


A Fifteen-Year Survey for Orthopedic Malpractice Claims in the Criminal Court of Rome
 ,
, {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
3. Results
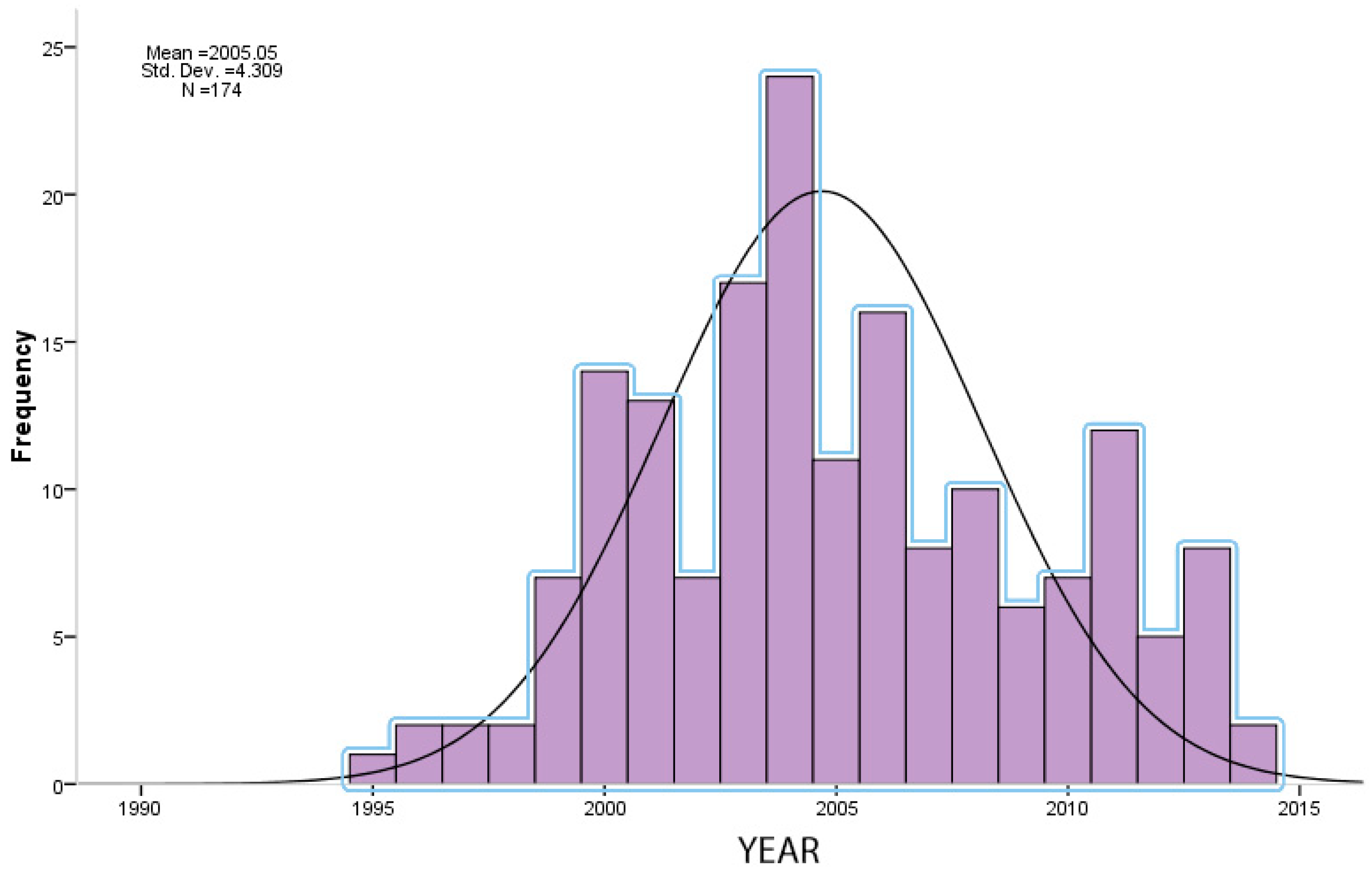
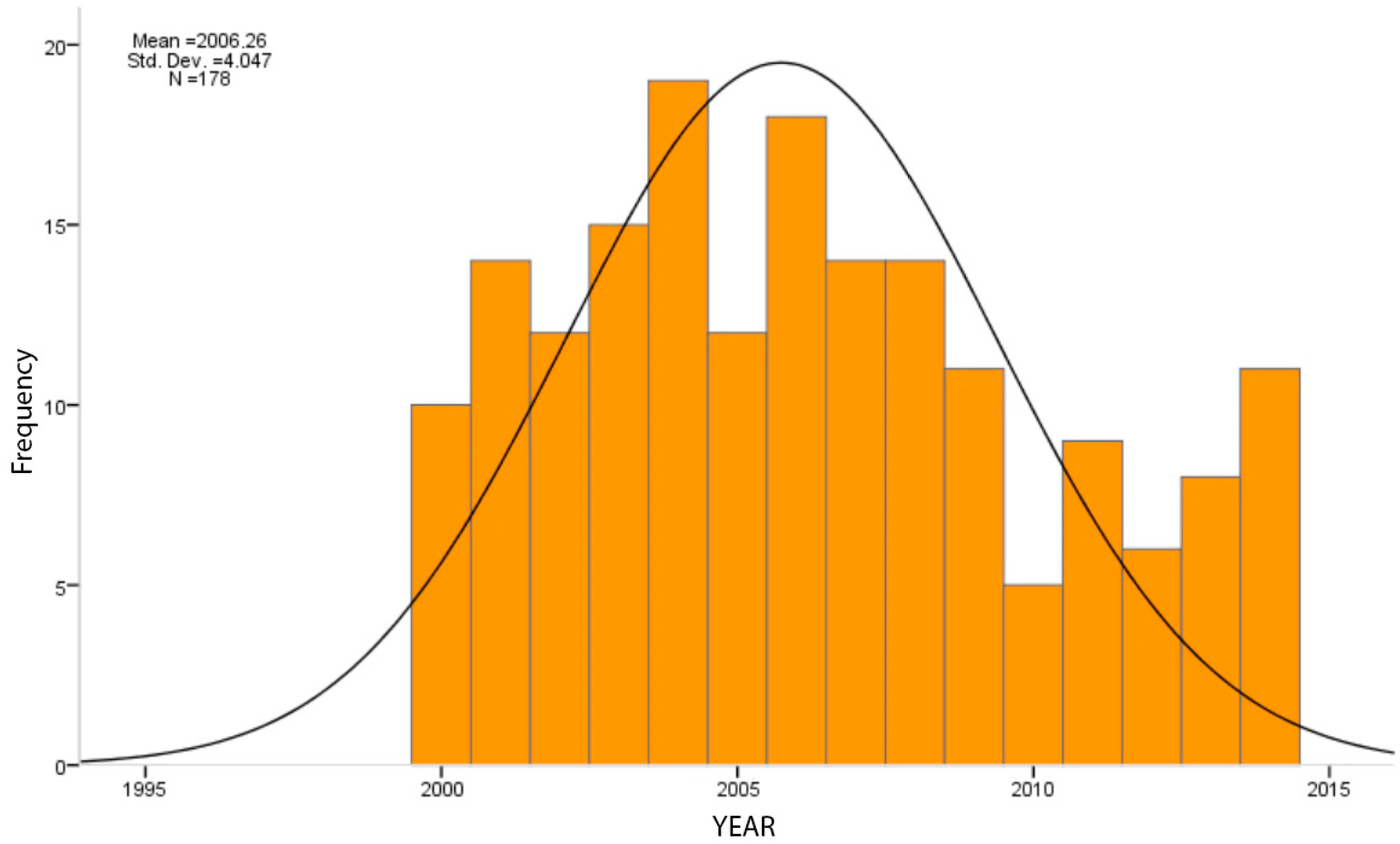
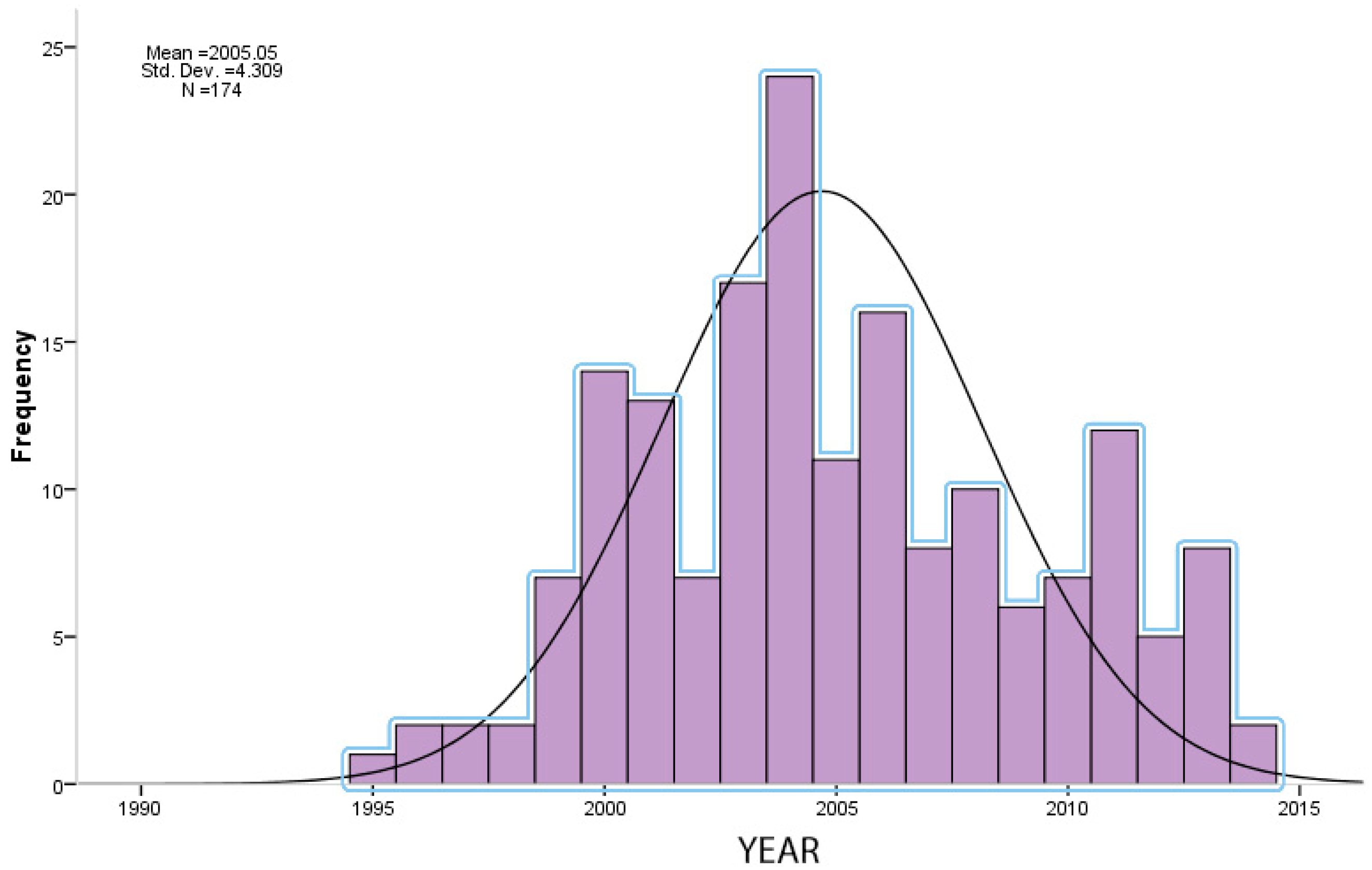
3.1. Trend in Years
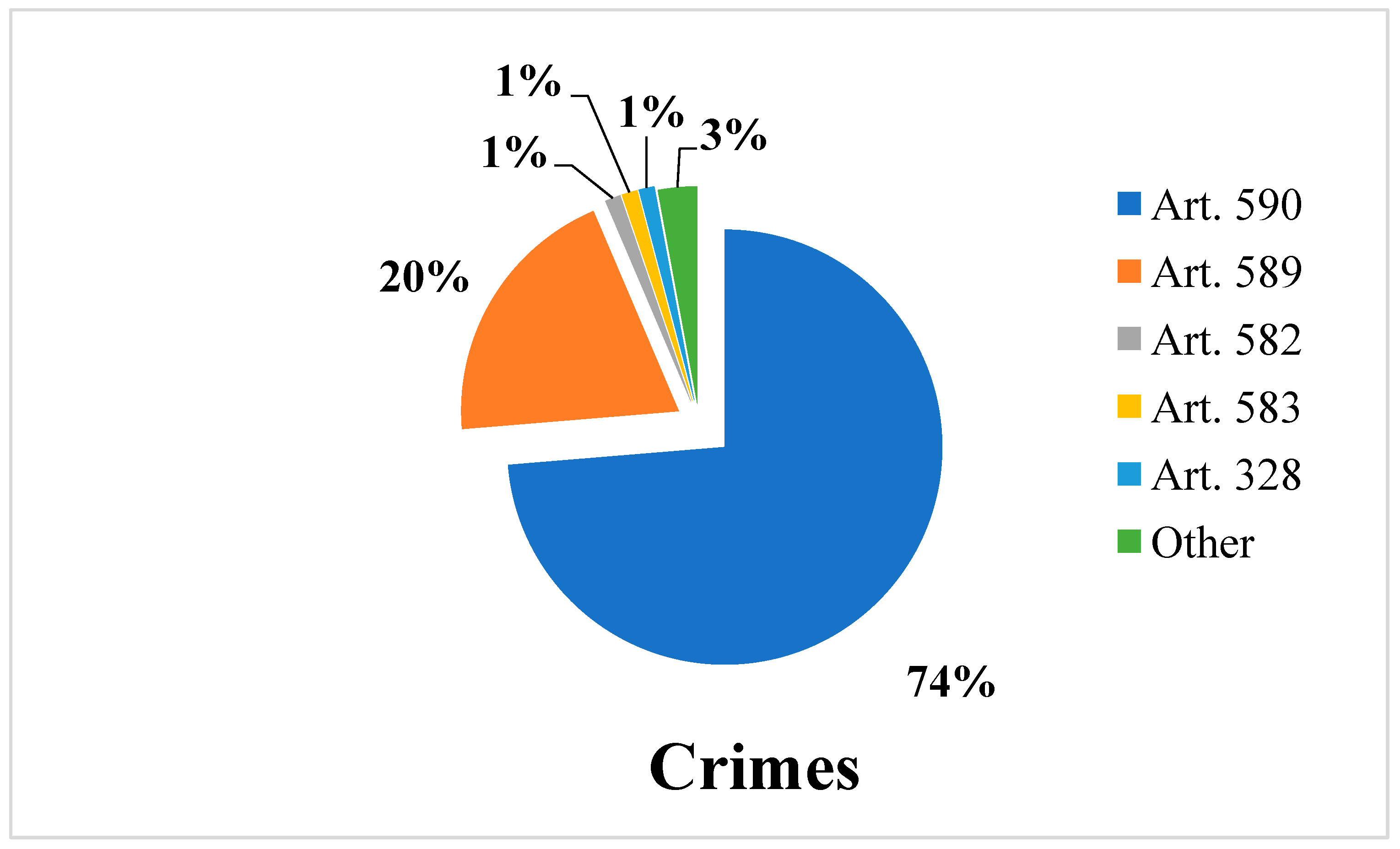
3.2. Types of Crimes
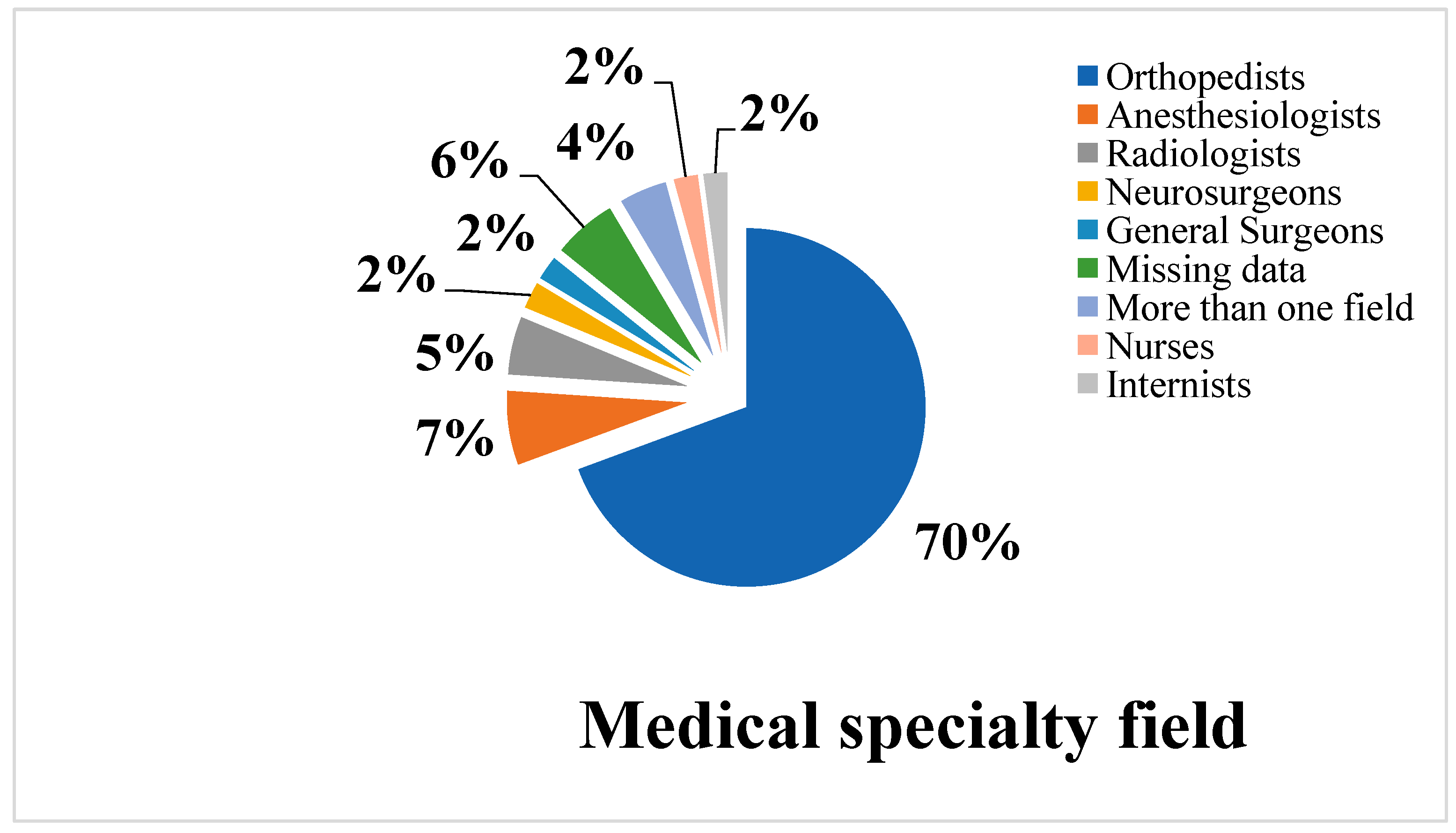
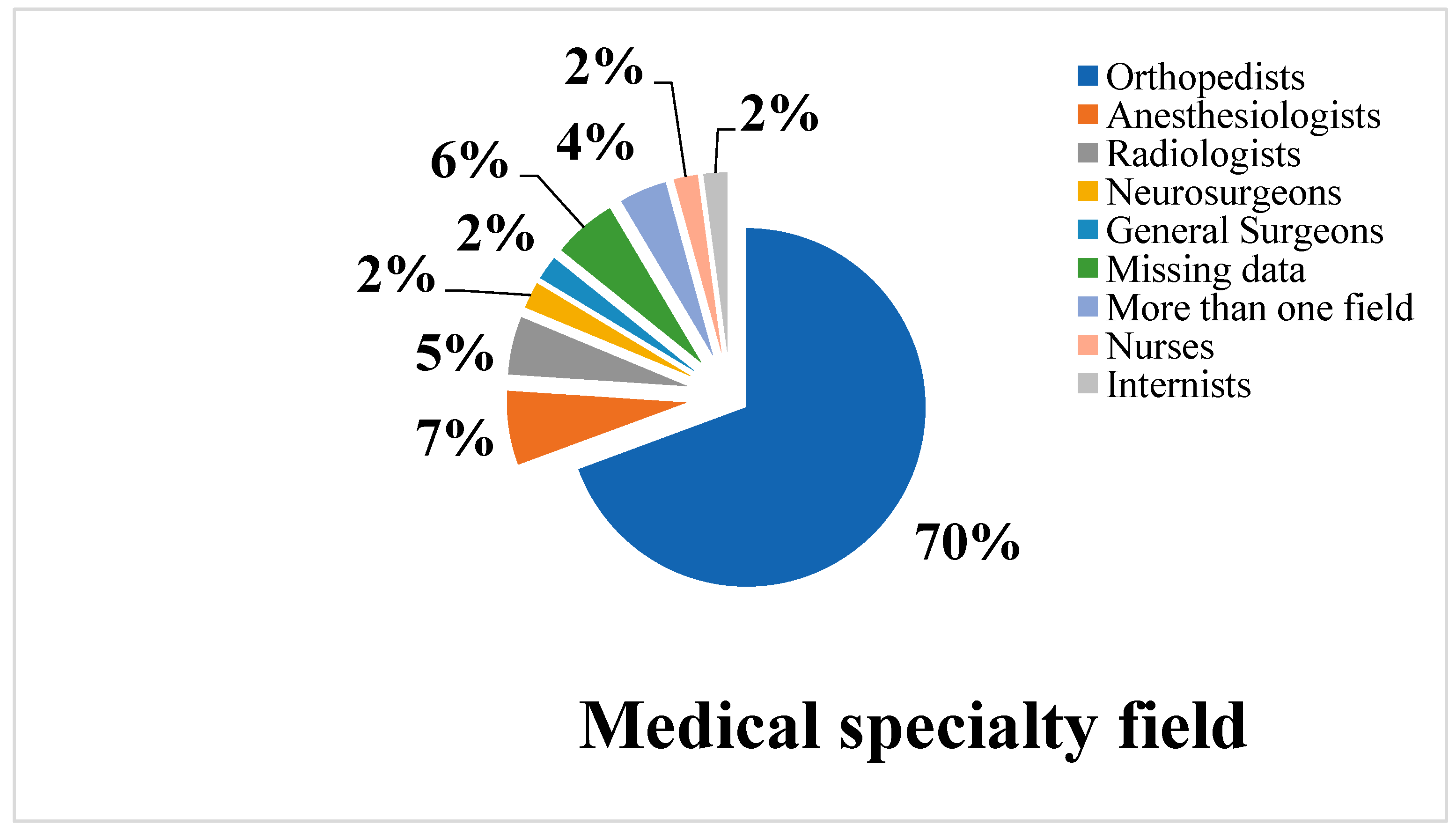
3.3. Involved Medical Specialty Fields
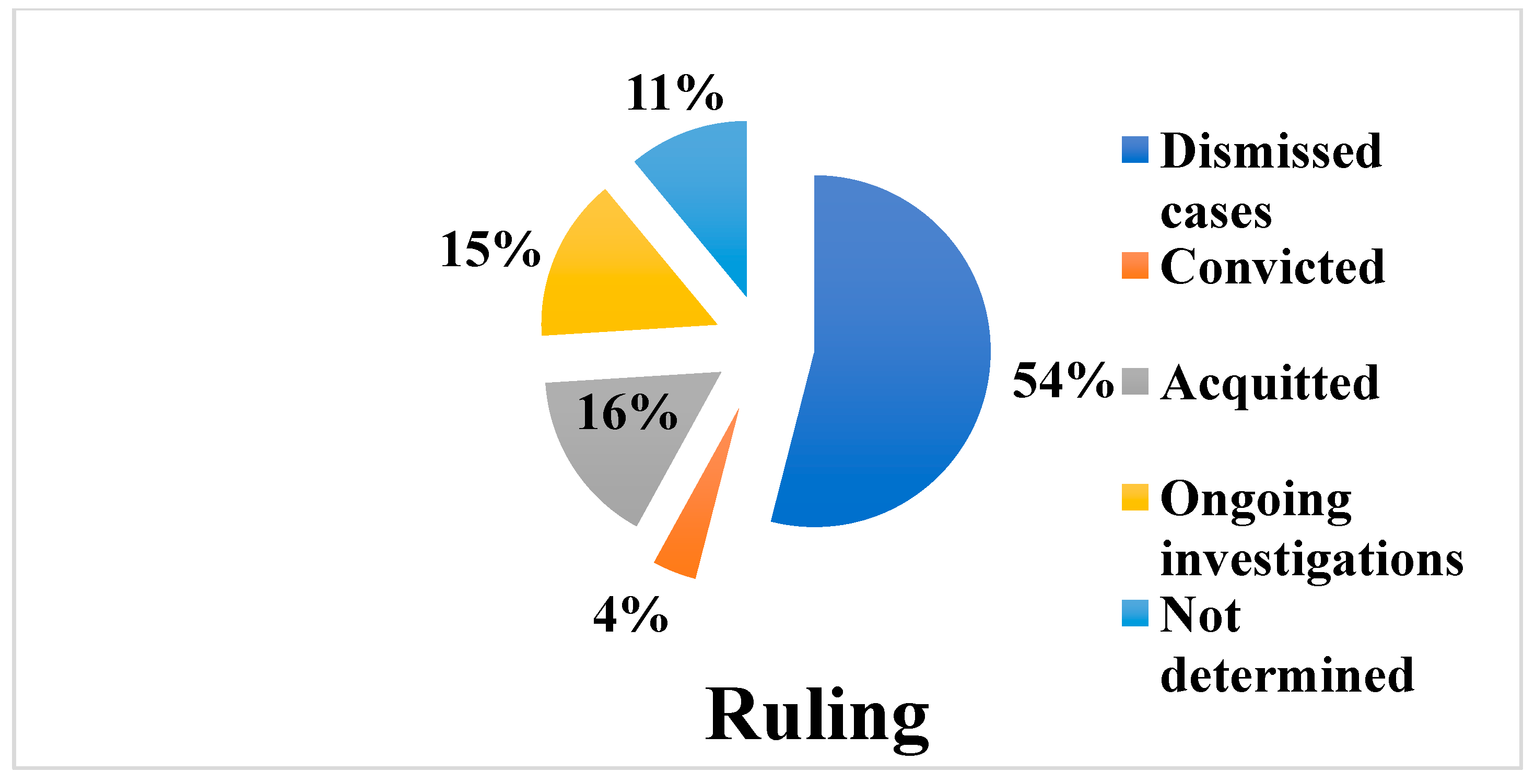
3.4. Trial Characteristics
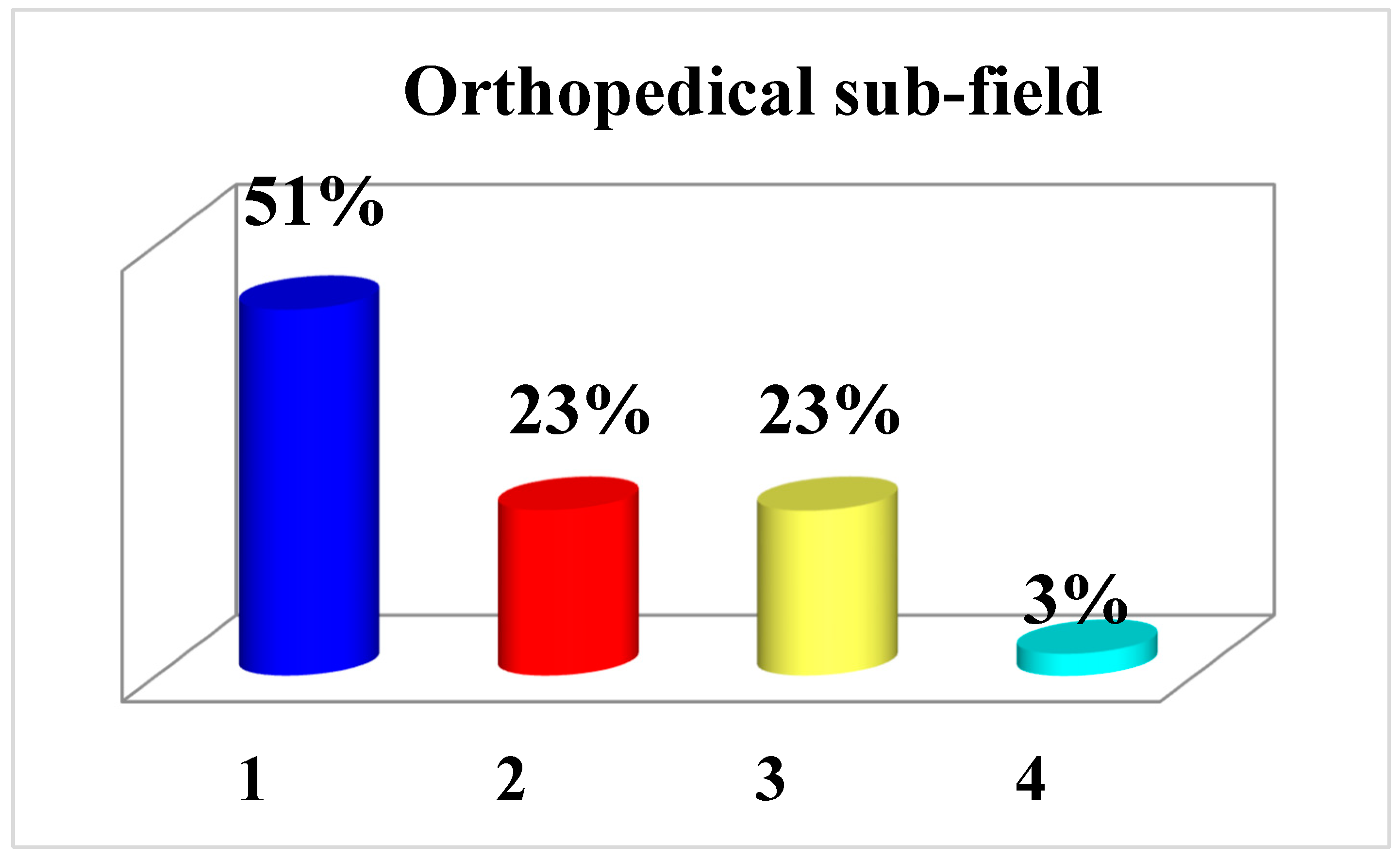
3.5. Orthopedic Sub-Fields Involved
3.6. Type of Healthcare Facility
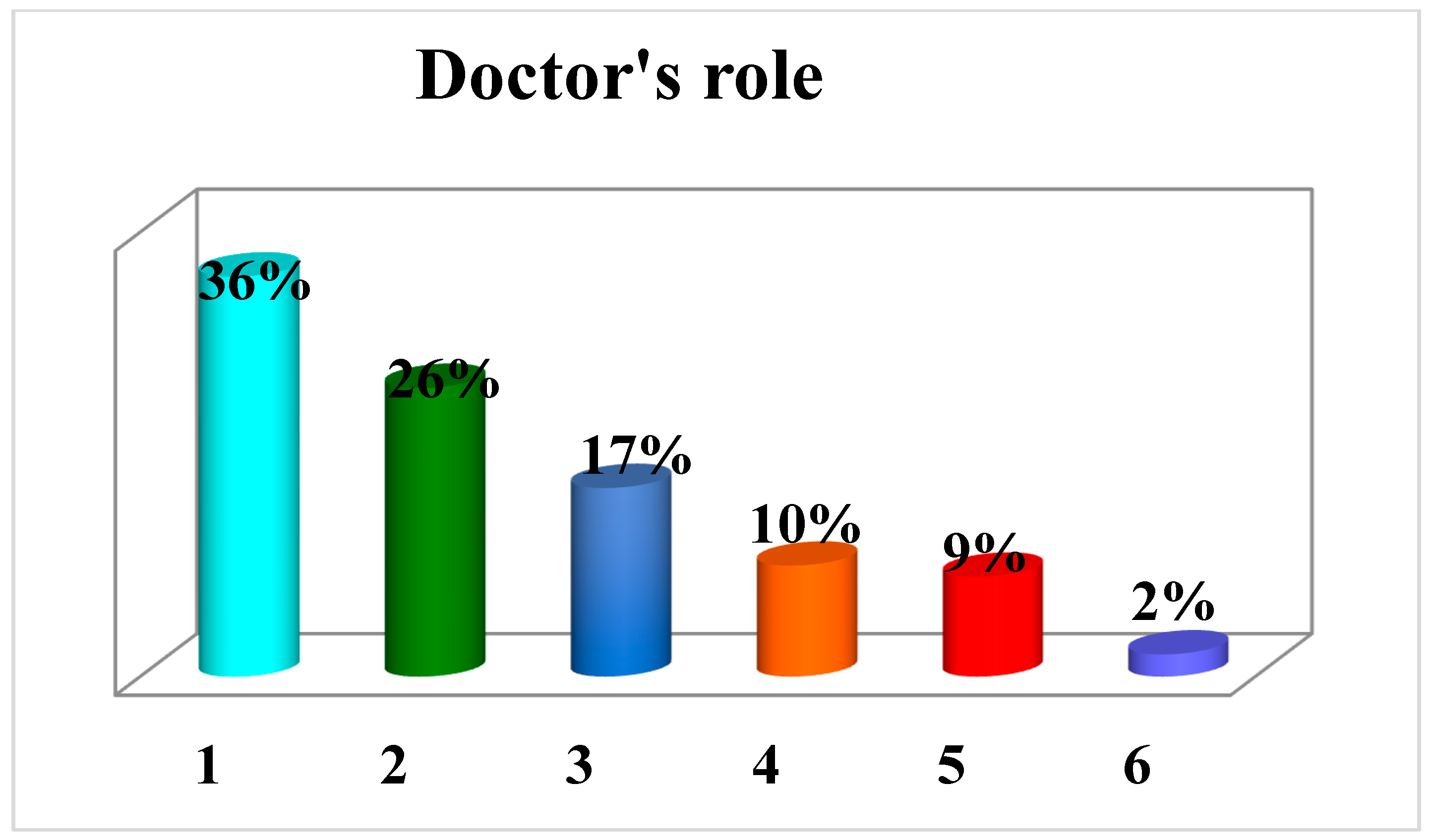
3.7. Role of Orthopedist
3.8. Causes of Deaths
3.9. Causes of Complaints
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Purcărea, V.L.; Gheorghe, I.R.; Petrescu, C.M. The Assessment of Perceived Service Quality of Public Health Care Services in Romania Using the SERVQUAL Scale. Procedia Econ. Financ. 2013, 6, 573–585. [Google Scholar] [CrossRef] [Green Version]
- Vetrugno, G.; Foti, F.; Grassi, V.M.; De-Giorgio, F.; Cambieri, A.; Ghisellini, R.; Clemente, F.; Marchese, L.; Sabatelli, G.; Delogu, G.; et al. Malpractice Claims and Incident Reporting: Two Faces of the Same Coin? Int. J. Environ. Res. Public Health 2022, 19, 16253. [Google Scholar] [CrossRef] [PubMed]
- Ries, M.D.; Bertino, J.S., Jr.; Nafziger, A.N. Distribution of orthopaedic surgeons, lawyers, and malpractice claims in New York. Clin. Orthop. Relat. Res. 1997, 337, 256–260. [Google Scholar] [CrossRef] [PubMed]
- Brennan, T.A.; Leape, L.L.; Laird, N.M.; Hebert, L.; Localio, A.R.; Lawthers, A.G.; Newhouse, J.P.; Weiler, P.C.; Hiatt, H.H. Incidence of adverse events and negligence in hospitalized patients: Results of the Harvard Medical Practice Study I. 1991. Qual. Saf. Health Care 2004, 13, 145–151, discussion 151–142. [Google Scholar] [CrossRef]
- Weiler, P.C.; Hiatt, H.H.; Newhouse, J.P.; Johnson, W.G.; Brennan, T.A.; Leape, L.L. A Measure of Malpractice. Medical Injury, Malpractice Litigation, and Patient Compensation; Harvard University Press: Cambridge, MA, USA, 1993. [Google Scholar]
- The Perverse Nature of the Medical Liability System. Available online: https://www.jec.senate.gov/public/_cache/files/1d42a169-05de-444f-954d-e0497581fcd4/the-perverse-nature-of-the-medical-liability-system-03-21-05.pdf (accessed on 12 December 2022).
- Sohn, D.H. Negligence, genuine error, and litigation. Int. J. Gen. Med. 2013, 6, 49–56. [Google Scholar] [CrossRef] [Green Version]
- Thornton, T.; Saha, S. The need for tort reform as part of health care reform. J. Long-Term Eff. Med. Implant. 2008, 18, 321–327. [Google Scholar] [CrossRef]
- Weinstein, S.L. Medical liability reform crisis 2008. Clin. Orthop. Relat. Res. 2009, 467, 392–401. [Google Scholar] [CrossRef] [Green Version]
- Institute of Medicine. To Err Is Human: Building a Safer Health System; The National Academies Press: Washington, DC, USA, 2000. [Google Scholar]
- Adamson, T.E.; Baldwin, D.C., Jr.; Sheehan, T.J.; Oppenberg, A.A. Characteristics of surgeons with high and low malpractice claims rates. West. J. Med. 1997, 166, 37–44. [Google Scholar]
- American Academy of Orthopaedic Surgery. Femur fracture care frequent cause of lawsuit. AAOS Bull. 2001, 49, 17–18. [Google Scholar]
- Gidwani, S.; Zaidi, S.M.; Bircher, M.D. Medical negligence in orthopaedic surgery: A review of 130 consecutive medical negligence reports. J. Bone Jt. Surg. Br. Vol. 2009, 91, 151–156. [Google Scholar] [CrossRef] [Green Version]
- Machin, J.; Briggs, T.; Krishnan, H.; Saker, S.; Bhamra, J.; Gillott, E. Litigation in trauma and orthopaedic surgery. J. Trauma Orthop. 2014, 2, 32–38. [Google Scholar]
- Tarantino, U.; Giai Via, A.; Macrì, E.; Eramo, A.; Marino, V.; Marsella, L.T. Professional liability in orthopaedics and traumatology in Italy. Clin. Orthop. Relat. Res. 2013, 471, 3349–3357. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Treglia, M.; Pallocci, M.; Passalacqua, P.; Giammatteo, J.; De Luca, L.; Mauriello, S.; Cisterna, A.M.; Marsella, L.T. Medical Liability: Review of a Whole Year of Judgments of the Civil Court of Rome. Int. J. Environ. Res. Public Health 2021, 18, 6019. [Google Scholar] [CrossRef]
- Casali, M.B.; Mobilia, F.; Sordo, S.D.; Blandino, A.; Genovese, U. The medical malpractice in Milan-Italy. A retrospective survey on 14 years of judicial autopsies. Forensic Sci. Int. 2014, 242, 38–43. [Google Scholar] [CrossRef] [PubMed]
- Feola, A.; Minotti, C.; Marchetti, D.; Caricato, M.; Capolupo, G.T.; Marsella, L.T.; La Monaca, G. A Five-Year Survey for Plastic Surgery Malpractice Claims in Rome, Italy. Medicina 2021, 57, 571. [Google Scholar] [CrossRef] [PubMed]
- Genovese, U.; Blandino, A.; Midolo, R.; Casali, M.B. Alleged malpractice in anesthesiology: Analysis of a series of private insurance claims. Minerva Anestesiol. 2016, 82, 202–209. [Google Scholar]
- Manca, R.; Bruti, V.; Napoletano, S.; Marinelli, E. A 15 years survey for dental malpractice claims in Rome, Italy. J. Forensic Leg. Med. 2018, 58, 74–77. [Google Scholar] [CrossRef]
- Traina, F. Medical malpractice: The experience in Italy. Clin. Orthop. Relat. Res. 2009, 467, 434–442. [Google Scholar] [CrossRef] [Green Version]
- Cascini, F.; Santaroni, F.; Lanzetti, R.; Failla, G.; Gentili, A.; Ricciardi, W. Developing a Data-Driven Approach in Order to Improve the Safety and Quality of Patient Care. Front. Public Health 2021, 9, 667819. [Google Scholar] [CrossRef]
- Foti, F.; De-Giorgio, F.; Vetrugno, G. Communication and Resolution Programs in the COVID-19 Era: A Unique Opportunity to Enhance Patient Safety (and Save Money). J. Patient Saf. 2021, 17, 174. [Google Scholar] [CrossRef]
- Foti, F.; Vetrugno, G.; De-Giorgio, F.; Cicconi, M. Consent for elective surgery: Audiovisual devices could be used. BMJ Clin. Res. Ed. 2020, 370, m3158. [Google Scholar] [CrossRef] [PubMed]
- De-Giorgio, F.; Panarella, L.; Miscusi, M.; d’Aloja, E.; Spagnolo, A.G.; Pascali, V.L.; Vetrugno, G. Look but … please don’t touch! Med. Sci. Law 2015, 55, 315–317. [Google Scholar] [CrossRef] [PubMed]
- Vetrugno, G.; Foti, F.; Spagnolo, A.; De-Giorgio, F. Reconciling patients’ need for compensation with doctors’ need for protection. BMJ Clin. Res. Ed. 2019, 365, l1717. [Google Scholar] [CrossRef] [PubMed]
- Supreme Court of Cassation, Sixth Penal Section, Verdict 07/03/2019 n° 10093. Available online: https://www.cortedicassazione.it/corte-di-cassazione/it/servizi_online.page (accessed on 14 January 2023).
- De Giorgio, F.; Vetrugno, G. The future of academic forensic medicine cannot renounce its past and must live up to the challenges of modern public health care—The role of forensic social medicine and of forensic clinical risk management. Forensic Sci. Int. 2007, 168, e56–e57, author reply e58. [Google Scholar] [CrossRef]
- Kessler, D.; McClellan, M. Malpractice law and health care reform: Optimal liability policy in an era of managed care. J. Public Econ. 2002, 84, 175–197. [Google Scholar] [CrossRef]
- Garcia-Alamino, J.M.; López-Cano, M. Overdiagnosis and overtreatment—More is better? Cir. Esp. 2022, 100, 793–794. [Google Scholar] [CrossRef]
- Gupta, P.; Gupta, M.; Koul, N. Overdiagnosis and overtreatment; how to deal with too much medicine. J. Fam. Med. Prim. Care 2020, 9, 3815–3819. [Google Scholar] [CrossRef]
- Tozzi, Q. Il Progetto Agenas sulla Medicina Difensiva. Available online: https://www.agenas.gov.it/images/agenas/Agenews/newsletter5-2015/Medicina_Difensiva_Articolo.pdf (accessed on 16 January 2023).





Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bernardinangeli, C.; Giannace, C.; Cerciello, S.; Grassi, V.M.; Lodise, M.; Vetrugno, G.; De-Giorgio, F. A Fifteen-Year Survey for Orthopedic Malpractice Claims in the Criminal Court of Rome. Healthcare 2023, 11, 962. https://doi.org/10.3390/healthcare11070962
Bernardinangeli C, Giannace C, Cerciello S, Grassi VM, Lodise M, Vetrugno G, De-Giorgio F. A Fifteen-Year Survey for Orthopedic Malpractice Claims in the Criminal Court of Rome. Healthcare. 2023; 11(7):962. https://doi.org/10.3390/healthcare11070962
Chicago/Turabian StyleBernardinangeli, Camilla, Carolina Giannace, Simone Cerciello, Vincenzo M. Grassi, Maria Lodise, Giuseppe Vetrugno, and Fabio De-Giorgio. 2023. "A Fifteen-Year Survey for Orthopedic Malpractice Claims in the Criminal Court of Rome" Healthcare 11, no. 7: 962. https://doi.org/10.3390/healthcare11070962
APA StyleBernardinangeli, C., Giannace, C., Cerciello, S., Grassi, V. M., Lodise, M., Vetrugno, G., & De-Giorgio, F. (2023). A Fifteen-Year Survey for Orthopedic Malpractice Claims in the Criminal Court of Rome. Healthcare, 11(7), 962. https://doi.org/10.3390/healthcare11070962