellum, J.A. COVID-19 and Acute Kidney Injury. Crit. Care Clin. 2022, 38, 473–489. [Google Scholar] [CrossRef]
- Sanfilippo, F.; Martucci, G.; La Via, L.; Cuttone, G.; Dimarco, G.; Pulizzi, C.; Arcadipane, A.; Astuto, M. Hemoperfusion and blood purification strategies in patients with COVID-19: A systematic review. Artif. Organs 2021, 45, 1466–1476. [Google Scholar] [CrossRef] [PubMed]
- Boonyasai, R.T.; Murthy, V.K.; Liu, G.Y.-G.; Garibaldi, B.T.; Brotman, D.J.; Streiff, M.B.; Omron, R. Venous Thromboembolism in Hospitalized Patients With COVID-19 Receiving Prophylactic Anticoagulation. Mayo Clin. Proc. 2020, 95, 2291–2293. [Google Scholar] [CrossRef] [PubMed]
- Colantuoni, A.; Martini, R.; Caprari, P.; Ballestri, M.; Capecchi, P.L.; Gnasso, A.; Presti, R.L.; Marcoccia, A.; Rossi, M.; Caimi, G. COVID-19 Sepsis and Microcirculation Dysfunction. Front. Physiol. 2020, 11, 747. [Google Scholar] [CrossRef] [PubMed]
- Martins-Filho, P.R.; Tavares, C.S.S.; Santos, V.S. Factors associated with mortality in patients with COVID-19. A quantitative evidence synthesis of clinical and laboratory data. Eur. J. Intern. Med. 2020, 76, 97–99. [Google Scholar] [CrossRef] [PubMed]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Drager, L.F.; Pio-Abreu, A.; Lopes, R.D.; Bortolotto, L.A. Is Hypertension a Real Risk Factor for Poor Prognosis in the COVID-19 Pandemic? Curr. Hypertens. Rep. 2020, 22, 43. [Google Scholar] [CrossRef]
- Petrilli, C.M.; Jones, S.A.; Yang, J.; Rajagopalan, H.; O’Donnell, L.; Chernyak, Y.; Tobin, K.A.; Cerfolio, R.J.; Francois, F.; Horwitz, L.I. Factors associated with hospital admission and critical illness among 5279 people with coronavirus disease 2019 in New York City: Prospective cohort study. BMJ 2020, 369, m1966. [Google Scholar] [CrossRef]
- Palaiodimos, L.; Kokkinidis, D.G.; Li, W.; Karamanis, D.; Ognibene, J.; Arora, S.; Southern, W.N.; Mantzoros, C.S. Severe obesity, increasing age and male sex are independently associated with worse in-hospital outcomes, and higher in-hospital mortality, in a cohort of patients with COVID-19 in the Bronx, New York. Metabolism 2020, 108, 154262. [Google Scholar] [CrossRef]
- Hur, K.; Price, C.P.E.; Gray, E.L.; Gulati, R.K.; Maksimoski, M.; Racette, S.D.; Schneider, A.L.; Khanwalkar, A.R. Factors Associated With Intubation and Prolonged Intubation in Hospitalized Patients With COVID-19. Otolaryngol. Neck Surg. 2020, 163, 170–178. [Google Scholar] [CrossRef]
- Chen, R.; Liang, W.; Jiang, M.; Guan, W.; Zhan, C.; Wang, T. Risk factors of fatal outcome in hospitalized subjects with coro-navirus disease 2019 from a nationwide analysis in China. Chest 2020, 158, 97–105. [Google Scholar] [CrossRef]
- Zhao, Q.; Meng, M.; Kumar, R.; Wu, Y.; Huang, J.; Lian, N.; Lin, S.; Deng, Y. The impact of COPD and smoking 13. history on the severity of COVID-19: A systemic review and meta-analysis. J. Med. Virol. 2020, 92, 1915–1921. [Google Scholar] [CrossRef]
- Kammar-García, A.; Vidal-Mayo, J.D.; Vera-Zertuche, J.M.; Lazcano-Hernández, M.; Vera-López, O.; Segura-Badilla, O.; Aguilar-Alonso, P.; Navarro-Cruz, A.R. Impact of comorbidities in Mexican SARS-CoV-2-positive patients: A retrospective analysis in a national cohort. Rev. Investig. Clin. 2020, 72, 151–158. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.-J.; Dong, X.; Liu, G.-H.; Gao, Y.-D. Risk and Protective Factors for COVID-19 Morbidity, Severity, and Mortality. Clin. Rev. Allergy Immunol. 2023, 64, 90–107. [Google Scholar] [CrossRef] [PubMed]
- The Government of Saudi Arabia, Riyadh. The Kingdom of Saudi Arabia’s Experience in Health Preparedness and Response to COVID-19 Pandemic; MOH Publications: Riyadh, Saudi Arabia, 2020.
- Khan, A.; Alsofayan, Y.; Alahmari, A.; Alowais, J.; Algwizani, A.; Alserehi, H.; Assiri, A.; Jokhdar, H. COVID-19 in Saudi Arabia: The national health response. East. Mediterr. Health J. 2021, 27, 1114. [Google Scholar] [CrossRef] [PubMed]
- Mietzner, M. Populist Anti-Scientism, Religious Polarisation, and Institutionalised Corruption: How Indonesia’s Democratic Decline Shaped Its COVID-19 Response. J. Curr. Southeast Asian Aff. 2020, 39, 227–249. [Google Scholar] [CrossRef]
- Albano, P.M.; Notarte, K.I.; Macaranas, I.; Maralit, B. Cross-contamination in molecular diagnostic laboratories in low-and mid-dle-income countries. PJP 2020, 5, 7–11. [Google Scholar] [CrossRef]
- Aljondi, R.; Alghamdi, S.; Tajaldeen, A.; Abdelaziz, I.; Bushara, L.; Alghamdi, H.A.; Alhinishi, H.; Alharbi, B.; Alshehri, R.; Aljehani, A.; et al. Chest Radiological Findings and Clinical Characteristics of Laboratory-Confirmed COVID-19 Patients from Saudi Arabia. Med. Sci. Monit. Int. Med. J. Exp. Clin. Res. 2021, 27, e932441-1–e932441-9. [Google Scholar] [CrossRef]
- Assiri, R.A.; Bepari, A.; Patel, W.; Hussain, S.A.; Niazi, S.K.; Alshangiti, A.; Alshangiti, S.A.; Cordero, M.A.W.; Sheereen, S. Exploration of Sex and Age-Based Associations in Clinical Characteristics, Predictors of Severity, and Duration of Stay among COVID-19 Patients at the University Hospital of Saudi Arabia. Healthcare 2023, 11, 751. [Google Scholar] [CrossRef]
- Ibrahim, M.E.; Al-Aklobi, O.S.; Abomughaid, M.M.; Al-Ghamdi, M.A. Epidemiological, clinical, and laboratory findings for patients of different age groups with confirmed coronavirus disease 2019 (COVID-19) in a hospital in Saudi Arabia. PLoS ONE 2021, 16, e0250955. [Google Scholar] [CrossRef]
- Bairwa, M.; Kumar, R.; Beniwal, K.; Kalita, D.; Bahurupi, Y. Hematological profile and biochemical markers of COVID-19 non-survivors: A retrospective analysis. Clin. Epidemiology Glob. Health 2021, 11, 100770. [Google Scholar] [CrossRef]
- Ghaith, M.M.; Albanghali, M.A.; Aldairi, A.F.; Iqbal, M.S.; Almaimani, R.A.; AlQuthami, K.; Alqasmi, M.H.; Almaimani, W.; El-Readi, M.Z.; Alghamdi, A.; et al. Potential Predictors of Poor Prognosis among Severe COVID-19 Patients: A Single-Center Study. Can. J. Infect. Dis. Med. Microbiol. 2021, 2021, 6656092. [Google Scholar] [CrossRef] [PubMed]
- Kantri, A.; Ziati, J.; Khalis, M.; Haoudar, A.; El Aidaoui, K.; Daoudi, Y.; Chikhaoui, I.; El Yamani, K.; Mouhaoui, M.; El Bak-kouri, J.; et al. Hematological and biochemical abnormalities associated with severe forms of COVID-19: A retrospective sin-gle-center study from Morocco. PLoS ONE 2021, 16, e0246295. [Google Scholar] [CrossRef] [PubMed]
- Available online: https://www.arabnews.com/node/1778286/saudi-arabia (accessed on 25 August 2023).
- MOH. COVID-19 Statistics E-Platform. Available online: https://covid19.moh.gov.sa/ (accessed on 15 February 2023).
- Li, L.Q.; Huang, T.; Wang, Y.Q.; Wang, Z.P.; Liang, Y.; Huang, T.B.; Zhang, H.Y.; Sun, W.; Wang, Y. COVID-19 patients’ clinical characteristics, discharge rate, and fatality rate of meta-analysis. J. Med. Virol. 2020, 92, 577–583. [Google Scholar] [CrossRef]
- Xia, W.; Shao, J.; Guo, Y.; Peng, X.; Li, Z.; Hu, D. Clinical and CT features in pediatric patients with COVID-19 infection: Different points from adults. Pediatr. Pulmonol. 2020, 55, 1169–1174. [Google Scholar] [CrossRef] [PubMed]
- Channappanavar, R.; Fett, C.; Mack, M.; Ten Eyck, P.P.; Meyerholz, D.K.; Perlman, S. Sex-Based Differences in Susceptibility to Severe Acute Respiratory Syndrome Coronavirus Infection. J. Immunol. 2017, 198, 4046–4053. [Google Scholar] [CrossRef]
- Badawi, A.; Ryoo, S.G. Prevalence of comorbidities in the Middle East respiratory syndrome coronavirus (MERS-CoV): A systematic review and meta-analysis. Int. J. Infect. Dis. 2016, 49, 129–133. [Google Scholar] [CrossRef]
- Bwire, G.M. Coronavirus: Why Men are More Vulnerable to COVID-19 Than Women? SN Compr. Clin. Med. 2020, 2, 874–876. [Google Scholar] [CrossRef]
- Hippisley-Cox, J.; Young, D.; Coupland, C.; Channon, K.M.; San Tan, P.; Harrison, D.A.; Rowan, K.; Aveyard, P.; Watkinson, P.J. Risk of severe COVID-19 disease with ACE inhibitors and angiotensin receptor blockers: Cohort study including 8.3 million people. Heart 2020, 106, 1503–1511. [Google Scholar] [CrossRef]
- Alrashed, A.A.; Khan, T.M.; Alhusseini, N.K.; Asdaq, S.M.B.; Enani, M.; Alosaimi, B.; Alkhani, N.M.; Mohzari, Y.; Alghalbi, M.M.; Alfahad, W.; et al. Severity of COVID-19 infection in ACEI/ARB users in specialty hospitals: A retrospective cohort study. J. Infect. Public Health 2021, 14, 726–733. [Google Scholar] [CrossRef]
- Ñamendys-Silva, S.A.; Gutiérrez-Villaseñor, A.; Romero-González, J.P. Hospital mortality in mechanically ventilated COVID-19 patients in Mexico. Intensiv. Care Med. 2020, 46, 2086–2088. [Google Scholar] [CrossRef]
- Peñuelas, O.; del Campo-Albendea, L.; de Aledo, A.L.G.; Añón, J.M.; Rodríguez-Solís, C.; Mancebo, J.; Frutos-Vivar, F. Long-Term Survival of Mechanically Ventilated Patients with Severe COVID-19: An Observational Cohort Study. Ann. Intensive Care 2021, 11, 143. [Google Scholar] [CrossRef] [PubMed]
- Arabi, Y.M.; Al Aseri, Z.; Alaama, T.; Alqahtani, A.; Alharthy, A.; Almotairi, A.; Al Qasim, E.; Alzahrani, A.; Al Qarni, M.; Abdukahil, S.A.; et al. National Approach to Standardize and Improve Mechanical Ventilation. Ann. Thorac. Med. 2019, 14, 101–105. [Google Scholar] [CrossRef] [PubMed]
- The Government of Saudi Arabia, Riyadh. Key Health Indicators 2021; MOH Publications: Riyadh, Saudi Arabia, 2021.
- Qureshi, A.Z.; Ullah, S.; Ullah, R. The trend of hospital accreditation in the Kingdom of Saudi Arabia. Saudi Med. J. 2012, 33, 1350–1351. [Google Scholar] [PubMed]
- Amodio, E.; Genovese, D.; Fallucca, A.; Ferro, P.; Sparacia, B.; D’azzo, L.; Fertitta, A.; Maida, C.M.; Vitale, F. Clinical Severity in Different Waves of SARS-CoV-2 Infection in Sicily: A Model of Smith’s “Law of Declining Virulence” from Real-World Data. Viruses 2022, 15, 125. [Google Scholar] [CrossRef]
- Khan, A.; Althunayyan, S.; Alsofayan, Y.; Alotaibi, R.; Mubarak, A.; Arafat, M.; Assiri, A.; Jokhdar, H. Risk factors associated with worse outcomes in COVID-19: A retrospective study in Saudi Arabia. East. Mediterr. Health J. 2020, 26, 1371–1380. [Google Scholar] [CrossRef]
- Rosenthal, N.; Cao, Z.; Gundrum, J.; Sianis, J.; Safo, S. Risk Factors Associated With In-Hospital Mortality in a US National Sample of Patients With COVID-19. JAMA Netw. Open 2020, 3, e2029058, Erratum in JAMA Netw. Open 2021, 1, e2036103. [Google Scholar] [CrossRef]
- Williamson, E.J.; Walker, A.J.; Bhaskaran, K.; Bacon, S.; Bates, C.; Morton, C.E.; Curtis, H.J.; Mehrkar, A.; Evans, D.; Inglesby, P.; et al. Factors associated with COVID-19-related death using OpenSAFELY. Nature 2020, 584, 430–436. [Google Scholar] [CrossRef]
- Yang, Y.; Cai, Z.; Zhang, J. Insulin Treatment May Increase Adverse Outcomes in Patients With COVID-19 and Diabetes: A Systematic Review and Meta-Analysis. Front. Endocrinol. 2021, 12, 696087. [Google Scholar] [CrossRef]
- Yuengsrigul, A.; Chin, T.W.; Nussbaum, E. Decreased Cytokine Production from Human Peripheral Blood Mononuclear Cells(Pbmcs) by Furosemide. 77. Pediatr. Res. 1996, 39, 15. [Google Scholar] [CrossRef]
- Brennecke, A.; Villar, L.; Wang, Z.; Doyle, L.; Meek, A.; Reed, M.; Barden, C.; Weaver, D. Is Inhaled Furosemide A Potential Therapeutic For COVID-19? Am. J. Med. Sci. 2020, 360, 216–221. [Google Scholar] [CrossRef]
- Alhandod, T.A.; Rabbani, S.I.; Almuqbil, M.; Alshehri, S.; Hussain, S.A.; Alomar, N.F.; Mir, M.A.; Asdaq, S.M.B. A Systematic Review on the Safety and Efficacy of COVID-19 Vaccines Approved in Saudi Arabia. Vaccines 2023, 11, 281. [Google Scholar] [CrossRef] [PubMed]
- Notarte, K.I.; Catahay, J.A.; Peligro, P.J.; Velasco, J.V.; Ver, A.T.; Guerrero, J.J.; Liu, J.; Lippi, G.; Benoit, S.W.; Henry, B.M.; et al. Humoral Response in Hemodialysis Patients Post-SARS-CoV-2 mRNA Vaccination: A Systematic Review of Literature. Vaccines 2023, 11, 724. [Google Scholar] [CrossRef] [PubMed]
- Notarte, K.I.; Catahay, J.A.; Velasco, J.V.; Pastrana, A.; Ver, A.T.; Pangilinan, F.C.; Peligro, P.J.; Casimiro, M.; Guerrero, J.J.; Gellaco, M.M.L.; et al. Impact of COVID-19 vaccination on the risk of developing long-COVID and on existing long-COVID symptoms: A systematic review. eClinicalMedicine 2022, 53, 101624. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristics | Variables | Number (%) | p Value * |
|---|---|---|---|
| Age (years) | ≤50 | 173 (52) | 0.645 |
| >50 | 160 (48) | ||
| BMI | ≤25 | 151 (45) | 0.382 |
| >25 | 182 (55) | ||
| Ethnicity | White | 299 (90) | 0.001 |
| Black | 30 (9) | ||
| Others | 04 (1) | ||
| Gender | Male | 255 (77) | 0.001 |
| Female | 78 (23) | ||
| Smoking | Yes | 38 (11) | 0.001 |
| No | 295 (89) |
| Characteristics | Variables | Frequency | Percentage | p Value * |
|---|---|---|---|---|
| Need for the nasal cannula | Yes | 150 | 45.05% | 0.341 |
| No | 183 | 54.95% | ||
| Need for high-flow oxygen on admission | Yes | 58 | 17.42% | 0.001 |
| No | 275 | 82.58% | ||
| Need for intubation on admission. | Yes | 63 | 18.92% | 0.001 |
| No | 270 | 81.08% | ||
| Radiological severity of patients | Mild | 179 | 53.75% | 0.041 |
| Moderate | 100 | 30.03% | ||
| Severe | 45 | 13.51% | ||
| Very Severe | 9 | 2.70% |
| Characteristics | Intubated (63), n (%) | Non-Intubated (270), n (%) | p Value * |
|---|---|---|---|
| Age (years) | 0.067 | ||
| ≥50 | 37 (58.73) | 122 (45.18) | |
| ˂50 | 26 (41.26) | 148 (54.81) | |
| Gender | 0.156 | ||
| Male | 49 (77.77) | 206 (76.29) | |
| Female | 14 (22.22) | 64 (23.70) | |
| Smoking status | 0.132 | ||
| Yes | 5 (7.93) | 33 (12.22) | |
| No | 58 (92.06) | 237 (87.77) | |
| Chronic disease status | 0.032 | ||
| Diabetes | 36 (57.14) | 96 (35.55) | |
| Hypertension | 31 (49.20) | 74 (27.40) | |
| Asthma | 08 (12.69) | 37 (13.70) | |
| Established cardiovascular diseases | 08 (12.69) | 06 (2.22) | |
| Radiological severity | 0.021 | ||
| Mild | 10 (15.87) | 169 (62.59) | |
| Moderate | 21 (33.33) | 79 (29.25) | |
| Severe | 24 (38.09) | 21 (7.77) | |
| Very severe | 08 (12.69) | 01 (.37) | |
| Mortality status | 0.049 | ||
| Yes | 13 (20.63) | 09 (3.33) | |
| No | 50 (79.36) | 261 (96.66) | |
| Characteristics | Deceased (22), n (%) | Discharged (311), n (%) | p Value * |
|---|---|---|---|
| Age (years) | 0.078 | ||
| ≥50 | 13 (59.09) | 146 (46.94) | |
| ˂50 | 09 (40.90) | 165 (53.05) | |
| Gender | 0.039 | ||
| Male | 20 (90.90) | 235 (75.56) | |
| Female | 02 (9.10) | 76 (24.43) | |
| Smoking status | 0.001 | ||
| Yes | 09 (40.90) | 29 (9.37) | |
| No | 13 (59.09) | 282 (90.67) | |
| Chronic disease status | 0.022 | ||
| Diabetes | 12 (54.54) | 119(38.26) | |
| Hypertension | 12 (54.54) | 94 (30.22) | |
| Asthma | 04 (18.18) | 41 (13.18) | |
| Established cardiovascular diseases | 08 (36.36) | 06 (1.92) | |
| Radiological severity | 0.011 | ||
| Mild | 04 (18.18) | 175 (56.27) | |
| Moderate | 02 (9.10) | 98 (31.51) | |
| Severe | 10 (45.45) | 35 (11.25) | |
| Very severe | 06 (27.27) | 03 (.96) | |
| Characteristics | Odds Ratio | Confidence Interval | p Value | |
|---|---|---|---|---|
| Lower | Upper | |||
| Sex | 3.42 | 2.38 | 5.49 | 0.021 |
| Intubation | 1.67 | 1.21 | 2.34 | 0.034 |
| Diabetes and hypertension | 7.85 | 4.31 | 9.32 | 0.001 |
| Diabetes | 5.43 | 3.21 | 7.21 | 0.001 |
| Hypertension | 4.21 | 2.98 | 5.32 | 0.001 |
| Established CV diseases | 3.81 | 2.87 | 5.98 | 0.001 |
| Smoking | 4.32 | 2.11 | 6.21 | 0.001 |
| Characteristics | Odds Ratio | Confidence Interval | p Value | |
|---|---|---|---|---|
| Lower | Upper | |||
| Sex | 2.92 | 1.88 | 3.69 | 0.021 |
| Diabetes and hypertension | 6.29 | 4.98 | 8.22 | 0.001 |
| Diabetes | 5.64 | 3.66 | 6.55 | 0.001 |
| Hypertension | 4.71 | 2.83 | 5.72 | 0.001 |
| Established CV diseases | 1.91 | 1.07 | 2.76 | 0.001 |
| Insulin | 3.93 | 2.79 | 5.77 | 0.001 |
| Furosemide | 3.65 | 2.81 | 4.89 | 0.001 |
| Age more than 50 years | 1.81 | 1.76 | 3.21 | 0.034 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Almuqbil, M.; Almoteer, A.I.; Suwayyid, A.M.; Bakarman, A.H.; Alrashed, R.F.; Alrobish, M.; Alasalb, F.; Alhusaynan, A.A.; Alnefaie, M.H.; Altayar, A.S.; et al. Characteristics of COVID-19 Patients Admitted to Intensive Care Unit in Multispecialty Hospital of Riyadh, Saudi Arabia: A Retrospective Study. Healthcare 2023, 11, 2500. https://doi.org/10.3390/healthcare11182500
Almuqbil M, Almoteer AI, Suwayyid AM, Bakarman AH, Alrashed RF, Alrobish M, Alasalb F, Alhusaynan AA, Alnefaie MH, Altayar AS, et al. Characteristics of COVID-19 Patients Admitted to Intensive Care Unit in Multispecialty Hospital of Riyadh, Saudi Arabia: A Retrospective Study. Healthcare. 2023; 11(18):2500. https://doi.org/10.3390/healthcare11182500
Chicago/Turabian StyleAlmuqbil, Mansour, Ali Ibrahim Almoteer, Alwaleed Mohammed Suwayyid, Abdulaziz Hussain Bakarman, Raed Fawaz Alrashed, Majed Alrobish, Fahad Alasalb, Abdulaziz Abdulrahman Alhusaynan, Mohammed Hadi Alnefaie, Abdullah Saud Altayar, and et al. 2023. "Characteristics of COVID-19 Patients Admitted to Intensive Care Unit in Multispecialty Hospital of Riyadh, Saudi Arabia: A Retrospective Study" Healthcare 11, no. 18: 2500. https://doi.org/10.3390/healthcare11182500
APA StyleAlmuqbil, M., Almoteer, A. I., Suwayyid, A. M., Bakarman, A. H., Alrashed, R. F., Alrobish, M., Alasalb, F., Alhusaynan, A. A., Alnefaie, M. H., Altayar, A. S., Alobid, S. E., Almadani, M. E., Alshehri, A., Alghamdi, A., & Asdaq, S. M. B. (2023). Characteristics of COVID-19 Patients Admitted to Intensive Care Unit in Multispecialty Hospital of Riyadh, Saudi Arabia: A Retrospective Study. Healthcare, 11(18), 2500. https://doi.org/10.3390/healthcare11182500