
An Evaluation of Patient Privacy Protection with Fuzzy Conjoint Analysis—A Case Study from Nurses’ Perspective
 ,
,
Abstract
1. Introduction
- information system dependence,
- medical device connections,
- multiple software usage,
- multi-user shared devices.
- A suggestion of the electronically stored minimum and maximum data sets needing to be protected.
- The access mechanisms to these data sets.
- The authorization mechanisms of healthcare staff.
- The education/awareness/informing mechanisms of healthcare staff about patient privacy.
2. Materials and Methods
2.1. Ethical Considerations
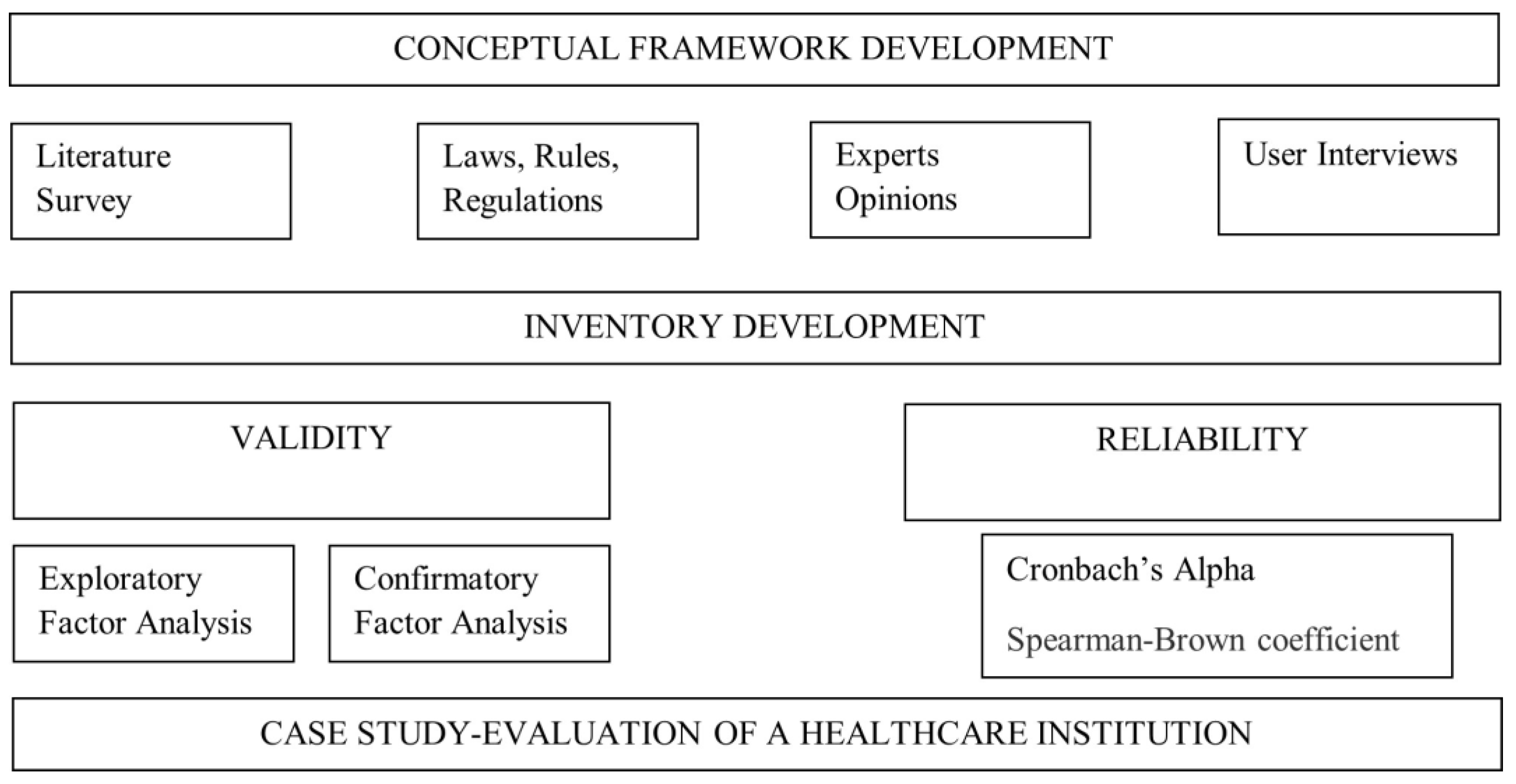
2.2. Study Design
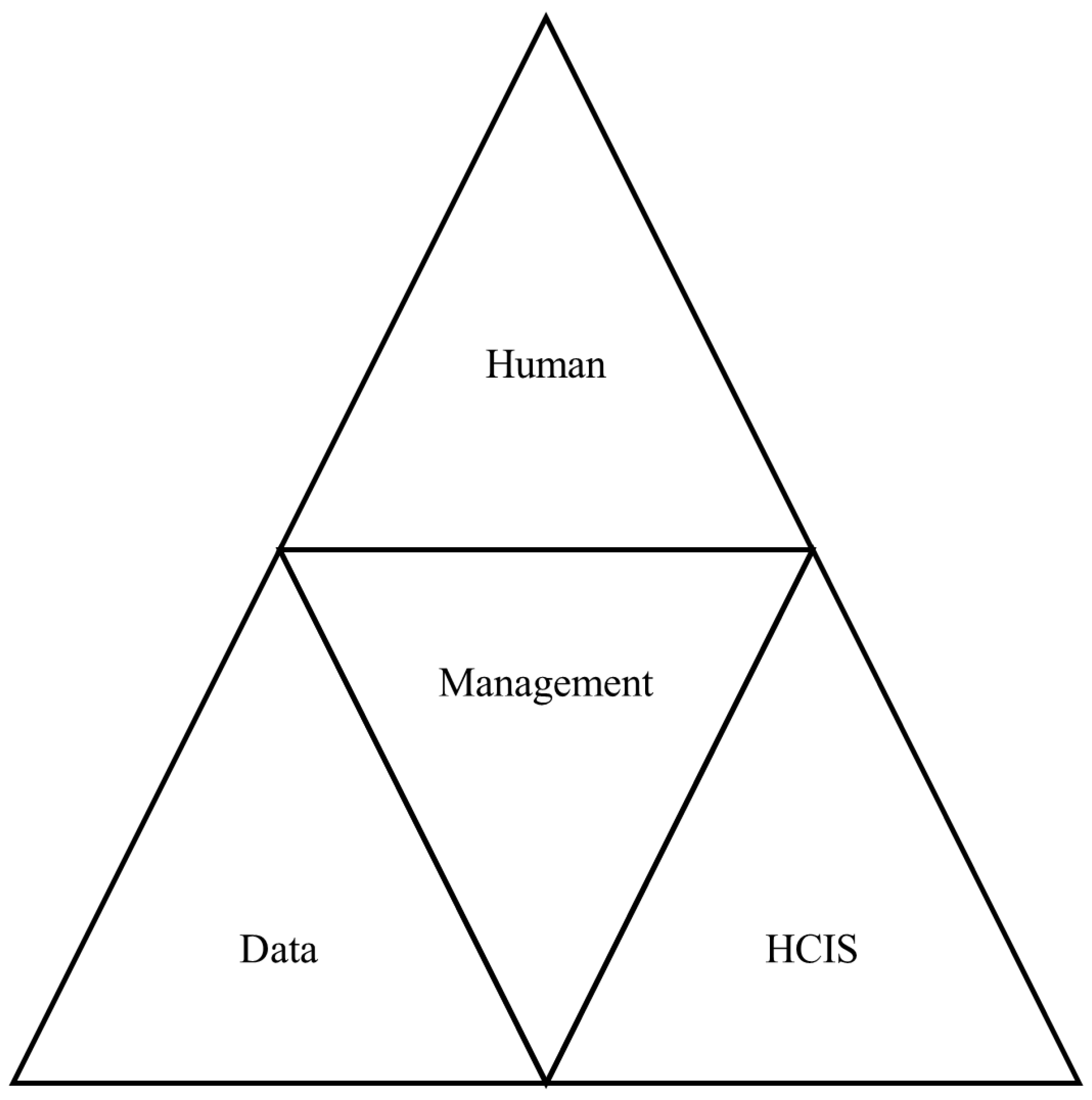
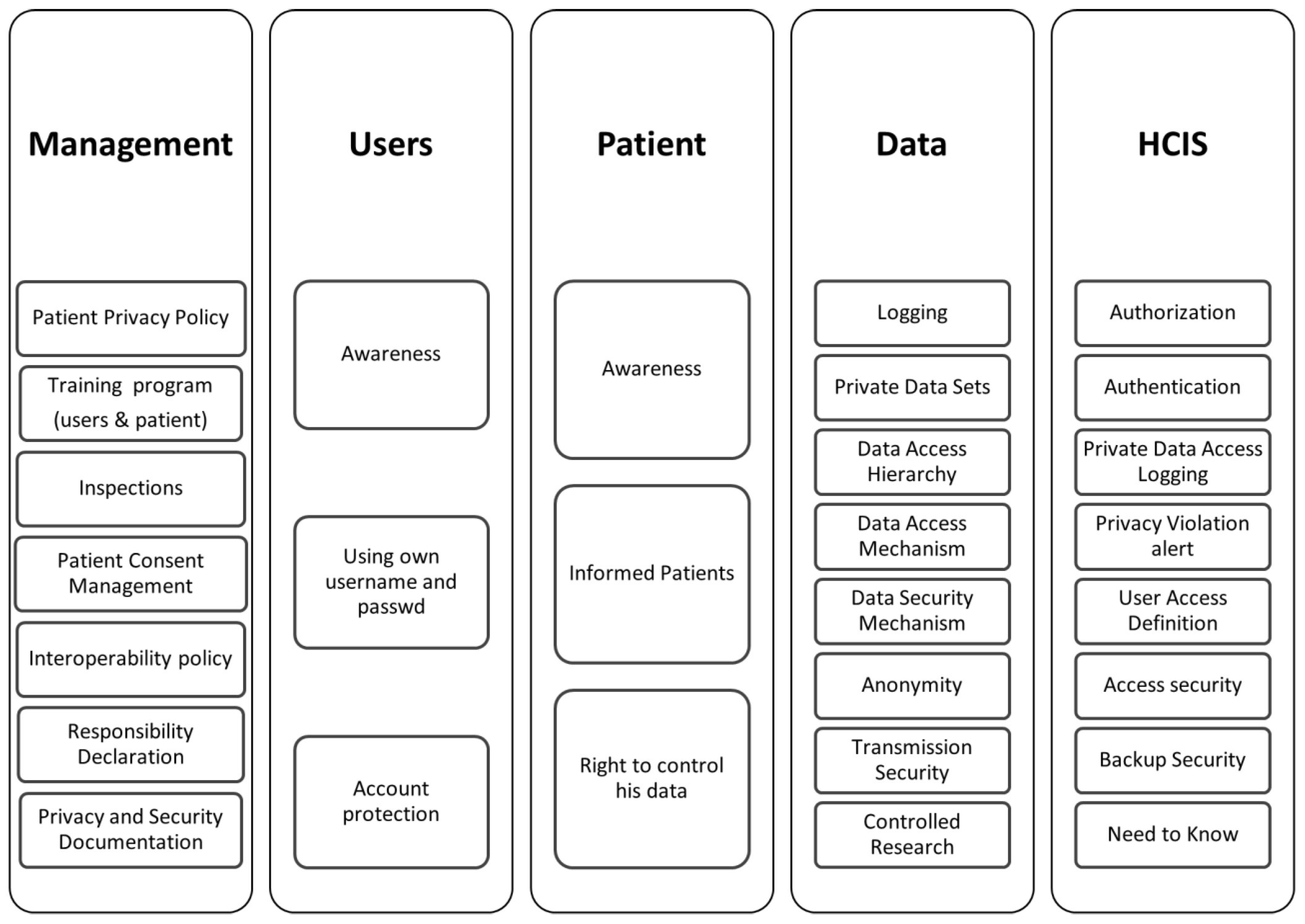
2.3. Conceptual Framework
- Management
- Users
- Patient
- Data
- Healthcare Information System (HCIS)
- Names.
- All elements of dates (except year).
- Phone numbers.
- Fax numbers.
- E-mail addresses.
- Social security numbers.
- Medical record numbers.
- Health plan numbers.
- Account numbers.
- Certificate/license numbers.
- All means of vehicle numbers.
- All means of device identifiers.
- Web Universal Resource Locators (URLs).
- Internet Protocol (IP) addresses.
- All means of biometric identifiers.
- Any comparable images.
- Any other unique identifying numbers.
2.4. Data Collection
2.5. Statistical Analysis
2.5.1. Content Validity
2.5.2. Structure Validity
2.5.3. Reliability
2.5.4. Patient Privacy Protection Maturity Inventory
2.5.5. Evaluation
- wi is the answer given by the i-th participant,
- ∑Wi is the sum of the answers given to the ith inventory item,
- wi/∑Wi is the weight of the i-th participant,
- Xi is the corresponding fuzzy set of the i-th respondents (if the answer is “Moderately disagree”, then Xi is (0, 0.25, 0.5)),
- Fj is the jth inventory item,
- n is the total number of answers.
- Ri (yj, A) is the fuzzy set determined by 2 (Formula (2)),
- F (xj, l) is the standard fuzzy sets defined (Table 1)
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sun, W.; Cai, Z.; Li, Y.; Liu, F.; Fang, S.; Wang, G. Security and privacy in the medical internet of things: A review. Secur. Commun. Netw. 2018, 2018, 5978636. [Google Scholar] [CrossRef]
- Tertulino, R.; Antunes, N.; Morais, H. Privacy in electronic health records: A systematic mapping study. J. Public Health 2024, 32, 435–454. [Google Scholar] [CrossRef]
- Yayla, A.; İlgin, V.E.; Özlü, Z.K. Development of the Perioperative Privacy Scale: A Validity and Reliability Study. J. PeriAnesthesia Nurs. 2022, 37, 227–233. [Google Scholar] [CrossRef] [PubMed]
- Goodman, K.W. Confidentiality and Privacy. In Guidance for Healthcare Ethics Committees; Hester Micah, D., Schonfeld, T.L., Eds.; Cambridge University Press: Cambridge, UK; London, UK, 2022; pp. 85–94. [Google Scholar]
- Hurst, W.; Boddy, A.; Merabti, M.; Shone, N. Patient privacy violation detection in healthcare critical infrastructures: An investigation using density-based benchmarking. Future Internet 2020, 12, 100. [Google Scholar] [CrossRef]
- Wallace, I.M. Is Patient Confidentiality Compromised with the Electronic Health Record?: A Position Paper. Comput. Inform. Nurs. 2016, 33, 58–62. [Google Scholar] [CrossRef] [PubMed]
- Jimmy, F.N.U. Cyber security Vulnerabilities and Remediation through Cloud Security Tools. J. Artif. Intell. Gen. Sci. (JAIGS) 2024, 2, 129–171. [Google Scholar]
- Ak, B.; Tanrıkulu, F.; Gündoğdu, H.; Yılmaz, D.; Öner, Ö.; Ziyai, N.Y.; Dikmen, Y. Cultural viewpoints of nursing students on patient privacy: A qualitative study. J. Relig. Health 2021, 60, 188–201. [Google Scholar] [CrossRef]
- Akar, Y.; Özyurt, E.; Erduran, S.; Uğurlu, D.; Aydın, İ. Hasta mahremiyetinin değerlendirilmesi [Evaluation of patient confidentiality]. Sağlık Akad. Derg. [Health Care Acad. J.] 2021, 6, 18–24. [Google Scholar]
- Hartigan, L.; Cussen, L.; Meaney, S.; O’Donoghue, K. Patients’ perception of privacy and confidentiality in the emergency department of a busy obstetric unit. BMC Health Serv. Res. 2018, 18, 978. [Google Scholar] [CrossRef]
- Aslan, A.; Greve, M.; Diesterhöft, T.; Kolbe, L. Can Our Health Data Stay Private? A Review and Future Directions for IS Research on Privacy-Preserving AI in Proceedings of Healthcare Wirtschaftsinformatik 2022, 8. Available online: https://aisel.aisnet.org/wi2022/digital_health/digital_health/8 (accessed on 2 May 2024).
- Kaur, R.; Shahrestani, S.; Ruan, C. Security and Privacy of Wearable Wireless Sensors in Healthcare: A Systematic Review. Comput. Netw. Commun. 2024, 2, 24–48. [Google Scholar] [CrossRef]
- Zhang, C.; Shahriar, H.; Riad, A.K. Security and Privacy Analysis of Wearable Health Device. In Proceedings of the IEEE 44th Annual Computers, Software, and Applications Conference (COMPSAC), Madrid, Spain, 13–17 July 2020; pp. 1767–1772. [Google Scholar]
- Haris, M.; Haddadi, H.; Hui, P. Privacy leakage in mobile computing: Tools, methods, and characteristics. arXiv 2014, arXiv:1410.4978. [Google Scholar]
- Shen, N.; Sequeira, L.; Silver, M.P.; Carter-Langford, A.; Strauss, J.; Wiljer, D. Patient privacy perspectives on health information exchange in a mental health context: Qualitative study. JMIR Ment. Health 2019, 6, e13306. [Google Scholar] [CrossRef]
- Murdoch, B. Privacy and artificial intelligence: Challenges for protecting health information in a new era. BMC Med. Ethics 2021, 22, 122. [Google Scholar] [CrossRef]
- George, A.S.; Baskar, T.; Srikaanth, P.B. Cyber Threats to Critical Infrastructure: Assessing Vulnerabilities Across Key Sectors. Partn. Univers. Int. Innov. J. 2024, 2, 51–75. [Google Scholar]
- Goldberg, S.G.; Johnson, G.A.; Shriver, S.K. Regulating privacy online: An economic evaluation of the GDPR. Am. Econ. J. Econ. Policy 2024, 16, 325–358. [Google Scholar] [CrossRef]
- Öztürk, H.; Torun Kılıç, Ç.; Kahriman, İ.; Meral, B.; Çolak, B. Assessment of nurses’ respect for patient privacy by patients and nurses: A comparative study. J. Clin. Nurs. 2021, 30, 1079–1090. [Google Scholar] [CrossRef] [PubMed]
- Wu, H.; Dwivedi, A.D.; Srivastava, G. Security and privacy of patient information in medical systems based on blockchain technology. ACM Trans. Multimed. Comput. Commun. Appl. (TOMM) 2021, 17, 60. [Google Scholar] [CrossRef]
- Rychik, J. You can only change what you measure: An argument for more detailed characterization in the Fontan circulation. Eur. Heart J. 2022, 43, 2385–2387. [Google Scholar] [CrossRef] [PubMed]
- Sebetci, Ö. Enhancing end-user satisfaction through technology compatibility: An assessment on health information system. Health Policy Technol. 2018, 7, 265–274. [Google Scholar] [CrossRef]
- Bastug, M. The structural relationship of reading attitude, reading comprehension and academic achievement. Int. J. Soc. Sci. Educ. 2014, 4, 931–946. [Google Scholar]
- Ilhan, M.; Cetin, B. Comparing the analysis results of the structural equation models (SEM) conducted using LISREL and AMOS. J. Meas. Eval. Educ. Psychol.-Epod 2014, 5, 26–42. [Google Scholar]
- Sofian, S.S.; Rambely, A.S. Measuring perceptions of students toward game and recreational activity using fuzzy conjoint analysis. Indones. J. Electr. Eng. Comput. Sci. 2020, 20, 395–404. [Google Scholar]
- Turksen, I.B.; Willson, I.A. A fuzzy set preference model for consumer choice. Fuzzy Sets Syst. 1994, 68, 253–266. [Google Scholar] [CrossRef]
- Leech, N.; Barrett, K.; Morgan, G.A. SPSS for Intermediate Statistics: Use and Interpretation; Lawrence Erlbaum Associates Inc.: Mahwah, NJ, USA, 2013; pp. 154–158. [Google Scholar]
- Huang, M.; Liu, A.; Wang, T.; Huang, C. Green data gathering under delay differentiated services constraint for internet of things. Wirel. Commun. Mob. Comput. 2018, 2018, 1–23. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Data | Hierarchy Level |
|---|---|
| Name | 7 |
| Phone Number | 6 |
| Certificate number | 4 |
| Plate Number | 4 |
| Social Security Number | 7 |
| Data | Hierarchy Level |
|---|---|
| Physician | 7 |
| Nurse | 5 |
| Technician | 2 |
| Lab technician | 2 |
| Office Worker | 1 |
| Perfect Fit | Acceptable Fit | |
|---|---|---|
| AGFI | 0.90 ≤ AGFI ≤ 1.00 | 0.85 ≤ AGFI ≤ 0.90 |
| GFI | 0.95 ≤ GFI ≤ 1.00 | 0.90 ≤ GFI ≤ 0.95 |
| CFI | 0.95 ≤ CFI ≤ 1.00 | 0.90 ≤ CFI ≤ 0.95 |
| NFI | 0.95 ≤ NFI ≤ 1.00 | 0.90 ≤ NFI ≤ 0.95 |
| RMSEA | 0.00 ≤ RMSEA ≤ 0.05 | 0.05 ≤ RMSEA ≤ 0.08 |
| χ2/df | 2 ≤ χ2/df ≤ 3 | 3 ≤ χ2/df ≤ 5 |
| Data | Hierarchy Level |
|---|---|
| Strongly Agree | 0.75, 1, 1 |
| Moderately Agree | 0.5, 0.75, 1 |
| Not Sure | 0.25, 0.5, 0.75 |
| Moderately Disagree | 0, 0.25, 0.5 |
| Strongly Disagree | 0, 0, 0.25 |
| Dimension | Cronbach’s Alpha | Spearman-Brown | Guttman’s |
|---|---|---|---|
| Management | 0.929 | 0.870 | 0.930 |
| User | 0.834 | 0.830 | 0.834 |
| Patient | 0.853 | 0.768 | 0.856 |
| Data | 0.930 | 0.906 | 0.930 |
| Information system | 0.925 | 0.903 | 0.926 |
| Perfect Fit | Acceptable Fit | Study Value | |
|---|---|---|---|
| AGFI | 0.90 ≤ AGFI ≤ 1.00 | 0.85 ≤ AGFI ≤ 0.90 | 0.876 |
| GFI | 0.95 ≤ GFI ≤ 1.00 | 0.90 ≤ GFI ≤ 0.95 | 0.954 |
| CFI | 0.95 ≤ CFI ≤ 1.00 | 0.90 ≤ CFI ≤ 0.95 | 0.969 |
| NFI | 0.95 ≤ NFI ≤ 1.00 | 0.90 ≤ NFI ≤ 0.95 | 0.963 |
| RMSEA | 0.00 ≤ RMSEA ≤ 0.05 | 0.05 ≤ RMSEA ≤ 0.08 | 0.497 |
| χ2/df | 2 ≤ χ2/df ≤ 3 | 3 ≤ χ2/df ≤ 5 | 2.87 |
| Variable | Similarity | Strongly Disagree | Moderately Disagree | Not Sure | Moderately Agree | Strongly Agree |
|---|---|---|---|---|---|---|
| M1 | Moderately Disagree | 0.718218 | 0.784835 | 0.519829 | 0.426298 | 0.384119 |
| M2 | Moderately Disagree | 0.699176 | 0.80075 | 0.532724 | 0.43434 | 0.390028 |
| M3 | Moderately Disagree | 0.650733 | 0.843053 | 0.564349 | 0.449726 | 0.398236 |
| M4 | Moderately Disagree | 0.709998 | 0.788945 | 0.52799 | 0.430863 | 0.386971 |
| M5 | Moderately Disagree | 0.684141 | 0.818907 | 0.540279 | 0.437499 | 0.39033 |
| M6 | Moderately Disagree | 0.628925 | 0.828878 | 0.587218 | 0.461348 | 0.403716 |
| M7 | Moderately Disagree | 0.668136 | 0.844412 | 0.546092 | 0.439264 | 0.390171 |
| M8 | Moderately Disagree | 0.66005 | 0.842132 | 0.556088 | 0.444531 | 0.393638 |
| M9 | Moderately Disagree | 0.668635 | 0.827864 | 0.552673 | 0.443886 | 0.393705 |
| U1 | Moderately Disagree | 0.733799 | 0.766653 | 0.514777 | 0.424011 | 0.382616 |
| U2 | Moderately Disagree | 0.650898 | 0.837291 | 0.565584 | 0.451363 | 0.39905 |
| U3 | Moderately Disagree | 0.642923 | 0.8332 | 0.572724 | 0.456872 | 0.403466 |
| U4 | Moderately Disagree | 0.668369 | 0.834325 | 0.550549 | 0.442125 | 0.393091 |
| P1 | Moderately Disagree | 0.663697 | 0.827674 | 0.557226 | 0.446755 | 0.396578 |
| P2 | Moderately Disagree | 0.691294 | 0.807406 | 0.538052 | 0.436991 | 0.391008 |
| P3 | Moderately Disagree | 0.642528 | 0.843339 | 0.571963 | 0.452661 | 0.398293 |
| P4 | Moderately Disagree | 0.624436 | 0.823395 | 0.590312 | 0.466845 | 0.409217 |
| P5 | Moderately Disagree | 0.698044 | 0.801263 | 0.533885 | 0.434788 | 0.388898 |
| D1 | Moderately Disagree | 0.6586 | 0.840305 | 0.558345 | 0.445075 | 0.393691 |
| D2 | Moderately Disagree | 0.62853 | 0.838854 | 0.585223 | 0.459092 | 0.402227 |
| D3 | Moderately Disagree | 0.647867 | 0.861636 | 0.561251 | 0.446213 | 0.393621 |
| D4 | Moderately Disagree | 0.630309 | 0.831065 | 0.585698 | 0.45986 | 0.403015 |
| D5 | Moderately Disagree | 0.650272 | 0.857155 | 0.560497 | 0.445853 | 0.393649 |
| D6 | Moderately Disagree | 0.648802 | 0.847849 | 0.564973 | 0.448839 | 0.396096 |
| HCIS1 | Moderately Disagree | 0.627952 | 0.860448 | 0.579846 | 0.455302 | 0.39888 |
| HCIS2 | Moderately Disagree | 0.671541 | 0.832493 | 0.547898 | 0.440915 | 0.39221 |
| HCIS3 | Moderately Disagree | 0.663280 | 0.839029 | 0.553546 | 0.444322 | 0.394377 |
| HCIS4 | Moderately Disagree | 0.624389 | 0.836324 | 0.589115 | 0.461753 | 0.404283 |
| HCIS5 | Moderately Disagree | 0.637784 | 0.851736 | 0.573845 | 0.452763 | 0.397918 |
| HCIS6 | Moderately Disagree | 0.654471 | 0.847441 | 0.559831 | 0.445748 | 0.394069 |
| Dimension | Similarity | Strongly Disagree | Moderately Disagree | Not Sure | Moderately Agree | Strongly Agree |
|---|---|---|---|---|---|---|
| Management | Moderately Disagree | 0.676446 | 0.819975 | 0.547471 | 0.440862 | 0.392324 |
| User | Moderately Disagree | 0.673997 | 0.817867 | 0.550909 | 0.443593 | 0.394556 |
| Patient | Moderately Disagree | 0.664 | 0.820615 | 0.558287 | 0.447608 | 0.396799 |
| Data | Moderately Disagree | 0.644063 | 0.846144 | 0.569331 | 0.450822 | 0.39705 |
| Information System | Moderately Disagree | 0.64657 | 0.844579 | 0.567347 | 0.450134 | 0.396956 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gürsel, G.; Bayer, N.; Turunç, Ö.; Çalışkan, A.; Akkoç, İ.; Demirci, A.; Çetin, M.; Köroğlu, Ö. An Evaluation of Patient Privacy Protection with Fuzzy Conjoint Analysis—A Case Study from Nurses’ Perspective. Healthcare 2024, 12, 1363. https://doi.org/10.3390/healthcare12131363
Gürsel G, Bayer N, Turunç Ö, Çalışkan A, Akkoç İ, Demirci A, Çetin M, Köroğlu Ö. An Evaluation of Patient Privacy Protection with Fuzzy Conjoint Analysis—A Case Study from Nurses’ Perspective. Healthcare. 2024; 12(13):1363. https://doi.org/10.3390/healthcare12131363
Chicago/Turabian StyleGürsel, Güney, Nükhet Bayer, Ömer Turunç, Abdullah Çalışkan, İrfan Akkoç, Ayhan Demirci, Melike Çetin, and Özlem Köroğlu. 2024. "An Evaluation of Patient Privacy Protection with Fuzzy Conjoint Analysis—A Case Study from Nurses’ Perspective" Healthcare 12, no. 13: 1363. https://doi.org/10.3390/healthcare12131363
APA StyleGürsel, G., Bayer, N., Turunç, Ö., Çalışkan, A., Akkoç, İ., Demirci, A., Çetin, M., & Köroğlu, Ö. (2024). An Evaluation of Patient Privacy Protection with Fuzzy Conjoint Analysis—A Case Study from Nurses’ Perspective. Healthcare, 12(13), 1363. https://doi.org/10.3390/healthcare12131363