

Ethnic Minorities’ Experiences of Cardiac Rehabilitation: A Scoping Review
 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Inclusion and Exclusion Criteria
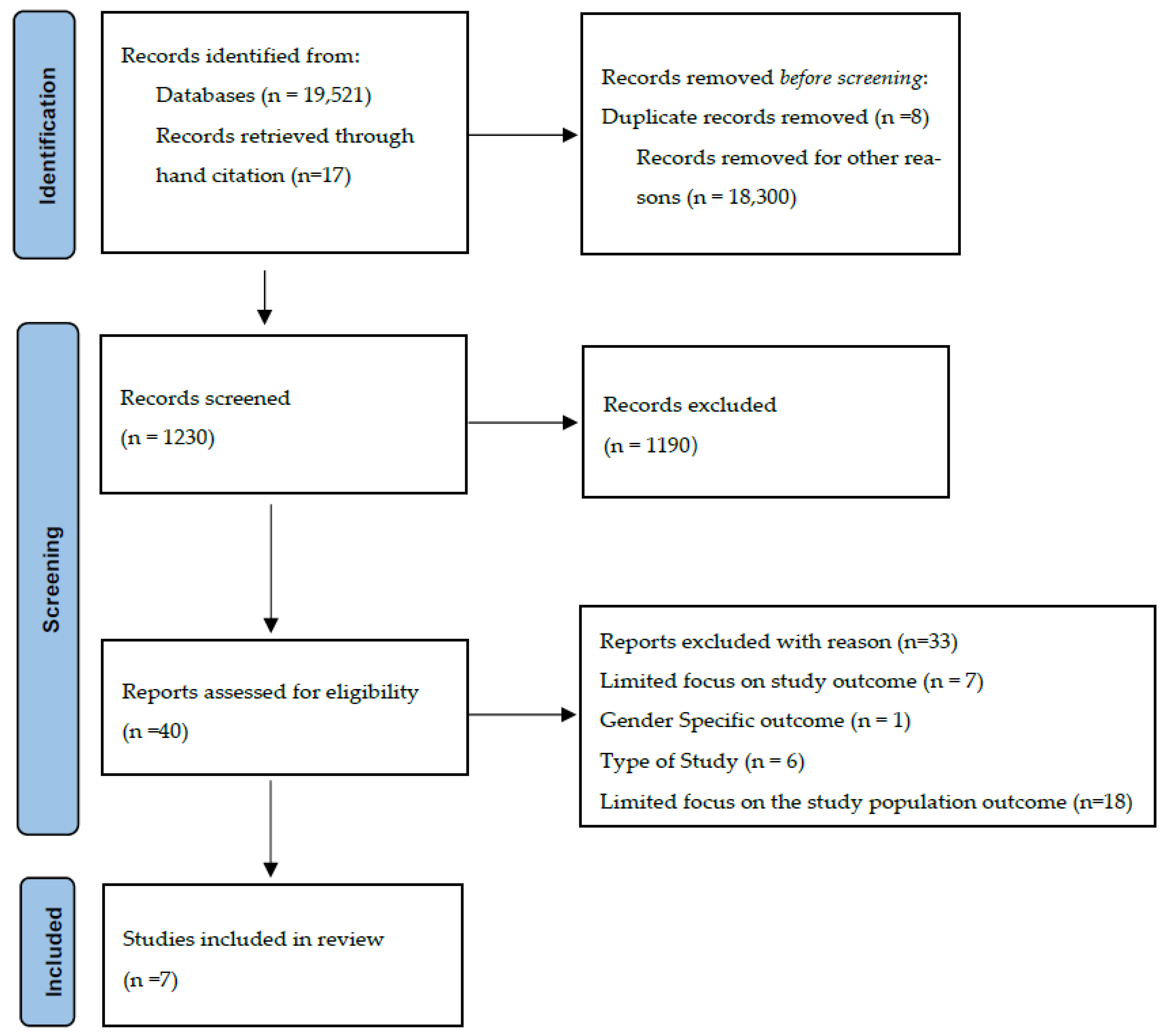
2.3. Screening and Study Selection
2.4. Quality Appraisal
2.5. Data Extraction
3. Results
3.1. Studies Characteristics
3.2. Comparison Studies Examining Experiences of White and Ethnic-Minority Patients
3.3. Factors Encouraging Patients to Attend Rehabilitation Sessions or Engage in Rehabilitation Activities
3.4. Factors Discouraging Patients to Attend Rehabilitation Sessions or Engage in Rehabilitation Activities
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
| CINAHL Complete and CINAHL Ultimate Retrievals-801 | (MM “Rehabilitation, Cardiac”) or (“cardiovascular disease”)) AND ((experiences or perceptions or attitudes or views or qualitative or interviews or views)) AND (((MM “Ethnic Groups”) ‘ethnic minorit*” or “racial minorit*” or “ethnic groups” or “underrepresented groups”* or *“black American*’’ or *“African patients*’’or “American Indian*’’ or “Alaska Native*’’ “Asian*’’ or ‘’Hispanic or Latino’’ or “Native Hawaiian*’’ or “White’’ “Mideastern’’ or ‘’North Africa*’’)) |
| APA PsycInfo– Retrievals-86 | ( (MM “Cardiac Rehabilitation ”) or (“cardiovascular disease”)) AND ((experiences or perceptions or attitudes or views or qualitative or interviews or views)) AND (((MM “Ethnic Groups”) ‘ethnic minorit*” or “racial minorit*” or “ethnic groups” or “underrepresented groups”* or *“black American*’’ or *“African patients*’’or “American Indian*” or “Alaska Native*” “Asian*’’ or “Hispanic or Latino’’ or “Native Hawaiian*” or “White’’ “Mideastern’’ or “North Africa*”) ) |
| Medline- Retrievals Retrievals-134 | ((MM “Cardiac Rehabilitation ”) or (“cardiovascular disease”)) AND ((experiences or perceptions or attitudes or views or qualitative or interviews or views)) AND (((MM “Ethnic Groups”) ‘ethnic minorit*” or “racial minorit*” or “ethnic groups” or “underrepresented groups”* or *“black American*’’ or *“African patients*”or“American Indian*” or “Alaska Native*” “Asian*” or “Hispanic or Latino” or “Native Hawaiian*” or “White” “Mideastern’’ or “North Africa*”) |
| Google scholar Retrievals- 18,500 (Supplementary Search, only searching the first 200 articles only) | ethnic minority or ethnic and cardiovascular rehabilitation’ and qualitative experiences or perceptions or attitudes or views or feelings or perspectives |
References
- World Health Organization. Cardiovascular Diseases; World Health Organization: Geneva, Switzerland, 2023.
- American Association of Cardiovascular and Pulmonary Rehabilitation. Guidelines for Cardiac Rehabilitation and Secondary Prevention Programs, 5th ed.; Human Kinetics: Champaign, IL, USA, 2013; p. 336. [Google Scholar]
- The National Institute for Health and Care Excellence. Cardiovascular Disease: Risk Assessment and Reduction, Including Lipid Modification; National Institute for Health and Care Excellence: Sutton-in-Ashfield, UK, 2016. [Google Scholar]
- Centre of Health Protection Department of Health the Government of the Hong Kong Special Administrative, R. Heart Diseases. 2022. Available online: https://www.chp.gov.hk/en/healthtopics/content/25/57.html (accessed on 8 December 2022).
- Canada, G.O. Prevention of Heart Disease and Conditions. Prevention of Heart Disease and Conditions. 2017. Available online: https://www.canada.ca/en/public-health/services/diseases/heart-health/heart-diseases-conditions/prevention-heart-diseases-conditions.html (accessed on 8 December 2022).
- Thomas, R.J.; Balady, G.; Banka, G.; Beckie, T.M.; Chiu, J.; Gokak, S.; Ho, P.M.; Keteyian, S.J.; King, M.; Lui, K.; et al. 2018 ACC/AHA Clinical Performance and Quality Measures for Cardiac Rehabilitation: A Report of the American College of Cardiology/American Heart Association Task Force on Performance Measures. J. Am. Coll. Cardiol. 2018, 71, 1814–1837. [Google Scholar] [CrossRef] [PubMed]
- Hedbäck, B.; Perk, J.; Hörnblad, M.; Ohlsson, U. Cardiac rehabilitation after coronary artery bypass surgery: 10-year results on mortality, morbidity and readmissions to hospital. J. Cardiovasc. Risk 2001, 8, 153–158. [Google Scholar] [CrossRef]
- Doherty, P.; Harrison, A.; Petre, C.; Onion, N.; Hemingway, J.; Tang, L. The National Audit of Cardiac Rehabilitation (NACR) Annual Statistical Report; British Heart Foundation: London, UK, 2021. [Google Scholar]
- England, N.H.S. Increase Uptake of Cardiac Rehabilitation for People with Coronary Artery Disease and Following Acute Heart Failure. 2014. Available online: https://www.england.nhs.uk/wp-content/uploads/2014/02/pm-fs-3-10.pdf (accessed on 8 January 2023).
- Oldridge, N.B.; Pakosh, T.M.; Thomas, J.R. Cardiac Rehabilitation in Low- and Middle-Income Countries: A Review on Cost and Cost-Effectiveness. Int. Health 2016, 8, 77–82. [Google Scholar] [CrossRef] [Green Version]
- Shields, G.E.; Wells, A.; Doherty, P.; Heagerty, A.; Buck, D.; Davies, M.L. Cost-Effectiveness of Cardiac Rehabilitation: A Systematic Review. Br. Med. J. 2018, 104, 1403–1410. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Service, N.H. Coronary Heart Disease-Recovery. NHS.UK. 2020. Available online: https://www.nhs.uk/conditions/coronary-heart-disease/recovery/ (accessed on 8 January 2023).
- Chow, C.K.; Jolly, S.; Rao-Melacini, P.; Fox, A.A.K.; Anand, S.S.; Yusuf, S. Association of Diet, Exercise and Smoking Modification with Risk of Early Cardiovascular Events after Acute Coronary Syndromes. Circulation 2010, 121, 750–758. [Google Scholar] [CrossRef] [Green Version]
- Garfein, J.; Guhl, E.N.; Swabe, G.; Sekikawa, A.; Barinas-Mitchell, E.; Forman, D.E.; Magnani, J.W. Racial and Ethnic Differences in Cardiac Rehabilitation Participation: Effect Modification by Household Income. J. Am. Heart Assoc. 2022, 11, e025591. [Google Scholar] [CrossRef]
- Sumner, J.; Grace, S.L.; Doherty, P. Predictors of Cardiac Rehabilitation Utilization in England: Results from the National Audit. J. Am. Heart Assoc. 2016, 5, e003903. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prince, D.Z.; Sobolev, M.; Gao, J.; Taub, C.C. Racial disparities in cardiac rehabilitation initiation and the effect on survival. PMR 2014, 6, 486–492. [Google Scholar] [CrossRef]
- Peterson, E.; Yancy, C.W. Eliminating Racial and Ethnic Disparities in Cardiac Care. N. Engl. J. Med. 2009, 360, 1172–1174. [Google Scholar] [CrossRef]
- Ritchey, M.D.; Maresh, S.; McNeely, J.; Shaffer, T.; Jackson, S.L.; Keteyian, S.J.; Brawner, C.A.; Whooley, M.A.; Chang, T.; Stolp, H.; et al. Tracking Cardiac Rehabilitation Participation and Completion Among Medicare Beneficiaries to Inform the Efforts of a National Initiative. Circ. Cardiovasc. Qual. Outcomes 2020, 13, e005902. [Google Scholar] [CrossRef]
- Suaya, J.A.; Shepard, D.S.; Normand, S.-L.T.; Ades, P.A.; Prottas, J.; Stason, W.B. Use of Cardiac Rehabilitation by Medicare Beneficiaries After Myocardial Infarction or Coronary Bypass Surgery. Circulation 2007, 116, 1653–1662. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tian, Y.; Deng, P.; Bing, L.; Wang, J.; Li, J.; Huang, J.; Zheng, Y. Treatment Models of Cardiac Rehabilitation in patients with Coronary Heart Disease and Related Factors Affecting patient Compliance. Rev. Cardiovasc. Med. 2019, 20, 27–33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Office of Management Budget. Revisions to the Standards for the Classification of Federal Data on Race and Ethnicity; The White House: Washington, DC, USA, 1997.
- Boland, A.; Cherry, G.; Dickson, R. Doing a Systematic Review: A Student’s Guide; Sage: London, UK, 2013. [Google Scholar]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, T.P. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haddaway, N.R.; Collins, A.M.; Coughlin, D.; Kirk, S. The Role of Google Scholar in Evidence Reviews and Its Applicability to Grey Literature Searching. PLoS ONE 2015, 10, e0138237. [Google Scholar] [CrossRef] [Green Version]
- Kotera, Y.; Lyons, M.; Vione, K.C.; Norton, B. Effect of Nature Walks on Depression and Anxiety: A Systematic Review. Sustainability 2021, 13, 4015. [Google Scholar] [CrossRef]
- Grace, L.S.; Chessex, C.; Arthur, H.; Chan, S.; Cyr, C.; Dafoe, W.; Juneau, M.; Oh, P.; Suskin, N. Systematizing Inpatient Referral to Cardiac Rehabilitation 2010. J. Cardiopulm. Rehabil. Prev. 2011, 31, E1–E8. [Google Scholar] [CrossRef]
- Polanin, J.R.; Pigott, T.D.; Espelage, D.L.; Grotpeter, J.K. Best practice guidelines for abstract screening large-evidence systematic reviews and meta-analyses. Res. Synth. Methods 2019, 10, 330–342. [Google Scholar] [CrossRef] [Green Version]
- Critical Appraisal Skills Programme. CASP Checklists-Critical Appraisal Skills Programme; CASP-Critical Appraisal Skills Programme: Oxford, UK, 2018. [Google Scholar]
- Dalton, J.; Booth, A.; Noyes, J.; Sowden, A.J. Potential value of systematic reviews of qualitative evidence in informing user-centered health and social care: Findings from a descriptive overview. J. Clin. Epidemiol. 2017, 88, 37–46. [Google Scholar] [CrossRef] [PubMed]
- Astin, F.; Atkin, K.; Darr, A. Family support and cardiac rehabilitation: A comparative study of the experiences of South Asian and White-European patients and their carer’s living in the United Kingdom. Eur. J. Cardiovasc. Nurs. 2008, 7, 43–51. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bhattacharyya, M.; Stevenson, F.; Walters, K. Exploration of the psychological impact and adaptation to cardiac events in South Asians in the UK: A qualitative study. BMJ Open 2016, 6, e010195. [Google Scholar] [CrossRef] [Green Version]
- Banerjee, A.T.; Grace, S.L.; Thomas, S.G.; Faulkner, G. Cultural factors facilitating cardiac rehabilitation participation among Canadian South Asians: A qualitative study. Heart Lung 2010, 39, 494–503. [Google Scholar] [CrossRef]
- Dilla, D.; Ian, J.; Martin, J.; Michelle, H.; Felicity, A. “I don’t do it for myself, I do it for them”: A grounded theory study of South Asians’ experiences of making lifestyle change after myocardial infarction. J. Clin. Nurs. 2020, 29, 3687–3700. [Google Scholar] [CrossRef]
- Galdas, P.M.; Kang, H.B.K. Punjabi Sikh patients’ cardiac rehabilitation experiences following myocardial infarction: A qualitative analysis. J. Clin. Nurs. 2010, 19, 3134–3142. [Google Scholar] [CrossRef] [PubMed]
- Koehler, A.; Hoggson, J.; Rappleyea, D.; Knight, S.; Dodor, B. African American patients’ lived experience through cardiac event/surgery and recovery. Wake For. J. Sci. Med. 2020, 5, 32–43. [Google Scholar]
- Wong, E.M.L.; Zhong, X.B.; Sit, J.W.H.; Chair, S.Y.; Leung, D.Y.P.; Leung, C.; Leung, K.C. Attitude toward the out-patient cardiac rehabilitation program and facilitators for maintenance of exercise behavior. Psychol. Health Med. 2016, 21, 724–734. [Google Scholar] [CrossRef]
- Lloyd, C.E.M.; Reid, G.; Kotera, Y. From Whence Cometh My Help? Psychological Distress and Help-Seeking in the Evangelical Christian Church. Front. Psychol. 2021, 12, 744432. [Google Scholar] [CrossRef]
- Ades, P.A.; Khadanga, S.; Savage, P.D.; Gaalema, D.E. Enhancing participation in cardiac rehabilitation: Focus on underserved populations. Prog. Cardiovasc. Dis. 2022, 70, 102–110. [Google Scholar] [CrossRef]
- Jolly, K.; Greenfield, S.M.; Hare, R. Attendance of Ethnic Minority Patients in Cardiac Rehabilitation. J. Cardiopulm. Rehabil. Prev. 2004, 24, 308–312. [Google Scholar] [CrossRef] [PubMed]
- Valencia, H.E.; Savage, P.D.; Ades, P.A. Cardiac Rehabilitation Participation in Underserved Populations. J. Cardiopulm. Rehabil. Prev. 2011, 31, 203–210. [Google Scholar] [CrossRef] [PubMed]
- Vanzella, L.M.; Oh, P.; Pakosh, M.; Ghisi, G.L.M. Barriers to Cardiac Rehabilitation in Ethnic Minority Groups: A Scoping Review. J. Immigr. Minor. Health 2021, 23, 824–839. [Google Scholar] [CrossRef] [PubMed]
- Kotera, Y.; Conway, E.; Green, P. Construction And factorial validation of a short version of the Academic Motivation Scale. Br. J. Guid. Couns. 2021, 1–10. [Google Scholar] [CrossRef]
- Kotera, Y.; Taylor, E.; Wilkes, J.; Veasey, C.; Maybury, S.; Jackson, J.; Lieu, J.; Asano, K. Construction and factorial validation of a short version of the Attitudes Towards Mental Health Problems Scale (SATMHPS). Ment. Health Relig. Cult. 2022. [CrossRef]
- Yohannes, A.M.; Doherty, P.; Bundy, C.; Yalfani, A. The long-term benefits of cardiac rehabilitation on depression, anxiety, physical activity and quality of life. J. Clin. Nurs. 2010, 19, 2806–2813. [Google Scholar] [CrossRef] [PubMed]
- Kotera, Y.; Ozaki, A.; Miyatake, H.; Tsunetoshi, C.; Nishikawa, Y.; Kosaka, M.; Tanimoto, T. Qualitative Investigation into the Mental Health of Healthcare Workers in Japan during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2022, 19, 568. [Google Scholar] [CrossRef] [PubMed]
- Rathore, S.; Kumar, B.; Tehrani, S.; Khanra, D.; Duggal, B.; Chandra Pant, D. Cardiac rehabilitation: Appraisal of current evidence and utility of technology aided home-based cardiac rehabilitation. Indian Heart J. 2020, 72, 491–499. [Google Scholar] [CrossRef]
- Kotera, Y.; Rennick-Egglestone, S.; Ng, F.; Llewellyn-Beardsley, J.; Ali, Y.; Newby, C.; Yeo, C.; Slade, E.; Bradstreet, S.; Harrison, J.; et al. Assessing diversity and inclusivity is the next frontier in mental health recovery narrative research and practice. JMIR Ment. Health 2023, preprint. [Google Scholar] [CrossRef]
- Kotera, Y.; Cockerill, V.; Green, P.; Hutchinson, L.; Shaw, P.; Bowskill, N. Towards another kind of borderlessness: Online students with disabilities. Distance Educ. 2019, 40, 170–186. [Google Scholar] [CrossRef]
- Pines, R.L.; Jones, L.; Sheeran, N. Using Family Members as Medical Interpreters: An Explanation of Healthcare Practitioners’ Normative Practices in Pediatric and Neonatal Departments in Australia. Health Commun. 2020, 35, 902–909. [Google Scholar] [CrossRef]
- White, J.; Plompen, T.; Tao, L.; Micallef, E.; Haines, T. What is needed in culturally competent healthcare systems? A qualitative exploration of culturally diverse patients and professional interpreters in an Australian healthcare setting. BMC Public Health 2019, 19, 1096. [Google Scholar] [CrossRef]
- Coulter, A.; Ellins, J. Effectiveness of strategies for informing, educating, and involving patients. BMJ 2007, 335, 24–27. [Google Scholar] [CrossRef] [Green Version]
- Subhan, F.B.; Chan, C.B. Diet quality and risk factors for cardiovascular disease among South Asians in Alberta. Appl. Physiol. Nutr. Metab. 2019, 44, 886–893. [Google Scholar] [CrossRef] [Green Version]
- Gadgil, M.D.; Anderson, C.A.M.; Kandula, N.R.; Kanaya, A.M. Dietary Patterns Are Associated with Metabolic Risk Factors in South Asians Living in the United States. J. Nutr. 2015, 145, 1211–1217. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kotera, Y.; Kaluzeviciute, G.; Bennett-Viliardos, L. Qualitative Investigation into Pre- and Post-Natal Experience of Parents of Triplets. J. Child Fam. Stud. 2022, 31, 1785–1797. [Google Scholar] [CrossRef] [PubMed]
- Uneno, Y.; Kotera, Y.; Fujisawa, D.; Kataoka, Y.; Kosugi, K.; Murata, N.; Kessoku, T.; Ozaki, A.; Miyatake, H.; Muto, M. Development of a novel COMPAssion focused online psyChoTherapy for bereaved informal caregivers: The COMPACT feasibility trial protocol. BMJ Open 2022, 12, e067187. [Google Scholar] [CrossRef] [PubMed]
- McIntosh, N.; Fix, G.M.; Allsup, K.; Charns, M.; McDannold, S.; Manning, K.; Forman, D.E. A Qualitative Study of Participation in Cardiac Rehabilitation Programs in an Integrated Health Care System. Mil. Med. 2017, 182, e1757–e1763. [Google Scholar] [CrossRef] [Green Version]
- Kotera, Y. A qualitative investigation into the experience of neuro-linguistic programming certification training among Japanese career consultants. Br. J. Guid. Couns. 2018, 46, 39–50. [Google Scholar] [CrossRef]
- Gaalema, D.E.; Elliott, R.J.; Savage, P.D.; Rengo, J.L.; Cutler, A.Y.; Pericot-Valverde, I.; Priest, J.S.; Shepard, D.S.; Higgins, S.T.; Ades, P.A. Financial Incentives to Increase Cardiac Rehabilitation Participation Among Low-Socioeconomic Status Patients: A Randomized Clinical Trial. JACC Heart Fail. 2019, 7, 537–546. [Google Scholar] [CrossRef]
- Mathews, L.; Akhiwu, O.; Mukherjee, M.; Blumenthal, R.S.; Matsushita, K.; Ndumele, C.E. Disparities in the Use of Cardiac Rehabilitation in African Americans. Curr. Cardiovasc. Risk Rep. 2022, 16, 31–41. [Google Scholar] [CrossRef]
- Nadarajah, S.; Berger, A.M.; Thomas, S.A. Current Status of Spirituality in Cardiac Rehabilitation Programs: A Review of Literature. J. Cardiopulm. Rehabil. Prev. 2013, 33, 135–143. [Google Scholar] [CrossRef]
- Li, S.; Fonarow, G.C.; Mukamal, K.; Xu, H.; Matsouaka, R.A.; Devore, A.D.; Bhatt, D.L. Sex and Racial Disparities in Cardiac Rehabilitation Referral at Hospital Discharge and Gaps in Long-Term Mortality. J. Am. Heart Assoc. 2018, 7, e008088. [Google Scholar] [CrossRef]
- Scheppers, E.; van Dongen, E.; Dekker, J.; Geertzen, J.; Dekker, J. Potential barriers to the use of health services among ethnic minorities: A review. Fam. Pract. 2006, 23, 325–348. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grace, S.L.; Chessex, C.; Arthur, H.; Chan, S.; Cyr, C.; Dafoe, W.; Juneau, M.; Oh, P.; Suskin, N. Systematizing inpatient referral to cardiac rehabilitation 2010: Canadian Association of Cardiac Rehabilitation and Canadian Cardiovascular Society joint position paper endorsed by the Cardiac Care Network of Ontario. Can. J. Cardiol. 2011, 27, 192–199. [Google Scholar] [CrossRef] [PubMed]
- Thomas, R.J.; Beatty, A.L.; Beckie, T.M.; Brewer, L.C.; Brown, T.M.; Forman, D.E.; Franklin, B.A.; Keteyian, S.J.; Kitzman, D.W.; Regensteiner, J.G.; et al. Home-Based Cardiac Rehabilitation: A Scientific Statement From the American Association of Cardiovascular and Pulmonary Rehabilitation, the American Heart Association, and the American College of Cardiology. J. Am. Coll. Cardiol. 2019, 74, 133–153. [Google Scholar] [CrossRef] [PubMed]

| Population | Male and female ethnic minority patients: individuals of American Indian, Asian, Black or African American, Hispanic, and White descent having origins in any of the original peoples of Europe, the Middle East, or North Africa, as defined by the Office of Management and Budget to the Standards of the Classification of Federal Data on Race and Ethnicity (1997) aged 18 > who attended any cardiac rehabilitation interventions at any time and experienced any clinical cardiovascular trauma/disease in their lifetime. |
| Intervention | All cardiac rehabilitation programs, i.e., behaviour and lifestyle modification, health education and psychological, therapy, or physical exercise given for the care and recovery of any cardiac event that requires cardiac rehabilitation. |
| Comparison | NA |
| Outcome | Qualitative views or perceptions of attending cardiac rehabilitation; positive or negative personal or group experiences of attending CR services. |
| Author and Year | Country | Study Design | Sample Size | Sample Participants Ethnicity | Male: Female Participants | Relevant Themes | Quality Assessment |
|---|---|---|---|---|---|---|---|
| Astin, et al. (2008) [30] | UK | Qualitative | 65 | South Asian & White-European | 36:29 | Provision of advice and information, exercise, and Dietary change, | 7/10 |
| Banerjee 2010 et al. (2010) [32] | Canada | Qualitative | 16 | South Asian | 13:3 | Predisposing factors -Patients felt safe when performing exercise in sessions Pts had positive views of CR from relatives Positive education of physical activity & nutritional info Enabling Factors- Accessible Transport, Flexibility of CR Sessions Physician Referral Reinforcing Factors- Family support, physician support and FU, caring and support staff, experiencing positive outcomes. | 7/10 |
| Bhattacharyya, et al. (2016) [31] | UK | Qualitative | 28 | White British, Indians and Bangladeshis | 23:5 | Low mood, anxiety and fear, perception of self and how others perceive them, Physical Impact, attitudes towards the future, Cardiac rehabilitation, Social and professional support, lifestyle changes and return to work | 7/10 |
| Dilla et al. (2020) [33] | UK | Qualitative | 14 | South Asian | 9:5 | Dietary Information Exercise Religious Faith | 8/10 |
| Galdas et al. (2010) [34] | Canada | Qualitative | 15 | South Asian | 10:5 | Dietary advice Religious Faith ongoing interaction with peers- offered psychological support | 8/10 |
| Koehler et al. (2020) [35] | United States | Qualitative | 7 | African American | 4:3 | Religious Faith Physician Referral Participants experienced inconsistent referral to and utilization of Cardiac Rehabilitation Barriers to CR was discussed | 7/10 |
| Wong et al. (2016) [36] | Hong Kong | Qualitative | 22 | Chinese | 15:7 | Participants attitude toward OCRP, which included informant perception, affection, and practice Exercise Behaviour – intention and maintenance | 7/10 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Carew Tofani, A.; Taylor, E.; Pritchard, I.; Jackson, J.; Xu, A.; Kotera, Y. Ethnic Minorities’ Experiences of Cardiac Rehabilitation: A Scoping Review. Healthcare 2023, 11, 757. https://doi.org/10.3390/healthcare11050757
Carew Tofani A, Taylor E, Pritchard I, Jackson J, Xu A, Kotera Y. Ethnic Minorities’ Experiences of Cardiac Rehabilitation: A Scoping Review. Healthcare. 2023; 11(5):757. https://doi.org/10.3390/healthcare11050757
Chicago/Turabian StyleCarew Tofani, Aiesha, Elaina Taylor, Ingrid Pritchard, Jessica Jackson, Alison Xu, and Yasuhiro Kotera. 2023. "Ethnic Minorities’ Experiences of Cardiac Rehabilitation: A Scoping Review" Healthcare 11, no. 5: 757. https://doi.org/10.3390/healthcare11050757