
Task Shifting and Task Sharing Implementation in Africa: A Scoping Review on Rationale and Scope


Abstract
:1. Introduction
2. Materials and Methods
3. Results
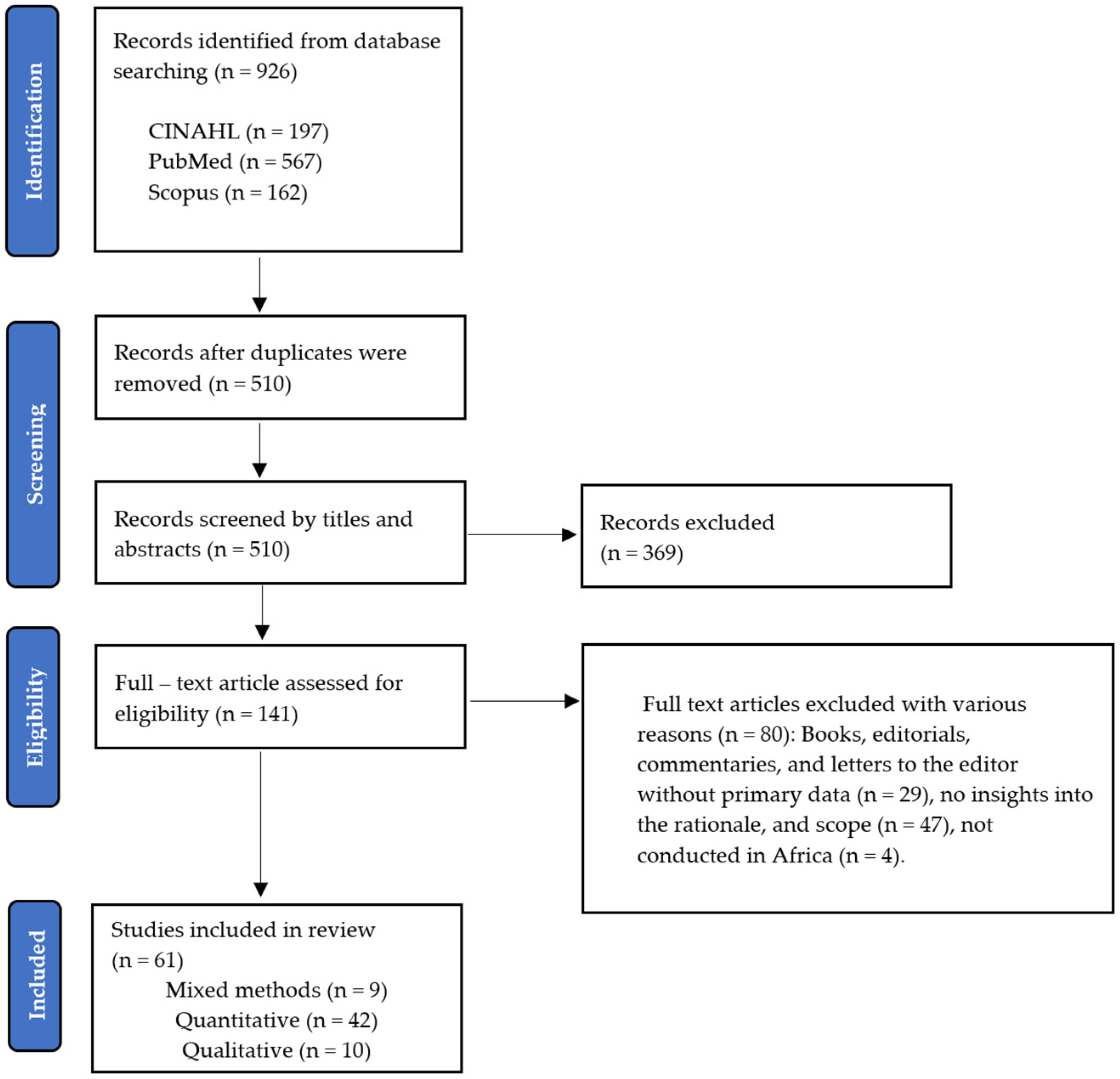
3.1. Description of Studies
3.2. Characteristics of the Included Studies
3.3. Main Themes from the Included Studies
3.3.1. Rationale for Task Shifting and Task Sharing
Health Worker Shortages
Optimally Utilize Existing Health Workers
Expand Access to Health Services
3.3.2. Scope of Shifted and Shared Tasks
HIV/AIDS Care
Hypertension Management
Diabetes Management
Mental Health
Maternal and Child Healthcare
Sexual and Reproductive Health Services
Eye Care
Tuberculosis Care
Surgical Care and Procedures
Medicines’ Management
Emergency Care
4. Discussion
4.1. Implications for Policy and Practice
4.2. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
| Section | Item | Prisma-ScR Checklist Item | Reported on Page # |
|---|---|---|---|
| TITLE | |||
| Title | 1 | Identify the report as a scoping review. | 1 |
| ABSTRACT | |||
| Structured summary | 2 | Provide a structured summary that includes (as applicable): background, objectives, eligibility criteria, sources of evidence, charting methods, results, and conclusions that relate to the review questions and objectives. | 1 |
| INTRODUCTION | |||
| Rationale | 3 | Describe the rationale for the review in the context of what is already known. Explain why the review questions/objectives lend themselves to a scoping review approach. | 2, 3 |
| Objectives | 4 | Provide an explicit statement of the questions and objectives being addressed with reference to their key elements (e.g., population or participants, concepts, and context) or other relevant key elements used to conceptualize the review questions and/or objectives. | 3 |
| METHODS | |||
| Protocol and registration | 5 | Indicate whether a review protocol exists, state if and where it can be accessed (e.g., a Web address), and if available, provide registration information, including the registration number. | - |
| Eligibility criteria | 6 | Specify characteristics of the sources of evidence used as eligibility criteria (e.g., years considered, language, and publication status), and provide a rationale. | 4 |
| Information sources | 7 | Describe all information sources in the search (e.g., databases with dates of coverage and contact with authors to identify additional sources), as well as the date the most recent search was executed. | 4 |
| Search | 8 | Present the full electronic search strategy for at least 1 database, including any limits used, such that it could be repeated. | 3 |
| Selection of sources of Evidence | 9 | State the process for selecting sources of evidence (i.e., screening and eligibility) included in the scoping review. | 4 |
| Data charting process | 10 | Describe the methods of charting data from the included sources of evidence (e.g., calibrated forms or forms that have been tested by the team before their use, and whether data charting was done independently or in duplicate) and any processes for obtaining and confirming data from investigators. | 4 |
| Data items | 11 | List and define all variables for which data were sought and any assumptions and simplifications made. | 3 |
| Critical appraisal of individual sources of evidence | 12 | If done, provide a rationale for conducting a critical appraisal of included sources of evidence. Describe the methods used and how this information was used in any data synthesis (if appropriate). | - |
| Synthesis of results | 13 | Describe the methods of handling and summarizing the data that were charted. | 4, 5 |
References
- World Health Organization. WHO Recommendations: Optimizing Health Worker Roles to Improve Access to Key Maternal and Newborn Health Interventions through Task Shifting; World Health Organization: Geneva, Switzerland, 2012.
- World Health Organization. Task Shifting: Rational Redistribution of Tasks among health Workforce Teams: Global Recommendations and Guidelines; World Health Organization: Geneva, Switzerland, 2007.
- Orkin, A.M.; Rao, S.; Venugopal, J.; Kithulegoda, N.; Wegier, P.; Ritchie, S.D.; Vanderburgh, D.; Martiniuk, A.; Salamanca-Buentello, F.; Upshur, R. Conceptual framework for task shifting and task sharing: An international Delphi study. Hum. Resour. Health 2021, 19, 61. [Google Scholar] [CrossRef]
- World Health Organization. The State of the Health Workforce in the WHO African Region; World Health Organization: Brazzaville, Congo, 2021.
- World Health Organization. The State of Health in the WHO African Region: An Analysis of the Status of Health, Health Services and Health Systems in the Context of the Sustainable Development Goals; World Health Organization: Brazzaville, Congo, 2018.
- World Health Organization. Road Map for Scaling up the Human Resources for Health for Improved Health Service Delivery in the African Region 2012–2025: Adopted by the Sixty-Second Session of the Regional Committee; World Health Organization: Brazzaville, Congo, 2013.
- World Health Organization. Everybody’s Business: Strengthening Health Systems to Improve Health Outcomes: WHO’s Framework for Action; World Health Organization: Geneva, Switzerland; Brazzaville, Congo, 2007.
- World Health Organization. The World Health Report 2006—Working Together for Health; World Health Organization: Geneva, Switzerland, 2006.
- Russo, G.; Xu, L.; McIsaac, M.; Matsika-Claquin, M.D.; Dhillon, I.; Mcpake, B.; Campbell, J. Health workers’ strikes in low-income countries: The available evidence. Bull. World Health Organ. 2019, 97, 460. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Global Strategy on Human Resources for Health: Workforce 2030; World Health Organization: Geneva, Switzerland, 2016.
- Esu, E.B.; Chibuzor, M.; Aquaisua, E.; Udoh, E.; Sam, O.; Okoroafor, S.; Ongom, M.; Effa, E.; Oyo-Ita, A.; Meremikwu, M. Interventions for improving attraction and retention of health workers in rural and underserved areas: A systematic review of systematic reviews. J. Public Health 2021, 43, i54–i66. [Google Scholar] [CrossRef] [PubMed]
- Orkin, A.M.; Venugopal, J.; Curran, J.D.; Fortune, M.K.; Mcarthur, A.; Mew, E.; Ritchie, S.D.; Drennan, I.R.; Exley, A.; Jamieson, R.; et al. Emergency care with lay responders in underserved populations: A systematic review. Bull. World Health Organ. 2021, 99, 514–528H. [Google Scholar] [CrossRef]
- Federspiel, F.; Mukhopadhyay, S.; Milsom, P.J.; Scott, J.W.; Riesel, J.N.; Meara, J.G. Global surgical, obstetric, and anesthetic task shifting: A systematic literature review. Surgery 2018, 164, 553–558. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Y.; Hagel, C.; Tweheyo, R.; Sirili, N.; Gathara, D.; English, M. Task-sharing to support paediatric and child health service delivery in low- and middle-income countries: Current practice and a scoping review of emerging opportunities. Hum. Resour. Health 2021, 19, 95. [Google Scholar] [CrossRef] [PubMed]
- Polus, S.; Lewin, S.; Glenton, C.; Lerberg, P.M.; Rehfuess, E.; Gülmezoglu, A.M. Optimizing the delivery of contraceptives in low- and middle-income countries through task shifting: A systematic review of effectiveness and safety. Reprod. Health 2015, 12, 27. [Google Scholar] [CrossRef]
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef]
- Colquhoun, H.L.; Levac, D.; O’Brien, K.K.; Straus, S.; Tricco, A.C.; Perrier, L.; Kastner, M.; Moher, D. Scoping reviews: Time for clarity in definition, methods, and reporting. J. Clin. Epidemiol. 2014, 67, 1291–1294. [Google Scholar] [CrossRef]
- Cox, R.; Molineux, M.; Kendall, M.; Tanner, B.; Miller, E. Co-produced capability framework for successful patient and staff partnerships in healthcare quality improvement: Results of a scoping review. BMJ Qual. Saf. 2022, 31, 134–146. [Google Scholar] [CrossRef] [PubMed]
- Majid, U.; Gagliardi, A. Clarifying the degrees, modes, and muddles of “meaningful” patient engagement in health services planning and designing. Patient Educ. Couns. 2019, 102, 1581–1589. [Google Scholar] [CrossRef] [PubMed]
- Tessema, G.A.; Kinfu, Y.; Dachew, B.A.; Tesema, A.G.; Assefa, Y.; Alene, K.A.; Aregay, A.F.; Ayalew, M.B.; Bezabhe, W.M.; Bali, A.G.; et al. The COVID-19 pandemic and healthcare systems in Africa: A scoping review of preparedness, impact and response. BMJ Glob. Health 2021, 6, e007179. [Google Scholar] [CrossRef] [PubMed]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’brien, K.; Colquhoun, H.; Kastner, M.; Levac, D.; NG, C.; Sharpe, J.P.; Wilson, K. A scoping review on the conduct and reporting of scoping reviews. BMC Med. Res. Methodol. 2016, 16, 15. [Google Scholar] [CrossRef]
- Bemelmans, M.; van den Akker, T.; Ford, N.; Philips, M.; Zachariah, R.; Harries, A.; Schouten, E.; Hermann, K.; Mwagomba, B.; Massaquoi, M. Providing universal access to antiretroviral therapy in Thyolo, Malawi through task shifting and decentralization of HIV/AIDS care. Trop. Med. Int. Health 2010, 15, 1413–1420. [Google Scholar] [CrossRef] [PubMed]
- De Wet, K.; Wouters, E.; Engelbrecht, M. Exploring task-shifting practices in antiretroviral treatment facilities in the Free State Province, South Africa. J. Public Health Policy 2011, 32, S94–S101. [Google Scholar] [CrossRef] [PubMed]
- Ledikwe, J.H.; Kejelepula, M.; Maupo, K.; Sebetso, S.; Thekiso, M.; Smith, M.; Mbayi, B.; Houghton, N.; Thankane, K.; O’Malley, G. Evaluation of a well-established task-shifting initiative: The lay counselor cadre in Botswana. PLoS ONE 2013, 8, e61601. [Google Scholar] [CrossRef]
- Baine, S.O.; Kasangaki, A. A scoping study on task shifting, the case of Uganda. BMC Health Serv. Res. 2014, 14, 184. [Google Scholar] [CrossRef]
- Mwangala, S.; Moland, K.M.; Nkamba, H.C.; Usonda, K.G.; Monze, M.; Musukwa, K.K.; Fylkesnes, K. Task-shifting and quality of HIV testing services: Experiences from a national reference hospital in Zambia. PLoS ONE 2015, 10, e0143075. [Google Scholar] [CrossRef]
- Chamberlain, S.; Stolz, U.; Dreifuss, B.; Elson, S.W.; Hammerstedt, H.; Andinda, J.; Maling, S.; Bisanzo, M. Mortality related to acute illness and injury in rural Uganda: Task shifting to improve outcomes. PLoS ONE 2015, 10, e0122559. [Google Scholar] [CrossRef]
- Charyeva, Z.; Oguntunde, O.; Orobaton, N.; Otolorin, E.; Inuwa, F.; Alalade, O.; Abegunde, D. Task shifting provision of contraceptive implants to community health extension workers: Results of operations research in northern Nigeria. Glob. Health Sci. Pract. 2015, 3, 382–394. [Google Scholar] [CrossRef]
- Landes, M.; Thompson, C.; Mwinjiwa, E.; Thaulo, E.; Gondwe, C.; Akello, H.; Chan, A.K. Task shifting of triage to peer expert informal care providers at a tertiary referral HIV clinic in Malawi: A cross-sectional operational evaluation. BMC Health Serv. Res. 2017, 17, 341. [Google Scholar] [CrossRef] [PubMed]
- Okyere, E.; Mwanri, L.; Ward, P. Is task-shifting a solution to the health workers’ shortage in Northern Ghana? PLoS ONE 2017, 12, e0174631. [Google Scholar] [CrossRef]
- Lulebo, A.M.; Kaba, D.K.; Atake, S.E.-H.; Mapatano, M.A.; Mafuta, E.M.; Mampunza, J.M.; Coppieters, Y. Task shifting in the management of hypertension in Kinshasa, Democratic Republic of Congo: A cross-sectional study. BMC Health Serv. Res. 2017, 17, 67–73. [Google Scholar] [CrossRef] [PubMed]
- Naikoba, S.; Senjovu, K.D.; Mugabe, P.; Mccarthy, C.F.; Riley, P.L.; Kadengye, D.T.; Dalal, S. Improved HIV and TB knowledge and competence among mid-level providers in a cluster-randomized trial of one-on-one mentorship for task shifting. JAIDS J. Acquir. Immune Defic. Syndr. 2017, 75, e120–e127. [Google Scholar] [CrossRef]
- Millogo, T.; Kouanda, S.; Tran, N.T.; Kaboré, B.; Keita, N.; Ouedraogo, L.; Tall, F.; Kiarie, J.; Thatte, N.; Festin, M. Task sharing for family planning services, Burkina Faso. Bull. World Health Organ. 2019, 97, 783. [Google Scholar] [CrossRef] [PubMed]
- Gbagbo, F.; Morhe, E. Increasing access to intrauterine contraceptive device uptake in Ghana: Stakeholders views on task sharing service delivery with community health nurses. Ghana Med. J. 2020, 54, 114–120. [Google Scholar] [CrossRef] [PubMed]
- Peresu, E.; Heunis, J.C.; Kigozi, N.G.; De Graeve, D. Task-shifting directly observed treatment and multidrug-resistant tuberculosis injection administration to lay health workers: Stakeholder perceptions in rural Eswatini. Hum. Resour. Health 2020, 18, 1–12. [Google Scholar] [CrossRef]
- Lund, C.; Schneider, M.; Garman, E.C.; Avies, T.; Munodawafa, M.; Honikman, S.; Bhana, A.; Bass, J.; Bolton, P.; Dewey, M. Task-sharing of psychological treatment for antenatal depression in Khayelitsha, South Africa: Effects on antenatal and postnatal outcomes in an individual randomised controlled trial. Behav. Res. Ther. 2020, 130, 103466. [Google Scholar] [CrossRef]
- Sevene, E.; Boene, H.; Vidler, M.; Valá, A.; Macuacua, S.; Augusto, O.; Fernandes, Q.; Bique, C.; Macete, E.; Sidat, M. Feasibility of task-sharing with community health workers for the identification, emergency management and referral of women with pre-eclampsia, in Mozambique. Reprod. Health 2021, 18, 145. [Google Scholar] [CrossRef]
- Boullé, C.; Kouanfack, C.; Laborde-Balen, G.; Carrieri, M.P.; Dontsop, M.; Boyer, S.; Aghokeng, A.F.; Spire, B.; Koulla-Shiro, S.; Delaporte, E. Task shifting HIV care in rural district hospitals in Cameroon: Evidence of comparable antiretroviral treatment-related outcomes between nurses and physicians in the Stratall ANRS/ESTHER trial. J. Acquir. Immune Defic. Syndr. 2013, 62, 569–576. [Google Scholar] [CrossRef]
- Paul, M.; Gemzell-Danielsson, K.; Kiggundu, C.; Kiggundu, C.; Namugenyi, R.; Klingberg-Allvin, M. Barriers and facilitators in the provision of post-abortion care at district level in central Uganda–a qualitative study focusing on task sharing between physicians and midwives. BMC Health Serv. Res. 2014, 14, 28. [Google Scholar] [CrossRef] [PubMed]
- O’Malley, G.; Asrat, L.; Sharma, A.; Hamunime, N.; Stephanus, Y.; Brandt, L.; Ali, D.; Kaindjee-Tjituka, F.; Natanael, S.; Gweshe, J. Nurse task shifting for antiretroviral treatment services in Namibia: Implementation research to move evidence into action. PLoS ONE 2014, 9, e92014. [Google Scholar] [CrossRef] [PubMed]
- Suzan-Monti, M.; Blanche, J.; Boyer, S.; Kouanfack, C.; Delaporte, E.; Bonono, R.C.; Carrieri, P.; Protopopescu, C.; Laurent, C.; Spire, B. Benefits of task-shifting HIV care to nurses in terms of health-related quality of life in patients initiating antiretroviral therapy in rural district hospitals in C ameroon [Stratall Agence Nationale de Recherche sur le SIDA (ANRS) 12110/Ensemble pour une Solidarité Thérapeutique Hospitalière en Réseau (ESTHER) substudy]. HIV Med. 2015, 16, 307–318. [Google Scholar] [PubMed]
- Farley, J.E.; Ndjeka, N.; Kelly, A.M.; Whitehouse, E.; Lachman, S.; Budhathoki, C.; Lowensen, K.; Bergren, E.; Mabuza, H.; Mlandu, N. Evaluation of a nurse practitioner-physician task-sharing model for multidrug-resistant tuberculosis in South Africa. PLoS ONE 2017, 12, e0182780. [Google Scholar] [CrossRef]
- Tariku, Y.; Gerum, T.; Mekonen, M.; Takele, H. Surgical task shifting helps reduce neonatal mortality in Ethiopia: A retrospective cohort study. Surg. Res. Pract. 2019, 2019, 5367068. [Google Scholar] [CrossRef]
- Tweya, H.; Feldacker, C.; Ben-Smith, A.; Eigel, R.; Boxshall, M.; Phiri, S.; Jahn, A. ‘Task shifting’ in an antiretroviral clinic in Malawi: Can health surveillance assistants manage patients safely? Public Health Action 2012, 2, 178–180. [Google Scholar] [CrossRef]
- Some, D.; Edwards, J.K.; Reid, T.; Van Den Bergh, R.; Kosgei, R.J.; Wilkinson, E.; Baruani, B.; Kizito, W.; Khabala, K.; Shah, S. Task shifting the management of non-communicable diseases to nurses in Kibera, Kenya: Does it work? PLoS ONE 2016, 11, e0145634. [Google Scholar] [CrossRef]
- Davis, D.N.; Lemani, C.; Kamtuwanje, N.; Phiri, B.; Masepuka, P.; Kuchawo, S.; Bhushan, N.L.; Tang, J.H. Task shifting levonorgestrel implant insertion to community midwife assistants in Malawi: Results from a non-inferiority evaluation. Contracept. Reprod. Med. 2018, 3, 24. [Google Scholar] [CrossRef]
- Galukande, M.; Kaggwa, S.; Sekimpi, P.; Kakaire, O.; Katamba, A.; Munabi, I.; Runumi, F.M.; Mills, E.; Hagopian, A.; Blair, G. Use of surgical task shifting to scale up essential surgical services: A feasibility analysis at facility level in Uganda. BMC Health Serv. Res. 2013, 13, 292. [Google Scholar] [CrossRef]
- Bolkan, H.A.; Van Duinen, A.; Waalewijn, B.; Elhassein, M.; Kamara, T.; Deen, G.; Bundu, I.; Ystgaard, B.; Von Schreeb, J.; Wibe, A. Safety, productivity and predicted contribution of a surgical task-sharing programme in Sierra Leone. J. Br. Surg. 2017, 104, 1315–1326. [Google Scholar] [CrossRef]
- Wiedenmayer, K.A.; Kapologwe, N.; Charles, J.; Chilunda, F.; Mapunjo, S. The reality of task shifting in medicines management-a case study from Tanzania. J. Pharm. Policy Pract. 2015, 8, 13. [Google Scholar] [CrossRef] [PubMed]
- Agyapong, V.I.; Osei, A.; Farren, C.K.; Mcauliffe, E. Task shifting–Ghana’s community mental health workers’ experiences and perceptions of their roles and scope of practice. Glob. Health Action 2015, 8, 28955. [Google Scholar] [CrossRef]
- Dos Santos, P.F.; Wainberg, M.L.; Caldas-de-Almeida, J.M.; Saraceno, B.; Mari, J.D.J. Overview of the mental health system in Mozambique: Addressing the treatment gap with a task-shifting strategy in primary care. Int. J. Ment. Health Syst. 2016, 10, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Agyapong, V.I.O.; Farren, C.; McAuliffe, E. Improving Ghana’s mental healthcare through task-shifting-psychiatrists and health policy directors perceptions about government’s commitment and the role of community mental health workers. Glob. Health 2016, 12, 57. [Google Scholar] [CrossRef]
- Agyapong, V.I.; Osei, A.; Mcloughlin, D.M.; Mcauliffe, E. Task shifting—Perception of stake holders about adequacy of training and supervision for community mental health workers in Ghana. Health Policy Plan. 2016, 31, 645–655. [Google Scholar] [CrossRef]
- Sayed, S.; Field, A.; Rajab, J.; Mutuiri, A.; Githanga, J.; Mungania, M.; Okinda, N.; Moloo, Z.; Abdillah, A.; Ayara, B. Task sharing and shifting to provide pathology diagnostic services: The Kenya fine-needle aspiration biopsy cytology and bone marrow aspiration and trephine biopsy training program. J. Glob. Oncol. 2018, 4, 1–11. [Google Scholar] [CrossRef]
- Gessessew, A.; Barnabas, G.A.; Prata, N.; Weidert, K. Task shifting and sharing in Tigray, Ethiopia, to achieve comprehensive emergency obstetric care. Int. J. Gynaecol. Obs. 2011, 113, 28–31. [Google Scholar] [CrossRef]
- Awolude, O.A.; Oyerinde, S.O.; Akinyemi, J.O. Screen and triage by community extension workers to facilitate screen and treat: Task-sharing strategy to achieve universal coverage for cervical cancer screening in Nigeria. J. Glob. Oncol. 2018, 4, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Dambisya, Y.M.; Matinhure, S. Policy and programmatic implications of task shifting in Uganda: A case study. BMC Health Serv. Res. 2012, 12, 61. [Google Scholar] [CrossRef]
- Kiweewa, F.M.; Wabwire, D.; Nakibuuka, J.; Mubiru, M.; Bagenda, D.; Musoke, P.; Fowler, M.G.; Antelman, G. Noninferiority of a task-shifting HIV care and treatment model using peer counselors and nurses among Ugandan women initiated on ART: Evidence from a randomized trial. J. Acquir. Immune Defic. Syndr. 2013, 63, e125–e132. [Google Scholar] [CrossRef]
- Jennings, L.; Yebadokpo, A.S.; Affo, J.; Agbogbe, M.; Tankoano, A. Task shifting in maternal and newborn care: A non-inferiority study examining delegation of antenatal counseling to lay nurse aides supported by job aids in Benin. Implement Sci. 2011, 6, 2. [Google Scholar] [CrossRef] [PubMed]
- Kosgei, R.J.; Wools-Kaloustian, K.K.; Braitstein, P.; Sidle, J.; Sang, E.; Gitau, J.; Sitienei, J.; Owino, R.; Mamlin, J.; Kimaiyo, S. Task shifting in HIV clinics, Western Kenya. East Afr. Med. J. 2010, 87, 299–303. [Google Scholar] [PubMed]
- Umar, N.A.; Hajara, M.J.; Khalifa, M. Reduction of client waiting time using task shifting in an anti-retroviral clinic at Specialist Hospital Bauchi, Nigeria. J. Public Health Afr. 2011, 2, e2. [Google Scholar] [CrossRef] [PubMed]
- Born, L.J.; Wamulume, C.; Neroda, K.A.; Quiterio, N.; Giganti, M.J.; Morris, M.; Bolton-Moore, C.; Baird, S.; Sinkamba, M.; Topp, S.M.; et al. Evaluation of a Task-Shifting Strategy Involving Peer Educators in HIV Care and Treatment Clinics in Lusaka, Zambia. J. Public Health Afr. 2012, 3, e3. [Google Scholar] [CrossRef]
- Naburi, H.; Ekström, A.M.; Mujinja, P.; Kilewo, C.; Manji, K.; Biberfeld, G.; Sando, D.; Chalamila, G.; Bärnighausen, T. The potential of task-shifting in scaling up services for prevention of mother-to-child transmission of HIV: A time and motion study in Dar es Salaam, Tanzania. Hum. Resour. Health 2017, 15, 35. [Google Scholar] [CrossRef]
- Marotta, C.; Giaquinto, C.; Di Gennaro, F.; Chhaganlal, K.D.; Saracino, A.; Moiane, J.; Maringhini, G.; Pizzol, D.; Putoto, G.; Monno, L. Pathways of care for HIV infected children in Beira, Mozambique: Pre-post intervention study to assess impact of task shifting. BMC Public Health 2018, 18, 703. [Google Scholar] [CrossRef]
- Labhardt, N.D.; Balo, J.R.; Ndam, M.; Grimm, J.J.; Manga, E. Task shifting to non-physician clinicians for integrated management of hypertension and diabetes in rural Cameroon: A programme assessment at two years. BMC Health Serv. Res. 2010, 10, 339. [Google Scholar] [CrossRef]
- Hoke, T.H.; Wheeler, S.B.; Lynd, K.; Green, M.S.; Razafindravony, B.H.; Rasamihajamanana, E.; Blumenthal, P.D. Community-based provision of injectable contraceptives in Madagascar: ‘task shifting’ to expand access to injectable contraceptives. Health Policy Plan 2012, 27, 52–59. [Google Scholar] [CrossRef]
- Wright, J.; Chiwandira, C. Building capacity for community mental health care in rural Malawi: Findings from a district-wide task-sharing intervention with village-based health workers. Int. J. Soc. Psychiatry 2016, 62, 589–596. [Google Scholar] [CrossRef]
- Gyamfi, J.; Plange-Rhule, J.; Iwelunmor, J.; Lee, D.; Blackstone, S.R.; Mitchell, A.; Ntim, M.; Apusiga, K.; Tayo, B.; Yeboah-Awudzi, K. Training nurses in task-shifting strategies for the management and control of hypertension in Ghana: A mixed-methods study. BMC Health Serv. Res. 2017, 17, 104. [Google Scholar]
- Tilahun, Y.; Lew, C.; Belayihun, B.; Hagos, K.L.; Asnake, M. Improving contraceptive access, use, and method mix by task sharing Implanon insertion to frontline health workers: The experience of the Integrated Family Health Program in Ethiopia. Glob. Health Sci. Pract. 2017, 5, 592–602. [Google Scholar] [CrossRef]
- Gueye, B.; Wesson, J.; Koumtingue, D.; Stratton, S.; Viadro, C.; Talla, H.; Dioh, E.; Cissé, C.; Sebikali, B.; Daff, B.M. Mentoring, task sharing, and community outreach through the TutoratPlus approach: Increasing use of long-acting reversible contraceptives in Senegal. Glob. Health Sci. Pract. 2016, 4, S33–S43. [Google Scholar] [CrossRef]
- Mafigiri, D.K.; McGrath, J.W.; Whalen, C.C. Task shifting for tuberculosis control: A qualitative study of community-based directly observed therapy in urban Uganda. Glob. Public Health 2012, 7, 270–284. [Google Scholar] [CrossRef]
- Dlamini-Simelane, T.; Moyer, E. Task shifting or shifting care practices? The impact of task shifting on patients’ experiences and health care arrangements in Swaziland. BMC Health Serv. Res. 2017, 17, 20. [Google Scholar] [CrossRef]
- Kaindjee-Tjituka, F.; Sawadogo, S.; Lowrance, D.; Maher, A.; Salomo, N.; Mutandi, G.; Mbapaha, C.; Neo, M.; Beukes, A.; Gweshe, J. Task-shifting point-of-care CD4+ testing to lay health workers in HIV care and treatment services in Namibia. Afr. J. Lab. Med. 2017, 6, 1–5. [Google Scholar] [CrossRef]
- Wall, J.T.; Kaiser, B.N.; Friis-Healy, E.A.; Ayuku, D.; Puffer, E.S. What about lay counselors’ experiences of task-shifting mental health interventions? Example from a family-based intervention in Kenya. Int. J. Ment. Health Syst. 2020, 14, 1–14. [Google Scholar] [CrossRef]
- Andriamanjato, H.H.; Mathenge, W.; Kalua, K.; Courtright, P.; Lewallen, S. Task shifting in primary eye care: How sensitive and specific are common signs and symptoms to predict conditions requiring referral to specialist eye personnel? Hum. Resour. Health 2014, 12, S3. [Google Scholar] [CrossRef] [PubMed]
- Eliah, E.; Lewallen, S.; Kalua, K.; Courtright, P.; Gichangi, M.; Bassett, K. Task shifting for cataract surgery in eastern Africa: Productivity and attrition of non-physician cataract surgeons in Kenya, Malawi and Tanzania. Hum. Resour. Health 2014, 12, S4. [Google Scholar] [CrossRef]
- Akeju, D.O.; Vidler, M.; Sotunsa, J.; Osiberu, M.; Orenuga, E.; Oladapo, O.T.; Adepoju, A.; Qureshi, R.; Sawchuck, D.; Adetoro, O.O. Human resource constraints and the prospect of task-sharing among community health workers for the detection of early signs of pre-eclampsia in Ogun State, Nigeria. Reprod. Health 2016, 13, 115–122. [Google Scholar] [CrossRef] [PubMed]
- Asfaw, E.; Dominis, S.; Palen, J.G.; Wong, W.; Bekele, A.; Kebede, A.; Johns, B. Patient satisfaction with task shifting of antiretroviral services in Ethiopia: Implications for universal health coverage. Health Policy Plan. 2014, 29, ii50–ii58. [Google Scholar] [CrossRef] [PubMed]
- Yator, O.; Kagoya, M.; Khasakhala, L.; John-Stewart, G.; Kumar, M. Task-sharing and piloting WHO group interpersonal psychotherapy (IPT-G) for adolescent mothers living with HIV in Nairobi primary health care centers: A process paper. AIDS Care 2021, 33, 873–878. [Google Scholar] [CrossRef] [PubMed]
- Selke, H.M.; Kimaiyo, S.; Sidle, J.E.; Vedanthan, R.; Tierney, W.M.; Shen, C.; Denski, C.D.; Katschke, A.R.; Wools-Kaloustian, K. Task-shifting of antiretroviral delivery from health care workers to persons living with HIV/AIDS: Clinical outcomes of a community-based program in Kenya. J. Acquir. Immune Defic. Syndr. 2010, 55, 483–490. [Google Scholar] [CrossRef] [PubMed]
- Chibanda, D.; Mesu, P.; Kajawu, L.; Cowan, F.; Araya, R.; Abas, M.A. Problem-solving therapy for depression and common mental disorders in Zimbabwe: Piloting a task-shifting primary mental health care intervention in a population with a high prevalence of people living with HIV. BMC Public Health 2011, 11, 828. [Google Scholar] [CrossRef] [PubMed]
- Jacobs, Y.; Myers, B.; van der Westhuizen, C.; Brooke-Sumner, C.; Sorsdahl, K. Task sharing or task dumping: Counsellors experiences of delivering a psychosocial intervention for mental health problems in South Africa. Community Ment. Health J. 2021, 57, 1082–1093. [Google Scholar] [CrossRef] [PubMed]
- Boniol, M.; Kunjumen, T.; Nair, T.S.; Siyam, A.; Campbell, J.; Diallo, K. The global health workforce stock and distribution in 2020 and 2030: A threat to equity and ‘universal’health coverage? BMJ Glob. Health 2022, 7, e009316. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Health Workforce Requirements for Universal Health Coverage and the Sustainable Development Goals; Human Resources for Health Observer, 17; World Health Organization: Geneva, Switzerland, 2016.
- World Health Organization. WHO Guideline on Health Workforce Development, Attraction, Recruitment and Retention in Rural and Remote Areas: Web Annexes; World Health Organization: Geneva, Switzerland, 2021.
- Malakoane, B.; Heunis, J.C.; Chikobvu, P.; Kigozi, N.G.; Kruger, W.H. Public health system challenges in the Free State, South Africa: A situation appraisal to inform health system strengthening. BMC Health Serv. Res. 2020, 20, 58. [Google Scholar] [CrossRef] [PubMed]
- Ahmat, A.; Okoroafor, S.C.; Kazanga, I.; Asamani, J.A.; Millogo, J.J.S.; Illou, M.M.A.; Mwinga, K.; Nyoni, J. The health workforce status in the WHO African Region: Findings of a cross-sectional study. BMJ Glob. Health 2022, 7, e008317. [Google Scholar] [CrossRef]
- Okoroafor, S.; Ahmat, A.; Osubor, M.; Nyoni, J.; Bassey, J.; Alemu, W. Assessing the staffing needs for primary health care centers in Cross River State, Nigeria: A workload indicators of staffing needs study. Hum. Resour. Health 2022, 19, 108. [Google Scholar] [CrossRef]
- World Health Organization. Workload Indicators of Staffing Need; User’s Manual; World Health Organization: Geneva, Switzerland, 2010.
- Mudie, K.; Jin, M.M.; Kendall, L.; Addo, J.; Dos-Santos-Silva, I.; Quint, J.; Smeeth, L.; Cook, S.; Nitsch, D.; Natamba, B. Non-communicable diseases in sub-Saharan Africa: A scoping review of large cohort studies. J. Glob. Health 2019, 9, 020409. [Google Scholar] [CrossRef]
- Vos, T.; Lim, S.S.; Abbafati, C.; Abbas, K.M.; Abbasi, M.; Abbasifard, M.; Abbasi-Kangevari, M.; Abbastabar, H.; Abd-Allah, F.; Abdelalim, A. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1204–1222. [Google Scholar] [CrossRef]
- Nuzzo, J.B.; Meyer, D.; Snyder, M.; Ravi, S.J.; Lapascu, A.; Souleles, J.; Andrada, C.I.; Bishai, D. What makes health systems resilient against infectious disease outbreaks and natural hazards? Results from a scoping review. BMC Public Health 2019, 19, 1310. [Google Scholar]
- World Health Organization. The African Regional Framework for the Implementation of the Global Strategy on Human Resources for Health: Workforce 2030; World Health Organization: Geneva, Switzerland, 2020.

| Criteria | Component(s) | Explanation |
|---|---|---|
| Population (P) | Population Health workforce | Everyone accessing health services. Healthcare workers such as physicians, nurses, midwives, and community health workers that are working as frontline contact in the healthcare system. |
| Concept (C) | Rationale Scope | Usual reasons or the logical explanations for task shifting and task sharing. Extent or range of services that are task-shifted or -shared amongst various categories of health workers. |
| Context (C) | Healthcare services African countries | Healthcare services within essential service packages that are either sought or received by the population at any healthcare service delivery level in both public and private sectors. Any country within the African continent. |
| Source of Literature | Task Shifting/Sharing Terms | Health System/Services Terms | Africa Terms |
|---|---|---|---|
| PubMed | “task shifting” [Title/Abstract] OR “task sharing” [Title/Abstract] AND (“Africa”) [Mesh] | “health system*” [tiab] OR “healthcare system*” [tiab] OR “health care system*” [tiab] OR “healthcare sector*” [tiab] OR “healthcare industr*” [tiab] OR “health industr*” [tiab] OR “health facilit*” [tiab] OR “hospital*” [tiab] OR “healthcare” [tiab] OR “health care” [tiab] OR “health service*” [tiab] OR “healthcare service*” [tiab] OR “health cent*” [tiab] OR “care, health” [tiab] OR “system, health care” [tiab] OR “systems, health care” [tiab] OR “system, healthcare” [tiab] | Africa*[tiab] OR Algeria*[tiab] OR Angola*[tiab] OR Benin*[tiab] OR Botswana*[tiab] OR Burkina Faso [tiab] OR Burundi*[tiab] OR Cape Verde*[tiab] OR Cabo Verde [tiab] OR Cameron*[tiab] OR Cameroon*[tiab] OR Chad*[tiab] OR Comoros*[tiab] OR Congo*[tiab] OR Cote d’Ivoire[tiab] OR Ivory coast [tiab] OR Djibouti*[tiab] OR Egypt*[tiab] OR Eritrea*[tiab] OR Ethiopia*[tiab] OR Gabon*[tiab] OR Gambia*[tiab] OR Ghana*[tiab] OR Guinea*[tiab] OR Kenya*[tiab] OR Lesotho*[tiab] OR Liberia*[tiab] OR Libya*[tiab] OR Madagascar*[tiab] OR Malawi*[tiab] OR Mali*[tiab] OR Maurit*[tiab] OR Morocc*[tiab] OR Mozambiqu*[tiab] OR Namibia*[tiab] OR Niger*[tiab] OR Rwanda*[tiab] OR Senegal*[tiab] OR Seychelles[tiab] OR Sierra Leone*[tiab] OR Somalia*[tiab] OR South Africa*[tiab] OR Sudan*[tiab] OR Swaziland*[tiab] OR Tanzania*[tiab] OR Togo*[tiab] OR Tunisia*[tiab] OR Uganda*[tiab] OR Zambia*[tiab] OR Zimbabwe*[tiab] |
| CINHAL | TI “task shifting” OR AB “task shifting” OR TI “task sharing” OR AB “task sharing” OR MH “task shifting” OR MH “task sharing” | TI” health system*” OR AB “health system*” OR TI” healthcare system*” OR AB” healthcare system*” OR TI” health care system*” OR AB” health care system*” OR TI” healthcare sector*” OR AB” healthcare sector*” OR TI” health facilit*” OR AB” health facilit*” OR TI “hospital*” OR AB “hospital*” OR TI” healthcare” OR AB” healthcare” OR TI “health care” OR AB “health care” OR TI” health service*” OR AB” health service*” OR TI” healthcare service*” OR AB” healthcare service*” OR TI” health cent*” OR AB” health cent*” OR TI” care, health” OR AB” care, health” OR TI “system, health care” OR AB “system, health care” OR TI “systems, health care” OR AB “systems, health care” OR TI “system, healthcare” OR TI “system, healthcare” | MH Africa OR TI Africa* OR AB Africa* OR TI Algeria* OR AB Algeria* OR TI Angola*OR AB Angola* OR TI Benin*OR AB Benin* OR TI Botswana* OR AB Botswana OR TI “Burkina Faso*” OR AB “Burkina Faso*” OR TI Burundi* OR AB Burundi* OR TI “Cape Verde*” OR AB “Cape Verde*” OR TI Cameron* OR AB Cameron*OR TI Cameroon*OR AB Cameroon* OR TI Chad* OR AB chad* OR TI Comoros* OR AB Comoros* OR TI Congo* OR AB Congo* OR TI “Cote d’Ivoire” OR AB “Cote d’Ivoire” OR TI “Ivory coast” OR AB “Ivory coast” OR TI Djibouti* OR AB Djibouti* OR TI Egypt* OR AB Egypt* OR TI Eritrea* OR AB Eritrea* OR TI Ethiopia* OR AB Ethiopia* OR TI Gabon* OR AB Gabon* OR TI Gambia*OR AB Gambia* OR TI Ghana* OR AB Ghana OR TI Guinea* OR AB Guinea* OR TI Kenya* OR AB Kenya* OR TI Lesotho* OR Lesotho* OR TI Liberia* OR AB Liberia OR TI Libya* AB Libya* OR TI Madagascar* OR AB Madagascar* OR TI Malawi* OR AB Malawi* OR TI Mali* OR AB Mali* OR TI Maurit* OR AB Maurit* OR TI Morocc* OR AB Morocc* OR TI Mozambiqu* OR AB Mozambiqu* OR TI Namibia* OR AB Namibia* OR TI Niger* OR AB Niger* OR TI Rwanda* OR AB Rwanda* OR TI Senegal* OR AB Senegal* OR TI Seychelles* OR TI Seychelles* OR TI “Sierra Leone*” OR AB “Sierra Leone*” OR TI Somalia* OR AB Somalia” OR TI South Africa* OR AB South Africa* OR TI Sudan* OR AB Sudan* OR TI Swaziland* OR AB Swaziland* OR TI Tanzania* OR AB Tanzania* OR TI Togo* OR AB Togo* OR TI Tunisia* OR AB Tunisia OR TI Uganda* OR AB Uganda* OR TI Zambia* OR TI Zambia* OR TI Zimbabwe* OR AB Zimbabwe* |
| Scopus | “task shifting” OR “task sharing” | “health system*” OR “healthcare system*” [tiab] OR “health care system*” OR “healthcare sector*” OR “healthcare industr*” OR “health industr*” OR “health facilit*” OR “hospital*” OR “healthcare” OR “health care” OR “health service*” OR “healthcare service*” OR “health cent*” OR “care, health” OR “system, health care” OR “systems, health care” OR “system, healthcare” | TITLE-ABS-KEY (“Africa” OR “Algeria*” OR “Angola*” OR “Benin*” OR “Botswana*” OR “Burkina Faso” OR “Burundi*” OR “Cape Verde*” OR “Cabo Verde” OR “Cameron*” OR “Cameroon*” OR “Chad*” OR “Comoros*” OR “Congo*” OR “Cote d’Ivoire” OR “Ivory coast” OR “Djibou*” OR “Egypt*” OR “Eritrea*” OR “Ethiopia*” OR “Gabon*” OR “Gambia*” OR “Ghana*” OR “Guinea*” OR “Kenya*” OR “Lesotho*” OR “Liberia*” OR “Libya*” OR “Madagascar*” OR “Malawi*” OR “Mali*” OR “Maurit*” OR “Morocc*” OR “Mozambiqu*” OR “Namibia*” OR “Niger*” OR “Rwanda*” OR “Senegal*” OR “Seychelles” OR “Sierra Leone*” OR “Somalia*” OR “South Africa*” OR “Sudan*” OR “Swaziland*” OR “Tanzania*” OR “Togo*” OR “Tunisia*” OR “Uganda*” OR “Zambia*” OR “Zimbabwe*”) |
| Paper Characteristics | Categories | Results | |
|---|---|---|---|
| n | % | ||
| Year of publication | 2010 | 4 | 7 |
| 2011 | 5 | 8 | |
| 2012 | 5 | 8 | |
| 2013 | 4 | 7 | |
| 2014 | 6 | 10 | |
| 2015 | 6 | 10 | |
| 2016 | 7 | 11 | |
| 2017 | 11 | 18 | |
| 2018 | 4 | 7 | |
| 2019 | 2 | 3 | |
| 2020 | 4 | 7 | |
| 2021 | 3 | 5 | |
| Country of study | Benin | 1 | 2 |
| Botswana | 1 | 2 | |
| Burkina Faso | 1 | 2 | |
| Cameroon | 3 | 5 | |
| Democratic Republic of the Congo | 1 | 2 | |
| Eswatini | 1 | 2 | |
| Ethiopia | 4 | 7 | |
| Ghana | 6 | 10 | |
| Kenya | 6 | 10 | |
| Madagascar | 1 | 2 | |
| Malawi | 5 | 8 | |
| Mozambique | 3 | 5 | |
| Namibia | 2 | 3 | |
| Nigeria | 4 | 7 | |
| Senegal | 1 | 2 | |
| Sierra Leone | 1 | 2 | |
| South Africa | 4 | 7 | |
| Swaziland | 1 | 2 | |
| Tanzania | 2 | 3 | |
| Uganda | 8 | 13 | |
| Zambia | 2 | 3 | |
| Zimbabwe | 1 | 2 | |
| Multi-country | 2 | 3 | |
| Type of article | Original research | 61 | 100 |
| Study design | Quantitative research | 42 | 69 |
| Qualitative research | 10 | 16 | |
| Mixed methods | 9 | 15 | |
| Main focus | Rationale | 1 | 2 |
| Scope | 7 | 11 | |
| Both | 53 | 87 | |
| Level of care | Community care level | 8 | 13 |
| Primary care level | 13 | 21 | |
| Primary and community care level | 15 | 25 | |
| Secondary and primary care level | 7 | 11 | |
| Secondary care level | 13 | 21 | |
| Secondary, primary, and community care level | 2 | 3 | |
| Tertiary care level | 2 | 3 | |
| All levels | 1 | 2 | |
| First Author (Year) | Country | Study Title | Study Design and Population | Study Focus | Level of Care |
|---|---|---|---|---|---|
| Bemelmans 2010 | Malawi | Providing universal access to antiretroviral therapy in Thyolo, Malawi through task shifting and decentralization of HIV⁄AIDS care | Design Cross-sectional study (descriptive) Population: People living with HIV/AIDS Health workers: Nurses to health surveillance assistant (HSA)/lay counsellor, medical doctors, clinical officer, medical assistant, and nurses. | Rationale, Scope | Secondary and primary care level |
| Kosgei 2010 | Kenya | Task shifting in HIV clinics, Western Kenya | Design Cross-sectional study (descriptive) | Rationale, Scope | Primary care level |
| Population: People living with HIV/AIDS | |||||
| Health workers: Nurses and clinical officer. | |||||
| Labhardt 2010 | Cameroon | Task shifting to non-physician clinicians for integrated management of hypertension and diabetes in rural Cameroon: a programme assessment at two years | Design: Cross-sectional study (implementation) | Rationale, Scope | Primary care level |
| Population: People requiring hypertension and diabetes care | |||||
| Health workers: Non-physician clinician (NPC)—nurses | |||||
| Selke 2010 | Kenya | Task-Shifting of antiretroviral delivery from health care workers to persons living with HIV/AIDS: clinical outcomes of a community-based program in Kenya | Design: Prospective cluster-randomized controlled clinical trial Population: People living with HIV/AIDS Health workers: People living with HIV/AIDS (PLWAs) as community care coordinators (CCCs) | Scope | Primary care level |
| De Wet 2011 | South Africa | Exploring task-shifting practices in antiretroviral treatment facilities in the Free State Province, South Africa | Design: Prospective cluster-randomized controlled clinical trial Population: People living with HIV/AIDS Health workers: Nurses and community health workers—‘lay workers’, ‘community care workers’, ‘home-based carers’, ‘directly observed treatment (DOT) supporters’, or ‘lay counselors. | Rationale, Scope | Primary care level |
| Chibanda 2011 | Zimbabwe | Problem-solving therapy for depression and common mental disorders in Zimbabwe: piloting a task-shifting primary mental health care intervention in a population with a high prevalence of people living with HIV | Design: Cross-sectional study (implementation) | Scope | Primary care level |
| Population: General population with a high prevalence of people living with HIV | |||||
| Health workers: Lay workers (health promoters) | |||||
| Gessessew 2011 | Ethiopia | Task shifting and sharing in Tigray, Ethiopia, to achieve comprehensive emergency obstetric care | Design: Cross-sectional study (retrospective review of hospital records) | Scope | Secondary and primary care level |
| Population: Women of reproductive age receiving obstetric care | |||||
| Health workers: Non-physician clinicians (NPCs) | |||||
| Jennings 2011 | Benin | Task shifting in maternal and newborn care: a non-inferiority study examining delegation of antenatal counseling to lay nurse aides supported by job aids in Benin | Design: Non-inferiority quasi-experimental design | Rationale, Scope | Primary care level |
| Population: Women of reproductive age receiving maternal and newborn health service | |||||
| Health workers: Nurse-midwives and lay nurse aides | |||||
| Umar 2011 | Nigeria | Reduction of client waiting time using task shifting in an anti-retroviral clinic at Specialist Hospital Bauchi, Nigeria. | Design: Cross-sectional study (implementation) | Rationale, Scope | Secondary care level |
| Population: People living with HIV/AIDS | |||||
| Health workers: Doctors and nurses | |||||
| Tweya 2012 | Malawi | Task shifting’ in an antiretroviral clinic in Malawi: can health surveillance assistants manage patients safely? | Design: Cross-sectional study (implementation) | Rationale, Scope | Primary care level |
| Population: People living with HIV/AIDS | |||||
| Health workers: Health surveillance assistants (HSAs) | |||||
| Hoke 2012 | Madagascar | Community-based provision of injectable contraceptives in Madagascar: ‘task shifting’ to expand access to injectable contraceptives | Design: Cross-sectional study (implementation) | Rationale, Scope | Community care level |
| Population: Women of reproductive age requiring contraceptives | |||||
| Health workers: Community-based distribution (CBD) agents/community health workers | |||||
| Born 2012 | Zambia | Evaluation of a task-shifting strategy involving peer educators in HIV care and treatment clinics in Lusaka, Zambia | Design: Cross-sectional mixed-methods study | Rationale, Scope | Community care level |
| Population: People living with HIV/AIDS | |||||
| Health workers: Peer educators (PEs). | |||||
| Dambisya 2012 | Uganda | Policy and programmatic implications of task shifting in Uganda: a case study | Design: Cross-sectional, qualitative descriptive study | Rationale, Scope | Secondary, primary, and community care level |
| Population: General population, PLWHA, etc. | |||||
| Health workers: Clinical officers, nurses, midwives, and CHWs | |||||
| Mafigiri 2012 | Uganda | Task shifting for tuberculosis control: A qualitative study of community-based directly observed therapy in urban Uganda | Design Cross-sectional mixed-methods study | Rationale, Scope | Community care level |
| Population: People living receiving TB care | |||||
| Health workers: Laypersons | |||||
| Kiweewa 2013 | Uganda | Noninferiority of a task-shifting HIV care and treatment model using peer counselors and nurses among Ugandan women initiated on ART: evidence from a randomized trial | Design: Prospective randomized intervention trial study | Rationale, Scope | Secondary care level |
| Population: Women on ART | |||||
| Health workers: peer counselors and nurses | |||||
| Boullé 2013 | Cameroon | Task shifting HIV care in rural district hospitals in Cameroon | Design cohort study | Rationale, Scope | Secondary care level |
| Population: People living with HIV/AIDS | |||||
| Health workers: Nurses | |||||
| Ledikwe 2013 | Botswana | Evaluation of a well-established task-shifting initiative: The lay counselor cadre in Botswana | Design: Cross-sectional multi-method study | Rationale, Scope | Primary and community care level |
| Population: People living with HIV/AIDS | |||||
| Health workers: Lay Counselors | |||||
| Galukande 2013 | Uganda | Use of surgical task shifting to scale up essential surgical services: a feasibility analysis at facility level in Uganda | Design: Cross-sectional qualitative study | Rationale, Scope | Secondary care level |
| Population General population | |||||
| Health workers: surgical specialists | |||||
| Baine 2014 | Uganda | A scoping study on task shifting: the case of Uganda | Design: Cross-sectional qualitative study | Rationale, Scope | Secondary, primary, and community care levels |
| Population: General population | |||||
| Health workers: Clinical officers, nurses | |||||
| Asfaw 2014 | Ethiopia | Patient satisfaction with task shifting of antiretroviral services in Ethiopia: implications for universal health coverage | Design: Cross-sectional study | Scope | Secondary and primary care level |
| Population: People living with HIV/AIDS | |||||
| Health workers: Health officers and nurses | |||||
| Paul 2014 | Uganda | Barriers and facilitators in the provision of post-abortion care at district level in central Uganda—a qualitative study focusing on task sharing between physicians and midwives | Design: Cross-sectional qualitative study | Rationale, Scope | Secondary care level |
| Population: Women of reproductive health | |||||
| Health workers: Midwives | |||||
| O’Malley 2014 | Namibia | Nurse task shifting for antiretroviral treatment services in Namibia: implementation research to move evidence into action | Design: Cross-sectional study (implementation) | Rationale, Scope | Secondary and primary care level |
| Population: People living with HIV/AIDS | |||||
| Health workers: Nurses | |||||
| Andriamanjato 2014 | Madagascar, Malawi, and Rwanda | Task shifting in primary eye care: how sensitive and specific are common signs and symptoms to predict conditions requiring referral to specialist eye personnel? | Design: Cross-sectional study (implementation) | Rationale, Scope | Secondary care level |
| Population: General population | |||||
| Health workers: General primary healthcare (PHC) workers—ophthalmic clinical officers | |||||
| Eliah 2014 | Kenya, Malawi, and Tanzania | Task shifting for cataract surgery in eastern Africa: productivity and attrition of non-physician cataract surgeons in Kenya, Malawi, and Tanzania | Design: Cross-sectional study (implementation) | Rationale, Scope | Secondary care level |
| Population: General population | |||||
| Health workers: Non-physician cataract surgeons | |||||
| Wiedenmayer 2015 | Tanzania | The reality of task shifting in medicines management- a case study from Tanzania | Design: Cross-sectional study | Rationale, Scope | Secondary and primary care level |
| Population: General population | |||||
| Health workers: Nurses and medical attendants | |||||
| Mwangala 2015 | Zambia | Task-shifting and quality of HIV testing services: experiences from a National Reference Hospital in Zambia | Design: Cross-sectional qualitative study | Rationale, Scope | Secondary care level |
| Population: General population. | |||||
| Health workers: Lay counselors, nurses, and laboratory personnel | |||||
| Suzan-Monti 2015 | Cameroon | Benefits of task-shifting HIV care to nurses in terms of health-related quality of life in patients initiating antiretroviral therapy in rural district hospitals in Cameroon | Design: Cross-sectional study (implementation) | Rationale, Scope | Secondary care level |
| Population: People living with HIV/AIDS | |||||
| Health workers: Nurses | |||||
| Chamberlain 2015 | Uganda | Mortality related to acute illness and injury in rural Uganda: task shifting to improve outcomes | Design: Cross-sectional study (intervention) | Rationale, Scope | Secondary care level |
| Population: General population | |||||
| Health workers: Nurses | |||||
| Charyeva 2015 | Nigeria | Task shifting provision of contraceptive implants to community health extension workers: results of operations research in northern Nigeria | Design: Cross-sectional study (intervention) | Rationale, Scope | Community care level |
| Population: Women of reproductive age | |||||
| Health workers: Community health extension workers | |||||
| Agyapon 2015 | Ghana | Task shifting Ghana’s community mental health workers’ experiences and perceptions of their roles and scope of practice | Design: Cross-sectional study | Rationale, Scope | Community care level |
| Population: General population | |||||
| Health workers: Community mental health workers—community psychiatric nurses (CPNs), clinical psychiatric officers (CPOs), and community mental health officers (CMHOs) | |||||
| Akeju 2016 | Nigeria | Human resource constraints and the prospect of task-sharing among community health workers for the detection of early signs of pre-eclampsia in Ogun State, Nigeria | Design: Cross-sectional qualitative study | Rationale, Scope | Primary care level |
| Population: Women of reproductive age | |||||
| Health workers: Community health extension workers (CHEW) | |||||
| Wright 2016 | Malawi | Building capacity for community mental health care in rural Malawi: Findings from a district-wide task-sharing intervention with village-based health workers | Design: Cross-sectional study (intervention) | Rationale, Scope | Primary and community care level |
| Population: General population | |||||
| Health workers: Village-based health workers | |||||
| Gueye 2016 | Senegal | Mentoring, task sharing, and community outreach through the TutoratPlus approach: increasing use of long-acting reversible contraceptives in Senegal | Design: Cross-sectional study (intervention) | Rationale, Scope | Primary and community care level |
| Population: Women of reproductive age | |||||
| Health workers: Nurses, non-clinical family planning counselors, and community health workers | |||||
| Dos Santos 2016 | Mozambique | Overview of the mental health system in Mozambique: addressing the treatment gap with a task-shifting strategy in primary care | Design: Cross-sectional study (intervention) | Rationale, Scope | Primary and community care level |
| Population: General population | |||||
| Health workers: Psychiatric technicians | |||||
| Agyapong 2016a | Ghana | Improving Ghana’s mental healthcare through task-shifting psychiatrists’ and health policy directors’ perceptions about government’s commitment and the role of community mental health workers | Design: Cross-sectional study (mixed methods) | Rationale, Scope | Primary and community care level |
| Population: General population | |||||
| Health workers: Community mental health workers—community mental health officers (CMHOs), clinical psychiatric officers (CPOs), and clinical psychiatric nurses (CPNs) | |||||
| Some 2016 | Kenya | Task shifting the management of non-communicable diseases to nurses in Kibera, Kenya: does it work? | Design: Cross-sectional study (descriptive retrospective) | Rationale, Scope | Primary care level |
| Population: General population | |||||
| Health workers: Nurses | |||||
| Agyapong 2016b | Ghana | Task shifting perception of stake holders about adequacy of training and supervision for community mental health workers in Ghana | Design: Cross-sectional study (mixed methods) | Rationale, Scope | Primary and community care level |
| Population: General population | |||||
| Health workers: Community mental health workers—community mental health officers (CMHOs), clinical psychiatric officers (CPOs) and, clinical psychiatric nurses (CPNs) | |||||
| Landes 2017 | Malawi | Task shifting of triage to peer expert informal care providers at a tertiary referral HIV clinic in Malawi: a cross-sectional operational evaluation | Design Cross-sectional study (implementation) | Rationale, Scope | Tertiary care level |
| Population: People living with HIV/AIDS | |||||
| Health workers: Lay health cadre of expert patients (EPs) | |||||
| Okyere 2017 | Ghana | Is task-shifting a solution to the health workers’ shortage in Northern Ghana? | Design: Cross-sectional study (qualitative) | Rationale | All levels |
| Population: General population | |||||
| Health workers: Medical assistants (MA), midwives, general registered nurses (GRN), enrolled nurses (EN), community health officers (CHO), disease control officers (DCO), psychiatric nurses (PN), optometrist, and health nurse aides | |||||
| Tilahun 2017 | Ethiopia | Improving contraceptive access, use, and method mix by task sharing Implanon insertion to frontline health workers: the experience of the integrated family health program in Ethiopia | Design: Cross-sectional study (intervention) | Rationale, Scope | Primary and community care level |
| Population: Women of reproductive age | |||||
| Health workers: Health extension workers | |||||
| Bolkan 2017 | Sierra Leone | Safety, productivity and predicted contribution of a surgical task-sharing programme in Sierra Leone | Design: Prospective observational study | Rationale, Scope | Secondary care level |
| Population: General population | |||||
| Health workers: Associate clinicians/community health officers (CHOs) and junior doctors | |||||
| Farley 2017 | South Africa | Evaluation of a nurse practitioner–physician task-sharing model for multidrug-resistant tuberculosis in South Africa | Design: Prospective cohort study | Rationale, Scope | Secondary care level |
| Population: People with multidrug-resistant tuberculosis | |||||
| Health workers: Clinical nurse practitioner (CNP) and a medical officer (MO) | |||||
| Lulebo 2017 | Democratic Republic of the Congo | Task shifting in the management of hypertension in Kinshasa, Democratic Republic of Congo: a cross-sectional study | Design: Cross-sectional study | Rationale, Scope | Primary care level |
| Population: People with hypertension | |||||
| Health workers: Nurses | |||||
| Gyamfi 2017 | Ghana | Training nurses in task-shifting strategies for the management and control of hypertension in Ghana: a mixed-methods study | Design: Mixed-methods study | Rationale, Scope, | Secondary, and primary care level |
| Population: People with hypertension | |||||
| Health workers: Community health nurses (CHNs) and enrolled nurses (ENs) | |||||
| Dlamini-Simelane 2017 | Swaziland | Task shifting or shifting care practices? The impact of task shifting on patients’ experiences and health care arrangements in Swaziland | Design: Cross-sectional (qualitative—ethnographic) study | Rationale, Scope | Primary and community care level |
| Population: People living with HIV/AIDS | |||||
| Health workers: Lay counsellors and nurses | |||||
| Kaindjee-Tjituka 2017 | Namibia | Task-shifting point-of-care CD4+ testing to lay health workers in HIV care and treatment services in Namibia | Design: Cross-sectional study | Rationale, Scope | Primary and community care level |
| Population: People living with HIV/AIDS | |||||
| Health workers: Lay health workers and nurses | |||||
| Naburi 2017 | Tanzania | The potential of task-shifting in scaling up services for prevention of mother-to-child transmission of HIV: a time and motion study in Dar es Salaam, Tanzania | Design: Cross-sectional study (intervention) | Rationale, Scope | Primary and community care level |
| Population: People living with HIV/AIDS | |||||
| Health workers: Community health workers (CHWs) and nurses | |||||
| Naikoba 2017 | Uganda | Improved HIV and TB knowledge and competence among mid-level providers in a cluster-randomized trial of one-on-one mentorship for task shifting | Design: Cluster-randomized trial | Rationale, Scope | Secondary and primary care level |
| Population: People living with HIV/AIDS | |||||
| Health workers: Mid-level providers (MLPs)—clinical officers, registered nurses, and registered midwives | |||||
| Marotta 2018 | Mozambique | Pathways of care for HIV-infected children in Beira, Mozambique: pre–post intervention study to assess impact of task shifting | Design: Cross-sectional study (intervention) | Rationale, Scope | Primary and community care level |
| Population: People living with HIV/AIDS | |||||
| Health workers: Maternal and child nurses | |||||
| Davis 2018 | Malawi | Task shifting levonorgestrel implant insertion to community midwife assistants in Malawi: results from a non-inferiority evaluation | Design: Cross-sectional study (intervention) | Rationale, Scope | Primary and community care level |
| Population: Women of reproductive age requiring contraceptives | |||||
| Health workers: Community midwife assistants (CMAs) | |||||
| Awolude 2018 | Nigeria | Screen and triage by community extension workers to facilitate screen and treat: task-sharing strategy to achieve universal coverage for cervical cancer screening in Nigeria | Design: Cross-sectional study (intervention) | Rationale, Scope | Primary care level |
| Population: Women of reproductive age | |||||
| Health workers: CHEWs and CHOs | |||||
| Sayed 2018 | Kenya | Task Sharing and shifting to provide pathology diagnostic services: The Kenya fine-needle aspiration biopsy cytology and bone marrow aspiration and trephine biopsy training program | Design: Cross-sectional study (intervention) | Rationale, Scope | Tertiary care level |
| Population: General population | |||||
| Health workers: Pathologists, medical officers (MO), clinical officers (CO), and technologists | |||||
| Millogo 2019 | Burkina Faso | Task sharing for family planning services, Burkina Faso | Design: Cross-sectional study (intervention) | Rationale, Scope | Primary and community care level |
| Population: Women of reproductive age requiring contraceptives | |||||
| Health workers: Community health workers (CHWs), auxiliary nurses, and auxiliary midwives | |||||
| Tariku 2019 | Ethiopia | Surgical task shifting helps reduce neonatal mortality in Ethiopia: A retrospective cohort study | Design: Retrospective cohort study | Rationale, Scope | Secondary care level |
| Population: Women of reproductive age requiring contraceptives | |||||
| Health workers: Non-physician surgeons (NPS) | |||||
| Wall 2020 | Kenya | What about lay counselors’ experiences of task-shifting mental health interventions? Example from a family-based intervention in Kenya | Design: Cross-sectional study (mixed methods) | Scope | Community care level |
| Population: General population | |||||
| Health workers: Lay counselors | |||||
| Gbagbo 2020 | Ghana | Increasing access to intrauterine contraceptive device uptake in Ghana: stakeholders’ views on task sharing service delivery with community health nurses | Design: Cross-sectional qualitative study | Rationale, Scope | Community care level |
| Population: Women of reproductive age requiring contraceptives | |||||
| Health workers: Community health nurses | |||||
| Peresu 2020 | Eswatini | Task-shifting directly observed treatment and multidrug-resistant tuberculosis injection administration to lay health workers: stakeholder perceptions in rural Eswatini | Design: Mixed-methods study—cross-sectional survey and qualitative study | Rationale, Scope | Community care level |
| Population: People with tuberculosis | |||||
| Health workers: Lay health workers (LHWs)/community treatment supporter (CTS) | |||||
| Lund 2020 | South Africa | Task-sharing of psychological treatment for antenatal depression in Khayelitsha, South Africa: Effects on antenatal and postnatal outcomes in an individual randomized controlled trial | Design: Randomized controlled trial | Rationale, Scope | Primary and community care level |
| Population: Women of reproductive age | |||||
| Health workers: Non-specialist community health workers | |||||
| Sevene 2021 | Mozambique | Feasibility of task-sharing with community health workers for the identification, emergency management, and referral of women with pre-eclampsia, in Mozambique | Design: Mixed-methods study | Rationale, Scope | Primary and community care level |
| Population: Pregnant women | |||||
| Health workers: Community health workers | |||||
| Jacobs 2021 | South Africa | Task sharing or task dumping: counsellors experiences of delivering a psychosocial intervention for mental health problems in South Africa | Design: Cross-sectional qualitative study | Scope | Primary care level |
| Population: General population | |||||
| Health workers: Non-specialist—facility-based counsellors (FBCs), specific cadre of community health workers trained to deliver health promotion and HIV adherence counselling services | |||||
| Yator 2021 | Kenya | Task-sharing and piloting WHO group interpersonal psychotherapy (IPT-G) for adolescent mothers living with HIV in Nairobi primary health care centers: a process paper | Design: Cross-sectional study (intervention) | Scope | Primary care level |
| Population: Postpartum adolescent (PPA) mothers living with HIV | |||||
| Health workers: Community health workers (CHWs) |
| Main Theme | Sub-Themes |
|---|---|
| Rationale for task shifting and task sharing | Health worker shortages |
| Optimally utilize existing health workers | |
| Expand access to health services | |
| Scope of shifted and shared tasks | HIV/AIDS care |
| Hypertension management | |
| Diabetes management | |
| Mental health | |
| Maternal and child healthcare | |
| Sexual and reproductive health services | |
| Eye care | |
| Tuberculosis care | |
| Surgical care and procedures | |
| Medicines’ management | |
| Emergency care |
| First Author (Year) | Country | Health Services Context | Key Findings |
|---|---|---|---|
| Bemelmans 2010 | Malawi | Access to HIV⁄AIDS care | Rationale: Staff shortages in the levels of care and by location. Scope: HIV testing and counselling from nurses to health surveillance assistant (HSA)/lay counsellor, antiretroviral therapy (ART) initiations from medical doctors to non-physician clinicians—clinical officer, medical assistant, and nurse |
| Kosgei 2010 | Kenya | Access to HIV⁄AIDS care | Rationale: Scarcity of healthcare providers and the need to improve patient outcomes without increasing clinic human resources. Scope: ART care |
| Labhardt 2010 | Cameroon | Access to care for hypertension and type 2 diabetes care | Rationale: Majority of the rural population does not have access to adequate hypertension and diabetes care. Scope: Hypertension and diabetes care |
| Selke 2010 | Kenya | Access to HIV⁄AIDS care | Scope: Delivery of medications and provision of follow-up care to patients on ART in the community with support of an electronic decision tool, and 3 monthly visits to facilities compared to the usual monthly visit. |
| De Wet 2011 | South Africa | Access to HIV⁄AIDS care | Rationale: Shortage of health workers (physicians and nurses). Scope: Task shifting from nurses to community health workers for HIV treatment and care. HIV counselling, drug readiness training, distribution of nutritional supplements, and capturing and updating electronic information. |
| Chibanda 2011 | Zimbabwe | Access to mental health intervention/services | Scope: Depression and other common mental disorders (CMD)—screening and monitoring CMD and in delivering the intervention |
| Gessessew 2011 | Ethiopia | Access to comprehensive obstetric care | Rationale: Shortage of physicians in rural areas. Scope: Comprehensive emergency obstetric care (CEmOC) |
| Jennings 2011 | Benin | Access to maternal and newborn health services | Rationale: Need to expand the role of lay nurse aides. Scope: Counselling in maternal and newborn care. |
| Umar 2011 | Nigeria | Access to HIV⁄AIDS care | Rationale: Long waiting time of HIV/AIDS patients in the clinic due to the high workload of available doctors. Scope: Consultation for HIV patients presenting for routine refill and follow-up visits |
| Tweya 2012 | Malawi | Access to HIV⁄AIDS care | Rationale: Shortage of clinicians and nurses. Scope Provision of antiretroviral therapy (ART) to stable patients. |
| Hoke 2012 | Madagascar | Access to injectable contraceptives | Rationale Lack of access to health facilities. Scope: Injection (re-injection) and counselling of patients. |
| Born 2012 | Zambia | Access to HIV⁄AIDS care | Rationale: Rapid expansion of antiretroviral therapy (ART) using existing health workers. Scope: Provision of counselling, education talks, and adherence support to patients in HIV care. |
| Dambisya 2012 | Uganda | Access to HIV⁄AIDS care, maternal and child health, general healthcare, etc. | Rationale: Severe health worker shortage and a high demand for healthcare services. Scope: Community health workers (CHW) and PLWHA in care and support of AIDS patients, ophthalmic clinical officers conduct cataract surgery, psychiatric clinical officers cover the same scope as the psychiatrists, but are more community-oriented than the psychiatrists, who tend to be mainly hospital-based. Nurses set IV lines in upcountry due to lack of physicians, midwives conduct manual vacuum extraction, manual removal of the placenta, and manual vacuum aspiration due to shortage of doctors. CHWs and community members involved in delivery of expanded program on immunization (EPI) services, etc. |
| Mafigiri 2012 | Uganda | Access to TB care | Rationale: To address barriers to successful DOTS in rural areas. Scope: Directly observed treatment short course (DOTS) |
| Kiweewa 2013 | Uganda | Access to HIV⁄AIDS care | Rationale Shortage of physicians. Scope: ART follow-up care to postpartum women |
| Boullé 2013 | Cameroon | Access to HIV⁄AIDS care | Rationale Shortage of physicians |
| Ledikwe 2013 | Botswana | Access to HIV⁄AIDS care | Rationale: Shortage of health workers. Scope: HIV tests and related counselling at public health facilities |
| Galukande 2013 | Uganda | Access to surgical services | Rationale: Shortage and maldistribution of surgical specialists. Scope: Emergency and essential surgical care |
| Baine 2014 | Uganda | Access to health services | Rationale: Shortage of health workers in Uganda. Scope: Surgical care, sexual and reproductive health, HIV/AIDS, tuberculosis DOTS therapy. |
| Asfaw 2014 | Ethiopia | Access to HIV⁄AIDS care | Scope: Antiretroviral therapy |
| Paul 2014 | Uganda | Access to post-abortion care | Rationale Absence of physicians. Scope: Post-abortion care |
| O’Malley 2014 | Namibia | Access to HIV⁄AIDS care | Rationale: Shortage of physicians. Scope: Antiretroviral treatment services |
| Andriamanjato 2014 | Madagascar, Malawi, and Rwanda | Access to eye care | Rationale: Shortage of health workers trained in eye care. Scope: Primary eye care |
| Eliah 2014 | Kenya, Malawi, and Tanzania | Access to eye care | Rationale: Shortage and maldistribution of ophthalmologists. Scope: Cataract surgery |
| Wiedenmayer 2015 | Tanzania | Access to medicines | Rationale: Severe shortage of pharmaceutical staff. Scope: Pharmaceutical management |
| Mwangala 2015 | Zambia | Access to HIV testing | Rationale: Shortage of human resources. Scope: HIV testing services |
| Suzan-Monti 2015 | Cameroon | Access to HIV⁄AIDS care | Rationale: Shortage of physicians in rural areas. Scope: Initiating antiretroviral therapy (ART) |
| Chamberlain 2015 | Uganda | Access to emergency care services | Rationale: Critical shortages of acute care and healthcare workers in resource-limited settings. Scope: Emergency care services in a rural setting |
| Charyeva 2015 | Nigeria | Access to contraceptive implants | Rationale: Severe shortage of human resources. Scope: Provision of contraceptive implants |
| Agyapon 2015 | Ghana | Access to mental health services | Rationale: Inadequate numbers of psychiatrists. Scope: Mental healthcare |
| Akeju 2016 | Nigeria | Access to maternal health services | Rationale: Non-availability of health personnel at the primary healthcare level. Scope: Detection of early signs of pre-eclampsia |
| Wright 2016 | Malawi | Access to mental health services | Rationale: Improve access to primary mental healthcare. Scope: Primary mental healthcare |
| Gueye 2016 | Senegal | Access to family planning services | Rationale: To improve access to family planning in rural areas and improve contraceptive prevalence. Scope: Provision of family planning services—long-acting reversible contraceptives (LARC), specifically implants and the intrauterine device. |
| Dos Santos 2016 | Mozambique | Access to mental health services | Rationale: To expand access to primary mental healthcare due to low numbers of psychiatrists and psychologists Scope: Delivery of psychiatric care |
| Agyapong 2016a | Ghana | Access to mental health services | Rationale: Expand mental healthcare delivery due to shortage of psychiatrists. Scope: CPNs and CMHOs are primarily responsible for case detection in the community, referral of patients to CPOs and psychiatrists. CPOs are responsible for diagnosing and treating a range of common psychiatric conditions |
| Some 2016 | Kenya | Access to non-communicable diseases (NCDs) care | Rationale: Shortage of health workers at the primary level of care and need to increase access to NCD care in primary healthcare settings. Scope: Management of NCDs (hypertension, diabetes mellitus type 2, epilepsy, asthma, and sickle cell) |
| Agyapong 2016b | Ghana | Access to mental health services | Rationale: Shortage of psychiatrists. Scope: Case detection and referral, and diagnosis and treatment of common psychiatric conditions. |
| Landes 2017 | Malawi | Access to HIV⁄AIDS care | Rationale: Shortage of health workers Scope: Triaging of HIV/AIDS patients |
| Okyere 2017 | Ghana | Rationale: Insufficient health workers. | |
| Tilahun 2017 | Ethiopia | Access to family planning services | Rationale: To improve access to family planning in rural areas and improve contraceptive prevalence. Scope: Provision of long-acting contraceptive (Implanon) family planning services. |
| Bolkan 2017 | Sierra Leone | Access to emergency surgical care | Rationale: Shortage of surgical providers. Scope: Surgical and obstetric emergencies |
| Farley 2017 | South Africa | Access to TB treatment services | Rationale: Shortages of medical officers to implement decentralization of MDR-TB treatment service to outpatient settings/lower-level health facilities. Scope: Multidrug-resistant tuberculosis (MDR-TB) treatment |
| Lulebo 2017 | Democratic Republic of the Congo | Access to hypertension management services | Rationale: Shortage of health workers. Scope: Hypertension management |
| Gyamfi 2017 | Ghana | Access to hypertension management services | Rationale: To expand service delivery to lower levels. Scope: Hypertension management and control |
| Dlamini-Simelane 2017 | Swaziland | Access to HIV⁄AIDS care | Rationale: Decentralized ART provision to improve access. Scope: HIV counselling by lay counsellors (predominantly PLHIV), initiation of patients on ART by nurses |
| Kaindjee-Tjituka 2017 | Namibia | Access to CD4+ testing | Rationale: Roll-out and scale-up of POC CD4+ testing in HCT settings in public health facilities. Scope: Point-of-care (POC) CD4+ testing |
| Naburi 2017 | Tanzania | Access to HIV⁄AIDS care—PMTCT services | Rationale: Reduce nurses’ workload and health system costs. Scope: Prevention of mother-to-child transmission of HIV (PMTCT) service delivery |
| Naikoba 2017 | Uganda | Access to HIV/AIDS and TB services | Rationale: Health worker shortages. Scope: HIV care and treatment |
| Marotta 2018 | Mozambique | Access to HIV/AIDS services for children < 5 years | Rationale: To improve ART initiation and retention of HIV-infected children. Scope: Care for HIV-positive children < 5 years old |
| Davis 2018 | Malawi | Access to contraceptive implants | Rationale: Shortage of nurses/midwives. Scope: Long-acting reversible contraception (LARC) insertion (levonorgestrel (LNG) contraceptive implants) |
| Awolude 2018 | Nigeria | Access to cervical cancer screenings | Rationale: Shortage of doctors and nurses in rural areas. Scope: Screen for cervical cancer using visual inspection with acetic acid |
| Sayed 2018 | Kenya | Access to cancer screenings | Rationale: Scarcity of pathologists in Kenya. Scope: Fine-needle aspiration biopsy cytology and bone marrow aspiration and trephine biopsy |
| Millogo 2019 | Burkina Faso | Access to contraceptives | Rationale Shortage of qualified health staff. Scope: Community health workers (CHWs) to offer oral and injectable contraceptives to new users, and auxiliary nurses and auxiliary midwives to provide implants and intrauterine devices. |
| Tariku 2019 | Ethiopia | Access to contraceptives | Rationale: Shortage of physicians, improve access to surgical services and reduce neonatal mortality. Scope: Caesarean section |
| Wall 2020 | Kenya | Access to mental health services | Rationale: Improve access at the community level. Scope: Community-based family therapy mental health interventions |
| Gbagbo 2020 | Ghana | Access to intrauterine contraceptive device | Rationale: Addressing persistent human resources shortages. Scope: Intrauterine contraceptive device |
| Peresu 2020 | Eswatini | Access to multidrug-resistant tuberculosis (MDR-TB) treatment in rural areas | Rationale: Shortage of human resources for health (HRH) and limited access to multidrug-resistant tuberculosis (MDR-TB) treatment in rural areas. Scope: Directly observed treatment (DOT) supervision and administration of intramuscular MDR-TB injections |
| Lund 2020 | South Africa | Access to mental health services | Rationale: Dearth of mental health professionals. Scope: Psychological treatment for perinatal depression |
| Sevene 2021 | Mozambique | Access to hypertension services | Rationale: Delays in reaching health facilities and insufficient healthcare professionals. Scope: Initial screening and initiation of obstetric emergency care for pre-eclampsia/eclampsia |
| Jacobs 2021 | South Africa | Access to mental health services | Scope: Mental health counselling |
| Yator 2021 | Kenya | Access to HIV/AIDS care | Scope: Interpersonal psychotherapy (IPT-G) for adolescent mothers living with HIV |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Okoroafor, S.C.; Christmals, C.D. Task Shifting and Task Sharing Implementation in Africa: A Scoping Review on Rationale and Scope. Healthcare 2023, 11, 1200. https://doi.org/10.3390/healthcare11081200
Okoroafor SC, Christmals CD. Task Shifting and Task Sharing Implementation in Africa: A Scoping Review on Rationale and Scope. Healthcare. 2023; 11(8):1200. https://doi.org/10.3390/healthcare11081200
Chicago/Turabian StyleOkoroafor, Sunny C., and Christmal Dela Christmals. 2023. "Task Shifting and Task Sharing Implementation in Africa: A Scoping Review on Rationale and Scope" Healthcare 11, no. 8: 1200. https://doi.org/10.3390/healthcare11081200
APA StyleOkoroafor, S. C., & Christmals, C. D. (2023). Task Shifting and Task Sharing Implementation in Africa: A Scoping Review on Rationale and Scope. Healthcare, 11(8), 1200. https://doi.org/10.3390/healthcare11081200