


COPD and Depression Analysis in Regard to Obstructive Pulmonary Levels
 ,
, 
 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Methods
- Patient Health Questionnaire-9 (PHQ-9);
- Quality of Life Enjoyment and Satisfaction Questionnaire–Short Form (Q-LES-Q-SF);
- Hamilton Depression Rating Scale-17 (HDRS).
2.3. Statistical Analysis
3. Results
3.1. Sample Characteristics
3.2. COPD Stages in Patients
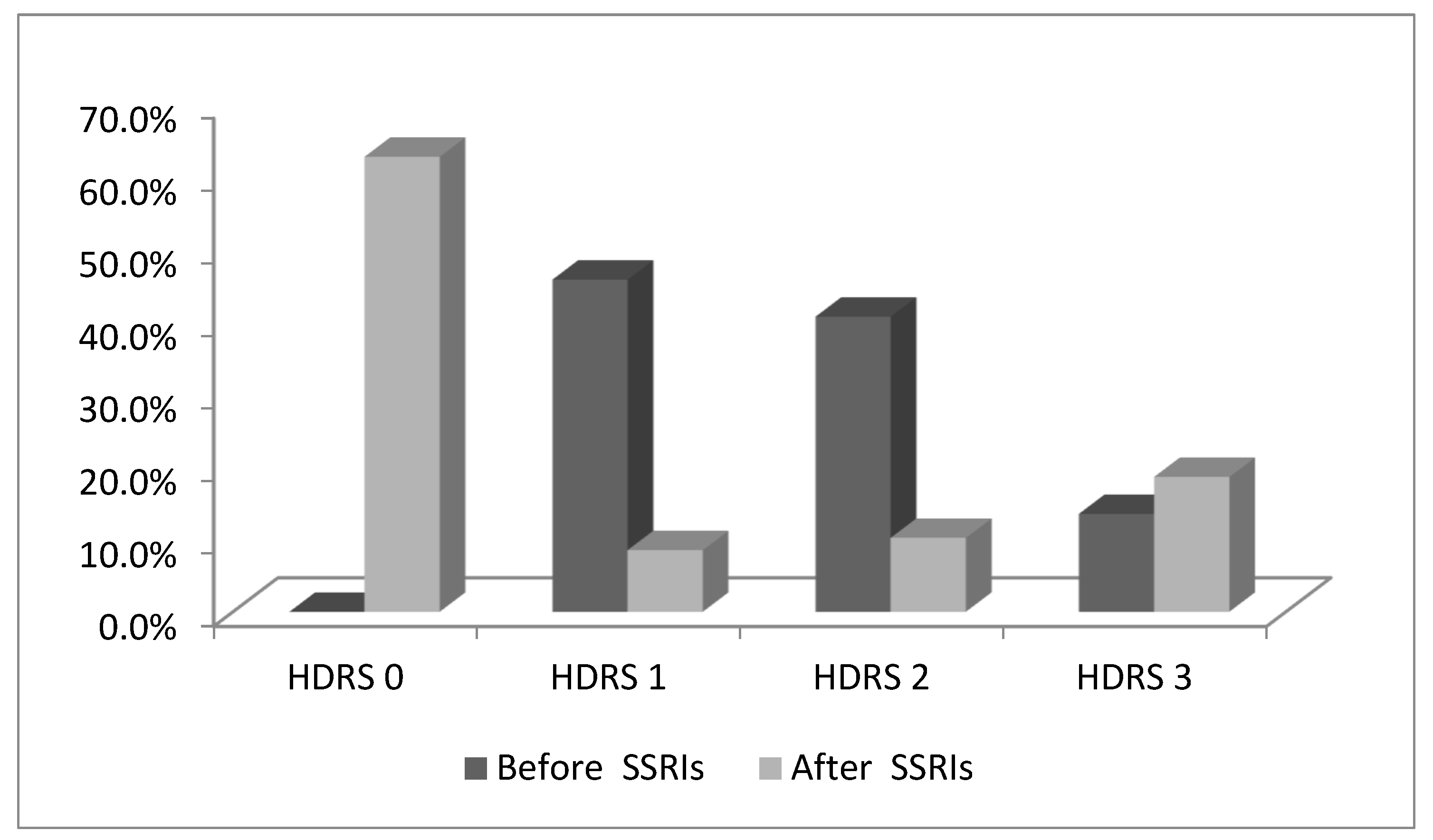
3.3. Depression in COPD Patients before and after Therapy
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
| Variable | Before SSRIs | After SSRIs | p | |
|---|---|---|---|---|
| (n, %) | (n, %) | |||
| Social behavior | ||||
| Level 0 | 16 (18.4) | 5 (5.7) | <0.01 | |
| Level 1 | 27 (31) | |||
| Level 2 | 21 (24.1) | 1 (1.1) | ||
| Level 3 | 11 (12.6) | 1 (1.1) | ||
| Family behavior | ||||
| Level 0 | 20 (23) | 19 (21.8) | >0.05 | |
| Level 1 | 27 (31) | 21 (24.1) | ||
| Level 2 | 21 (24.1) | 15 (17.2) | ||
| Level 3 | 11 (12.6) | 9 (10.3) | ||
| A sense of wellbeing | ||||
| Level 0 | 19 (21.8) | 3 (3.4) | ||
| Level 1 | 32 (36.8) | 1 (1.1) | <0.01 | |
| Level 2 | 23 (26.4) | 1 (1.1) | ||
| Level 3 | 11 (12.6) | 3 (3.4) | ||
| Characteristics | Before SSRIs | After SSRIs | p |
|---|---|---|---|
| (n, %) | (n, %) | ||
| Free activity | |||
| Level 0 | 20 (23) | 1 (1.1) | <0.01 |
| Level 1 | 25 (28.7) | - | |
| Level 2 | 16 (18.4) | 1 (1.1) | |
| Level 3 | 10 (11.5) | - | |
| Functioning in daily life | |||
| Level 0 | 19 (21.8) | 1 (1.1) | <0.01 |
| Level 1 | 23 (26.4) | 2 (2.3) | |
| Level 2 | 17 (19.5) | 1 (1.1) | |
| Level 3 | 9 (10.3) | 3 (3.4) | |
| Variable | Before SSRIs | After SSRIs | p |
|---|---|---|---|
| (n, %) | (n, %) | ||
| Social behavior | |||
| Stage I | 7 (8) | 1 (1.1) | <0.01 |
| Stage II | 53 (60.9) | 5 (5.7) | |
| Stage III | 13 (14.9) | 1 (1.1) | |
| Stage IV | 2 (2.3) | 1 (1.1) | |
| Family behavior | |||
| Stage I | 9 (10.3) | 8 (9.2) | >0.05 |
| Stage II | 54 (62.1) | 42 (48.3) | |
| Stage III | 14 (16.1) | 13 (14.9) | |
| Stage IV | 2 (2.3) | 1 (1.1) | |
| A sense of wellbeing | |||
| Stage I | 11 (12.6) | - | <0.01 |
| Stage II | 57 (65.5) | 5 (5.7) | |
| Stage III | 15 (17.2) | 3 (3.4) | |
| Stage IV | 2 (2.3) | - | |
| Characteristics | Before SSRIs | After SSRIs | p |
|---|---|---|---|
| (n, %) | (n, %) | ||
| Free activity | |||
| Stage I | 7 (8) | - | <0.01 |
| Stage II | 47 (54) | - | |
| Stage III | 15 (17.2) | 2 (2.3) | |
| Stage IV | 2 (2.3) | - | |
| Functioning in daily life | |||
| Stage I | 10 (11.5) | 1 (1.1) | <0.01 |
| Stage II | 43 (49.4) | 4 (4.6) | |
| Stage III | 13 (14.9) | 1 (1.1) | |
| Stage IV | 2 (2.3) | 1 (1.1) | |
References
- Clarke, S.; Munro, P.E.; Lee, A.L. The role of manual therapy in patients with COPD. Healthcare 2019, 7, 21. [Google Scholar] [CrossRef]
- Vukoja, M.; Kopitovic, I.; Lazic, Z.; Milenkovic, B.; Stankovic, I.; Zvezdin, B.; Ilic, A.D.; Cekerevac, I.; Vukcevic, M.; Zugic, V.; et al. Diagnosis and management of chronic obstructive pulmonary disease in Serbia: An expert group position statement. Int. J. Chronic Obstr. Pulm. Dis. 2019, 14, 1993–2002. [Google Scholar] [CrossRef] [PubMed]
- Global Initiative for Chronic Obstructive Lung Disease. Pocket Guide to COPD Diagnosis, Management, and Prevention. Global Initiative for Chronic Obstructive Lung Disease, 2017. Available online: https://goldcopd.org/wp-content/uploads/2017/02/wms-GOLD-2017-FINAL.pdf (accessed on 25 December 2021).
- Dua, R.; Das, A.; Kumar, A.; Kumar, S.; Mishra, M.; Sharma, K. Association of comorbid anxiety and depression with chronic obstructive pulmonary disease. Lung India 2018, 35, 31–36. [Google Scholar] [CrossRef] [PubMed]
- Lacasse, Y.; Rousseau, L.; Maltais, F. Prevalence of depressive symptoms and depression in patients with severe oxygen-dependent chronic obstructive pulmonary disease. J. Cardiopulm. Rehabil. Prev. 2011, 21, 80–86. [Google Scholar] [CrossRef] [PubMed]
- Yin, H.L.; Yin, S.Q.; Lin, Q.Y.; Xu, Y.; Xu, H.W.; Liu, T. Prevalence of comorbidities in chronic obstructive pulmonary disease patients: A meta-analysis. Medicine 2017, 96, e6836. [Google Scholar] [CrossRef] [PubMed]
- Yohannes, A.M.; Alexopoulos, G.S. Depression and anxiety in patients with COPD. Eur. Respir. Rev. 2014, 23, 345–349. [Google Scholar] [CrossRef]
- Matte, D.L.; Pizzichini, M.M.; Hoepers, A.T.; Diaz, A.P.; Karloh, M.; Dias, M.; Pizzichini, E. Prevalence of depression in COPD: A systematic review and meta-analysis of controlled studies. Respir. Med. 2016, 117, 154–161. [Google Scholar] [CrossRef]
- Dubois, T.; Reynaert, C.; Jacques, D.; Zdanowicz, N. The PsychoImmunological Model as a Psychosomatic Entity: A Literature Review of Interactions between Depression and Immunity. Psychiatr. Danub. 2017, 29, 254–258. [Google Scholar]
- Moitra, S.; Puri, R.; Paul, D.; Huang, Y.C.T. Global perspectives of emerging occupational and environmental lung diseases. Curr. Opin. Pulm. Med. 2015, 21, 114–120. [Google Scholar] [CrossRef]
- De Aquino, J.P.; Londono, A.; Carvalho, A.F. An update on the epidemiology of major depressive disorder across cultures. In Understanding Depression; Springer: Berlin/Heidelberg, Germany, 2018; pp. 309–315. [Google Scholar]
- Barnes, P.J. Chronic Obstructive pulmonary Disease: Effect beyond the lungs. PLoS Med. 2010, 7, e1000220. [Google Scholar] [CrossRef]
- Janson, C.; Björnsson, E.; Hetta, J.; Boman, G. Anxiety and depression in relation to respiratory symptoms and asthma. Am. J. Respir. Crit. Care Med. 2014, 149, 930–934. [Google Scholar] [CrossRef] [PubMed]
- Hsu, K.Y.; Lin, J.R.; Lin, M.S.; Chen, W.; Chen, Y.J.; Yan, Y.H. The modified Medical Research Council dyspnea scale is a good indicator of health-related quality of life in patients with chronic obstructive pulmonary disease. Singap. Med. J. 2013, 54, 321–327. [Google Scholar] [CrossRef] [PubMed]
- Criner, G.J.; Celli, B.R.; Brightling, C.E.; Agusti, A.; Papi, A.; Singh, D.; Sin, D.D.; Vogelmeier, C.F.; Sciurba, F.C.; Bafadhel, M.; et al. Benralizumab for the Prevention of COPD Exacerbations. N. Engl. J. Med. 2019, 381, 1023. [Google Scholar] [CrossRef] [PubMed]
- Van den Bemt, L.; Schermer, T.; Bor, H.; Smink, R.; van Weel-Baumgarten, E.; Lucassen, P.; van Weel, C. The risk for depression comorbidity in patients with COPD. Chest 2009, 135, 108–114. [Google Scholar] [CrossRef] [PubMed]
- Way, B.M.; Lieberman, M. Is there a genetic contribution to cultural differences? Collectivism, individualism and genetic markers of social sensitivity. Soc. Cogn. Affect. Neurosci. 2010, 5, 203–211. [Google Scholar] [CrossRef]
- Safa, M.; Tafti, S.F.; Talischi, F.; Boroujerdi, F.G. Severity of anxiety disorders in patients with chronic obstructive pulmonary disease. Iran. J. Psychiatry 2015, 10, 128–132. [Google Scholar]
- Alqahtani, J.S.; Njoku, C.M.; Bereznick, I.B.; Wimmer, B.C.; Peterson, G.M.; Kinsman, L.; Aldabayan, Y.S.; Alrajeh, A.M.; Aldhahir, A.M.; Mandal, S.; et al. Risk factors for all-cause hospital readmission following exacerbation of COPD: A systematic review and meta-analysis. Eur. Respir. Rev. 2020, 29, 190166. [Google Scholar] [CrossRef]
- Volpato, E.; Banfi, P.; Pagnini, F. Promoting Acceptance and Adherence to Noninvasive Ventilation in Chronic Obstructive Pulmonary Disease: A Randomized Controlled Trial. Psychosom. Med. 2022, 84, 488–504. [Google Scholar] [CrossRef]
- Bratek, A.; Zawada, K.; Beil-Gawelczyk, J.J.; Beil, S.; Sozanska, E.; Krysta, K.; Barczyk, A.; Krupka-Matuszczyk, I.; Pierzchala, W. Depressiveness, symptoms of anxiety and cognitive dysfunctions in patients with asthma and chronic obstructive pulmonary disease (COPD): Possible associations with inflammation markers: A pilot study. J. Neural Transm. 2015, 122, S83–S91. [Google Scholar] [CrossRef]
- Martínez-Gestoso, S.; García-Sanz, M.T.; Carreira, J.M.; Salgado, F.J.; Calvo-Álvarez, U.; Doval-Oubiña, L.; Camba-Matos, S.; Peleteiro-Pedraza, L.; González-Pérez, M.A.; Penela-Penela, P.; et al. Impact of anxiety and depression on the prognosis of copd exacerbations. BMC Pulm. Med. 2022, 22, 169. [Google Scholar]
- Yohannes, A.M.; Baldwin, R.C.; Connolly, M.J. Depression and anxiety in elderly patients with chronic obstructive pulmonary disease. Age Ageing 2006, 35, 457–459. [Google Scholar] [CrossRef]
- Maric, D.; Jovanovic, D.; Obradovic, L.N.; Vukicevic, T.A.; Popevic, S.; Pekmezovic, T. Self-Reported Physical and Mental Health of Copd and Nsclc Caregivers: Relevance for Palliative Care Implementation in Serbia. Research Square 2021. [Google Scholar] [CrossRef]
- Jelic, I.; Folic, M.; Mihajlovic, F.; Jankovic, S.; Mihajlovic, G. The Effects of Antidepressant Therapy on Health-Related Quality of Life in Patients with a Chronic Obstructive Pulmonary Disease and Depressive Symptoms. Serb. J. Exp. Clin. Res. 2022, in press. [CrossRef]
- Global Initiative for Chronic Obstructive Lung Disease (GOLD). Global Strategy for the Diagnosis, Management and Prevention of Chronic Obstructive Pulmonary Disease: 2019 Report. Available online: https://goldcopd.org/wp-content/uploads/2018/11/GOLD-2019-v1.7-FINAL-14Nov2018-WMS.pdf (accessed on 4 February 2022).
- Bhatt, S.P.; Balte, P.P.; Schwartz, J.E.; Cassano, P.A.; Couper, D.; Jacobs, D.R.; Oelsner, E.C. Discriminative Accuracy of FEV1: FVC Thresholds for COPD-Related Hospitalization and Mortality. JAMA 2019, 321, 2438. [Google Scholar] [CrossRef] [PubMed]
- Mahler, D.A.; Wells, C.K. Evaluation of clinical methods for rating dyspnea. Chest 1988, 93, 580–586. [Google Scholar] [CrossRef]
- Hamilton, M. The Hamilton rating scale for depression. In Assessment of Depression; Springer: Berlin/Heidelberg, Germany, 1986; pp. 143–152. [Google Scholar]
- Kuehner, C. Why is depression more common among women than among men? Lancet Psychiatry 2017, 4, 146–158. [Google Scholar] [CrossRef]
- Carvalho, N.S.; Ribeiro, P.R.; Ribeiro, M.; Nunes, M.D.P.T.; Cukier, A.; Stelmach, R. Comparing asthma and chronic obstructive pulmonary disease in terms of symptoms of anxiety and depression. J. Bras. Pneumol. 2007, 33, 1–6. [Google Scholar] [CrossRef]
- Schane, R.E.; Walter, L.C.; Dinno, A.; Covinsky, K.E.; Woodruff, P.G. Prevalence and risk factors for depressive symptoms in persons with chronic obstructive pulmonary disease. J. Gen. Intern. Med. 2018, 23, 1757–1762. [Google Scholar] [CrossRef] [PubMed]
- Steffen, A.; Nübel, J.; Jacobi, F.; Bätzing, J.; Holstiege, J. Mental and somatic comorbidity of depression: A comprehensive cross-sectional analysis of 202 diagnosis groups using German nationwide ambulatory claims data. BMC Psychiatry 2020, 20, 142. [Google Scholar] [CrossRef]
- Raherison, C.; Girodet, P.O. Epidemiology of COPD. Eur. Respir. Rev. 2009, 18, 213–221. [Google Scholar] [CrossRef]
- Perera, W.R.; Hurst, J.R.; Wilkinson, T.M.A.; Sapsford, R.J.; Müllerova, H.; Donaldson, G.C.; Wedzicha, J.A. Inflammatory changes, recovery and recurrence at COPD exacerbation. Eur. Respir. J. 2007, 29, 527–534. [Google Scholar] [CrossRef] [PubMed]
- Huynh, N.N.; McIntyre, R.S. What Are the Implications of the STAR*D Trial for Primary Care? A Review and Synthesis. Prim. Care Companion J. Clin. Psychiatry 2008, 10, 91–96. [Google Scholar] [CrossRef] [PubMed]
- Souza, N.P.; Garbin, C.A. Assessment of health-related quality of life and related factors in patients with chronic liver disease. Braz. J. Inf. Dis. 2015, 19, 590–595. [Google Scholar] [CrossRef] [PubMed]
- Khan, S.; Patil, B.B. Risk of depression in patients with chronic obstructive pulmonary disease and its determinants. Indian J. Health Sci. Biomed. Res. 2017, 10, 110–115. [Google Scholar] [CrossRef]
- Cafarella, P.A.; Effing, T.W.; Usmani, Z.A.; Frith, P.A. Treatments for anxiety and depression in patients with chronic obstructive pulmonary disease: A literature review. Respirology 2012, 17, 627–638. [Google Scholar] [CrossRef]
- World Health Organization. Depression and Other Common Mental Disorders: Global Health Estimates; WHO: Geneva, Switzerland, 2017. [Google Scholar]
| FEV1/mMRC | n (%) | p | Age | p | Sex (n, %) | p | |
|---|---|---|---|---|---|---|---|
| Female | Male | ||||||
| FEV1 | |||||||
| Stage I | 11 (12.6) | <0.01 | 42.2 ± 6.02 | <0.05 | 8 (9.2) | 3 (3.4) | >0.05 |
| Stage II | 59 (67.8) | 49.9 ± 6.6 | 39 (44.8) | 20 (23) | |||
| Stage III | 15 (17.2) | 44.7 ± 9.6 | 9 (10.3) | 6 (6.9) | |||
| Stage IV | 2 (2.3) | 42 ± 1.4 | 1 (1.1) | 1 (1.1) | |||
| mMRC | |||||||
| Level 0 | 20 (23) | <0.05 | 51.2 ± 5.9 | <0.05 | 13 (14.9) | 7 (8) | >0.05 |
| Level 1 | 33 (37.9) | 44.9 ± 6.9 | 23 (26.4) | 10 (11.5) | |||
| Level 2 | 23 (26.4) | 50.7 ± 6.9 | 16 (18.4) | 7 (8) | |||
| Level 3 | 11 (12.6) | 52.7 ± 7.7 | 5 (5.7) | 6 (6.9) | |||
| Variables | HDRS (%) | p | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Before SSRIs | After SSRIs | ||||||||
| 0 | 1 | 2 | 3 | 0 | 1 | 2 | 3 | ||
| FEV1 | |||||||||
| Stage I | 0 | 12.6 | / | / | 9.2 | / | 3.4 | / | <0.01 |
| Stage II | 0 | 31 | 27.6 | 9.2 | 42.5 | 5.7 | 6.9 | 12.6 | |
| Stage III | 0 | 8 | / | 9.2 | 16.1 | 1.1 | / | / | |
| Stage IV | 0 | 2.3 | / | / | 2.3 | / | / | / | |
| mMRC | |||||||||
| Level 0 | 0 | 5.7 | 12.6 | 4.6 | 16.1 | 2.3 | 2.3 | 2.3 | <0.01 |
| Level 1 | 0 | 33.3 | 3.4 | 1.1 | 29.9 | 1.1 | 3.4 | 3.4 | |
| Level 2 | 0 | 11.5 | 9.2 | 5.7 | 12.6 | 3.4 | 3.4 | 6.9 | |
| Level 3 | 0 | 3.4 | 2.3 | 6.9 | 11.5 | / | 1.1 | / | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jelić, I.; Mihajlović, G.; Mihajlović, F.; Minić, N.; Ratinac, M.; Pantović-Stefanović, M. COPD and Depression Analysis in Regard to Obstructive Pulmonary Levels. Healthcare 2023, 11, 1175. https://doi.org/10.3390/healthcare11081175
Jelić I, Mihajlović G, Mihajlović F, Minić N, Ratinac M, Pantović-Stefanović M. COPD and Depression Analysis in Regard to Obstructive Pulmonary Levels. Healthcare. 2023; 11(8):1175. https://doi.org/10.3390/healthcare11081175
Chicago/Turabian StyleJelić, Ivana, Goran Mihajlović, Filip Mihajlović, Nataša Minić, Miloš Ratinac, and Maja Pantović-Stefanović. 2023. "COPD and Depression Analysis in Regard to Obstructive Pulmonary Levels" Healthcare 11, no. 8: 1175. https://doi.org/10.3390/healthcare11081175
APA StyleJelić, I., Mihajlović, G., Mihajlović, F., Minić, N., Ratinac, M., & Pantović-Stefanović, M. (2023). COPD and Depression Analysis in Regard to Obstructive Pulmonary Levels. Healthcare, 11(8), 1175. https://doi.org/10.3390/healthcare11081175