
Impact of Sertraline, Fluoxetine, and Escitalopram on Psychological Distress among United States Adult Outpatients with a Major Depressive Disorder



Abstract
:1. Introduction
2. Materials and Methods
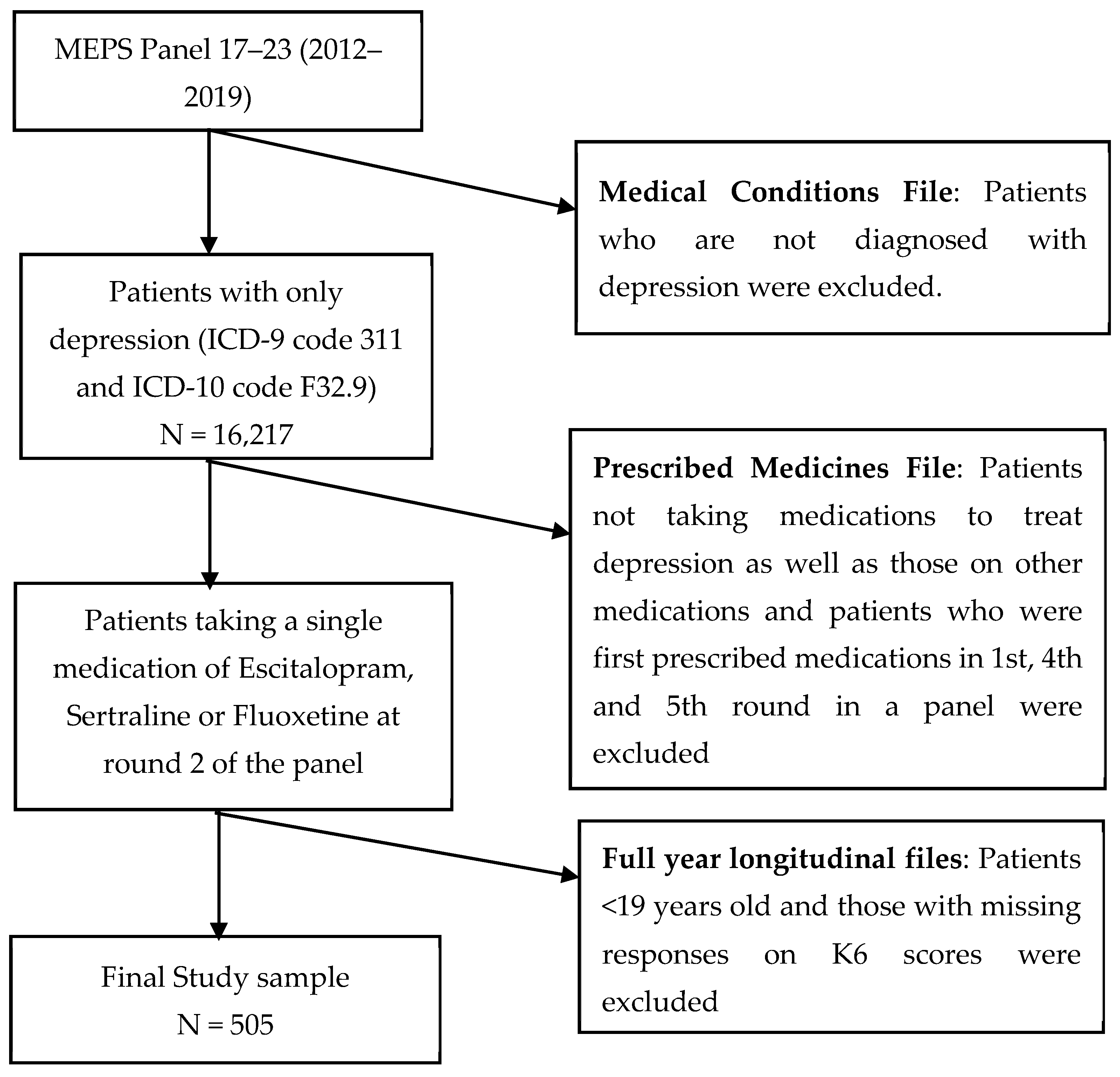
2.1. Data Source
2.2. Study Design
2.3. Outcome Measures
2.4. Statistical Analysis
3. Results
Demographic Characteristics of Study Population
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Santo, L.; Kang, K. National Hospital Ambulatory Medical Care Survey: 2019 National Summary Tables. 20 January 2023. Available online: https://stacks.cdc.gov/view/cdc/123251 (accessed on 21 February 2023).
- NIMH » Major Depression. The National Institute of Mental Health Information Resource Center. 2020. Available online: https://www.nimh.nih.gov/health/statistics/major-depression#part_2631 (accessed on 29 September 2021).
- Depression. 13 September 2021. Available online: https://www.who.int/news-room/fact-sheets/detail/depression (accessed on 28 November 2021).
- Shah, A.J. Depression and History of Attempted Suicide as Risk Factors for Heart Disease Mortality in Young Individuals. Arch. Gen. Psychiatry 2011, 68, 1135–1142. [Google Scholar] [CrossRef] [Green Version]
- Greenberg, P.E.; Fournier, A.-A.; Sisitsky, T.; Pike, C.T.; Kessler, R.C. The Economic Burden of Adults with Major Depressive Disorder in the United States (2005 and 2010). J. Clin. Psychiatry 2015, 76, 155–162. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Greenberg, P.E.; Fournier, A.-A.; Sisitsky, T.; Simes, M.; Berman, R.; Koenigsberg, S.H.; Kessler, R.C. The Economic Burden of Adults with Major Depressive Disorder in the United States (2010 and 2018). Pharmacoeconomics 2021, 39, 653–665. [Google Scholar] [CrossRef] [PubMed]
- Antidepressant Use among Persons Aged 12 and Over: United States, 2011–2014. Centers for Disease Control and Prevention. August 2017. Available online: https://www.cdc.gov/nchs/products/databriefs/db283.htm (accessed on 11 October 2021).
- Thaler, K.; Gartlehner, G.; Hansen, R.; Morgan, L.; Lux, L.; Van Noord, M.; Mager, U.; Gaynes, B.; Thieda, P.; Strobelberger, M.; et al. The comparative efficacy of second-generation antidepressants for the accompanying symptoms of depression: A systematic review. Eur. Psychiatry 2011, 26, 697. [Google Scholar] [CrossRef]
- Song, F.; Freemantle, N.; Sheldon, T.A.; House, A.; Watson, P.; Long, A.; Mason, J. Selective serotonin reuptake inhibitors: Meta-analysis of efficacy and acceptability. BMJ 1993, 306, 683–687. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Montgomery, S.A.; Henry, J.; McDonald, G.; Dinan, T.; Lader, M.; Hindmarch, I.; Clare, A.; Nutt, D. Selective serotonin reuptake inhibitors. Int. Clin. Psychopharmacol. 1994, 9, 47–54. [Google Scholar] [CrossRef]
- Ferguson, J.M. SSRI Antidepressant Medications. Prim. Care Companion J. Clin. Psychiatry 2001, 3, 22–27. [Google Scholar] [CrossRef]
- Sanchez, C.; Reines, E.H.; Montgomery, S.A. A comparative review of escitalopram, paroxetine, and sertraline. Int. Clin. Psychopharmacol. 2014, 29, 185–196. [Google Scholar] [CrossRef] [PubMed]
- Sheridan, S.D.A. Second-Generation Antidepressants for Depression in Adults. Implementing AHRQ Effective Health Care Reviews-American Family Physician. 15 November 2013. Available online: https://www.aafp.org/afp/2013/1115/p687.html#afp20131115p687-b1 (accessed on 11 October 2021).
- Edinoff, A.; Akuly, H.; Hanna, T.; Ochoa, C.; Patti, S.; Ghaffar, Y.; Kaye, A.; Viswanath, O.; Urits, I.; Boyer, A.; et al. Selective Serotonin Reuptake Inhibitors and Adverse Effects: A Narrative Review. Neurol. Int. 2021, 13, 387–401. [Google Scholar] [CrossRef]
- Bymaster, F.P.; Zhang, W.; Carter, P.A.; Shaw, J.; Chernet, E.; Phebus, L.; Wong, D.T.; Perry, K.W. Fluoxetine, but not other selective serotonin uptake inhibitors, increases norepinephrine and dopamine extracellular levels in prefrontal cortex. Psychopharmacology 2002, 160, 353–361. [Google Scholar] [CrossRef]
- Marken, P.A.; Munro, J.S. Selecting a Selective Serotonin Reuptake Inhibitor. Prim. Care Companion J. Clin. Psychiatry 2000, 2, 205–210. [Google Scholar] [CrossRef]
- Lam, R. Antidepressants and QTc prolongation. J. Psychiatry Neurosci. 2013, 38, E5–E6. [Google Scholar] [CrossRef] [Green Version]
- Hashimoto, K. Sigma-1 Receptors and Selective Serotonin Reuptake Inhibitors: Clinical Implications of their Relationship. Central Nerv. Syst. Agents Med. Chem. 2009, 9, 197–204. [Google Scholar] [CrossRef]
- Noordam, R.; Aarts, N.; Verhamme, K.M.; Sturkenboom, M.C.M.; Stricker, B.H.; Visser, L.E. Prescription and indication trends of antidepressant drugs in the Netherlands between 1996 and 2012: A dynamic population-based study. Eur. J. Clin. Pharmacol. 2015, 71, 369–375. [Google Scholar] [CrossRef] [PubMed]
- Forns, J.; Pottegård, A.; Reinders, T.; Poblador-Plou, B.; Morros, R.; Brandt, L.; Cainzos-Achirica, M.; Hellfritzsch, M.; Schink, T.; Prados-Torres, A.; et al. Antidepressant use in Denmark, Germany, Spain, and Sweden between 2009 and 2014: Incidence and comorbidities of antidepressant initiators. J. Affect. Disord. 2019, 249, 242–252. [Google Scholar] [CrossRef] [PubMed]
- Haro, J.M.; Lamy, F.-X.; Jönsson, B.; Knapp, M.; Brignone, M.; Caillou, H.; Chalem, Y.; Hammer-Helmich, L.; Rive, B.; Saragoussi, D. Characteristics of patients with depression initiating or switching antidepressant treatment: Baseline analyses of the PERFORM cohort study. BMC Psychiatry 2018, 18, 80. [Google Scholar] [CrossRef]
- Cuijpers, P.; Smits, N.; Donker, T.; Have, M.T.; de Graaf, R. Screening for mood and anxiety disorders with the five-item, the three-item, and the two-item Mental Health Inventory. Psychiatry Res. 2009, 168, 250–255. [Google Scholar] [CrossRef] [PubMed]
- Viertiö, S.; Kiviruusu, O.; Piirtola, M.; Kaprio, J.; Korhonen, T.; Marttunen, M.; Suvisaari, J. Factors contributing to psychological distress in the working population, with a special reference to gender difference. BMC Public Health 2021, 21, 611. [Google Scholar] [CrossRef]
- Mauramo, E.; Lahti, J.; Lallukka, T.; Lahelma, E.; Pietiläinen, O.; Rahkonen, O. Changes in common mental disorders and diagnosis-specific sickness absence: A register-linkage follow-up study among Finnish municipal employees. Occup. Environ. Med. 2019, 76, 230–235. [Google Scholar] [CrossRef]
- Jena, B.N.; Kalra, S.; Yeravdekar, R. Emotional and psychological needs of people with diabetes. Indian J. Endocrinol. Metab. 2018, 22, 696–704. [Google Scholar] [CrossRef]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B.W.; Löwe, B. The Patient Health Questionnaire Somatic, Anxiety, and Depressive Symptom Scales: A systematic review. Gen. Hosp. Psychiatry 2010, 32, 345–359. [Google Scholar] [CrossRef] [PubMed]
- Beck, A.T.; Steer, R.A.; Ball, R.; Ranieri, W.F. Comparison of Beck Depression Inventories-IA and-II in Psychiatric Outpatients. J. Pers. Assess. 1996, 67, 588–597. [Google Scholar] [CrossRef] [PubMed]
- Kang, Y.-K.; Guo, W.-J.; Xu, H.; Chen, Y.-H.; Li, X.-J.; Tan, Z.-P.; Li, N.; Gesang, Z.-R.; Wang, Y.-M.; Liu, C.-B.; et al. The 6-item Kessler psychological distress scale to survey serious mental illness among Chinese undergraduates: Psychometric properties and prevalence estimate. Compr. Psychiatry 2015, 63, 105–112. [Google Scholar] [CrossRef]
- Andersen, L.S.; Grimsrud, A.; Myer, L.; Williams, D.R.; Stein, D.J.; Seedat, S. The psychometric properties of the K10 and K6 scales in screening for mood and anxiety disorders in the South African Stress and Health study. Int. J. Methods Psychiatr. Res. 2011, 20, 215–223. [Google Scholar] [CrossRef] [PubMed]
- Shelton, R.C.; Tollefson, G.D.; Tohen, M.; Stahl, S.; Gannon, K.S.; Jacobs, T.G.; Buras, W.R.; Bymaster, F.P.; Zhang, W.; Spencer, K.A.; et al. A Novel Augmentation Strategy for Treating Resistant Major Depression. Am. J. Psychiatry 2001, 158, 131–134. [Google Scholar] [CrossRef]
- Rush, A.J.; Kraemer, H.C.; Sackeim, H.A.; Fava, M.; Trivedi, M.H.; Frank, E.; Ninan, P.T.; Thase, M.E.; Gelenberg, A.J.; Kupfer, D.J.; et al. Report by the ACNP Task Force on Response and Remission in Major Depressive Disorder. Neuropsychopharmacology 2006, 31, 1841–1853. [Google Scholar] [CrossRef] [Green Version]
- Fava, M.; Davidson, K.G. Definition and epidemiology of treatment-resistant depression. Psychiatr. Clin. N. Am. 1996, 19, 179–200. [Google Scholar] [CrossRef]
- Papakostas, G.I.; Shelton, R.C.; Smith, J.; Fava, M. Augmentation of Antidepressants with Atypical Antipsychotic Medications for Treatment-Resistant Major Depressive Disorder: A meta-analysis. J. Clin. Psychiatry 2007, 68, 826–831. [Google Scholar] [CrossRef]
- Methodology Report #24: Estimation Procedures for the 2007 Medical Expenditure Panel Survey Household Component. (n.d.). Available online: https://meps.ahrq.gov/data_files/publications/mr24/mr24.shtml (accessed on 28 September 2021).
- What Is Depression? (n.d.). American Psychiatry Association. Available online: https://www.psychiatry.org/patients-families/depression/what-is-depression (accessed on 1 November 2021).
- Shah, D.; Vaidya, V.; Patel, A.; Borovicka, M.; Goodman, M.-H. Assessment of health-related quality of life, mental health status and psychological distress based on the type of pharmacotherapy used among patients with depression. Qual. Life Res. 2016, 26, 969–980. [Google Scholar] [CrossRef]
- Ford, D.E.; Erlinger, T.P. Depression and C-Reactive Protein in US Adults. Arch. Intern. Med. 2004, 164, 1010–1014. [Google Scholar] [CrossRef] [Green Version]
- Salk, R.H.; Hyde, J.S.; Abramson, L.Y. Gender differences in depression in representative national samples: Meta-analyses of diagnoses and symptoms. Psychol. Bull. 2017, 143, 783–822. [Google Scholar] [CrossRef] [PubMed]
- Albert, P.R. Why is depression more prevalent in women? J. Psychiatry Neurosci. 2015, 40, 219–221. [Google Scholar] [CrossRef]
- Bartels, M.; Cacioppo, J.T.; van Beijsterveldt, T.C.E.M.; Boomsma, D.I. Exploring the Association between Well-Being and Psychopathology in Adolescents. Behav. Genet. 2013, 43, 177–190. [Google Scholar] [CrossRef] [Green Version]
- Mojtabai, R.; Olfson, M. National Trends in Long-Term Use of Antidepressant Medications. J. Clin. Psychiatry 2013, 75, 169–177. [Google Scholar] [CrossRef]
- Vahratian, A. Symptoms of Anxiety or Depressive Disorder and Use of Mental Health. 1 April 2021. Available online: https://www.cdc.gov/mmwr/volumes/70/wr/mm7013e2.htm (accessed on 29 September 2021).
- Lee, J. Mental health effects of school closures during COVID-19. Lancet Child Adolesc. Health 2020, 4, 421. [Google Scholar] [CrossRef] [PubMed]
- Loades, M.E.; Chatburn, E.; Higson-Sweeney, N.; Reynolds, S.; Shafran, R.; Brigden, A.; Linney, C.; McManus, M.N.; Borwick, C.; Crawley, E. Rapid Systematic Review: The Impact of Social Isolation and Loneliness on the Mental Health of Children and Adolescents in the Context of COVID-19. J. Am. Acad. Child Adolesc. Psychiatry 2020, 59, 1218–1239.e3. [Google Scholar] [CrossRef]
- Racine, N.; McArthur, B.A.; Cooke, J.E.; Eirich, R.; Zhu, J.; Madigan, S. Global Prevalence of Depressive and Anxiety Symptoms in Children and Adolescents During COVID-19. JAMA Pediatr. 2021, 175, 1142. [Google Scholar] [CrossRef] [PubMed]
- Cipriani, A.; Furukawa, T.A.; Salanti, G.; Chaimani, A.; Atkinson, L.Z.; Ogawa, Y.; Leucht, S.; Ruhe, H.G.; Turner, E.H.; Higgins, J.P.T.; et al. Comparative efficacy and acceptability of 21 antidepressant drugs for the acute treatment of adults with major depressive disorder: A systematic review and network meta-analysis. Lancet 2018, 391, 1357–1366. [Google Scholar] [CrossRef] [Green Version]
- Kennedy, S.H.; Andersen, H.F.; Thase, M.E. Escitalopram in the treatment of major depressive disorder: A meta-analysis. Curr. Med. Res. Opin. 2008, 25, 161–175. [Google Scholar] [CrossRef]
- Wade, A.G.; Crawford, G.M.; Yellowlees, A. Efficacy, safety and tolerability of escitalopram in doses up to 50 mg in Major Depressive Disorder (MDD): An open-label, pilot study. BMC Psychiatry 2011, 11, 42. [Google Scholar] [CrossRef] [Green Version]
- Simon, G. Unipolar Major Depression in Adults: Choosing Initial Treatment; Post, T.W., Ed.; UpToDate Inc.: Waltham, MA, USA, 2023; Available online: https://www.uptodate.com/contents/unipolar-major-depression-in-adults-choosing-initial-treatment (accessed on 21 February 2023).
- Kupka, R. Rapid Cycling Bipolar Disorder in Adults: Treatment of Major Depression; Post, T.W., Ed.; UpToDate Inc.: Waltham, MA, USA, 2023; Available online: https://www.uptodate.com/contents/rapid-cycling-bipolar-disorder-in-adults-treatment-of-major-depression#H92692341 (accessed on 21 February 2023).



{kind=link}
{kind=link}
| Characteristics | Escitalopram N (%) | Sertraline N (%) | Fluoxetine N (%) |
|---|---|---|---|
| Total | 153 (25.98) | 251 (42.61) | 185 (31.41) |
| Gender | |||
| Male | 34 (22) | 73 (29) | 67 (36) |
| Female | 119 (78) | 178 (71) | 118 (64) |
| Age | |||
| 20–39 | 48 (31.2) | 80 (31.9) | 54 (29.0) |
| 40–59 | 65 (42.5) | 99 (39.6) | 80 (43.1) |
| 60–80 | 40 (26.2) | 72 (28.5) | 51 (27.9) |
| Race | |||
| White | 129 (84.31) | 205 (81.67) | 155 (83.78) |
| Black | 11 (7.19) | 29 (11.55) | 15 (8.11) |
| American Indian | 1 (0.65) | 5 (1.99) | 3 (1.62) |
| Asian | 4 (2.61) | 4 (1.59) | 7 (3.78) |
| Multi-race | 8 (5.23) | 8 (3.19) | 5 (2.70) |
| Second-Generation Antidepressants | Improved N (%) 467 (92.48) | Unchanged N (%) 31 (6.14) | Declined N (%) 7 (1.39) |
|---|---|---|---|
| Fluoxetine | 148 (94.27) | 6 (3.82) | 3 (1.91) |
| Escitalopram | 113 (91.13) | 10 (8.06) | 1 (0.81) |
| Sertraline | 206 (91.96) | 15 (6.70) | 3 (1.34) |
| Category Ref: Unchanged | Improvement Rate | Declined Rate | ||
|---|---|---|---|---|
| OR (95% CI) | p-Value | OR (95% CI) | p-Value | |
| Drug ref: Fluoxetine | ||||
| Escitalopram | 0.2823 (0.0209–3.812) | 0.340 | 0.4269 (0.1209–1.5067) | 0.185 |
| Sertraline | 0.4500 (0.06–3.3249) | 0.433 | 1.088 (0.2885–4.1027) | 0.901 |
| Sex: Female | ||||
| Male | 0.839 (0.466–1.212) | 0.530 | 0.605 (0.081–1.129) | 0.15 |
| Age ref: 20–39 | ||||
| 40–59 | 0.9911 (0.0998–9.839) | 0.994 | 1.8426 (0.5442–6.2379) | 0.325 |
| 60–80 | 0.6620 (0.0553–7.922) | 0.744 | 0.9330 (0.2930–2.9701) | 0.906 |
| Race ref: White | ||||
| Black | 33.304 (2.671–415.19) | 0.007 | 8.7937 (1.099–70.3069) | 0.040 |
| American Indian | 6.22 (0.3324–116.39) | 0.221 | 1.50 (1.35–1.66) | 0.00 |
| Asian | 5.31 (0.2243–125.79) | 0.300 | 0.5961 (0.0688–5.1633) | 0.638 |
| Multi-race | 1.80 (0.356–9.095) | 0.476 | 4.43 (3.88–4.98) | 0.00 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Adjei, K.; Adunlin, G.; Ali, A.A. Impact of Sertraline, Fluoxetine, and Escitalopram on Psychological Distress among United States Adult Outpatients with a Major Depressive Disorder. Healthcare 2023, 11, 740. https://doi.org/10.3390/healthcare11050740
Adjei K, Adunlin G, Ali AA. Impact of Sertraline, Fluoxetine, and Escitalopram on Psychological Distress among United States Adult Outpatients with a Major Depressive Disorder. Healthcare. 2023; 11(5):740. https://doi.org/10.3390/healthcare11050740
Chicago/Turabian StyleAdjei, Kwame, Georges Adunlin, and Askal Ayalew Ali. 2023. "Impact of Sertraline, Fluoxetine, and Escitalopram on Psychological Distress among United States Adult Outpatients with a Major Depressive Disorder" Healthcare 11, no. 5: 740. https://doi.org/10.3390/healthcare11050740
APA StyleAdjei, K., Adunlin, G., & Ali, A. A. (2023). Impact of Sertraline, Fluoxetine, and Escitalopram on Psychological Distress among United States Adult Outpatients with a Major Depressive Disorder. Healthcare, 11(5), 740. https://doi.org/10.3390/healthcare11050740