
Various Surgical Interventions in Treating Odontogenic Keratocyst: A Radiological Case Report


 ,
,  ,
,  ,
, {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
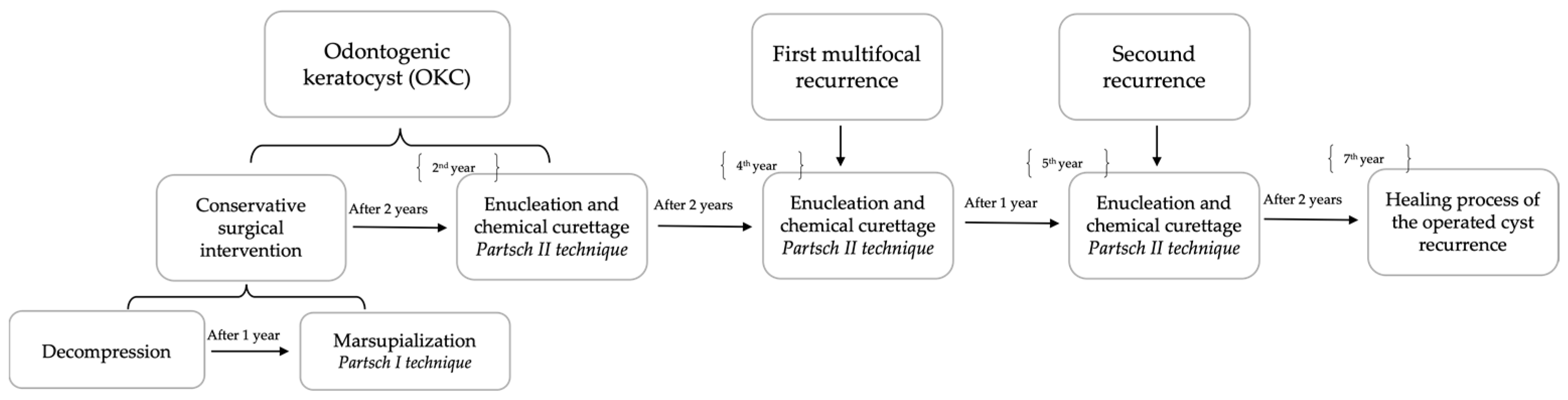
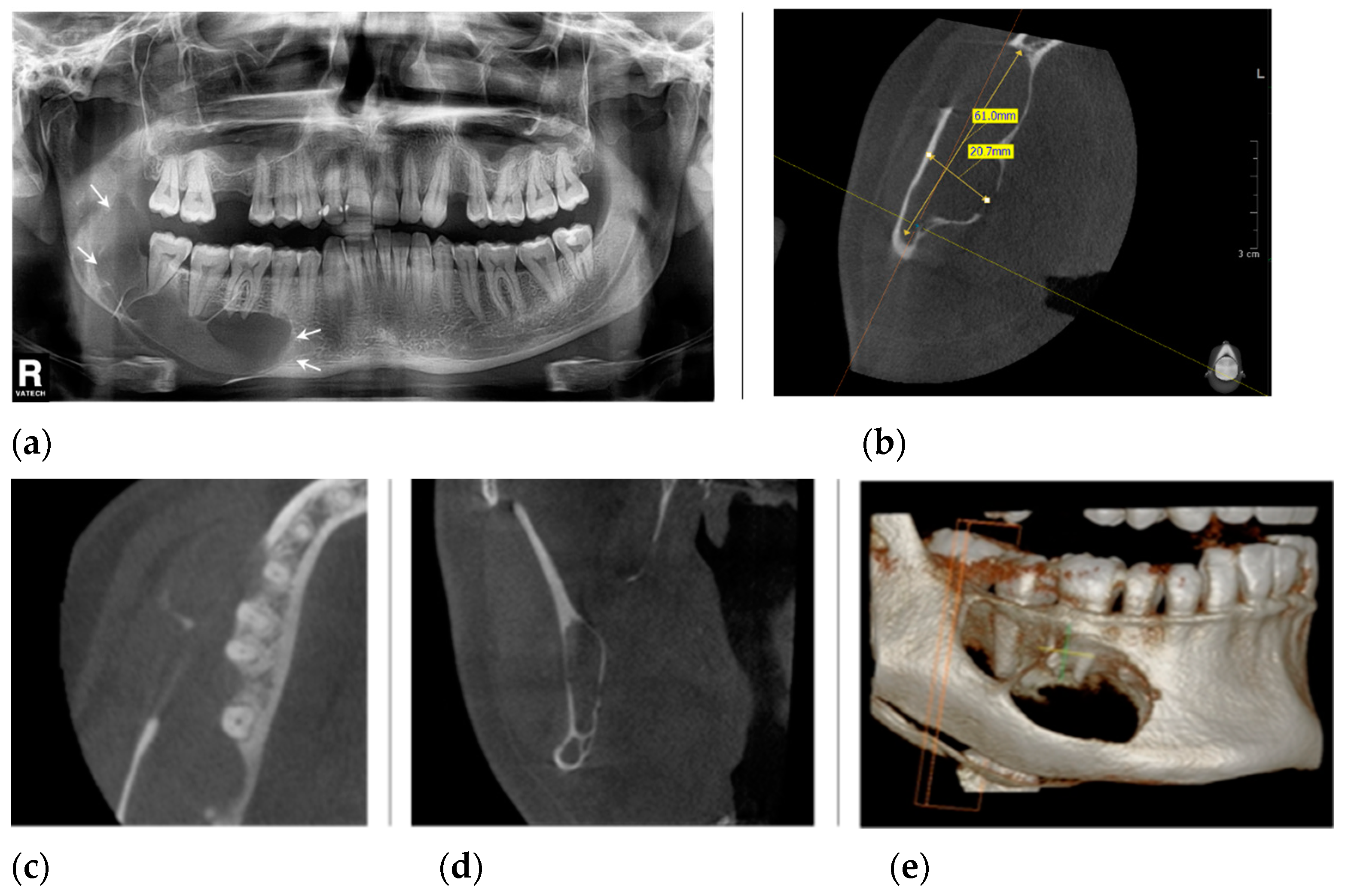
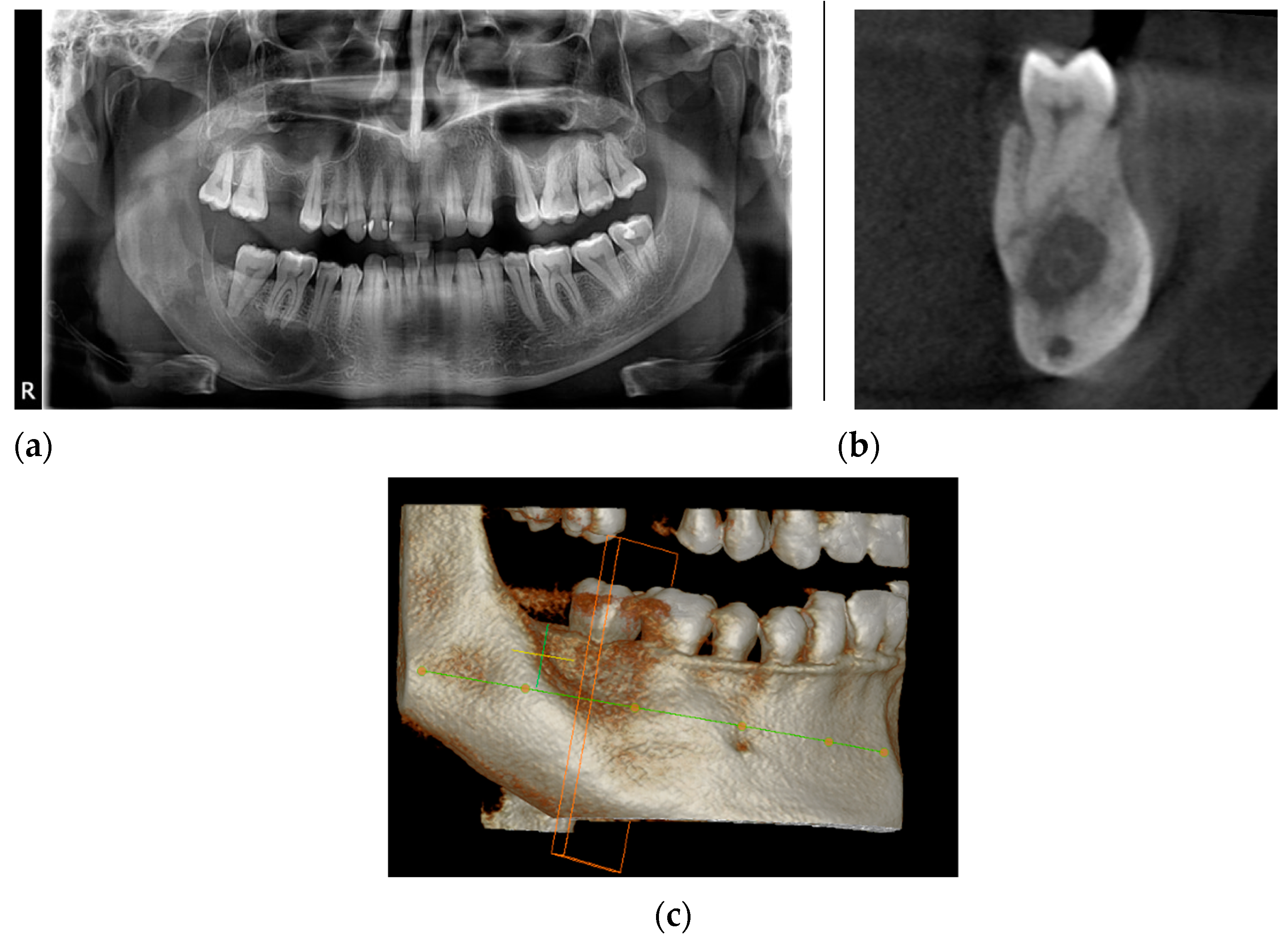
2. Case Presentation
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Reichart, P.; Sciubba, J.J.; Philipsen, H.P. Splitters or lumpers: The 2017 WHO Classification of Head and Neck Tumours. J. Am. Dent. Assoc. 2018, 149, 567–571. [Google Scholar] [CrossRef] [PubMed]
- Polak, K.; Jędrusik-Pawłowska, M.; Drozdzowska, B.; Morawiec, T. Odontogenic keratocyst of the mandible: A case report and literature review. Dent. Med. Probl. 2019, 56, 433–436. [Google Scholar] [CrossRef]
- El-Naggar, A.K.; Chan, J.K.C.; Grandis, J.R.; Takata, T.; Slootweg, P.J. WHO Classification of Head and Neck Tumours; Publisher IARC Press: Lyon, France, 2017; pp. 235–236. [Google Scholar]
- Chen, P.; Liu, B.; Wei, B.; Yu, S. The clinicopathological features and treatments of odontogenic keratocysts. Am. J. Cancer Res. 2022, 12, 3479–3485. [Google Scholar] [PubMed]
- Shear, M. Odontogenic keratocysts: Clinical features. Oral Maxillofac. Surg. Clin. N. Am. 2003, 15, 335–345. [Google Scholar] [CrossRef]
- Myoung, H.; Hong, S.P.; Hong, S.D.; Lee, J.I.; Lim, C.Y.; Choung, P.H.; Lee, J.H.; Choi, J.Y.; Seo, B.M.; Kim, M.J. Odontogenic keratocyst: Review of 256 cases for recurrence and clinicopathologic parameters. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2001, 91, 328–333. [Google Scholar] [CrossRef]
- MacDonald-Jankowski, D.S. Orthokeratinized odontogenic cyst: A systematic review. Dentomaxillofac. Radiol. 2010, 39, 455–467. [Google Scholar] [CrossRef] [PubMed]
- Menon, S. Keratocystic Odontogenic Tumours: Etiology, Pathogenesis and Treatment Revisited. J. Maxillofac. Oral Surg. 2015, 14, 541–547. [Google Scholar] [CrossRef]
- Rajeshkumar, B.P.; Rai, K.K.; Geetha, N.T.; Shivakumar, H.R.; Upasi, A.P. Carnoy’s in Aggressive Lesions: Our Experience. J. Maxillofac. Oral Surg. 2013, 12, 42–47. [Google Scholar] [CrossRef]
- Cutler, E.C.; Zollinger, R. Sclerosing solution in the treatment of cysts and fistulae. Am. J. Surg. 1933, 19, 411–418. [Google Scholar] [CrossRef]
- Donnelly, L.A.; Simmons, T.H.; Blitstein, B.J.; Pham, M.H.; Saha, P.T.; Phillips, C.; White, R.P.; Blakey, G.H. Modified Carnoy’s Compared to Carnoy’s Solution Is Equally Effective in Preventing Recurrence of Odontogenic Keratocysts. J. Oral Maxillofac. Surg. 2021, 79, 1874–1881. [Google Scholar] [CrossRef]
- Cakur, B.; Miloglu, O.; Yolcu, U.; Göregen, M.; Gürsan, N. Keratocystic odontogenic tumour invading the right maxillary sinus: A case report. J. Oral Sci. 2008, 50, 345–349. [Google Scholar] [PubMed]
- Walsh, M.; Hussein, M.A.; Carter, M.; Abdulrahman, S. Maxillary Odontogenic Keratocyst. J. Surg. Case Rep. 2022, 2022, rjac078. [Google Scholar] [CrossRef] [PubMed]
- Díaz-Belenguer, Á.; Sánchez-Torres, A.; Gay-Escoda, C. Role of Carnoy’s solution in the treatment of keratocystic odontogenic tumor: A systematic review. Med. Oral Patol. Oral Cir. Bucal. 2016, 21, e689–e695. [Google Scholar] [CrossRef]
- Woolgar, A.; Rippin, J.W.; Browne, R.M. A comparative study of the clinical and histological features of recurrent and non recurrent odontogenic keratocysts. Oral Pathol. Med. 1987, 16, 124–128. [Google Scholar] [CrossRef] [PubMed]
- Forssel, K.; Forssel, H.; Kahnberg, K.E. Recurrence of keratocysts in a long-term follow-up study. Int. J. Oral Maxillofac. Surg. 1988, 17, 25–28. [Google Scholar]
- Borghesi, A.; Nardi, C.; Giannitto, C.; Tironi, A.; Maroldi, R.; Di Bartolomeo, F.; Preda, L. Odontogenic keratocyst: Imaging features of a benign lesion with an aggressive behaviour. Insights Imaging. 2018, 9, 883–897. [Google Scholar] [CrossRef]
- González-Alva, P.; Tanaka, A.; Oku, Y.; Yoshizawa, D.; Itoh, S.; Sakashita, H.; Ide, F.; Tajima, Y.; Kusama, K. Keratocystic odontogenic tumor: A retrospective study of 183 cases. J. Oral Sci. 2008, 50, 205–212. [Google Scholar] [CrossRef]
- Kuroyanagi, N.; Sakuma, H.; Miyabe, S.; Machida, J.; Kaetsu, A.; Yokoi, M.; Maeda, H.; Warnakulasuriya, S.; Nagao, T.; Shimozato, K. Prognostic factors for keratocystic odontogenic tumor (odontogenic keratocyst): Analysis of clinico-pathologic and immunohistochemical findings in cysts treated by enucleation. J. Oral Pathol. Med. 2009, 38, 386–392. [Google Scholar] [CrossRef]
- Stoelinga, P.J. The treatment of odontogenic keratocysts by excision of the overlying, attached mucosa, enucleation, and treatment of the bony defect with Carnoy solution. J. Oral Maxillofac. Surg. 2005, 63, 1662–1666. [Google Scholar] [CrossRef] [PubMed]
- Mendes, R.A.; Carvalho, J.F.; van der Waal, I. Characterization and management of the keratocystic odontogenic tumor in relation to its histopathological and biological features. Oral Oncol. 2010, 46, 219–225. [Google Scholar] [CrossRef]
- Pogrel, M.A. Decompression and marsupialization as a treatment for the odontogenic keratocyst. Oral Maxillofac. Surg. Clin. N. Am. 2003, 15, 415–427. [Google Scholar] [CrossRef] [PubMed]
- Wushou, A.; Zhao, Y.J.; Shao, Z.M. Marsupialization is the optimal treatment approach for keratocystic odontogenic tumour. J. Cranio-Maxillofac. Surg. 2014, 42, 1540–1544. [Google Scholar] [CrossRef] [PubMed]
- Blanas, N.; Freund, B.; Schwartz, M.; Furst, I.M. Systematic review of the treatment and prognosis of the odontogenic keratocyst. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2000, 90, 553–558. [Google Scholar] [CrossRef] [PubMed]
- Dashow, J.E.; McHugh, J.B.; Braun, T.M.; Edwards, S.P.; Helman, J.I.; Ward, B.B. Significantly Decreased Recurrence Rates in Keratocystic Odontogenic Tumor With Simple Enucleation and Curettage Using Carnoy’s Versus Modified Carnoy’s Solution. J. Oral Maxillofac. Surg. 2015, 73, 2132–2135. [Google Scholar] [CrossRef] [PubMed]
- Kaczmarzyk, T.; Kisielowski, K.; Koszowski, R.; Rynkiewicz, M.; Gawełek, E.; Babiuch, K.; Bednarczyk, A.; Drozdzowska, B. Investigation of clinicopathological parameters and expression of COX-2, bcl-2, PCNA, and p53 in primary and recurrent sporadic odontogenic keratocysts. Clin. Oral Investig. 2018, 22, 3097–3106. [Google Scholar] [CrossRef]
- Raut, M.S.; Bansal, S.; Desai, R.S.; Raut, B.S. A comparative immunohistochemical analysis of cortactin in orthokeratinized odontogenic cyst (OOC), sporadic odontogenic keratocyst (OKC), and syndromic OKC. J. Oral Biosci. 2021, 63, 444–449. [Google Scholar] [CrossRef]
- Borrás-Ferreres, J.; Sánchez-Torres, A.; Alberdi-Navarro, J.; Aguirre-Urizar, J.M.; Mosqueda-Taylor, A.; Gay-Escoda, C. Therapeutic management of the odontogenic keratocyst. An energetic approach with a conservative perspective and review of the current therapeutic options. J. Clin. Exp. Dent. 2020, 12, e794–e799. [Google Scholar] [CrossRef]
- Doll, C.; Dauter, K.; Jöhrens, K.; Hartwig, S.; Voss, J.O.; Klein, M.; Heiland, M.; Raguse, J.D. Clinical characteristics and immunohistochemical analysis of p53, Ki-67 and cyclin D1 in 80 odontogenic keratocysts. J. Stomatol. Oral Maxillofac. Surg. 2018, 119, 359–364. [Google Scholar] [CrossRef] [PubMed]








Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gelețu, G.L.; Burlacu, A.; Baciu, E.-R.; Diaconu-Popa, D.; Murariu, A.; Foia, L.G.; Ungureanu, L.; Onică, N. Various Surgical Interventions in Treating Odontogenic Keratocyst: A Radiological Case Report. Healthcare 2023, 11, 416. https://doi.org/10.3390/healthcare11030416
Gelețu GL, Burlacu A, Baciu E-R, Diaconu-Popa D, Murariu A, Foia LG, Ungureanu L, Onică N. Various Surgical Interventions in Treating Odontogenic Keratocyst: A Radiological Case Report. Healthcare. 2023; 11(3):416. https://doi.org/10.3390/healthcare11030416
Chicago/Turabian StyleGelețu, Gabriela Luminița, Alexandru Burlacu, Elena-Raluca Baciu, Diana Diaconu-Popa, Alice Murariu, Liliana Georgeta Foia, Loredana Ungureanu, and Neculai Onică. 2023. "Various Surgical Interventions in Treating Odontogenic Keratocyst: A Radiological Case Report" Healthcare 11, no. 3: 416. https://doi.org/10.3390/healthcare11030416
APA StyleGelețu, G. L., Burlacu, A., Baciu, E.-R., Diaconu-Popa, D., Murariu, A., Foia, L. G., Ungureanu, L., & Onică, N. (2023). Various Surgical Interventions in Treating Odontogenic Keratocyst: A Radiological Case Report. Healthcare, 11(3), 416. https://doi.org/10.3390/healthcare11030416