Abstract
In Ireland, the extent of outpatient orthopedic waiting lists results in long waiting times for patients, delays in processing referrals, and variation in the consultant caseload. At the study site, the Define, Measure, Analyze, Improve, and Control (DMAIC) Lean Six Sigma framework was applied to evaluate sources of Non-Value-Added (NVA) activity in the process of registering and triaging patients referred to the trauma orthopedic service from the Emergency Department. A pre- (October–December 2021)/post- (April–August 2022) intervention design was employed, utilizing Gemba, Process Mapping, and the TIMWOODS tool. Embracing a person-centered approach, stakeholder Voice of Customer feedback was sought at each stage of the improvement process. Following data collection and analysis, a co-designed pilot intervention (March 2022) was implemented, consisting of a new triage template, dedicated trauma clinic slots, a consultant triage roster, and a new option to refer directly to physiotherapy services. This resulted in the total wait time of patients for review being reduced by 34%, a 51% reduction in the process steps required for registering, and an increase in orthopedic consultant clinic capacity of 22%. The reduction in NVA activities in the process and the increase in management options for triaging consultants have delivered a more efficient trauma and orthopedic pathway.
1. Introduction
In Ireland, musculoskeletal injuries are the most common reason for the presentation of patients to the Emergency Department (ED) [1]. The volume of musculoskeletal presentations to the ED, in turn, leads to a large number of referrals to trauma orthopedic services [1]. These injuries represent one-third of bed days used in hospitals and one-third of the reasons for acute surgery in Ireland each year [2]. In 2015, orthopedics was reported to have the highest volume of outpatient activity in the Irish health service [2], and recent analysis indicates a further 15% increase [3], with 10,393 patients on orthopedic waiting lists in April 2021 [4]. Similarly, high levels of outpatient activity and orthopedic surgery waiting times have been reported internationally [5,6]. Worldwide, the increase in waiting time for orthopedic and musculoskeletal complaints has negatively affected patient satisfaction [7,8].
This study was carried out in a private hospital in South Dublin, Ireland, and addresses similar processes to previous Lean Six Sigma (LSS) studies completed at the same site relating to patient flow from the ED [9] and medical documentation [10]. The hospital’s ED has over 13,000 presentations each year, with an average of 10% being referred to the trauma orthopedic service. In early 2022, overall presentations to the ED increased by 11% compared to the previous year, with a concurrent rise in ED referrals to trauma orthopedics. These referrals are triaged by consultants who assess the degree of case severity based on presenting signs and symptoms and assign an order of clinical priority [1]. The increasing volume heightens the responsibility of the six trauma orthopedic consultants who facilitate the pathway in combination with their own elective orthopedic caseloads and Public Health Service Executive (HSE) work. Many referrals to the orthopedic service do not require a review appointment with a consultant doctor [11] to continue accessing appropriate care. Unnecessary consultant appointments generate an associated volume of work, further increasing pressure on an already busy service [3].
As the study site has a large number of experienced staff trained in LSS (n = 382) and a track record of successful LSS improvement, it was the methodology of choice for this study. LSS is a merge of two process improvement methodologies: Lean, developed by Toyota, and Six Sigma, developed by Motorola [12]. Lean aims to eliminate waste or NVA activity, often using qualitative measures to achieve this goal [13], whereas Six Sigma targets variation and employs statistical analysis [14]. Additionally, both methodologies have contributed positively to solving problems when combined with a person-centered improvement approach [12] in ED and outpatient settings [15]. Therefore, our work was informed by a combined person-centered Lean Six Sigma approach [12].
A review of 66 articles (year range 2001–2018) relevant to LSS deployment in health systems reported that the methodology is effective in reducing overall waiting times for public hospital appointments [16]. Although there are no specific studies reviewing waiting lists (measured in days) for an outpatient orthopedic department, a reduction of 18% in median outpatient ophthalmology waiting times was achieved using LSS [17]. Within inpatient orthopedics, organizations have applied LSS tools to target length of stay (LOS) [18] or to improve disease-specific pathways [19] such as a reduction in LOS by 42% in 148 knee replacement patients [20]. Improta and colleagues [20] noted NVA in pre-operative planning and a lack of standardized procedures.
The main goal of this study was to reduce the average wait time for patients referred from the ED to trauma orthopedics. At the study site, previous LSS studies had identified duplication of administrative work in the registration of elective orthopedic surgeries [21]. Therefore, in addition to targeting patient waiting times, the project evaluated the impact of the reduction in wait times on the administrative process and consultant clinic caseload. The hypothesis was that improvements in these areas would improve satisfaction for both patients and staff.
2. Methods
LSS methodology was applied using the DMAIC improvement framework. The letters in the acronym stand for Define, Measure, Analyze, Improve, and Control. This framework structures the quality improvement process, encourages stakeholder engagement, and facilitates an implementation plan for devised solutions [16]. LSS methodology was employed via a pre- and post-intervention study design to measure variables relating to wait times, patient registration, and clinical caseload [21]. The methods used in the study are now outlined using the structure of the DMAIC framework.
2.1. Define Phase
A multidisciplinary project team was established to deliver the process improvement project. Membership included the lead trauma orthopedic surgeon, the orthopedic patient services lead, and the orthopedic patient services team. A project charter, one of a number of LSS tools (Table 1) used to structure the study, was completed to define the problem, document the project goal, and consider any risks associated with implementation [22]. Due to the large number of referrals and to enable a solution-focused proof of concept, the scope of the study was refined to include only ED patients referred for peripheral musculoskeletal symptoms such as proximal humerus fractures, distal fibular fractures, and ankle sprains. The scope excluded patients where a care pathway already existed, e.g., hand, spinal, or post-operative patients. An initial request for feedback from staff directly involved in the process determined the current process to be a source of staff ‘anxiety’, to be ‘time-consuming’, and identified that ‘certain referrals generally do not need to see a trauma surgeon’.

Table 1.
Lean Six Sigma tools are used by the project team.
To identify what quantitative data existed to capture the areas of NVA in the process, we completed an initial analysis of wait time data over a four-week period (20 September–22 October 2021). On the evaluation of this baseline data, a mean wait time for patients of 15.98 days was noted. An interquartile range of 15 days reflected the variability in the process wait time. The qualitative and quantitative baseline data were used to formulate a Critical to Quality (CTQ) tool. This is a tool that enables the information gathered from customers to be developed into critical process requirements that are measurable (Table 1) [25]. After our initial Voice of Customer (VOC) gathering and the completion of a CTQ, the key metrics for data collection were identified as:
- Waiting times:
- for a patient to be registered in the orthopedic service as a trauma orthopedic referral from the ED and informed of the receipt of their referral via text message;
- for the consultant to triage the referral;
- for the patient to attend their orthopedic trauma appointment following the ED referral.
- Time taken and number of steps or touch points (points at which staff come into contact with the patient or action the referral) to:
- register a referral;
- triage a referral;
- book the patient’s appointment.
- The efficiency of the trauma consultant’s (total n = 6) caseload is represented by the following:
- opportunity to review the elective caseload;
- conversion rate from appointment to surgery.
2.2. Measure Phase
To support our data collection, we completed a Gemba walk. This is a technique where the project team goes to the actual place of work, examines the process steps in real-time, and records the observations [27]. From this, we were able to formulate a high-level process map (Figure 1) [29]. This gave the project team an overview of the patient’s journey from ED referral to orthopedic surgeon consultation. The project scope centered on the final four steps (steps 12–15), which included the registration, triage, and booking processes for patients referred to the orthopedic service from the ED.
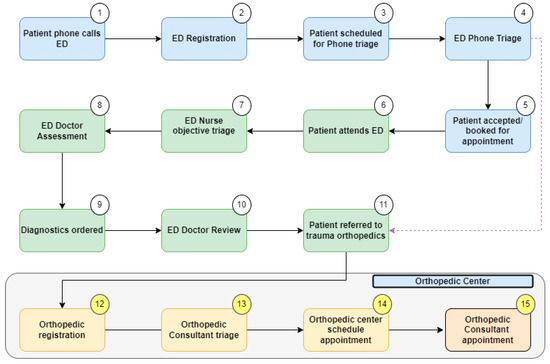
Figure 1.
High-level process map.
Gemba walks were timed to gather quantitative data on the duration of each step in the orthopedic patient services registration process. The number of touch points required to complete the registration and triage processes was also recorded. A touch point was defined as any physical interaction by orthopedic patient services or the trauma consultant with an IT system in order to progress the referral. The number of times staff had to switch between different hospital IT systems to complete this process was also recorded. Observations from the Gemba walk are illustrated on the process map (Figure 1), which is a graphical representation of the process [29]. This LSS tool facilitates visualization of the entire process, establishes process limitations, and addresses the question, ‘what the process actually is?’. The process map was developed in December 2021 following repeated Gemba and extensive VOC engagement. To reduce the risk of researcher misinterpretation of data, collated numerical information and observations were directly corroborated by the members of ED, patient services, and consultants who validated the map. A VOC was completed with the patient services team directly involved in registering ED referrals (n = 4) and with three trauma orthopedic consultants.
Patients routinely arrived at the orthopedic center only on the day of their appointment. Their wait time, the triage time, and the time taken (in days) to book their appointment were recorded by means of a retrospective audit of data from the hospital’s existing information system, MEDITECH, over three months (October–December 2021). The results of this audit are visualized as a linear process map (Figure 2) of pre-intervention or baseline waiting times for each phase of the patient journey, including registration, triage decision, and total appointment wait. The map also shows the baseline outcomes relative to the hospital’s key performance indicators (KPIs).
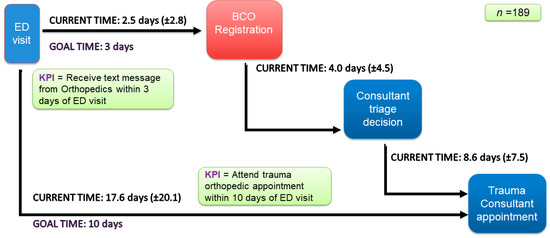
Figure 2.
Linear process map: pre-intervention waiting times.
To understand the patient’s perspective of the trauma orthopedic service, a purposive sample of all patients (n = 189) who attended ED over this pre-intervention period (October–December 2021) was surveyed by phone call (n = 30). Patients who attended the trauma orthopedic consultation were assigned a number, which was entered into a random number generator. Patients randomly selected were subsequently contacted. Ten patients per month were surveyed in an attempt to reduce temporal bias. The composition of consultant clinic caseload and surgeries was also gathered from MEDITECH over a five-month period (January–May 2022). The data collected from the orthopedic patient services questionnaires, consultant surveys, and patient surveys gave the project team an understanding of the NVA from the viewpoint of the patient, the staff, and the organization and the potential impact this had on satisfaction.
2.3. Analyze Phase
To evaluate the NVA in the data gathered from the VOC, Gemba, and audit, a TIMWOODS tool was used (Table 2). Each word of the acronym represents one of eight potential wastes in a process [30]. The VOC illustrated that patient services staff felt excessive time was required to complete the registration tasks; there were too many opportunities for manual error and the consultants’ belief that certain presentations could be managed differently. These themes representing waste were then evaluated further with stakeholders. This involved using an Ishikawa Fishbone diagram to enable a root cause analysis of the NVA identified and to target areas for improvement [27,28].
Table 2.
TIMWOOD tools are used to categorize waste in the process.
2.4. Improve Phase
Working collaboratively with stakeholders, we consolidated our analysis of NVA and root causes to enable us to co-design potential solutions that included:
- (1)
- Designing an IT system to track and triage patients (the “Patient Services Homework Tracker”).
- (2)
- Ring-fencing trauma orthopedic slots.
- (3)
- Developing an information leaflet about the pathway for staff and patients.
- (4)
- Offering physiotherapy as opposed to consultant review (where clinically indicated) as an option for patients.
- (5)
- Creating a consultant triage roster to enable optimal communication between the team with improved visibility of staffing.
A PICK (Possible, Implement, Challenge, Kill) chart was used to prioritize the potential improvements with the greatest positive yield [32]. The project team and stakeholders identified and categorized ideas according to how easy they would be to implement and their likely impact. A practicality tool [30] was subsequently used to consider and rank which of these solutions would be realistic for this particular setting.
The ‘Patient Services Homework Tracker’ (solution 1) was rated as the solution likely to have the greatest beneficial impact. A patient tracker was already used in the ED, following patients’ progress from registration to diagnostics and discharge. The ED Tracker was used as a method of observing patient progress in the department, including wait times and the onward referral destination. However, the ED Tracker stopped monitoring the patient’s journey at ED discharge and did not facilitate patient triage.
To address our problem, the existing tracker required adaptation to enable continued tracking of patients’ progress after ED discharge to orthopedic outpatient registration. In addition, the team suggested the tracker should include the opportunity for orthopedic consultants to triage patients electronically when they are not on the hospital campus. This would permit a quicker triage decision as many of the consultants had clinics operating at other hospital sites each week. Additionally, the triaging consultant would have the option to advise the patient to attend physiotherapy prior to seeing a consultant, if appropriate. This would also reduce patient follow-up wait times. Another suggested benefit of the tracker was improved communication between the emergency and orthopedic departments. The risk of error was also reduced as the current process of using a simple Excel sheet to log referrals would be discontinued.
The ‘Patient Services Homework Tracker’ was co-designed with patient services, IT, and trauma consultants (Figure 3).
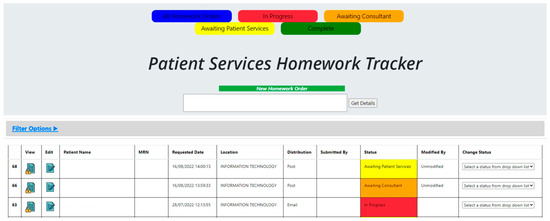
Figure 3.
New Tracker Prototype.
We applied visual management principles using the 5S tool (Table 1) [31] to develop a template that ensured entry fields were only gathering information necessary to complete triage. The triaging consultant was prompted to document three key fields:
- The urgency of the appointment is classified by the surgeons at the study site as operative routine, non-operative routine, and non-operative urgent.
- Which trauma consultant was the patient referred to by the triaging consultant.
- Whether or not a physiotherapy referral was advised.
The tracker template and other solutions (1–5) were implemented as a pilot before a repeat audit of the process. The audit permitted further analysis of the appropriateness of some template fields. Departmental resources were the same pre- and post-intervention.
3. Results
Pre-intervention patient record data on wait times were recorded on MEDITECH over three months between October and December 2021 and post-intervention in March 2022. This time period was used to analyze each of the three wait times and the number of surgeries.
3.1. Reduction in Patient Wait Times
The primary goal was achieved with more than 50% of patients (52%) attending the trauma orthopedic consultant within 10 days of their ED visit. This was an increase of 11% in baseline outcomes (Figure 4). The data illustrate a reduction in the total mean wait time between an ED visit and a trauma orthopedic appointment from 17.6 (±20.1) to 11.6 (±20.1) days. The improvement represents a 34% reduction (Figure 4) and was achieved by addressing the waiting time NVA identified in the TIMWOODS. The project also improved outcomes relative to the hospital’s KPIs.
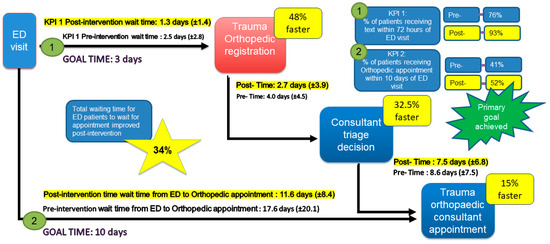
Figure 4.
The impact on waiting times.
3.2. Reduction in Registering and Triage time, Touch Points, and IT System
Gemba interventions, pre- (n = 10; December 2021) and post- (n = 10; August 2022), were completed on time and identified touchpoints in the process. An updated post-intervention TIMWOODS (Table 3) illustrates the impact of piloted solutions (numbers 1, 2, 4, and 5). The table details a reduction in the time taken to process a referral by 52%. Touchpoints are also reduced by 51% for patient services staff and 27% for consultants to triage referrals. The table also highlights other improvements to NVA, such as re-work due to inadequate information (Overprocessing, Overproduction, and Defects).
Table 3.
TIMWOOD tools illustrate the intervention impact.
3.3. Increased Trauma Consultant Clinic Capacity and Surgical Cases
Consultant (n = 6) clinic caseload was analyzed pre- (January–February 2022) and post- (April–May 2022) (Table 4). The solutions (numbers 1, 2, 4, and 5) were implemented in March 2022 for a trial month. The six trauma orthopedic consultants reviewed 51% more patients post-intervention. This indicated an improved capacity for consultants to review their post-operative caseload. A 22% increase in clinic capacity was also noted. Of the patients referred from the ED to trauma orthopedics, nearly one-quarter required surgery (22%) (Table 4). This was an improvement of 8% and indicated that with these new solutions, the consultants were assessing a more appropriate caseload. The improvement assisted in addressing the skills waste identified in the TIMWOODS analysis.
Table 4.
The impact on consultant caseload.
3.4. Patient and Staff Satisfaction
In total, pre- and post-intervention VOC was completed with consultants (n = 5), other staff (n = 9), and patients (n = 40). The post-intervention survey of patients indicated that both trauma orthopedic center key performance indicators (KPI) developed by the hospital were relevant and important in their care. The first KPI asserts that patients should receive a text from the orthopedic center confirming receipt of the referral within 72 h of their ED visit. The second KPI states that patients should receive an orthopedic appointment within 10 days of their ED visit. On average, patients believed that an appointment within 10.77 days (range 0–28 days) was necessary, with some stating they would consider seeking care elsewhere after this. If advised by the triage consultant, 70% of patients would be interested in pursuing physiotherapy as an alternative initial option. As the triage system was piloted in template form, following the pilot, we engaged with the stakeholders to record their opinions on the proposed solutions (numbers 1–5) before moving beyond the pilot phase. The consultant and patient services group were very positive and eager to proceed with the proposed changes. Table 5 displays the VOC (Patient and Patient Services Team) responses to sample questions surveyed pre- and post-intervention. Solution number 4 was developed with the pre-intervention VOC in mind to manage patient expectations. The stakeholder group designed a plan to implement the ‘Patient Services Homework Tracker’ for the trauma orthopedic service. This plan included the implementation of the triage template for the service while the project team liaised with IT to finalize the development of the electronic solution. A control plan was devised to support and monitor continued improvements. The impact of the pilot solutions was monitored through stakeholder feedback and compliance with the timed KPIs.
Table 5.
The impact of solutions on Voice of the Customer (VOC).
4. Discussion
The original goal of the study was to increase the number of patients attending their trauma orthopedic appointment within 10 days of their ED visit. We hypothesized that this could be achieved by reducing NVA in the registration, triage, and booking processes. We slightly exceeded our initial target of 50%, offering 52% of patients an appointment within 10 days (Figure 4). The total wait time from ED to consultant appointment was reduced by 34%, with a mean wait slightly longer than our KPI target of 10 days (11.6 ± 8.4 days). Significant reductions in NVA were generated in the registration process, with a 51% decrease in touch points required to register a patient (Table 3). This reduction in administrative workload corresponded with an improvement in staff satisfaction with the process (Table 5).
Consultants also reviewed more appropriate patients following the implementation of the solutions, with 22% of patients referred from the ED to the trauma orthopedic consultant requiring surgery. This indicated that consultant surgeons were assessing more appropriate patients. Although this was not specifically mentioned in patient surveys, those receiving care in the intervention phase reported a slightly improved satisfaction score relative to the baseline measures. The improved efficiency of the triage process, with patients seeing an appropriate medical professional at the right time, coincided with consultants having a greater opportunity to review their elective caseload. An elective patient signifies the non-trauma cohort of a consultant’s caseload, and these clinic appointments increased by 51% during the post-intervention phase (Table 4). This improvement was achieved through enhanced information gathering in the triage template and the option for consultants to refer patients not requiring surgical input to physiotherapy. This therapy pathway has been demonstrated successfully elsewhere, with physiotherapists participating in the triage process [9] and reviewing trauma orthopedic patients post-fracture [34].
The success of the project was enabled by extremely motivated internal champions and substantial senior-level management support, both of which have been shown to be hugely beneficial when completing an LSS project [35]. Senior management backing is a key factor in the success of LSS implementation, as a perceived lack of support can reduce project members’ motivation and result in project failure. Leaders have the potential to be role models for change and facilitators of LSS implementation [36]. The noted successes of previous Lean champions in supporting LSS initiatives are thought to have contributed to the creation of an improvement culture within the organization [37]. The fundamental desire of healthcare providers across each specialty to improve the service for trauma patients was noteworthy in this project. The principles underpinning the project were observed to align with participants’ core values of person-centered care [12]. Waring and Bishop [38] argue that LSS initiatives succeed through the mediation of the people involved as they interact and engage within enabling social structures. The organization continues to encourage staff to identify and engage in improvement projects by ensuring that they have access to education, training, and development opportunities that provide the tools and techniques to implement change. Additionally, these opportunities shape their attitudes and practices so that practice and process improvements become embedded and sustainable.
The solutions implemented in this study will positively affect the orthopedic center and improve patient flow through the department. However, later in the patient journey, due to the change in referral options, we recognized that there was a limitation: the potential for increased pressure on physiotherapy resources. Similarly, an increase in cases requiring surgical management will test an already busy Operating Room Department. This potential shift in workload from orthopedics to other departments would not represent respect for colleagues, a key principle of person-centered care and Lean [12]. Nor would it represent systems thinking, another key principle of Lean. To manage any potential risk of creating an uneven workload across the process, department managers, frontline staff, and local LSS practitioners in each department agreed to monitor referral numbers and clinic availability on a monthly basis. At a higher level, senior management reviews seasonality patterns in service, specialty staffing levels, and bottlenecks in the system. In the event of uneven workload or a department potentially becoming overburdened, the process will be revisited to identify if any NVA exists using, for example, Gemba or the TIMWOODS tool. The project team intends to continually work with stakeholders to develop a service that is person-centered throughout the organization.
A person-centered approach to Lean Six Sigma acknowledges the imperative of developing positive relationships between service users and staff to improve the healthcare experience for all [12]. It enabled the team to understand that a shift of workload from one department to another without agreed contingency planning would fail to consider the potential negative impact on other parts of the organization and colleagues’ workloads. Oshry [39] highlights the importance of awareness of systems and an appreciation of the conditions under which colleagues work in different parts of a system. In recognition of this, the project team comprised a mix of staff levels across various administrative and clinical roles. The diversity of perspectives aimed to limit the influence of personal, positional, professional, or disciplinary bias on diagnosis or solution formation [12] and to create the conditions to enable staff empowerment and engagement [40,41]. The involvement of frontline staff in the co-creation of solutions has been shown to contribute to the development of a sense of ownership in the system and improve the prospect of whole-system success [41,42,43].
The data from this project will be used to track the number of referrals and consequent workload on hospital services involved in the new pathway. Links between each department and clinical group have already been developed to ensure timely communication. These channels include email updates to consultants and physiotherapists regarding current clinic availability. ED and orthopedic patient services meetings are scheduled along with monthly trauma orthopedic meetings. A potential benefit across the wider hospital includes the opportunity for other outpatient departments to have patients referred, registered, and triaged using the ‘Patient Services Homework Tracker’. This system will also ensure triaging decisions are documented in patients’ medical charts, further enhancing communication using the ISBAR tool (Identify, Situation, Background, Assessment, Recommendation) [44].
We acknowledge that the study was completed at a single ED site. High trauma and complex trauma presentations were not triaged to this center. However, complex cases are very unlikely to enter the outpatient service through a triage system. The study results relied on a prototype rather than the finalized Tracker system. This phase depended heavily on the support of IT, which had a number of other simultaneously occurring projects. To take account of this, improvements to the process, separate from software implementation, were made. These included the provision of educational materials, a review of triage rosters, and the referral option to physiotherapy, all of which may be transferable to other sites. Further improvements, measurements, and analyses will be completed once the tracker is finalized. Gaining a deeper understanding of the service with the tracker in situ is the initial aim. However, future projects may consider the potential for injury-specific ED to trauma orthopedic pathways.
5. Conclusions
The application of LSS methodology to the process of registering, triaging, and booking ED patients for orthopedic appointments resulted in a reduction in wait time for this cohort. Further reductions in NVA were noted in time taken and touch points to complete administrative tasks, as well as improvements in consultant clinic efficiency. The use of LSS principles allowed the team to quantify the existing process, identify areas of waste, and thereby deliver more effective solutions. The project has resulted in long-term changes with improved customer satisfaction and a system to triage patients for the trauma orthopedic pathway, which has the potential to be rolled out across other outpatient specialties in the hospital. In addition, changes to the orthopedic triage pathway will allow patients to access physiotherapy and provide a means for the department to sustain improvements in the efficiency of consultants’ caseload management. The project also reflects the significant contribution and importance of strong senior management support and a multidisciplinary project team.
Author Contributions
All authors made a proportional contribution. Conceptualization, A.P., A.D., S.P.T. and B.O.; methodology, A.P., A.D. and S.P.T.; formal analysis, A.P.; investigation, A.P.; resources, A.P. and A.D.; data curation, A.P.; writing—original draft preparation, A.P. and S.P.T.; writing—review and editing, A.P., S.P.T. and M.M.; visualization, A.P., A.D. and S.P.T.; supervision, A.D. and S.P.T.; project administration, A.P. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
This work took place as part of an ongoing organizational quality improvement project and is covered by the study site’s institutional review board.
Informed Consent Statement
Informed consent was received from patients participating in surveys.
Data Availability Statement
All data are represented within the paper.
Acknowledgments
The authors acknowledge all staff members immediately involved in this project: all the orthopaedic Patient Services team and the orthopedic consultants for their invaluable support. We would also like to thank all IT, ED and Allied Therapy staff members. We thank other Beacon Hospital Green and Black Belts for their invaluable support and advice, the UCD Mater Lean Academy and Beacon Hospital.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Cummins, N.M.; Barry, L.A.; Caravan, C.; Devlin, C.; Corey, G.; Cummins, F.; Ryan, D.; Cronin, S.; Wallace, E.; McCarthy, G.; et al. The “better data, better planning” census: A cross-sectional, multi-centre study investigating the factors influencing patient attendance at the emergency department in Ireland. BMC Health Serv. Res. 2022, 22, 471. [Google Scholar] [CrossRef] [PubMed]
- O’Reilly, M.F.; Mohamed, K.M.; Sheehan, E.C. General practitioner attitudes and experiences of orthopedic services in the Irish midlands. Ir. J. Med. Sci. 2019, 188, 735–741. [Google Scholar] [CrossRef] [PubMed]
- RCSI University of Medicine and Health Sciences. Increase in Waiting Lists for Elective Orthopedic Appointments during Pandemic. Royal College of Surgeons in Ireland. Available online: https://www.rcsi.com/dublin/news-and-events/news/news-article/2021/11/increase-in-waiting-lists-for-elective-orthopaedic-appointments-during-pandemic (accessed on 18 August 2022).
- RCSI University of Medicine and Health Sciences. Impact of COVID-19 on Surgical Services Detailed in New NCPS Report. Royal College of Surgeons in Ireland. Available online: https://www.rcsi.com/dublin/news-and-events/news/news-article/2021/10/impact-of-covid-19-on-surgical-services-detailed-in-new-ncps-report (accessed on 18 August 2022).
- Australian Institute of Health and Welfare; Australian Government. Elective Surgery Waiting Times 2021–2022. Elective Surgery Access. Hospitals—Australian Institute of Health and Welfare. Available online: https://www.aihw.gov.au/reports-data/myhospitals/intersection/access/eswt#:~:text=National%20data%20is%20available.,than%20365%20days%20for%20surgery.&text=This%20table%20shows%20waiting%20times,%E2%80%9313%20and%202021%E2%80%9322 (accessed on 7 December 2022).
- NHS England. Statistical Press Notice, NHS Referral to Treatment (RTT) Waiting Times Data September 2022. Available online: https://www.england.nhs.uk/statistics/wp-content/uploads/sites/2/2022/11/Sep22-RTT-SPN-pre-release-version-34691.pdf (accessed on 7 December 2022).
- Glogovac, G.; Kennedy, M.E.; Wesigerber, M.R.; Kakazu, R.; Grawe, B.M. Wait times in musculoskeletal patients: What contributes to patient satisfaction. J. Patient Exp. 2020, 7, 549–553. [Google Scholar] [CrossRef]
- Strategy for the Design of Integrated Outpatient Services 2016–2020, Outpatient Services Improvement Program. Outpatient Services Performance Improvement Programme. Available online: https://www.hse.ie/eng/about/who/acute-hospitals-division/outpatient-services-performance-improvement-programme/ (accessed on 18 August 2022).
- Daly, A.; Teeling, S.P.; Ward, M.; McNamara, M.; Robinson, C. The use of Lean Six Sigma for improving availability of and access to Emergency Department data to facilitate patient flow. Int. J. Environ. Res. Public Health 2021, 18, 11030. [Google Scholar] [CrossRef] [PubMed]
- Wolfe, N.; Teeling, S.P.; Ward, M.; McNamara, M.; Koshy, L. Operation Note Transformation: The application of Lean Six Sigma to improve the process of documenting the operation note in a private hospital setting. Int. J. Environ. Res. Public Health 2021, 18, 12217. [Google Scholar] [CrossRef] [PubMed]
- Fennelly, O.; Blake, C.; Fitzgerald, O.; Breen, R.; Ashton, J.; Brennan, A.; Caffrey, A.; Desmeules, F.; Cunningham, C. Advanced practice physiotherapy-led triage in Irish orthopedic and rheumatology services: National data audit. BMC Musculoskelet. Disord. 2018, 19, 181. [Google Scholar] [CrossRef] [PubMed]
- Teeling, S.P.; Dewing, J.; Baldie, D. A realist inquiry to identify the contribution of Lean Six Sigma to Person-Centered Care and Cultures. Int. J. Environ. Res. Public Health 2021, 18, 10427. [Google Scholar] [CrossRef]
- Antony, J.; Snee, R.; Hoerl, R. Lean Six Sigma: Yesterday, today and tomorrow. Int. J. Qual. Reliab. Manag. 2017, 34, 1073–1093. [Google Scholar] [CrossRef]
- Antony, J. Six Sigma vs. Lean: Some perspectives from leading academics and practitioners. Int. J. Product. Perform. Manag. 2011, 50, 185–190. [Google Scholar] [CrossRef]
- Rosa, A.; Marolla, G.; Lega, F. Lean adoption in hospitals: The role of contextual factors and introduction strategy. BMC Health Serv. Res. 2021, 21, 889. [Google Scholar] [CrossRef]
- Al-Zuheri, A.; Vlachos, I.; Amer, Y. Application of Lean Six Sigma to reduce patient waiting time: Literature Review. Int. J. Qual. Res. 2021, 15, 241–258. [Google Scholar] [CrossRef]
- Kam, A.W.; Collins, S.; Park, T.; Mihail, M.; Stanway, F.F.; Lewis, N.L.; Polya, D.; Fraser-Bell, S.; Roberts, T.V.; Smith, J.E.H. Using Lean Six Sigma techniques to improve efficiency in outpatient ophthalmology clinics. BMC Health Serv. Res. 2021, 21, 38. [Google Scholar] [CrossRef]
- Niemeijer, G.C.; Trip, A.; Ahaus, K.T.; Does, R.J.; Wendt, K.W. Quality in trauma care: Improving the discharge procedure of patients by means of Lean Six Sigma. J. Trauma Acute Care Surg. 2010, 69, 614–618. [Google Scholar] [CrossRef]
- Müller, M.K.; Dedes, K.J.; Dindo, D.; Steiner, S.; Hahnlosser, D.; Clavien, P.A. Impact of clinical pathways in surgery. Langenbeck’s Arch. Surg. 2009, 394, 31–39. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Improta, G.; Balato, G.; Romano, M.; Ponsiglione, A.M.M.; Raiola, E.; Russo, M.A.; Cuccaro, P.; Santillo, L.C.; Cesarelli, M. Improving performances of the knee replacement surgery process by applying DMAIC principles. J. Eval. Clin. Pract. 2017, 23, 1401–1407. [Google Scholar] [CrossRef]
- These, M.S. Observational and interventional study design types: An overview. Biochem. Med. 2014, 23, 199–210. [Google Scholar] [CrossRef] [PubMed]
- Tjahjono, B.; Ball, P.; Vitanov, V.I.; Scorzafave, C.; Nogueira, J.; Calleja, J.; Minguet, M.; Narasimha, L.; Rivas, A.; Srivastava, A.; et al. Six Sigma: Literature Review. Int. J. Lean Six Sigma 2010, 1, 216–233. [Google Scholar] [CrossRef]
- Ogbeiwi, O. General concepts of goals and goal setting in healthcare, a narrative review. J. Manag. Organ. 2021, 27, 324–371. [Google Scholar] [CrossRef]
- Galli, B. Can project management help improve Lean Six Sigma. IEEE Eng. Manag. Rev. 2018, 26, 55–64. [Google Scholar] [CrossRef]
- Riebling, N.B.; Norouzzadeh, S.; Reeder, G.; Mouradian, C.; Hillier, A.; Cowan, R.; Doerfler, M. Quantifying patient satisfaction with process metrics using a weighted bundle approach. BMJ Open Qual. 2019, 8, e000458. [Google Scholar] [CrossRef]
- Found, P.; Harrison, R. Understanding Lean Voice of Customer. Int. J. Lean Six Sigma 2012, 3, 251–257. [Google Scholar] [CrossRef]
- Dalton, J. Gemba Walks. In Great Big Agile; Apress: Berkeley, CA, USA, 2019. [Google Scholar]
- Taghizadegan, S. Mastering Lean Six Sigma: Advanced Black Belt Concepts; Momentum Press: New York, NY, USA, 2013. [Google Scholar]
- Colligan, L.; Anderson, J.E.; Potts, H.W.W.; Berman, J. Does the process map influence the outcome of quality improvement work? A comparison of sequential flow diagram and a hierarchical task analysis diagram. BMC Health Serv. Res. 2010, 10, 7. [Google Scholar] [CrossRef]
- Egan, P.; Pierce, A.; Flynn, A.; Teeling, S.P.; Ward, M.; McNamara, M. Releasing operating room nursing time to care through the reduction of surgical case preparation time: A lean six sigma pilot study. Int. J. Environ. Res. Public Health 2021, 18, 12098. [Google Scholar] [CrossRef]
- Kanamori, S.; Sow, S.; Castro, M.C.; Matsuno, R.; Tsuru, A.; Jimba, M. Implementation of 5S management method for lean healthcare at a health center in Senegal; A qualitative study of staff perception. Glob. Health Action 2015, 8, 27256. [Google Scholar] [CrossRef]
- Brown, R.; Grehan, P.; Brennan, M.; Carter, D.; Brady, A.; Moore, E.; Teeling, S.P.; Ward, M.; Eaton, D. Using Lean Six Sigma to improve rates of day of surgery admission in a national thoracic surgery department. Int. J. Qual. Health Care 2019, 31, 14–21. [Google Scholar] [CrossRef] [PubMed]
- Sarker, A.; Mukhopadhyay, A.; Ghosh, S. An outline of the “Control Phase” for implementing Lean Six Sigma. Int. J. Lean Six Sigma 2014, 5, 230–252. [Google Scholar] [CrossRef]
- O’Reilly, M.; Breathnach, O.; Conlon, B.; Kiernan, C.; Sheehan, E. Trauma assessment clinic: Virtually a safe and smarter way of managing trauma care in Ireland. Injury 2019, 50, 898–902. [Google Scholar] [CrossRef]
- Pacheco, D.; Perher, I.; Vaccaro, G.L.R.; Jung, C.F. 18 comparative aspects between Lean and Six Sigma: Complementarity and implications. Int. J. Lean Six Sigma 2014, 6, 161–175. [Google Scholar] [CrossRef]
- Aij, K.H.; Simons, F.E.; Widdershoven, G.A.M.; Visse, M. Experiences of leaders in the implementation of Lean in a teaching hospital—Barriers and facilitators in clinical practices: A qualitative study. BMJ Open 2013, 3, e003605. [Google Scholar] [CrossRef] [PubMed]
- Daly, A.; Wolfe, N.; Teeling, S.P.; Ward, M.; McNamara, M. Redesigning the process for scheduling elective Orthopedic Surgery: A combined Lean Six Sigma and Person-Centered Approach. Int. J. Environ. Res. Public Health 2021, 18, 11946. [Google Scholar] [CrossRef] [PubMed]
- Waring, J.J.; Bishop, S. Lean healthcare: Rhetoric, ritual and resistance. Soc. Sci. Med. 2010, 71, 1332–1340. [Google Scholar] [CrossRef] [PubMed]
- Oshry, B. Context, Context, Context: How Our Blindness to Context Cripples Even the Smartest Organisations; Triarchy Press: Dorset, UK, 2018. [Google Scholar]
- Laloux, F. Reinventing Organisations: A Guide to Creating Organisations Inspired by the Next Stage of Human Conviousness, 1st ed.; Nelson Publishing: Brussels, Belgium, 2014. [Google Scholar]
- Daly, A.; Teeling, S.P.; Garvey, S.; Ward, M.; McNamara, M. Using a combined lean and person-centred approach to support the resumption of routine hospital activity following the first wave of COVID-19. Int. J. Environ. Res. Public Health 2022, 19, 2754. [Google Scholar] [CrossRef] [PubMed]
- Teeling, S.P.; Keown, A.M.; Cunningham, U.; Keegan, D. The application of a person-centred approach to process improvement in ophthalmology services in the North East of the Republic of Ireland. Int. Pract. Dev. J. 2023, 13, 6. [Google Scholar] [CrossRef]
- Teeling, S.P.; McGuirk, M.; McNamara, M.; McGroarty, M.; Igoe, A. The Utilization of Lean Six Sigma Methodologies in Enhancing Surgical Pathways and Surgical Rehabilitation. Appl. Sci. 2023, 13, 6920. [Google Scholar] [CrossRef]
- Müller, M.; Jürgens, J.; Raedaèlli, M.; Klingberg, K.; Haultz, W.E.; Stock, S. Impact of the communication and patient hand-off tool SBAR on patient safety: A systematic review. BMJ Open 2018, 8, e022202. [Google Scholar] [CrossRef]




Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).