Determinants of Acquisition, Persistence, and Clearance of Oncogenic Cervical Human Papillomavirus Infection in the Philippines Using a Multi-Omics Approach: DEFEAT HPV Study Protocol

 ,
,  ,
,  , ,
, ,  , , , ,
, , , , {kind=link}
Abstract
:1. Introduction
2. Materials and Methods
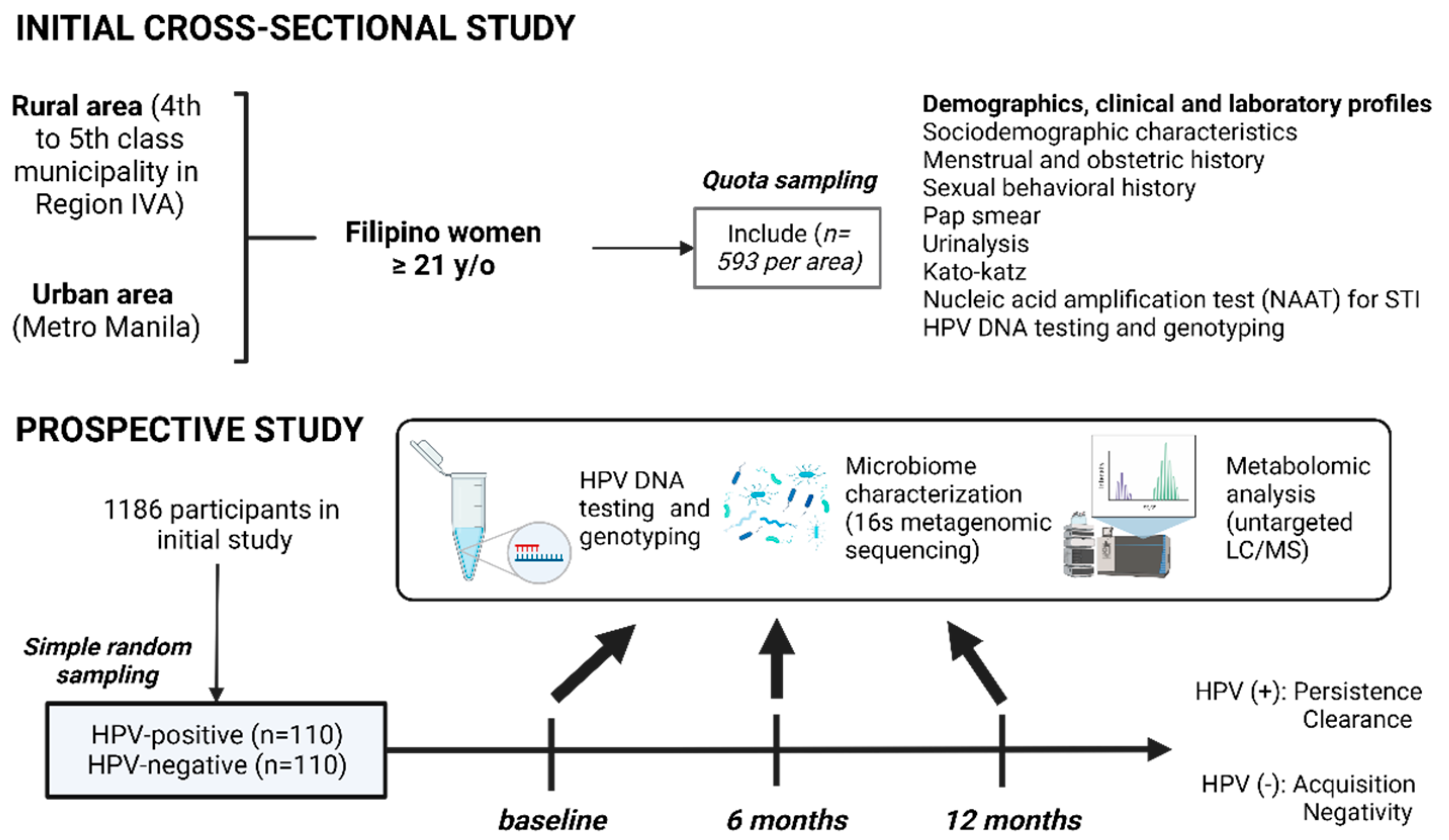
2.1. Study Design
2.2. Sampling Design
2.3. Sample Size
2.4. Study Sites
2.5. Study Population
2.5.1. Inclusion Criteria
2.5.2. Exclusion Criteria
2.6. Study Procedure
2.6.1. Process for Securing Consent from the Participants
2.6.2. Referral Plan
2.6.3. Grouping of HPV Status at One-Year Follow-Up
2.7. Data Collection Tools
2.7.1. Clinical Interview and Examination
2.7.2. Sample Collection and Transport
2.7.3. Genomic DNA Extraction
2.7.4. HPV Genotyping
2.7.5. Detection of Lower Reproductive Tract Infections
2.7.6. 16S Amplicon Metagenomic Sequencing Using 454 GS-FLX Plus
2.7.7. Metabolite Extraction and Separation Using LC/MS
2.8. Quality Control
2.9. Statistical Analyses
2.10. Ethical Consideration
3. Results
4. Discussion
Limitations of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bruni, L.; Albero, G.; Serrano, B.; Mena, M.; Collado, J.; Gomez, D.; Munoz, J.; Bosch, F.X.; de Sanjose, S. Human Papillomavirus and Related Diseases in the World. Summary Report 22 October 2021; ICO/IARC Information Centre on HPV and Cancer (HPV Information Centre): Barcelona, Spain, 2021; pp. 1–314. [Google Scholar]
- Bruni, L.; Albero, G.; Serrano, B.; Mena, M.; Collado, J.; Gómez, D.; Muñoz, J.; Bosch, F.; de Sanjosé, S. Human Papillomavirus and Related Diseases in United States of America. Summary Report 22 October 2021; ICO/IARC Information Centre on HPV and Cancer (HPV Information Centre): Barcelona, Spain, 2021. [Google Scholar]
- Bruni, L.; Albero, G.; Serrano, B.; Mena, M.; Collado, J.J.; Gomez, D.; Muñoz, J.; Bosch, F.X.; de Sanjosé, S. Human Papillomavirus and Related Diseases in China. Summary Report 22 October 2021; ICO/IARC Information Centre on HPV and Cancer (HPV Information Centre): Barcelona, Spain, 2021. [Google Scholar]
- Razzaghi, H.; Saraiya, M.; Thompson, T.D.; Henley, S.J.; Viens, L.; Wilson, R. Five-Year Relative Survival for Human Papillomavirus-Associated Cancer Sites. Cancer 2018, 124, 203–211. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cancer Statistics Working Group U.S. Cancer Statistics Data Visualizations Tool, Based on 2021 Submission Data (1999–2019): U.S. Department of Health and Human Services, Centers for Disease Control and Prevention and National Cancer Institute. Available online: https://www.cdc.gov/cancer/uscs/dataviz/index.htm (accessed on 1 October 2022).
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [Green Version]
- Chilaka, V.N.; Navti, O.B.; al Beloushi, M.; Ahmed, B.; Konje, J.C. Human Papillomavirus (HPV) in Pregnancy—An Update. Eur. J. Obstet. Gynecol. Reprod. Biol. 2021, 264, 340–348. [Google Scholar] [CrossRef]
- Laudico, A.V.; Mirasol-Lumague, M.R.; Medina, V.; Mapua, C.A.; Valenzuela, F.G.; Pukkala, E. Philippine Cancer Facts and Estimates; Philippine Cancer Society: Manila, Philippines, 2015; Available online: https://www.philcancer.org.ph/images/pdf/data/2010-Philippine-Cancer-Facts-Estimates.pdf (accessed on 1 October 2022).
- Bosch, F.X.; Manos, M.M.; Muñoz, N.; Sherman, M.; Jansen, A.M.; Peto, J.; Schiffman, M.H.; Moreno, V.; Kurman, R.; Shan, K.V. Prevalence of Human Papillomavirus in Cervical Cancer: A Worldwide Perspective. J. Natl. Cancer Inst. 1995, 87, 796–802. [Google Scholar] [CrossRef]
- Ngelangel, C.; Muñoz, N.; Bosch, F.X.; Limson, G.M.; Festin, M.R.; Deacon, J.; Jacobs, M.V.; Santamaria, M.; Meijer, C.J.; Walboomers, J.M. Causes of Cervical Cancer in the Philippines: A Case-Control Study. J. Natl. Cancer Inst. 1998, 90, 43–49. [Google Scholar] [CrossRef] [Green Version]
- Sherris, J.; Herdman, C.; Elias, C. Cervical Cancer in the Developing World. West. J. Med. 2001, 175, 231–233. [Google Scholar] [CrossRef] [Green Version]
- Tadesse, S.K. Socio-Economic and Cultural Vulnerabilities to Cervical Cancer and Challenges Faced by Patients Attending Care at Tikur Anbessa Hospital: A Cross Sectional and Qualitative Study. BMC Womens Health 2015, 15, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Walboomers, J.; Jacobs, M.; Manos, M.; Bosch, F.; Kummer, J.; Shah, K.; Snijders, P.J.F.; Peto, J.; Meijer, C.J.L.; Munoz, N. Human Papillomavirus Is a Necessary Cause. J. Pathol. 1999, 189, 12–19. [Google Scholar] [CrossRef]
- Burd, E.M. Human Papillomavirus and Cervical Cancer. Clin. Microbiol. Rev. 2003, 16, 1–17. [Google Scholar] [CrossRef] [Green Version]
- Münger, K.; Baldwin, A.; Edwards, K.M.; Hayakawa, H.; Nguyen, C.L.; Owens, M.; Grace, M.; Huh, K. Mechanisms of Human Papillomavirus-Induced Oncogenesis. J. Virol. 2004, 78, 11451–11460. [Google Scholar] [CrossRef] [Green Version]
- Chan, P.K.S.; Chang, A.R.; Cheung, J.L.K.; Chan, D.P.C.; Xu, L.Y.; Tang, N.L.S.; Cheng, A.F. Determinants of Cervical Human Papillomavirus Infection: Differences between High-and Low-Oncogenic Risk Types. J. Infect. Dis. 2002, 185, 28–35. [Google Scholar] [CrossRef]
- Lorincz, A.T.; Reid, R.; Jenson, B.A.; Greenberg, M.D.; Lancaster, W.; Kurman, R.J. Human Papillomavirus Infection of the Cervix: Relative Risk Associations of 15 Common Anogenital Types. Obstet. Gynecol. 1992, 79, 328–337. [Google Scholar] [CrossRef]
- Faridi, R.; Zahra, A.; Khan, K.; Idrees, M. Oncogenic Potential of Human Papillomavirus (HPV) and Its Relation with Cervical Cancer. Virol. J. 2011, 8, 269. [Google Scholar] [CrossRef] [Green Version]
- Ramakrishnan, S.; Partricia, S.; Mathan, G. Overview of High-Risk HPV’s 16 and 18 Infected Cervical Cancer: Pathogenesis to Prevention. Biomed. Pharmacother. 2015, 70, 103–110. [Google Scholar] [CrossRef]
- Conway, M.J.; Alam, S.; Ryndock, E.J.; Cruz, L.; Christensen, N.D.; Roden, R.B.S.; Meyers, C. Tissue-Spanning Redox Gradient-Dependent Assembly of Native Human Papillomavirus Type 16 Virions. J. Virol. 2009, 83, 10515–10526. [Google Scholar] [CrossRef] [Green Version]
- Domingo, E.J.; Dy Echo, A.V.V. Epidemiology, Prevention and Treatment of Cervical Cancer in the Philippines. J. Gynecol. Oncol. 2009, 20, 11–16. [Google Scholar] [CrossRef] [Green Version]
- Carr, S.; Hespe, C. Cervical Cancer Screening in Low-Income Countries: A Report on the Implementation of Cervical Screening in Luzon, Philippines. J. Glob. Heal. Rep. 2020, 4, e2020071. [Google Scholar] [CrossRef]
- Lintao, R.C.V.; Cando, L.F.T.; Perias, G.A.S.; Tantengco, O.A.G.; Tabios, I.K.B.; Velayo, C.L.; de Paz-Silava, S.L.M. Current Status of Human Papillomavirus Infection and Cervical Cancer in the Philippines. Front. Med. 2022, 9, 1805. [Google Scholar] [CrossRef]
- Tantengco, O.A.G.; Nakura, Y.; Yoshimura, M.; Llamas-Clark, E.F.; Yanagihara, I. Association of PIK3CA and MDM2 SNP309 with Cervical Squamous Cell Carcinoma in a Philippine Population. Asian Pac. J. Cancer Prev. 2019, 20, 2103–2107. [Google Scholar] [CrossRef]
- Bruni, L.; Albero, G.; Serrano, B.; Mena, M.; Collado, J.; Gómez, D.; Muñoz, J.; Bosch, F.X.; de Sanjosé, S. Philippines: Human Papillomavirus and Related Diseases Report; ICO/IARC Information Centre on HPV and Cancer (HPV Information Centre): Barcelona, Spain, 2021. [Google Scholar]
- Brisson, M.; Kim, J.J.; Canfell, K.; Drolet, M.; Gingras, G.; Burger, E.A.; Martin, D.; Simms, K.T.; Bénard, É.; Boily, M.-C.; et al. Impact of HPV Vaccination and Cervical Screening on Cervical Cancer Elimination: A Comparative Modelling Analysis in 78 Low-Income and Lower-Middle-Income Countries. Lancet 2020, 395, 575–590. [Google Scholar] [CrossRef] [Green Version]
- El-Zein, M.; Richardson, L.; Franco, E.L. Cervical Cancer Screening of HPV Vaccinated Populations: Cytology, Molecular Testing, Both or None. J. Clin. Virol. 2016, 76, S62–S68. [Google Scholar] [CrossRef] [Green Version]
- Gates, A.; Pillay, J.; Reynolds, D.; Stirling, R.; Traversy, G.; Korownyk, C.; Moore, A.; Thériault, G.; Thombs, B.D.; Little, J.; et al. Screening for the Prevention and Early Detection of Cervical Cancer: Protocol for Systematic Reviews to Inform Canadian Recommendations. Syst. Rev. 2021, 10, 1–22. [Google Scholar] [CrossRef]
- Victor Manuel, V. Screening and Prevention of Cervical Cancer in the World. J. Gynecol. Res. Obstet. 2017, 3, 86–92. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Comprehensive Cervical Cancer Control: A Guide to Essential Practice, 2nd ed.; World Health Organization: Geneva, Switzerland, 2014. [Google Scholar]
- World Health Organization. WHO Guideline for Screening and Treatment of Cervical Pre-Cancer Lesions for Cervical Cancer Prevention, 2nd ed.; World Health Organization: Geneva, Switzerland, 2021. [Google Scholar]
- Mishra, G.A.; Pimple, S.A.; Shastri, S.S. An Overview of Prevention and Early Detection of Cervical Cancers. Indian J. Med. Paediatr. Oncol. 2011, 32, 125–132. [Google Scholar] [CrossRef] [Green Version]
- McGraw, S.L.; Ferrante, J.M. Update on prevention and screening of cervical cancer. World J. Clin. Oncol. 2014, 5, 744–752. [Google Scholar] [CrossRef]
- Zhang, Z.; Zhang, D.; Xiao, B.B.; Zhang, R.; Bai, H.H.; Dong, H.Y.; Bi, H.; Liu, Z.H. Primary study on the relationship between high-risk HPV infection and vaginal cervical microbiota. Zhonghua Fu Chan Ke Za Zhi 2018, 53, 471–480. [Google Scholar] [CrossRef]
- Guerrero, A.M.; Genuino, A.J.; Santillan, M.; Praditsitthikorn, N.; Chantarastapornchit, V.; Teerawattananon, Y.; Alejandria, M.; Toral, J.A. A Cost-Utility Analysis of Cervical Cancer Screening and Human Papillomavirus Vaccination in the Philippines. BMC Public Health 2015, 15. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Cervical Cancer Country Profiles; World Health Organization: Geneva, Switzerland, 2021. [Google Scholar]
- Department of Health Philippines. Administrative Order No. 2005–2006: Establishment of a Cervical Cancer Screening Program; Department of Health: Manila, Philippines, 2005.
- Ngelangel, C.A.; Limson, G.M.; Ramiro, L.S.; Abelardo, A.; Avila, J.M.; Cordero, C.; Delgado, A.; Fajutrao, L.; Tan-Torres, T.; Banzon, E.; et al. Delineation of an Appropriate and Replicable Cervical Cancer Screening Program for Filipino Women. In Proceedings of the 1st Health Research for Action, Manila, Philippines, 28 June 2001; University of the Philippines Manila-Department of Health: Manila, Philippines, 2001; pp. 84–88. [Google Scholar]
- Bruni, L.; Serrano, B.; Roura, E.; Alemany, L.; Cowan, M.; Herrero, R.; Poljak, M.; Murillo, R.; Broutet, N.; Riley, L.M.; et al. Cervical Cancer Screening Programmes and Age-Specific Coverage Estimates for 202 Countries and Territories Worldwide: A Review and Synthetic Analysis. Lancet Glob. Health 2022, 10, e1115–e1127. [Google Scholar] [CrossRef]
- WHO. Global Strategy to Accelerate the Elimination of Cervical Cancer as a Public Health Problem; WHO: Geneva, Switzerland, 2020. [Google Scholar]
- Ho, F.D.V.; Arevalo, M.V.P.N.; de Claro, P.T.S.; Jacomina, L.E.; Germar, M.J.V.; Dee, E.C.; Eala, M.A.B. Breast and Cervical Cancer Screening in the Philippines: Challenges and Steps Forward. Prev. Med. Rep. 2022, 29. [Google Scholar] [CrossRef]
- Zhao, S.; Huang, L.; Basu, P.; Domingo, E.J.; Supakarapongkul, W.; Ling, W.Y.; Ocviyanti, D.; Rezhake, R.; Qiao, Y.; Tay, E.H.; et al. Cervical Cancer Burden, Status of Implementation and challenges of Cervical Cancer Screening in Association of Southeast Asian (ASEAN) Countries. Cancer Lett. 2022, 525, 22–32. [Google Scholar] [CrossRef]
- Dayrit, M.M.; Lagrada, L.P.; Picazo, O.F.; Pons, M.C.; Villaverde, M.C. Health Systems in Transition: The Philippines Health System Review, 2nd ed.; Regional Office for South-East Asia; World Health Organization: Geneva, Switzerland, 2018; Volume 8. [Google Scholar]
- Krassowski, M.; Das, V.; Sahu, S.K.; Misra, B.B. State of the Field in Multi-Omics Research: From Computational Needs to Data Mining and Sharing. Front. Genet. 2020, 11, 610798. [Google Scholar] [CrossRef]
- Kumari Duppala, S.; Yadala, R.; Velingkar, A.; Suravajhala, P.; Pawar, S.C.; Vuree, S. Integrative Multi-Omics Approaches for Identifying Cervical Cancer Therapeutic Targets. bioRxiv 2022. [Google Scholar] [CrossRef]
- Iden, M.; Tsaih, S.W.; Huang, Y.W.; Liu, P.; Xiao, M.; Flister, M.J.; Rader, J.S. Multi-Omics Mapping of Human Papillomavirus Integration Sites Illuminates Novel Cervical Cancer Target Genes. Br. J. Cancer 2021, 125, 1408–1419. [Google Scholar] [CrossRef]
- Łaniewski, P.; Barnes, D.; Goulder, A.; Cui, H.; Roe, D.J.; Chase, D.M.; Herbst-Kralovetz, M.M. Linking Cervicovaginal Immune Signatures, HPV and Microbiota Composition in Cervical Carcinogenesis in Non-Hispanic and Hispanic Women. Sci. Rep. 2018, 8, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Chase, D.; Goulder, A.; Zenhausern, F.; Monk, B.; Herbst-Kralovetz, M. The Vaginal and Gastrointestinal Microbiomes in Gynecologic Cancers: A Review of Applications in Etiology, Symptoms and Treatment. Gynecol. Oncol. 2015, 138, 190–200. [Google Scholar] [CrossRef]
- Audirac-Chalifour, A.; Torres-Poveda, K.; Bahena-Román, M.; Téllez-Sosa, J.; Martínez-Barnetche, J.; Cortina-Ceballos, B.; López-Estrada, G.; Delgado-Romero, K.; Burguete-García, A.I.; Cantú, D.; et al. Cervical Microbiome and Cytokine Profile at Various Stages of Cervical Cancer: A Pilot Study. PLoS ONE 2016, 11, e0153274. [Google Scholar] [CrossRef] [Green Version]
- Arokiyaraj, S.; Seo, S.S.; Kwon, M.; Lee, J.K.; Kim, M.K. Association of Cervical Microbial Community with Persistence, Clearance and Negativity of Human Papillomavirus in Korean Women: A Longitudinal Study. Sci. Rep. 2018, 8, 15479. [Google Scholar] [CrossRef] [Green Version]
- Usyk, M.; Zolnik, C.P.; Castle, P.E.; Porras, C.; Herrero, R.; Gradissimo, A.; Gonzalez, P.; Safaeian, M.; Schiffman, M.; Burk, R.D. Cervicovaginal Microbiome and Natural History of HPV in a Longitudinal Study. PLoS Pathog. 2020, 16, e1008376. [Google Scholar] [CrossRef] [Green Version]
- Norenhag, J.; Du, J.; Olovsson, M.; Verstraelen, H.; Engstrand, L.; Brusselaers, N. The Vaginal Microbiota, Human Papillomavirus and Cervical Dysplasia: A Systematic Review and Network Meta-Analysis. BJOG 2020, 127, 171–180. [Google Scholar] [CrossRef]
- Brusselaers, N.; Shrestha, S.; van de Wijgert, J.; Verstraelen, H. Vaginal Dysbiosis and the Risk of Human Papillomavirus and cervical Cancer: Systematic Review and Meta-Analysis. Am. J. Obstet. Gynecol. 2019, 221, 9–18.e8. [Google Scholar] [CrossRef]
- Casals-Pascual, C.; González, A.; Vázquez-Baeza, Y.; Song, S.J.; Jiang, L.; Knight, R. Microbial Diversity in Clinical Microbiome Studies: Sample Size and Statistical Power Considerations. Gastroenterology 2020, 158, 1524–1528. [Google Scholar] [CrossRef]
- ICO/IARC Information Centre on HPV and Cancer. Philippines Human Papillomavirus and Related Cancers, Fact Sheet 2017; ICO/IARC Information Centre on HPV and Cancer: Barcelona, Spain, 2017; Volume 2017. [Google Scholar]
- Philippe, G. Sampsize. Available online: https://sampsize.sourceforge.net/iface/index.html (accessed on 1 August 2022).
- Tantengco, O.A.G.; Nakura, Y.; Yoshimura, M.; Nishiumi, F.; Llamas-Clark, E.F.; Yanagihara, I. Co-Infection of Human Papillomavirus and Other Sexually Transmitted Bacteria in Cervical Cancer Patients in the Philippines. Gynecol. Oncol. Rep. 2022, 40, 100943. [Google Scholar] [CrossRef]
- Baasland, I.; Romundstad, P.R.; Eide, M.L.; Jonassen, C.M. Clinical Performance of Anyplex II HPV28 by Human Papillomavirus Type and Viral Load in a Referral Population. PLoS ONE 2019, 14, e0210997. [Google Scholar] [CrossRef] [Green Version]
- Estrade, C.; Sahli, R. Comparison of Seegene Anyplex II HPV28 with the PGMY-CHUV Assay for Human Papillomavirus Genotyping. J. Clin. Microbiol. 2014, 52, 607–612. [Google Scholar] [CrossRef] [Green Version]
- Bodiybadu, K.; Danielewski, J.; Plummer, E.; Bradshaw, C.S.; Machalek, D.A.; Garland, S.M.; Vodstrcil, L.A.; Murray, G.L. Comparison of Seegene AnyPlexTM II STI-7e with Standard-of-Care Diagnostic Methods for the Detection of Mycoplasma Genitalium, Chlamydia Trachomatis, Neisseria Gonorrhoeae, and Trichomonas Vaginalis. Lett. Appl. Microbiol. 2023, 76, ovac002. [Google Scholar] [CrossRef]
- Choe, H.-S.; Lee, D.S.; Lee, S.-J.; Hong, S.-H.; Park, D.C.; Lee, M.-K.; Kim, T.-H.; Cho, Y.-H. Performance of AnyplexTM II Multiplex Real-Time PCR for the Diagnosis of Seven Sexually Transmitted Infections: Comparison with Currently Available Methods. Int. J. Infect. Dis. 2013, 17, e1134–e1140. [Google Scholar] [CrossRef] [Green Version]
- Amsel, R.; Totten, P.A.; Spiegel, C.A.; Chen, K.C.; Eschenbach, D.; Holmes, K.K. Nonspecific Vaginitis. Diagnostic Criteria and Microbial and Epidemiologic Associations. Am. J. Med. 1983, 74, 14–22. [Google Scholar] [CrossRef]
- Nugent, R.P.; Krohn, M.A.; Hillier, S.L. Reliability of Diagnosing Bacterial Vaginosis Is Improved by a Standardized Method of Gram Stain Interpretation. J. Clin. Microbiol. 1991, 29, 297–301. [Google Scholar] [CrossRef] [Green Version]
- Sha, B.E.; Chen, H.Y.; Wang, Q.J.; Zariffard, M.R.; Cohen, M.H.; Spear, G.T. Utility of Amsel Criteria, Nugent Score, and Quantitative PCR for Gardnerella Vaginalis, Mycoplasma Hominis, and Lactobacillus Spp. for Diagnosis of Bacterial Vaginosis in Human Immunodeficiency Virus-Infected Women. J. Clin. Microbiol. 2005, 43, 4607–4612. [Google Scholar] [CrossRef] [Green Version]
- Khan, I.; Nam, M.; Kwon, M.; Seo, S.-S.; Jung, S.; Han, J.S.; Hwang, G.-S.; Kim, M.K. LC/MS-Based Polar Metabolite Profiling Identified Unique Biomarker Signatures for Cervical Cancer and Cervical Intraepithelial Neoplasia Using Global and Targeted Metabolomics. Cancers 2019, 11, 511. [Google Scholar] [CrossRef] [Green Version]
- Bruni, L.; Saura-Lázaro, A.; Montoliu Alexandra and Brotons, M.; Alemany, L.; Diallo Mamadou Saliou and Afsar, O.Z.; LaMontagne, D.S.; Mosina, L.; Contreras, M.; Velandia-González, M.; Pastore, R.; et al. HPV Vaccination Introduction Worldwide and WHO and UNICEF of National HPV Immunization Coverage 2010–2019. Prev. Med. 2021, 144, 106399. [Google Scholar] [CrossRef]
- World Health Organization. Human Papillomavirus (HPV) Vaccination Coverage. Available online: https://immunizationdata.who.int/pages/coverage/hpv.html (accessed on 1 August 2022).
- World Health Organization. Regional Office for South-East Asia. Accelerating the Elimination of Cervical Cancer as a Global Public Health Problem. World Health Organization. Regional Office for South-East Asia. 2019. Available online: https://apps.who.int/iris/handle/10665/327911 (accessed on 1 August 2022).
- Simelela, P.N. WHO Global Strategy to Eliminate Cervical Cancer as a Public Health Problem: An Opportunity to Make It a Disease of the Past. Int. J. Gynecol. Obstet. 2021, 152, 1–3. [Google Scholar] [CrossRef]
- Department of Health. Department Memorandum No. 2015-0316: Guidelines in the Implementation of Human Papillomavirus (HPV) Vaccination. Available online: https://doh.gov.ph/sites/default/files/health_programs/DM%202015-0316%20Guidelines%20in%20the%20Implementation%20of%20HPV%20Vaccination_0.pdf (accessed on 1 October 2022).
- Philippine Statistics Authority. Health Spending Registered 12.6 Percent Growth, Share of Health to Economy Went Up to 5.6 Percent in 2020. Philippine Statistics Authority Reference Number: 2021-427. Available online: https://psa.gov.ph/pnha-press-release/node/165216 (accessed on 1 October 2022).
- Smith, M.A.; Canfell, K. Projected Impact of HPV Vaccination and Primary HPV Screening on Cervical Adenocarcinoma: Example from Australia. Papillomavirus Res. 2017, 3, 134–141. [Google Scholar] [CrossRef]
- Launch of SUCCESS Project in the Philippines Intensifies Fight against Cervical Cancer. Available online: https://Ph.Ambafrance.Org/Launch-of-SUCCESS-Project-in-the-Philippines-Intensifies-Fight-against-Cervical (accessed on 1 December 2022).
- World Health Organization. Regional Office for South-East Asia Accelerating the Elimination of Cervical Cancer as a Public Health Problem: Towards Achieving 90–70–90 Targets by 2030; World Health Organization: Geneva, Switzerland, 2022. [Google Scholar]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
de Paz-Silava, S.L.M.; Tabios, I.K.B.; Tantengco, O.A.G.; Climacosa, F.M.M.; Velayo, C.L.; Lintao, R.C.V.; Cando, L.F.T.; Perias, G.A.S.; Idolor, M.I.C.; Francisco, A.G.; et al. Determinants of Acquisition, Persistence, and Clearance of Oncogenic Cervical Human Papillomavirus Infection in the Philippines Using a Multi-Omics Approach: DEFEAT HPV Study Protocol. Healthcare 2023, 11, 658. https://doi.org/10.3390/healthcare11050658
de Paz-Silava SLM, Tabios IKB, Tantengco OAG, Climacosa FMM, Velayo CL, Lintao RCV, Cando LFT, Perias GAS, Idolor MIC, Francisco AG, et al. Determinants of Acquisition, Persistence, and Clearance of Oncogenic Cervical Human Papillomavirus Infection in the Philippines Using a Multi-Omics Approach: DEFEAT HPV Study Protocol. Healthcare. 2023; 11(5):658. https://doi.org/10.3390/healthcare11050658
Chicago/Turabian Stylede Paz-Silava, Sheriah Laine M., Ian Kim B. Tabios, Ourlad Alzeus G. Tantengco, Fresthel Monica M. Climacosa, Clarissa L. Velayo, Ryan C. V. Lintao, Leslie Faye T. Cando, Glenmarie Angelica S. Perias, Maria Isabel C. Idolor, Abialbon G. Francisco, and et al. 2023. "Determinants of Acquisition, Persistence, and Clearance of Oncogenic Cervical Human Papillomavirus Infection in the Philippines Using a Multi-Omics Approach: DEFEAT HPV Study Protocol" Healthcare 11, no. 5: 658. https://doi.org/10.3390/healthcare11050658
APA Stylede Paz-Silava, S. L. M., Tabios, I. K. B., Tantengco, O. A. G., Climacosa, F. M. M., Velayo, C. L., Lintao, R. C. V., Cando, L. F. T., Perias, G. A. S., Idolor, M. I. C., Francisco, A. G., Catral, C. D. M., Chiong, C. M., & Dalmacio, L. M. M. (2023). Determinants of Acquisition, Persistence, and Clearance of Oncogenic Cervical Human Papillomavirus Infection in the Philippines Using a Multi-Omics Approach: DEFEAT HPV Study Protocol. Healthcare, 11(5), 658. https://doi.org/10.3390/healthcare11050658