

Developing a Low-Cost IoT-Based Remote Cardiovascular Patient Monitoring System in Cameroon

 ,
,  , ,
, , 
Abstract
:1. Introduction
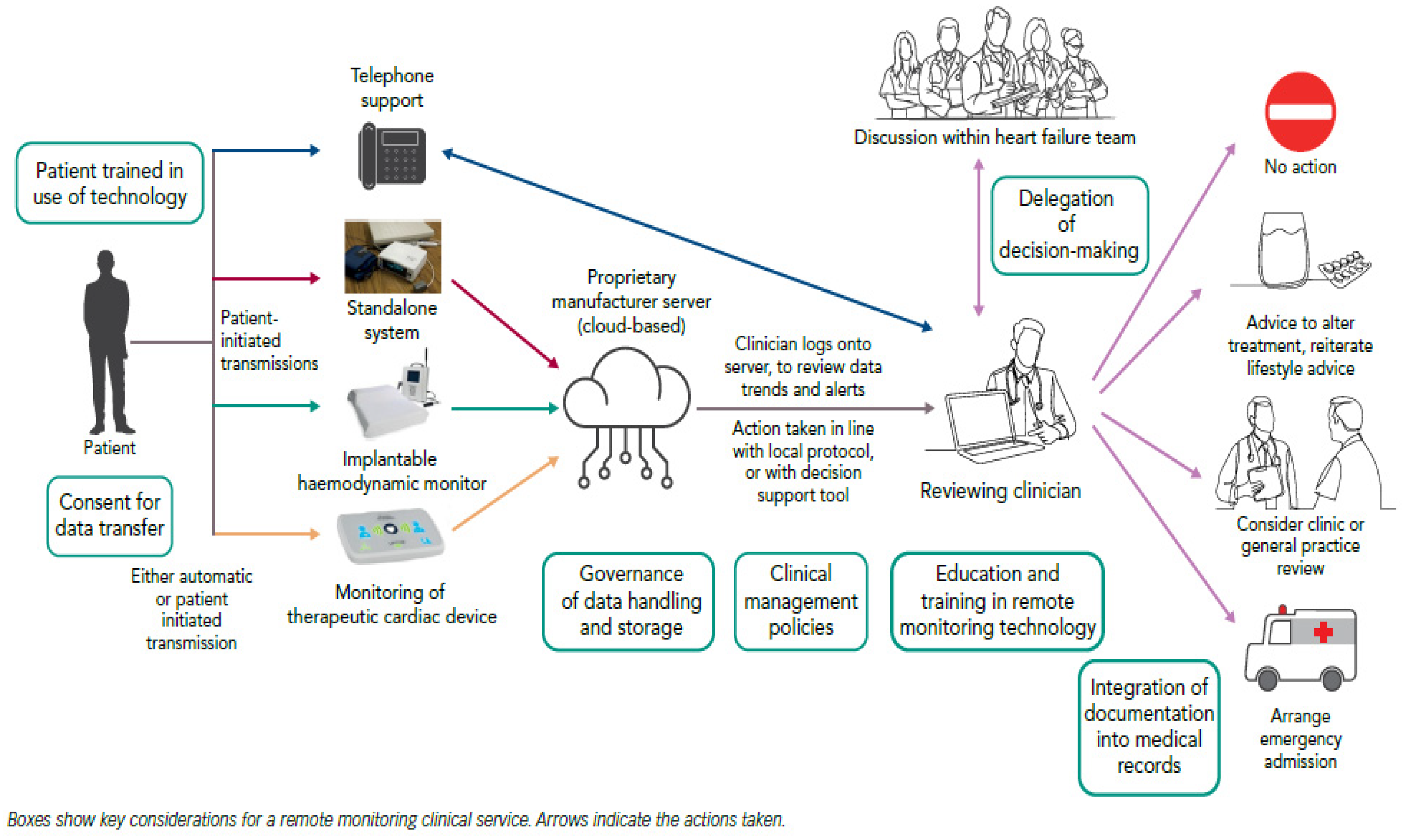
- Structured telephone support for patients: this is generally provided by specialists of the heart failure (HF) team; it assists in a disease management program or a post-discharge service;
- Standalone RPM systems: These devices can be used at home by patients to measure some physical parameters. e.g., BP, heart rate, weight, and oxygen saturation;
- Remote monitoring using cardiac implantable devices: These are used to collect real-time data to aid the HF management. They include devices, such as pacemakers and ICDs, implanted primarily for therapeutic purposes;
- Wearable devices: They include patches, watches, or textiles equipped with sensors that can monitor a patient’s parameters e.g., ECG, BP, body temperature, blood glucose concentration, and body posture.
2. Related Work
3. Materials and Methods
3.1. Study Design
3.2. Specify the Usage Context
- Remote monitoring: Have a digitized history of patients’ vital signs that are monitored remotely in real-time over the internet;
- Alert notifications: When the system recognizes an uncommon circumstance, to generate and establish notifications for patients, cardiologists or caretakers, and family members;
- Medical record: The system must be capable of keeping the medical records and providing easy, secure access to them in real time;
- Communication with family: The system must offer a feature to provide in-depth summaries of the doctor’s recommendations to the patient or family, in order to encourage the family participation in patient care;
- The subsequent UCD phase was initiated, in light of those findings.
3.3. Specify Requirements
3.3.1. System Architecture of the Cardiovascular RPM System
3.3.2. Hardware Tools
3.3.3. Software Requirements
- Users must be authenticated in the RPM application;
- The latest information gathered by the vital signs sensors should be displayed to caregivers through the RPM application;
- A communication module must be included in the RPM application for the cardiologist and care team to use, when speaking with the patient or their family;
- The RPM application should allow the cardiologist and care team to access the clinical information of the patient as required.
- The device with the sensors for monitoring the vital signs should have Bluetooth Smart (BLE), to send the generated data to the database;
- The availability of the system must be near permanent and offer a decent service level for the users;
- The stored data can be consulted.
3.3.4. Produce Design Solutions
- The connection of the Arduino Uno to all the other components;
- The implementation of the whole project on a solderless experiment board (breadboard);
- Obtaining the data and forwarding them to a connecter automatically, as a result of a Bluetooth/SMS request, or manually by pressing the pushbutton provided in the system.
4. Results and Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- World Health Organization. May 2022. Available online: https://www.who.int/news-room/fact-sheets/detail/cardiovascular-diseases-(cvds) (accessed on 11 August 2022).
- Dzudie, A.; Fourie, J.M.; Scholtz, W.; Scarlatescu, O.; Nel, G.; Kingue, S. PASCAR and WHF Cardiovascular Diseases Scorecard Project. Cardiovasc. J. Afr. 2020, 31, 103–110. Available online: https://hdl.handle.net/10520/EJC-1cdb86c459 (accessed on 23 July 2022). [CrossRef] [PubMed]
- Ojong, N. The COVID-19 Pandemic and the Pathology of the Economic and Political Architecture in Cameroon. Healthcare 2020, 8, 176. [Google Scholar] [CrossRef]
- Bang, H.N.; Balgah, R.A. The ramification of Cameroon’s Anglophone crisis: Conceptual analysis of a looming “Complex Disaster Emergency”. Int. J. Humanit. Action 2022, 7, 6. [Google Scholar] [CrossRef]
- Mvondo, M.C.; Giamberti, A.; Ngowe, M.N.; Mbuoh, H.A.; Milocco, I.; Tsague Kengni, H.N.; Cirri, S.; Frigiola, A. Cardiac Surgery Development in Cameroon: Unexpected Challenges from a Socio-Political Crisis. Front. Cardiovasc. Med. 2022, 9, 778075. [Google Scholar] [CrossRef] [PubMed]
- Nef, H.M.; Elsässer, A.; Möllmann, H.; Abdel-Hadi, M.; Bauer, T.; Brück, M.; Eggebrecht, H.; Ehrlich, J.R.; Ferrari, M.W.; Fichtlscherer, S.; et al. Impact of the COVID-19 pandemic on cardiovascular mortality and catherization activity during the lockdown in central Germany: An observational study. Clin. Res. Cardiol. 2021, 110, 292–301. [Google Scholar] [CrossRef] [PubMed]
- Craig, P.; Dieppe, P.; Macintyre, S.; Michie, S.; Nazareth, I.; Petticrew, M. Developing and evaluating complex interventions: The new Medical Research Council guidance. BMJ 2008, 337, a1655. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Malasinghe, L.P.; Ramzan, N.; Dahal, K. Remote patient monitoring: A comprehensive study. J. Ambient. Intell. Hum. Comput. 2019, 10, 57–76. [Google Scholar] [CrossRef] [Green Version]
- AHA. Using Remote Patient Monitoring Technologies for Better Cardiovascular Disease Outcomes Guidance. Available online: https://www.heart.org/-/media/files/about-us/policy-research/policy-positions/clinical-care/remote-patient-monitoring-guidance-2019.pdf?la=en (accessed on 28 April 2021).
- Brahmbhatt, D.H.; Cowie, M.R. Remote Management of Heart Failure: An Overview of Telemonitoring Technologies. Card. Fail. Rev. 2019, 5, 86–92. [Google Scholar] [CrossRef] [PubMed]
- Dohr, A.; Modre-Opsrian, R.; Drobics, M.; Hayn, D.; Schreier, G. The Internet of Things for Ambient Assisted Living. In Proceedings of the 2010 Seventh International Conference on Information Technology: New Generations, Las Vegas, NV, USA, 12–14 April 2010; pp. 804–809. [Google Scholar] [CrossRef]
- Suh, M.K.; Moin, T.; Woodbridge, J.; Lan, M.; Ghasemzadeh, H.; Bui, A.; Ahmadi, S.; Sarrafzadeh, M. Dynamic self-adaptive remote health monitoring system for diabetics. In Proceedings of the 2012 Annual International Conference of the IEEE Engineering in Medicine and Biology Society, San Diego, CA, USA, 28 August–1 September 2012; pp. 2223–2226. [Google Scholar] [CrossRef]
- Valsalan, P.; Baomar, T.A.B.; Baabood, A.H.O. IoT based health monitoring system. J. Crit. Rev. 2020, 7, 739–743. [Google Scholar] [CrossRef]
- Li, C.; Hu, X.; Zhang, L. The IoT-based heart disease monitoring system for pervasive healthcare service. Procedia Comput. Sci. 2017, 112, 2328–2334. [Google Scholar] [CrossRef]
- Manisha, M.; Neeraja, K.; Sindhura, V.; Ramya, P. IoT on heart attacks detection and heart rate monitoring. Int. J. Innov. Eng. Technol. 2016, 7, P459–P466. Available online: http://ijiet.com/wp-content/uploads/2016/09/67.pdf (accessed on 12 June 2022).
- Senthamilarasi, C.; Rani, J.J.; Vidhya, B.; Aritha, H. A smart patient health monitoring system using IoT. Int. J. Pure Appl. Math. 2018, 119, 59–70. [Google Scholar]
- Gurjar, A.; Sarnaik, N.A. Heart Attack Detection by Heartbeat Sensing using Internet Of Things: IoT. Int. Res. J. Eng. Technol. 2018, 5, P3332–P3335. [Google Scholar]
- Sethuraman, T.V.; Rathore, K.S.; Amritha, G.; Kanimozhi, G. IoT based system for Heart Rate Monitoring and Heart Attack Detection. Int. J. Eng. Adv. Technol. 2019, 8, 1459–1464. [Google Scholar]
- Gopi, S.; Punarselvam, E. Heart Attack Recognition and Heart Rate Monitoring System Using IOT. Int. J. Appl. Eng. Technol. 2019, 5, 5–10. [Google Scholar]
- Noubiap, J.J.; Jingi, A.M.; Kengne, A.P. Local innovation for improving primary care cardiology in resource-limited African settings: An insight on the Cardio Pad(®) project in Cameroon. Cardiovasc. Diagn. Ther. 2014, 4, 397–400. [Google Scholar] [CrossRef] [PubMed]
- Roman Richard, A.A.; Sadman, M.F.; Mim, U.H.; Rahman, I.; Zishan, M.S.R. Health Monitoring System for Elderly and Disabled People. In Proceedings of the 2019 International Conference on Robotics, Electrical and Signal Processing Techniques (ICREST), Dhaka, Bangladesh, 10–12 January 2019; pp. 677–681. [Google Scholar] [CrossRef]
- Hwang, W.; Salvendy, G. Number of people required for usability evaluation: The 10 + 2 rule. Commun. ACM 2010, 53, 130–133. [Google Scholar] [CrossRef]
- Goldman, A.I. Experts: Which ones should you trust? Philo. Phenomenol. Res. 2001, 63, 85–110. [Google Scholar] [CrossRef]
- Abras, C.; Maloney-Krichmar, D.; Preece, J. User-centered design. In Encyclopedia of Human-Computer Interaction; Bainbridge, W., Ed.; Sage Publications: Thousand Oaks, CA, USA, 2004; pp. 1–14. [Google Scholar]
- Gothelf and Seiden. Lean UX Process. 2016. Available online: https://www.oreilly.com/library/view/lean-ux-2nd/9781491953594/ (accessed on 24 October 2021).
- Presmman, R. Ingeniería del Software un Enfoque Práctico; Mc. Graw Hill: New York, NY, USA, 2010. [Google Scholar]
- Nielsen, J. Severity Ratings for Usability Problems. 1995. Available online: https://www.nngroup.com/articles/how-to-rate-the-severity-of-usability-problems/ (accessed on 24 April 2021).
- Harris, E. Cardiopad: Reaching the hearts of rural communities in Africa. WIPO MAGAZINE, 1 November 2015; pp. 20–22. Available online: https://search.informit.org/doi/10.3316/agispt.20201120039978(accessed on 10 December 2022).









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Components | Description |
|---|---|
 | Arduino is a microcontroller board, that contains a board power supply, a USB port to communicate with the PC, and an Atmel microcontroller chip. We decided to use Arduino Uno, based on the board size, pricing comparison, and connectivity, making our IoT-based RPM system suitable for it. |
 | This is the main monitoring device of our system. It is responsible for collecting the data (diastolic, systolic, and heart rate) using its sensors to send to the Arduino UNO through wires. Following our interview with the medical experts, it was adopted that the normal BP values depend on two factors: age and sex. The normal range for BP and HR measurements was given, based on the factors. |
 | This device has many features, but the ones we may look at are: connection to any global GSM network with any 2G SIM; the possibility to make and receive voice calls using an external 8Ω speaker and electret microphone; capability of sending and receiving SMS messages. This module was optional for our system, our application will be able to perform its function, that is sending SMS messages, but because of the quality of the internet connectivity, we thought it wise to have this module and a 2G SIM card to send and read the parameters. By doing this we are sure that even if the connectivity fails with the connecter, the medical expert and guardian can receive a message on the real-time physical condition of the patient. |
 | This is a liquid crystal display unit attached to a microcontroller. The role of the LCD unit in our system is to display the values from the sensing device, to confirm the correctness of the transmitted data. |
 | This was needed to reduce the voltage received from the microcontroller. |
 | Our pushbutton picks the parameters on the patient’s demand without any wireless connectivity (Bluetooth and GSM) instruction. |
 | We decided to use a HC-05 Bluetooth module to link our sensing layer device to the smartphone or computer. All data collected by the sensor are transmitted through Bluetooth under the JSON (JavaScript object notation) format. |
 | These devices are used in the second layer of our IoT design (the intermediate layer) as connectors. |
| Classification | Bingo–Location 1 | Shisong–Location 2 | Bamenda–Location 3 | Total |
|---|---|---|---|---|
| Can be improved | 5 | 7 | 8 | 20 |
| Minor problem | 0 | 1 | 1 | 2 |
| Serious problem | 4 | 0 | 1 | 5 |
| Critical problem | 1 | 0 | 0 | 1 |
| Catastrophe | 0 | 0 | 0 | 0 |
| Total | 10 | 8 | 10 | 28 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Armand, T.P.T.; Mozumder, M.A.I.; Ali, S.; Amaechi, A.O.; Kim, H.-C. Developing a Low-Cost IoT-Based Remote Cardiovascular Patient Monitoring System in Cameroon. Healthcare 2023, 11, 199. https://doi.org/10.3390/healthcare11020199
Armand TPT, Mozumder MAI, Ali S, Amaechi AO, Kim H-C. Developing a Low-Cost IoT-Based Remote Cardiovascular Patient Monitoring System in Cameroon. Healthcare. 2023; 11(2):199. https://doi.org/10.3390/healthcare11020199
Chicago/Turabian StyleArmand, Tagne Poupi Theodore, Md Ariful Islam Mozumder, Sikandar Ali, Austin Oguejiofor Amaechi, and Hee-Cheol Kim. 2023. "Developing a Low-Cost IoT-Based Remote Cardiovascular Patient Monitoring System in Cameroon" Healthcare 11, no. 2: 199. https://doi.org/10.3390/healthcare11020199
APA StyleArmand, T. P. T., Mozumder, M. A. I., Ali, S., Amaechi, A. O., & Kim, H.-C. (2023). Developing a Low-Cost IoT-Based Remote Cardiovascular Patient Monitoring System in Cameroon. Healthcare, 11(2), 199. https://doi.org/10.3390/healthcare11020199