
Reliability and Validity of the Health-Promoting Lifestyle Profile II Spanish Version in University Students
 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Sample
2.2. Data Collection
2.3. Data Collection Instruments
2.3.1. Information Form Including Sociodemographic Characteristics
2.3.2. Health-Promoting Lifestyle Profile-II
2.4. Linguistic Equivalence of the Scale
2.5. Data Analysis
2.6. Ethical Considerations
3. Results
3.1. Characteristics of Participants
3.2. Construct Validity Test
3.2.1. Reliability Test
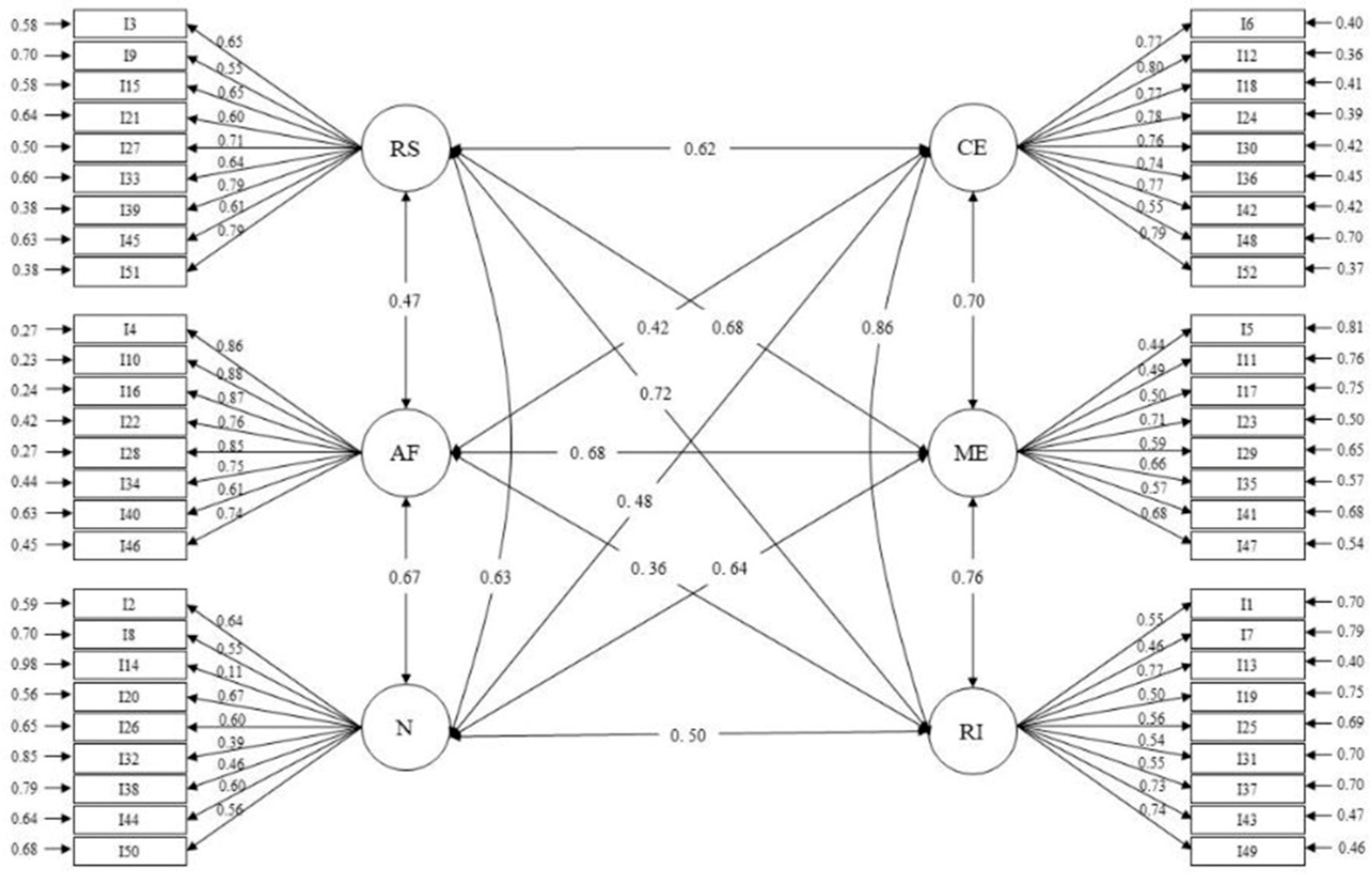
3.2.2. Confirmatory Factor Analysis (CFA)
3.3. Reliability Test
4. Discussion
5. Study Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- WHO. Life styles and Health. Soc. Sci. Med. 1986, 22, 117–124. [Google Scholar] [CrossRef] [PubMed]
- Vio, F.; Albala, C.; Crovetto, M. Health promotion in the epidemiological transition of Chile. Rev. Chil. Nutr. 2000, 27, 21–29. [Google Scholar]
- Vio, F.; Albala, C. Epidemiology of obesity in Chile. Rev. Chil. Nutr. 2000, 27, 97–112. [Google Scholar]
- Kumar, S.; Preetha, G. Health promotion: An effective tool for global health. Indian J. Community Med. 2012, 37, 5–12. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Terrazas, M.; Hernández, L.; Arizmendi, J.; Tapia, M.; Ortega, A. Lifestyle profile in university students of psychology and human communication in the State of Morelos. In Proceedings of the International Health Convention, Cuba Salud, Havana, Cuba, 20–24 April 2015. [Google Scholar]
- Castro-Cuesta, J.Y.; Abellán Huerta, J.; Leal Hernández, M.; Gómez Jara, P.; Ortín Ortín, E.J.; Abellán Alemán, J. Lifestyles related to cardiovascular risk in university students. Clin. Investig. Arterioscler. 2014, 26, 10–16. [Google Scholar] [CrossRef] [PubMed]
- Castelao-Naval, O.; Blanco-Fernández, A.; Meseguer-Barros, C.M.; Thuissard-Vasallo, I.J.; Cerdá, B.; Larrosa, M. Lifestyle and risk of atypical eating disorder in university students: Reality versus perception. Clin. Nurs. 2019, 29, 280–290. [Google Scholar]
- Cecilia, M.J.; Atucha, N.M.; García-Estañ, J. Health styles and healthy habits in students of the Degree in Pharmacy. Educ. Méd. 2018, 19, 294–305. [Google Scholar] [CrossRef]
- Cortés, S.B.; Zarceño, C.S.; de la Orden, S.G. Methodology for the estimation of use of tobacco, alcohol and other drugs. Nutr. Hosp. 2015, 31, 257–264, ISSN 0212-1611. [Google Scholar]
- Sakraida, J. Modelo de Promoción de la Salud. Nola J Pender. In Modelos y Teorías de Enfermería, 6th ed.; Maerriner, T.A., Rayle-Alligood, M., Eds.; Elsevier-Mosby: Barcelona, Spain, 2007. [Google Scholar]
- Walker, S.; Sechrist, K.; Pender, N. The health-Promoting Lifestyle Profile: Development and psychometric characteristics. Nurs. Res. 1987, 36, 76–81. [Google Scholar] [CrossRef]
- Heydari, A.; Khorashadizadeh, F. Pender’s health promotion model in medical research studies. J. Pak. Med. Assoc. 2014, 41, 59. [Google Scholar]
- Pender, N.J.; Pender, A.R. Illness prevention and health promotion services provided by nurse practitioners: Predicting potential consumers. Am. J. Public Health 1980, 70, 798–803. [Google Scholar] [CrossRef] [PubMed]
- Mohamadian, H.; Ghannaee, M.; Kortdzanganeh, J.; Meihan, L. Reliability and Construct Validity of the Iranian Version of Health-promoting Lifestyle Profile in a Female Adolescent Population. Int. J. Prev. Med. 2013, 4, 42–49. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3570910/ (accessed on 15 April 2024). [PubMed] [PubMed Central]
- Kamali, A.; Sadeghi, R.; Tol, A.; Yaseri, M. Reliability and Validity of Kurdish Language Version of Health Promoting Lifestyle 3UR¿OH II among Kurdish Healthcare Providers Kurdish Version of HPLP-II). Arch. Iran Med. 2016, 19, 824–831. Available online: https://www.researchgate.net/publication/312129229_Reliability_and_Validity_of_Kurdish_Language_Version_of_Health_Promoting_Lifestyle_Profile_II_among_Kurdish_Healthcare_Providers_Kurdish_Version_of_HPLP-II (accessed on 15 April 2024). [PubMed]
- Garmaroudi, G.; Tanjani, P.T.; Azadbakht, M.; Sahaf, R.; Fekrizadeh, Z. Validity and Reliability of Health Promoting Lifestyle Profile II in the Iranian Elderly. Int. J. Prev. Med. 2016, 7, 74. [Google Scholar] [CrossRef] [PubMed]
- Rathnayake, N.; Alwis, G.; Lenora, J.; Lekamwasam, S. Applicability of health promoting lifestyle profile-II for postmenopausal women in Sri Lanka—A validation study. Health Qual. Life Outcomes 2020, 18, 122. [Google Scholar] [CrossRef] [PubMed]
- Walker, S.N.; Kerr, M.J.; Pender, N.J.P.; Sechrist, K.R. A Spanish language version of the Health Promoting Lifestyle Profile. Nurs. Res. 1990, 39, 268–273. Available online: https://eurekamag.com/research/039/027/039027437.php (accessed on 15 April 2024). [CrossRef] [PubMed]
- Walker, S.; Hill-Polerecky, D. Psychometric Evaluation of the Health-Promoting Lifestyle Profile II; Unpublished Manuscript; University of Nebraska Medical Center: Omaha, NE, USA, 1996. [Google Scholar]
- Almutairi, K.M.; Alonazi, W.B.; Vinluan, J.M.; Almigbal, T.H.; Batais, M.A.; Al Odhayani, A.; Alsadhan, N.; Tumala, R.B.; Moussa, M.; Aboshaiqah, A.E.; et al. Health promoting lifestyle of university students in Saudi Arabia: A cross-sectional assessment. BMC Public Health 2018, 18, 1093. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Alzahrani, S.H.; Malik, A.A.; Bashawri, J.; Shaheen, S.A.; Shaheen, M.M.; Alsaib, A.A.; Mubarak, M.A.; Adam, Y.S.; Abdulwassi, H.K. Health-promoting lifestyle profile and associated factors among medical students in a Saudi university. SAGE Open Med. 2019, 7, 2050312119838426. [Google Scholar] [CrossRef] [PubMed]
- Paknazar, F.; Safaie, N.; Ketabi, S.; Kia, N.; Mirmohammadkhani, M.; Moonesan, M.R. Exploration of mental health problems in association with health-promoting lifestyle profile in Iranian medical students: A cross-sectional study. J. Educ. Health Promot. 2020, 9, 247. [Google Scholar] [CrossRef]
- Hussein, A.; Younis, N.; Ahmed, M. Health Promoting Lifestyle Profile among Nursing Students in Mosul University. 2020. Available online: https://www.researchgate.net/profile/NasirYounis/publication/344376375_Health_Promoting_Lifestyle_profile_Among_Nursing_Students_in_Mosul_University/links/5f6dc360458515b7cf4c67e8/Health-Promoting-Lifestyle-profile-Among-Nursing-Students-in-Mosul-University.pdf (accessed on 15 April 2024).
- Zeng, W.; Shang, S.; Fang, Q.; He, S.; Li, J.; Yao, Y. Health promoting lifestyle behaviors and associated predictors among clinical nurses in China: A cross-sectional study. BMC Nurs. 2021, 20, 230. [Google Scholar] [CrossRef]
- Walker, S.; Sechrist, K.; Pender, N. Health Promoting Lifestyle Profile II. Background and Permission for Use COLLEGE OF NURSING Community-Based Health Department. 1995. Available online: https://www.ijwhr.net/pdf/pdf_IJWHR_191_supp.pdf (accessed on 15 April 2024).
- Serrano-Fernández, M.; Boada-Grau, J.; Vigil-Colet, A.; Gil-Ripoll, C. Spanish adaptation of the HPLP-II scale with a sample of employees. Univ. Psychol. 2016, 15, 1–14. [Google Scholar] [CrossRef]
- Pérez-Fortis, A.; Díez, S.M.U.; Padilla, J. Psychometric properties of the Spanish version of the health-promoting lifestyle profile II. Res. Nurs. Health 2012, 35, 301–313. [Google Scholar] [CrossRef]
- Triviño, Z.; Stiepovich, J.; Merino, J. Predictors of health-promoting behaviors in peri-postmenopausal women in Cali, Colombia. Colom. Med. 2007, 38, 395–407. [Google Scholar]
- Salamanca-Ramos, E. Estilos de vida promotores de salud en mujeres de los programas sociales de Villavicencio-Colombia. Orinoquia 2015, 19, 213–219. Available online: http://www.scielo.org.co/scielo.php?script=sci_arttext&pid=S0121-37092015000200008&lng=en (accessed on 15 April 2024). [CrossRef]
- Triviño-Vargas, Z. Health-promoting behaviors in students of a higher education institution. Aquichan 2012, 12, 275–285. [Google Scholar] [CrossRef]
- Laguado, E.; Gómez, M. Healthy lifestyles in nursing students at the Universidad Cooperativa de Colombia. Towards Promoc. Health 2014, 19, 68–83. [Google Scholar]
- Valencia, C.; Henao Trujillo, O.; Gallego, F. Health-promoting behaviors and physical dependence in people with clinical diagnosis of chronic obstructive pulmonary disease. Glob. Nurs. 2017, 16, 56–79. [Google Scholar] [CrossRef]
- Browne, M.W.; Cudeck, R. Alternative ways of assessing model fit. In Testing Structural Equation Models; Bollen, K.A., Long, J.S., Eds.; Sage: Newbury Park, CA, USA, 1993; pp. 136–162. [Google Scholar]
- Tavakol, M.; Dennick, R. Making sense of Cronbach’s alpha. Int. J. Med. Educ. 2011, 2, 53–55. [Google Scholar] [CrossRef] [PubMed]
- Council for International Organizations of Medical Sciences (CIOMS); World Health Organization (WHO). International Ethical Guidelines for Health-Related Research Involving Human Subjects. 2013. Available online: https://cioms.ch/wp-content/uploads/2017/12/CIOMS-EthicalGuideline_SP_INTERIOR-FINAL.pdf (accessed on 15 April 2024).
- Por la Cual se Establecen las Normas Científicas, Técnicas y Administrativas para la Investigación en Salu. Resolucion Numero 8430 De 1993. Available online: https://www.minsalud.gov.co/sites/rid/Lists/BibliotecaDigital/RIDE/DE/DIJ/RESOLUCION-8430-DE-1993.PDF (accessed on 15 April 2024).
- Garson, D. Factor Analysis; North Caroline State University Press (Blue Books Serie): Asheboro, NC, USA, 2013. [Google Scholar]
- Raubenheimer, J. An item selection procedure to maximize scale reliability and validity. SA J. Ind. Psychol. 2004, 30, 59–64. [Google Scholar] [CrossRef]
- Pinar, R.; Celik, R.; Bahcecik, N. Reliability and construct validity of the Health-Promoting Lifestyle Profile II in an adult Turkish population. Nurs. Res. 2009, 58, 184–193. [Google Scholar] [CrossRef] [PubMed]
- Escobedo, M.; Hernández, J.; Estebané, V.; Martínez, G. Structural Equation Models: Characteristics, Phases, Construction, Application and Results. Cienc. Trab. 2016, 18, 16–22. [Google Scholar]
- Martínez, M. Market Orientation. A Model from the Perspective of Organizational Learning; Planeta: Mexico City, Mexico, 2003. [Google Scholar]
- Kuan, G.; Kueh, Y.C.; Abdullah, N.; Tai, E.L.M. Propiedades psicométricas del perfil de estilo de vida que promueve la salud II: Validación transcultural de la versión en malayo. BMC Public Health 2019, 19, 751. [Google Scholar] [CrossRef]
- Lolokote, S.; Hidru, T.H.; Li, X. Do socio-cultural factors influence college students’ self-rated health status and health-promoting lifestyles? A cross-sectional multicenter study in Dalian, China. BMC Public Health 2017, 17, 478 . [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Savarese, G.; Carpinelli, L.; Cavallo, P.; Vitale, M.P. Italian psychometric validation of the multidimensional student health-promoting lifestyle profile scale. Health 2018, 10, 1554–1575. [Google Scholar] [CrossRef]
- Olutende, O.; Wamukoya, E.; Wanzala, C. Validation of a Four-Factor Measurement Model of the Health Promoting Lifestyle Profile-II: A Confirmatory Study with Kenyan Undergraduate Students. Saudi J. Nurs. Health Care 2019, 2, 396–406. Available online: https://saudijournals.com/media/articles/SJNHC_212_396-406.pdf (accessed on 15 April 2024). [CrossRef]
- Kuster, A.E.; Fong, C.M. Further psychometric evaluation of the Spanish language health-promoting lifestyle profile. Nurs. Res. 1993, 42, 266–269. [Google Scholar] [CrossRef] [PubMed]
- Enríquez-Reyna, M.C.; Alejandro, P.P.; González, Á.D.I.; Infante, E.A.G.; Salazar, A.d.C.V.; Rodríguez, R.E.M. Psychometric properties of the Spanish version of the Health-Promoting Lifestyle Profile-II instrument in Mexican university students. Enferm. Glob. 2022, 21, 398–423. [Google Scholar] [CrossRef]
- Messick, S. Test validity and ethics of assessment. Am. Psychol. 1980, 35, 1012–1027. [Google Scholar] [CrossRef]
- Pender, N.J.; Walker, S.N.; Sechrist, K.R.; Stromborg, M.F. Development and testing of the health promotion model. Cardiovasc. Nurs. 1988, 24, 41–43. [Google Scholar]
- Pender, N.J.P.; Walker, S.N.; Sechrist, K.R.; Frank-Stromborg, M.E. Predicting health-promoting lifestyles in the workplace. Nurs. Res. 1990, 39, 326–332. [Google Scholar] [CrossRef]
- Lee, R.L.; Loke, A.Y.; Wu, C.S.; Ho, A.P. The Lifestyle Behaviours and Psychosocial Well-Being of Primary School Students in Hong Kong. J. Clin. Nurs. 2010, 19, 1462–1472. [Google Scholar] [CrossRef] [PubMed]
- Bryer, J.; Cherkis, F.; Raman, J. Health-promotion behaviors of undergraduate nursing students: A survey analysis. Nurs. Educ. Perspect. 2013, 34, 410–415. [Google Scholar] [CrossRef] [PubMed]
- Peng, S.; Othman, A.T.; Khairani, A.Z.; Zeng, G.; Xiaogang, Z.; Fang, Y. Effectiveness of pedometer- and accelerometer-based interventions in improving physical activity and health-related outcomes among college students: A systematic review and meta-analysis. Digit. Health 2023, 9, 20552076231188213. [Google Scholar] [CrossRef] [PubMed]
- Ringeval, M.; Wagner, G.; Denford, J.; Paré, G.; Kitsiou, S. Fitbit-Based Interventions for Healthy Lifestyle Outcomes: Systematic Review and Meta-Analysis. J. Med. Internet Res. 2020, 22, e23954. [Google Scholar] [CrossRef] [PubMed]
- Al-Nawaiseh, H.K.; McIntosh, W.A.; McKyer, L.J. An-m-Health Intervention Using Smartphone App to Improve Physical Activity in College Students: A Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2022, 19, 7228. [Google Scholar] [CrossRef]
- Aloufi, M.A.; Jarden, R.J.; Gerdtz, M.F.; Kapp, S. Reducing stress, anxiety and depression in undergraduate nursing students: Systematic review. Nurse Educ. Today 2021, 102, 104877. [Google Scholar] [CrossRef]

{kind=link}
| Characteristics | N (%) |
|---|---|
| Sex | |
| Male | 161 (21.1) |
| Female | 602 (78.9) |
| Age (years) | |
| Mean ± SD | 21.73± 4.29 |
| Ethnicity | |
| White | 181 (23.7) |
| Indigenous | 19 (2.5) |
| Mestizo | 428 (56.1) |
| Mulatto | 17 (2.2) |
| Black | 116 (15.2) |
| Raizal | 2 (0.3) |
| Socioeconomic stratum | |
| 1 | 90 (11.8) |
| 2 | 244 (32) |
| 3 | 271 (35.5) |
| 4 | 114 (14.9) |
| 5 | 36 (4.7) |
| 6 | 8 (1) |
| Academic program | |
| Pre-hospital care | 2 (0.3) |
| Nursing | 296 (38.8) |
| Physiotherapy | 55 (7.2) |
| Phonoaudiology | 18 (2.4) |
| Surgical instrumentation | 138 (18.1) |
| Dental mechanics | 1 (0.1) |
| Medicine | 221 (29) |
| Dentistry | 13 (1.7) |
| Psychology | 16 (2.1) |
| Pharmacy Regency | 1 (0.1) |
| Respiratory therapy | 2 (0.3) |
| Scale | Indicators | Mean ± SD | Item–Total Correlation | Corrected Item–Total Correlation | Factorial Loading (p Value) | |
|---|---|---|---|---|---|---|
| HR | Item 3 | 2.41 ± 0.66 | 0.51 | 0.49 | 0.65 (<0.001) | |
| Item 9 | 2.23 ± 0.72 | 0.46 | 0.45 | 0.55 (<0.001) | ||
| Item 15 | 2.53 ± 0.62 | 0.50 | 0.48 | 0.65 (<0.001) | ||
| Item 21 | 2.25 ± 0.71 | 0.49 | 0.48 | 0.60 (<0.001) | ||
| Item 27 | 2.38 ± 0.67 | 0.54 | 0.52 | 0.71 (<0.001) | ||
| Item 33 | 2.51 ± 0.67 | 0.52 | 0.50 | 0.63 (<0.001) | ||
| Item 39 | 2.37 ± 0.69 | 0.63 | 0.61 | 0.79 (<0.001) | ||
| Item 45 | 1.77 ± 0.76 | 0.47 | 0.47 | 0.61 (<0.001) | ||
| Item 51 | 2.64 ± 0.55 | 0.61 | 0.58 | 0.79 (<0.001) | ||
| PA | Item 4 | 2.04 ± 0.79 | 0.56 | 0.55 | 0.86 (<0.001) | |
| Item 10 | 2.14 ± 0.79 | 0.54 | 0.52 | 0.88 (<0.001) | ||
| Item 16 | 2.17 ± 0.75 | 0.60 | 0.59 | 0.87 (<0.001) | ||
| Item 22 | 2.15 ± 0.78 | 0.56 | 0.56 | 0.76 (<0.001) | ||
| Item 28 | 2.22 ± 0.76 | 0.57 | 0.56 | 0.86 (<0.001) | ||
| Item 34 | 2.27 ± 0.75 | 0.56 | 0.55 | 0.75 (<0.001) | ||
| Item 40 | 1.95 ± 0.80 | 0.43 | 0.42 | 0.61 (<0.001) | ||
| Item 46 | 1.98 ± 0.81 | 0.54 | 0.53 | 0.74 (<0.001) | ||
| N | Item 2 | 2.17 ± 0.69 | 0.45 | 0.45 | 0.65 (<0.001) | |
| Item 8 | 2.22 ± 0.73 | 0.39 | 0.38 | 0.55 (<0.001) | ||
| Item 14 | 1.88 ± 0.78 | 0.10 | 0.10 | 0.11 (<0.05) | ||
| Item 20 | 2.15 ± 0.68 | 0.48 | 0.47 | 0.67 (<0.001) | ||
| Item 26 | 2.27 ± 0.72 | 0.43 | 0.42 | 0.60 (<0.001) | ||
| Item 32 | 2.25 ± 0.71 | 0.31 | 0.30 | 0.39 (<0.001) | ||
| Item 38 | 2.66 ± 0.54 | 0.34 | 0.33 | 0.45 (<0.001) | ||
| Item 44 | 2.03 ± 0.81 | 0.44 | 0.43 | 0.60(<0.001) | ||
| Item 50 | 2.60 ± 0.59 | 0.42 | 0.40 | 0.556(<0.001) | ||
| CE | Item 6 | 2.76 ± 0.50 | 0.61 | 0.58 | 0.77 (<0.001) | |
| Item 12 | 2.88 ± 0.37 | 0.55 | 0.51 | 0.80 (<0.001) | ||
| Item 18 | 2.59 ± 0.57 | 0.54 | 0.50 | 0.77 (<0.001) | ||
| Item 24 | 2.71 ± 0.53 | 0.61 | 0.57 | 0.78 (<0.001) | ||
| Item 30 | 2.85 ± 0.39 | 0.59 | 0.56 | 0.76 (<0.001) | ||
| Items 36 | 2.58 ± 0.58 | 0.61 | 0.59 | 0.74 (<0.001) | ||
| Items 42 | 2.87 ± 0.36 | 0.57 | 0.53 | 0.77 (<0.001) | ||
| Items 48 | 2.37 ± 0.75 | 0.46 | 0.45 | 0.55 (<0.001) | ||
| Items 52 | 2.72 ± 0.49 | 0.65 | 0.63 | 0.79 (<0.001) | ||
| IR | Items 1 | 2.31 ± 0.63 | 0.43 | 0.40 | 0.55 (<0.001) | |
| Item 7 | 2.90 ± 0.36 | 0.32 | 0.30 | 0.47 (<0.001) | ||
| Items 13 | 2.83 ± 0.42 | 0.56 | 0.53 | 0.76 (<0.001) | ||
| Items 19 | 2.46 ± 0.62 | 0.41 | 0.40 | 0.50 (<0.001) | ||
| Items 25 | 2.53 ± 0.66 | 0.44 | 0.42 | 0.56 (<0.001) | ||
| Items 31 | 2.61 ± 0.62 | 0.42 | 0.40 | 0.55 (<0.001) | ||
| Items 37 | 2.43 ± 0.67 | 0.45 | 0.43 | 0.55 (<0.001) | ||
| Items 43 | 2.43 ± 0.69 | 0.57 | 0.55 | 0.73 (<0.001) | ||
| Items 49 | 2.81 ± 0.43 | 0.57 | 0.55 | 0.73 (<0.001) | ||
| SM | Items 5 | 2.42 ± 0.61 | 0.37 | 0.36 | 0.44 (<0.001) | |
| Items 11 | 2.34 ± 0.69 | 0.43 | 0.42 | 0.49 (<0.001) | ||
| Items 17 | 2.59 ± 0.57 | 0.44 | 0.42 | 0.50 (<0.001) | ||
| Items 23 | 2.58 ± 0.62 | 0.58 | 0.56 | 0.71 (<0.001) | ||
| Items 29 | 1.79 ± 0.78 | 0.49 | 0.49 | 0.59 (<0.001) | ||
| Items 35 | 2.37 ± 0.66 | 0.56 | 0.54 | 0.66 (<0.001) | ||
| Items 41 | 1.69 ± 0.76 | 0.46 | 0.45 | 0.57 (<0.001) | ||
| Items 47 | 2.06 ± 0.74 | 0.57 | 0.56 | 0.68 (<0.001) | ||
| Adjustment indices | ||||||
| Absolute adjustment measures | Incremental adjustment measures | |||||
| χ2; gl (p) | RMSEA (CI 90%) | SRMR | NFI | NNFI | AGFI | |
| Acceptable level of adjustment | - | ≤0.08 | ≤0.08 | >0.90 | ≥0.90 | ≥0.90 |
| Measure | 7168.98; 1268 (<0.001) | 0.078 (0.076; 0.080) | 0.079 | 0.956 | 0.954 | 0.95 |
| HR r | PA r | N r | SG r | IR r | SM r | |
|---|---|---|---|---|---|---|
| HR | 1 | |||||
| PA | 0.47 | 1 | ||||
| N | 0.63 | 0.67 | 1 | |||
| SG | 0.62 | 0.42 | 0.48 | 1 | ||
| IR | 0.72 | 0.36 | 0.50 | 0.86 | 1 | |
| SM | 0.68 | 0.68 | 0.64 | 0.76 | 0.70 | 1 |
| Cronbach’s alpha | 0.84 | 0.89 | 0.68 | 0.87 | 0.79 | 0.76 |
| Overall Cronbach’s alpha | 0.94 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zambrano Bermeo, R.N.; Estrada Gonzalez, C.; Herrera Guerra, E.d.P.; Aviles Gonzalez, C.I. Reliability and Validity of the Health-Promoting Lifestyle Profile II Spanish Version in University Students. Healthcare 2024, 12, 1330. https://doi.org/10.3390/healthcare12131330
Zambrano Bermeo RN, Estrada Gonzalez C, Herrera Guerra EdP, Aviles Gonzalez CI. Reliability and Validity of the Health-Promoting Lifestyle Profile II Spanish Version in University Students. Healthcare. 2024; 12(13):1330. https://doi.org/10.3390/healthcare12131330
Chicago/Turabian StyleZambrano Bermeo, Rosa Nury, Catalina Estrada Gonzalez, Eugenia del Pilar Herrera Guerra, and Cesar Ivan Aviles Gonzalez. 2024. "Reliability and Validity of the Health-Promoting Lifestyle Profile II Spanish Version in University Students" Healthcare 12, no. 13: 1330. https://doi.org/10.3390/healthcare12131330