
Lung Cancer Surgery in Octogenarians: Implications and Advantages of Artificial Intelligence in the Preoperative Assessment

 , , ,
, , , 
Abstract
1. Introduction
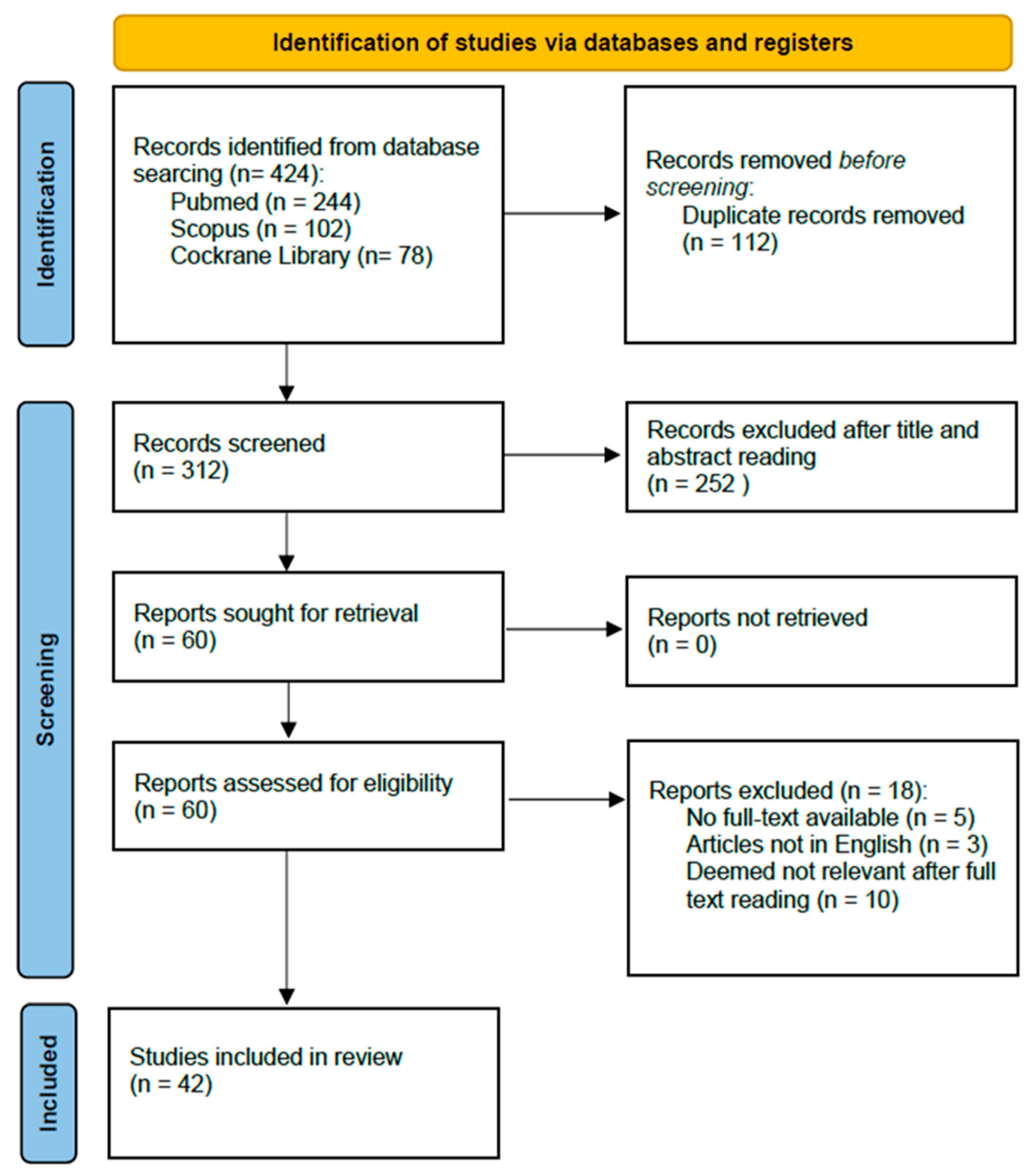
2. Materials and Methods
3. Preoperative Risk Assessment

{kind=link}
| Author | Objective | ML Algorithm | Main Results |
|---|---|---|---|
| Salati M et al. [19] | Prediction of cardiopulmonary complications in patients undergoing lung resection | XGBOOST | XGBOOST algorithm generated a model able to predict complications with an AUC of 0.75 |
| Huang G et al. [20] | Prediction of postoperative cardiopulmonary complications among Chinese patients with lung cancer | Logistic regression, random forest, and XGBOOST | Three models were developed and validated with AUCs of 0.728, 0.721, and 0.767 for the logistic regression, random forest, and extreme gradient boosting models, respectively |
| Bolourani et al. [21] | To identify risk factors for respiratory failure after pulmonary lobectomy | Random forest | Two ML-based prediction models were generated and optimized. The first model, with an accuracy of 99.7% and specificity of 75%, was suited for performance evaluation, while the second model, with an accuracy of 94.4% and sensitivity of 83.3%, was built for clinical decision making |
| Chang YJ et al. [22] | Predicting whether patients could be weaned immediately from ventilator after lung resection surgery | Naïve Bayes | The AI model with the Naïve Bayes Classifier algorithm had the best testing results with an accuracy of 0.845, sensitivity of 0.870, and specificity of 0.838 |
| Lee HA et al. [25] | To evaluate the usefulness of an ML model in estimating VO2max in patients requiring lung resection surgery with limited exercise capacity or when a CPET is not possible | Quadratic regression model | This model provides a closer estimation of VO2max values measured using a CPET than other existing equations (bias: −0.33 mL·kg−1·min−1) |
4. Predictors of Histological Tumor Characteristics
Spread through Air Spaces
5. Surgical Planning
5.1. 3D Reconstruction Models
5.2. Virtual Reality
6. Future Applications and Limitations
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lung Cancer Incidence Statistics. Available online: https://www.cancerresearchuk.org/health-professional/cancer-statistics/statistics-by-cancer-type/lung-cancer/incidence#heading-One (accessed on 20 December 2023).
- Ouchi, Y.; Rakugi, H.; Arai, H.; Akishita, M.; Ito, H.; Toba, K.; Kai, I. Redefining the elderly as aged 75 years and older: Proposal from the Joint Committee of Japan Gerontological Society and the Japan Geriatrics Society. Geriatr. Gerontol. Int. 2017, 17, 1045–1047. [Google Scholar] [CrossRef]
- Nakao, M.; Ichinose, J.; Matsuura, Y.; Okumura, S.; Mun, M. Outcomes after thoracoscopic surgery in octogenarian patients with clinical N0 non-small-cell lung cancer. Jpn. J. Clin. Oncol. 2020, 50, 926–932. [Google Scholar] [CrossRef] [PubMed]
- Spaggiari, L.; Petrella, F.; Maione, P.; Gridelli, C. Lung cancer resection in octogenarian patients. J. Thorac. Dis. 2018, 10 (Suppl. S17), S1995–S1997. [Google Scholar] [CrossRef] [PubMed]
- Saftic, I.; Bille, A.; Asemota, N.; de la Vega, L.B.; Routledge, T.; King, J.; Phipps, K.H.; Pilling, J. Risks and rewards of the surgical treatment of lung cancer in octogenarians. Interact. Cardiovasc. Thorac. Surg. 2021, 33, 905–912. [Google Scholar] [CrossRef] [PubMed]
- Lou, X.; Sanders, A.; Wagh, K.; Binongo, J.N.; Sancheti, M.; Javidfar, J.; Pickens, A.; Fernandez, F.; Force, S.; Khullar, O. Safety and Feasibility of Thoracoscopic Lung Resection for Non-Small-Cell Lung Cancer in Octogenarians. Innovations 2021, 16, 68–74. [Google Scholar] [CrossRef] [PubMed]
- Esteva, A.; Robicquet, A.; Ramsundar, B.; Kuleshov, V.; DePristo, M.; Chou, K.; Cui, C.; Corrado, G.; Thrun, S.; Dean, J. A guide to deep learning in healthcare. Nat. Med. 2019, 25, 24–29. [Google Scholar] [CrossRef] [PubMed]
- Joshi, G.; Jain, A.; Araveeti, S.R.; Adhikari, S.; Garg, H.; Bhandari, M. FDA-Approved Artificial Intelligence and Machine Learning (AI/ML)-Enabled Medical Devices: An Updated Landscape. Electronics 2024, 13, 498. [Google Scholar] [CrossRef]
- Xing, W.; Gao, W.; Lv, X.; Zhao, Z.; Xu, X.; Wu, Z.; Mao, G.; Chen, J. Artificial intelligence predicts lung cancer radiotherapy response: A meta-analysis. Artif. Intell. Med. 2023, 142, 102585. [Google Scholar] [CrossRef] [PubMed]
- Dacic, S.; Travis, W.D.; Giltnane, J.M.; Kos, F.; Abel, J.; Hilz, S.; Fujimoto, J.; Sholl, L.; Ritter, J.; Khalil, F.; et al. Artificial intelligence-powered assessment of pathologic response to neoadjuvant atezolizumab in patients with non-small cell lung cancer: Results from the LCMC3 study. J. Thorac. Oncol. 2023, in press. [CrossRef]
- Abadia, A.F.; Yacoub, B.; Stringer, N.B.; Snoddy, M.B.; Kocher, M.; Schoepf, U.J.; Aquino, G.J.; Kabakus, I.; Dargis, D.B.; Hoelzer, P.; et al. Diagnostic Accuracy and Performance of Artificial Intelligence in Detecting Lung Nodules in Patients with Complex Lung Disease: A Noninferiority Study. J. Thorac. Imaging 2022, 37, 154–161. [Google Scholar] [CrossRef]
- Morgan, H.; Baldwin, D.; Hubbard, R.; Navani, N.; West, D.; O’Dowd, E.L. Ninety-day mortality following lung cancer surgery: Outcomes from the English national clinical outcomes audit. Thorax 2022, 77, 724–726. [Google Scholar] [CrossRef]
- Voltolini, L.; Rapicetta, C.; Ligabue, T.; Luzzi, L.; Scala, V.; Gotti, G. Short- and long-term results of lung resection for cancer in octogenarians. Asian Cardiovasc. Thorac. Ann. 2009, 17, 147–152. [Google Scholar] [CrossRef]
- Dell’amore, A.; Monteverde, M.; Martucci, N.; Sanna, S.; Caroli, G.; Dolci, G.; Dell’amore, D.; Rocco, G. Lobar and sub-lobar lung resection in octogenarians with early stage non-small cell lung cancer: Factors affecting surgical outcomes and long-term results. Gen. Thorac. Cardiovasc. Surg. 2015, 63, 222–230. [Google Scholar] [CrossRef]
- Souza, R.V.; Bassi, M.; Mantovani, S.; Poggi, C.; Diso, D.; Vannucci, J.; Pagini, A.; Amore, D.; Venuta, F.; Anile, M. Comparison of preoperative scores predicting outcome in elderly undergoing lung malignancies resection. J. Thorac. Dis. 2020, 12, 7083–7088. [Google Scholar] [CrossRef]
- Berry, M.F.; Onaitis, M.W.; Tong, B.C.; Harpole, D.H.; DAmico, T.A. A model for morbidity after lung resection in octogenarians. Eur. J. Cardiothorac. Surg. 2011, 39, 989–994. [Google Scholar] [CrossRef] [PubMed]
- Bassi, M.; Vannucci, J.; Giorgi, F.M.; Vaz Souza, R.; Ferrante, F.; Bianco, M.; Mottola, E.; De Giacomo, T.; Diso, D.; Poggi, C.; et al. Lung cancer surgery in octogenarians: A meta-analysis of predictors for postoperative complications. Shanghai Chest 2023, 7, 14. [Google Scholar] [CrossRef]
- Bihorac, A.; Ozrazgat-Baslanti, T.; Ebadi, A.; Motaei, A.; Madkour, M.; Pardalos, P.M.; Lipori, G.; Hogan, W.R.; Efron, P.A.; Moore, F.; et al. MySurgeryRisk: Development and Validation of a Machine-learning Risk Algorithm for Major Complications and Death After Surgery. Ann. Surg. 2019, 269, 652–662. [Google Scholar] [CrossRef] [PubMed]
- Salati, M.; Migliorelli, L.; Moccia, S.; Andolfi, M.; Roncon, A.; Guiducci, G.M.; Xiumè, F.; Tiberi, M.; Frontoni, E.; Refai, M. A Machine Learning Approach for Postoperative Outcome Prediction: Surgical Data Science Application in a Thoracic Surgery Setting. World J. Surg. 2021, 45, 1585–1594. [Google Scholar] [CrossRef] [PubMed]
- Huang, G.; Liu, L.; Wang, L.; Li, S. Prediction of postoperative cardiopulmonary complications after lung resection in a Chinese population: A machine learning-based study. Front. Oncol. 2022, 12, 1003722. [Google Scholar] [CrossRef]
- Bolourani, S.; Wang, P.; Patel, V.M.; Manetta, F.; Lee, P.C. Predicting respiratory failure after pulmonary lobectomy using machine learning techniques. Surgery 2020, 168, 743–752. [Google Scholar] [CrossRef]
- Chang, Y.-J.; Hung, K.-C.; Wang, L.-K.; Yu, C.-H.; Chen, C.-K.; Tay, H.-T.; Wang, J.-J.; Liu, C.-F. A Real-Time Artificial Intelligence-Assisted System to Predict Weaning from Ventilator Immediately after Lung Resection Surgery. Int. J. Environ. Res. Public. Health. 2021, 18, 2713. [Google Scholar] [CrossRef]
- Brunelli, A.; Cicconi, S.; Decaluwe, H.; Szanto, Z.; Falcoz, P.E. Parsimonious Eurolung risk models to predict cardiopulmonary morbidity and mortality following anatomic lung resections: An updated analysis from the European Society of Thoracic Surgeons database. Eur. J. Cardiothorac. Surg. 2020, 57, 455–461. [Google Scholar] [CrossRef] [PubMed]
- Li, S.; Chen, Z.; Yan, W. Application of bedside ultrasound in predicting the outcome of weaning from mechanical ventilation in elderly patients. BMC Pulm. Med. 2021, 21, 217. [Google Scholar] [CrossRef]
- Lee, H.A.; Yu, W.; Choi, J.D.; Lee, Y.-S.; Park, J.W.; Jung, Y.J.; Sheen, S.S.; Jung, J.; Haam, S.; Kim, S.H.; et al. Development of Machine Learning Model for VO2max Estimation Using a Patch-Type Single-Lead ECG Monitoring Device in Lung Resection Candidates. Healthcare 2023, 11, 2863. [Google Scholar] [CrossRef]
- Chang, G.-C.; Chiu, C.-H.; Yu, C.-J.; Chang, Y.-C.; Chang, Y.-H.; Hsu, K.-H.; Wu, Y.-C.; Chen, C.-Y.; Hsu, H.-H.; Wu, M.-T.; et al. Low-dose CT screening among never-smokers with or without a family history of lung cancer in Taiwan: A prospective cohort study. Lancet Respir. Med. 2023, 12, 141–152. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.C.; Machac, J.; Krynyckyi, B.R.; Knesaurek, K.; Krellenstein, D.; Schultz, B.; Gribetz, A.; DePalo, L.; Teirstein, A.; Kim, C.K. Fluoro-deoxy-glucose positron emission tomography for evaluation of indeterminate lung nodules: Assigning a probability of malignancy may be preferable to binary readings. Ann. Nucl. Med. 2008, 22, 165–170, Correction in Ann. Nucl. Med. 2010, 24, 231. [Google Scholar] [CrossRef]
- Elia, S.; Pompeo, E.; Santone, A.; Rigoli, R.; Chiocchi, M.; Patirelis, A.; Mercaldo, F.; Mancuso, L.; Brunese, L. Radiomics and Artificial Intelligence Can Predict Malignancy of Solitary Pulmonary Nodules in the Elderly. Diagnostics 2023, 13, 384. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.; Wu, S. Identifying Lung Cancer Risk Factors in the Elderly Using Deep Neural Networks: Quantitative Analysis of Web-Based Survey Data. J. Med. Internet Res. 2020, 22, e17695. [Google Scholar] [CrossRef]
- Zhang, L.; Zeng, B.; Liu, J.; Lin, H.; Lei, P.; Fan, B.; Xu, R. Application Potential of Radiomics based on the Unenhanced CT Image for the Identification of Benign or Malignant Pulmonary Nodules. Curr. Med. Imaging 2024, 20, e15734056246425. [Google Scholar] [CrossRef]
- Hendrix, W.; Hendrix, N.; Scholten, E.T.; Mourits, M.; Jong, J.T.-D.; Schalekamp, S.; Korst, M.; van Leuken, M.; van Ginneken, B.; Prokop, M.; et al. Deep learning for the detection of benign and malignant pulmonary nodules in non-screening chest CT scans. Commun. Med. 2023, 3, 156. [Google Scholar] [CrossRef]
- Mantovani, S.; Pernazza, A.; Bassi, M.; Amore, D.; Vannucci, J.; Poggi, C.; Diso, D.; D’amati, G.; Della Rocca, C.; Rendina, E.A.; et al. Prognostic impact of spread through air spaces in lung adenocarcinoma. Interact. Cardiovasc. Thorac. Surg. 2022, 34, 1011–1015. [Google Scholar] [CrossRef] [PubMed]
- Chae, M.; Jeon, J.H.; Chung, J.-H.; Lee, S.Y.; Hwang, W.J.; Jung, W.; Hwang, Y.; Cho, S.; Kim, K.; Jheon, S. Prognostic significance of tumor spread through air spaces in patients with stage IA part-solid lung adenocarcinoma after sublobar resection. Lung Cancer 2021, 152, 21–26. [Google Scholar] [CrossRef] [PubMed]
- Anile, M.; Poggi, C.; Diso, D.; Mantovani, S.; Bassi, M.; Rendina, E.A.; Venuta, F. Do the right thing! J. Thorac. Dis. 2019, 11 (Suppl. S3), S266–S267. [Google Scholar] [CrossRef] [PubMed]
- Jin, W.; Shen, L.; Tian, Y.; Zhu, H.; Zou, N.; Zhang, M.; Chen, Q.; Dong, C.; Yang, Q.; Jiang, L.; et al. Improving the prediction of Spreading Through Air Spaces (STAS) in primary lung cancer with a dynamic dual-delta hybrid machine learning model: A multicenter cohort study. Biomark. Res. 2023, 11, 102. [Google Scholar] [CrossRef] [PubMed]
- Lin, M.-W.; Chen, L.-W.; Yang, S.-M.; Hsieh, M.-S.; Ou, D.-X.; Lee, Y.-H.; Chen, J.-S.; Chang, Y.-C.; Chen, C.-M. CT-Based Deep-Learning Model for Spread-Through-Air-Spaces Prediction in Ground Glass-Predominant Lung Adenocarcinoma. Ann. Surg. Oncol. 2023, 31, 1536–1545. [Google Scholar] [CrossRef]
- Han, X.; Fan, J.; Zheng, Y.; Ding, C.; Zhang, X.; Zhang, K.; Wang, N.; Jia, X.; Li, Y.; Liu, J.; et al. The Value of CT-Based Radiomics for Predicting Spread Through Air Spaces in Stage IA Lung Adenocarcinoma. Front. Oncol. 2022, 12, 757389. [Google Scholar] [CrossRef] [PubMed]
- Tao, J.; Liang, C.; Yin, K.; Fang, J.; Chen, B.; Wang, Z.; Lan, X.; Zhang, J. 3D convolutional neural network model from contrast-enhanced CT to predict spread through air spaces in non-small cell lung cancer. Diagn. Interv. Imaging 2022, 103, 535–544. [Google Scholar] [CrossRef] [PubMed]
- Bassi, M.; Russomando, A.; Vannucci, J.; Ciardiello, A.; Dolciami, M.; Ricci, P.; Pernazza, A.; D’amati, G.; Terracciano, C.M.; Faccini, R.; et al. Role of radiomics in predicting lung cancer spread through air spaces in a heterogeneous dataset. Transl. Lung Cancer Res. 2022, 11, 560–571. [Google Scholar] [CrossRef] [PubMed]
- Chen, D.; She, Y.; Wang, T.; Xie, H.; Li, J.; Jiang, G.; Chen, Y.; Zhang, L.; Xie, D.; Chen, C. Radiomics-based prediction for tumour spread through air spaces in stage I lung adenocarcinoma using machine learning. Eur. J. Cardiothorac. Surg. 2020, 58, 51–58. [Google Scholar] [CrossRef]
- Wang, F.; Pan, X.; Zhang, T.; Zhong, Y.; Wang, C.; Li, H.; Wang, J.; Guo, L.; Yuan, M. Predicting visceral pleural invasion in lung adenocarcinoma presenting as part-solid density utilizing a nomogram model combined with radiomics and clinical features. Thorac. Cancer. 2023, 15, 23–34. [Google Scholar] [CrossRef]
- Gong, J.; Fu, F.; Ma, X.; Wang, T.; Ma, X.; You, C.; Zhang, Y.; Peng, W.; Chen, H.; Gu, Y. Hybrid deep multi-task learning radiomics approach for predicting EGFR mutation status of non-small cell lung cancer in CT images. Phys. Med. Biol. 2023, 68, 245021. [Google Scholar] [CrossRef] [PubMed]
- Bracci, S.; Dolciami, M.; Trobiani, C.; Izzo, A.; Pernazza, A.; D’amati, G.; Manganaro, L.; Ricci, P. Quantitative CT texture analysis in predicting PD-L1 expression in locally advanced or metastatic NSCLC patients. Radiol. Med. 2021, 126, 1425–1433. [Google Scholar] [CrossRef] [PubMed]
- Betancourt, M.C.; Araújo, C.; Marín, S.; Buriticá, W. The Quantitative Impact of Using 3D Printed Anatomical Models for Surgical Planning Optimization: Literature Review. 3D Print. Addit. Manuf. 2023, 10, 1130–1139. [Google Scholar] [CrossRef] [PubMed]
- Vervoorn, M.T.; Wulfse, M.; Mohamed Hoesein, F.A.A.; Stellingwerf, M.; van der Kaaij, N.P.; de Heer, L.M. Application of three-dimensional computed tomography imaging and reconstructive techniques in lung surgery: A mini-review. Front. Surg. 2022, 9, 1079857. [Google Scholar] [CrossRef] [PubMed]
- Gossot, D.; Seguin-Givelet, A. Anatomical variations and pitfalls to know during thoracoscopic segmentectomies. J. Thorac. Dis. 2018, 10 (Suppl. S10), S1134–S1144. [Google Scholar] [CrossRef] [PubMed]
- Wu, Z.; Huang, Z.; Qin, Y.; Jiao, W. Progress in three-dimensional computed tomography reconstruction in anatomic pulmonary segmentectomy. Thorac. Cancer 2022, 13, 1881–1887. [Google Scholar] [CrossRef]
- Sardari Nia, P.; Olsthoorn, J.R.; Heuts, S.; Maessen, J.G. Interactive 3D Reconstruction of Pulmonary Anatomy for Preoperative Planning, Virtual Simulation, and Intraoperative Guiding in Video-Assisted Thoracoscopic Lung Surgery. Innovations 2019, 14, 17–26. [Google Scholar] [CrossRef] [PubMed]
- Yu, H.; Li, J.; Zhang, L.; Cao, Y.; Yu, X.; Sun, J. Design of lung nodules segmentation and recognition algorithm based on deep learning. BMC Bioinform. 2021, 22 (Suppl. S5), 314. [Google Scholar] [CrossRef]
- Lancaster, H.L.; Zheng, S.; Aleshina, O.O.; Yu, D.; Chernina, V.Y.; Heuvelmans, M.A.; de Bock, G.H.; Dorrius, M.D.; Gratama, J.W.; Morozov, S.P.; et al. Outstanding negative prediction performance of solid pulmonary nodule volume AI for ultra-LDCT baseline lung cancer screening risk stratification. Lung Cancer 2022, 165, 133–140. [Google Scholar] [CrossRef]
- Li, L.; Liu, Z.; Huang, H.; Lin, M.; Luo, D. Evaluating the performance of a deep learning-based computer-aided diagnosis (DL-CAD) system for detecting and characterizing lung nodules: Comparison with the performance of double reading by radiologists. Thorac. Cancer 2019, 10, 183–192. [Google Scholar] [CrossRef]
- Zhi, L.; Jiang, W.; Zhang, S.; Zhou, T. Deep neural network pulmonary nodule segmentation methods for CT images: Literature review and experimental comparisons. Comput. Biol. Med. 2023, 164, 107321. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Wang, Z.; Qi, Q.; Zhang, K.; Sui, X.; Wang, X.; Weng, W.; Wang, S.; Zhao, H.; Sun, C.; et al. A fully automated noncontrast CT 3-D reconstruction algorithm enabled accurate anatomical demonstration for lung segmentectomy. Thorac. Cancer 2022, 13, 795–803. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Xu, H.; Qi, Q.; Sun, C.; Jin, J.; Zhao, H.; Wang, X.; Weng, W.; Wang, S.; Sui, X.; et al. AI-based chest CT semantic segmentation algorithm enables semi-automated lung cancer surgery planning by recognizing anatomical variants of pulmonary vessels. Front. Oncol. 2022, 12, 1021084. [Google Scholar] [CrossRef] [PubMed]
- Chan, E.G.; Landreneau, J.R.; Schuchert, M.J.; Odell, D.D.; Gu, S.; Pu, J.; Luketich, J.D.; Landreneau, R.J. Preoperative (3-dimensional) computed tomography lung reconstruction before anatomic segmentectomy or lobectomy for stage I non-small cell lung cancer. J. Thorac. Cardiovasc. Surg. 2015, 150, 523–528. [Google Scholar] [CrossRef] [PubMed]
- Nardelli, P.; Jimenez-Carretero, D.; Bermejo-Pelaez, D.; Washko, G.R.; Rahaghi, F.N.; Ledesma-Carbayo, M.J.; Estepar, R.S.J. Pulmonary Artery-Vein Classification in CT Images Using Deep Learning. IEEE Trans. Med. Imaging 2018, 37, 2428–2440. [Google Scholar] [CrossRef] [PubMed]
- Charbonnier, J.P.; Brink, M.; Ciompi, F.; Scholten, E.T.; Schaefer-Prokop, C.M.; Van Rikxoort, E.M. Automatic pulmonary artery-vein separation and classification in computed tomography using tree partitioning and peripheral vessel matching. IEEE Trans. Med. Imaging 2016, 35, 882–892. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.; Liu, X.; Ni, L. Analysis of pulmonary nodules detected by annual low-dose computed tomography in the elderly during a 10-year follow-up. Geriatr. Gerontol. Int. 2022, 22, 865–869. [Google Scholar] [CrossRef] [PubMed]
- Copley, S.J.; Wells, A.U.; Hawtin, K.E.; Gibson, D.J.; Hodson, J.M.; Jacques, A.E.T.; Hansell, D.M. Lung morphology in the elderly: Comparative CT study of subjects over 75 years old versus those under 55 years old. Radiology 2009, 251, 566–573. [Google Scholar] [CrossRef] [PubMed]
- Gossner, J.; Nau, R. Geriatric chest imaging: When and how to image the elderly lung, age-related changes, and common pathologies. Radiol. Res. Pract. 2013, 2013, 584793. [Google Scholar] [CrossRef]
- Frajhof, L.; Borges, J.; Hoffmann, E.; Lopes, J.; Haddad, R. Virtual reality, mixed reality and augmented reality in surgical planning for video or robotically assisted thoracoscopic anatomic resections for treatment of lung cancer. J. Vis. Surg. 2018, 4, 143. [Google Scholar] [CrossRef]
- Perkins, S.L.; Krajancich, B.; Yang, C.J.; Hargreaves, B.A.; Daniel, B.L.; Berry, M.F. A Patient-Specific Mixed-Reality Visualization Tool for Thoracic Surgical Planning. Ann. Thorac. Surg. 2020, 110, 290–295. [Google Scholar] [CrossRef]
- Tokuno, J.; Chen-Yoshikawa, T.F.; Nakao, M.; Matsuda, T.; Date, H. Resection Process Map: A novel dynamic simulation system for pulmonary resection. J. Thorac. Cardiovasc. Surg. 2020, 159, 1130–1138. [Google Scholar] [CrossRef] [PubMed]
- Ujiie, H.; Yamaguchi, A.; Gregor, A.; Chan, H.; Kato, T.; Hida, Y.; Kaga, K.; Wakasa, S.; Eitel, C.; Clapp, T.R.; et al. Developing a virtual reality simulation system for preoperative planning of thoracoscopic thoracic surgery. J. Thorac. Dis. 2021, 13, 778–783. [Google Scholar] [CrossRef] [PubMed]
- Sadeghi, A.H.; Maat, A.P.M.; Taverne, Y.J.J.; Cornelissen, R.; Dingemans, A.-M.C.; Bogers, A.J.C.; Mahtab, E.A. Virtual reality and artificial intelligence for 3-dimensional planning of lung segmentectomies. JTCVS Tech. 2021, 7, 309–321. [Google Scholar] [CrossRef] [PubMed]
- Bakhuis, W.; Sadeghi, A.H.; Moes, I.; Maat, A.P.; Siregar, S.; Bogers, A.J.; Mahtab, E.A. Essential Surgical Plan Modifications After Virtual Reality Planning in 50 Consecutive Segmentectomies. Ann. Thorac. Surg. 2023, 115, 1247–1255. [Google Scholar] [CrossRef] [PubMed]
- Bellini, V.; Valente, M.; Del Rio, P.; Bignami, E. Artificial intelligence in thoracic surgery: A narrative review. J. Thorac. Dis. 2021, 13, 6963–6975. [Google Scholar] [CrossRef]
- De Margerie-Mellon, C.; Chassagnon, G. Artificial intelligence: A critical review of applications for lung nodule and lung cancer. Diagn. Interv. Imaging 2023, 104, 11–17. [Google Scholar] [CrossRef]

| Author | Objective | Models | Main Results |
|---|---|---|---|
| Jin W et al. [35] | To develop and validate a dual-delta deep learning and radiomics model based on pretreatment computed tomography (CT) image series to predict the STAS in patients with lung cancer | Multiple machine learning model | The dual-delta model showed satisfactory discrimination between STAS and non-STAS with an AUC of 0.94 in the internal cohort and 0.84 and 0.84 in two external validation cohorts |
| Lin MW et al. [36] | To develop a STAS deep learning (STAS-DL) prediction model in lung adenocarcinoma with tumors smaller than 3 cm and a consolidation-to-tumor (C/T) ratio less than 0.5 | Deep learning model (STAS-DL) and radiomics-based model | The proposed STAS-DL yielded the best performance with an AUC of 0.82 and an accuracy of 74%, and it was superior to the physicians with an AUC of 0.68. Moreover, STAS-DL achieved the highest standardized net benefit compared with the other methods |
| Han X et al. [37] | To develop and validate a CT-based radiomics model for predicting STAS in stage IA lung adenocarcinoma | Clinical/CT model, radiomics-based model and MixModel | The radiomics model achieved good performance with an AUC of 0.812 in the training set and 0.850 in the test set. The MixModel showed AUCs of 0.822 and 0.865 in the training and test cohorts, respectively |
| Tao J et al. [38] | To compare the efficacy of five noninvasive models, including a three-dimensional (3D) convolutional neural network (CNN) model, to predict STAS in NSCLC, and to obtain the best prediction model to provide a basis for clinical surgery planning | Clinicopathological/CT model, conventional radiomics model, computer vision model, 3D CNN model, and combined model | For predicting STAS, the 3D CNN model was superior to the others achieving an AUC of 0.93 (95% CI: 0.70–0.82) in the training cohort and 0.80 (95% CI: 0.65–0.86) in the validation cohort |
| Bassi M et al. [39] | To test a radiomics-based prediction model of STAS in a heterogeneous CT dataset, applicable to daily clinical practice | Radiological model, radiomics-based model, and mixed model | Radiomics, radiological, and mixed radiomics-radiological models reached an accuracy of 0.66 ± 0.02 after internal validation. In external validation, the best model was the mixed model with 0.78 accuracy, 0.89 sensitivity, 0.64 specificity and an AUC of 0.79 |
| Chen D et al. [40] | To assess the value of radiomics in predicting STAS in stage I lung adenocarcinoma | Radiomics model | The model exhibited good performance with an AUC of 0.63 (CI 0.55–0.71) in internal validation and 0.69 in external validation |
| Author | Objective | N Patients | AI-VR Tool | Results |
|---|---|---|---|---|
| Sardari Nia P et al. [48] | To demonstrate the feasibility of interactive 3D CT reconstructions for preoperative planning and intraoperative guiding in video-assisted thoracoscopic lung surgery | 25 | Three-dimensional intraoperative vision of CT reconstruction of the pulmonary anatomy | Preoperative 3D reconstruction of pulmonary vessels corresponded with the intraoperative findings in all patients, revealing anatomic variations in 4 (15.4%) patients. This contributed to the safety and accuracy of anatomic resections |
| Frajhof L et al. [61] | To develop a platform that allows for seeing, manipulating, and rotating anatomic models in full 3D dynamic reproduction before the surgical procedure for improving decision making and surgical planning | Case report | VR MR AR | Display of patient’s 3D data through VR, MR, and AR is a useful tool for surgical planning by providing the surgeon with a true and spatially accurate representation of the patient’s anatomy |
| Perkins SL et al. [62] | To facilitate noninvasive lung nodule localization by using 3D mixed-reality visualization technology | 3 | MR | Mixed-reality visualization during surgical planning may facilitate accurate and rapid identification of small lung lesions during minimally invasive surgeries and reduce the need for additional invasive preoperative localization procedures |
| Tokuno J et al. [63] | To develop a novel simulation system that generates dynamic images based on patient-specific computed tomography data | 18 | Resection Process Map (original software) | The Resection Process Map accurately delineated 98.6% of vessel branches and all the bronchi, generating a virtual dynamic image for each patient reflecting the intraoperative deformation of the lung. The median time required to obtain the images was 121.3 s |
| Ujiie H et al. [64] | To investigate the potential utility of this VR simulation system in both preoperative planning and intraoperative assistance | Case report | VR surgical navigation system using a head-mounted display. | The VR software with the use of the head-mounted display allowed surgeons to visualize and interact with real patient data in true 3D, providing a unique perspective |
| Sadeghi AH et al. [65] | First dedicated artificial intelligence-based and immersive 3D VR platform for preoperative planning of video-assisted thoracoscopic segmentectomies | 10 | PulmoVR (3D VR software) | Potential benefit of additional VR-guided planning for video-assisted thoracoscopic segmentectomies. In 40% of the cases, the surgical strategy was adjusted due to the 3-dimensional VR-based evaluation of anatomy |
| Bakhuis W et al. [66] | To investigate the added clinical value of PulmoVR for preoperative planning in pulmonary segmentectomy | 50 | PulmoVR (3D VR software) | The surgical plan was adjusted in 52%; the tumor was localized in a different segment in 14%; more lung-sparing resection was planned in 10%; and extended segmentectomy, including 1 lobectomy, was performed in 28% of cases after VR evaluation |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bassi, M.; Vaz Sousa, R.; Zacchini, B.; Centofanti, A.; Ferrante, F.; Poggi, C.; Carillo, C.; Pecoraro, Y.; Amore, D.; Diso, D.; et al. Lung Cancer Surgery in Octogenarians: Implications and Advantages of Artificial Intelligence in the Preoperative Assessment. Healthcare 2024, 12, 803. https://doi.org/10.3390/healthcare12070803
Bassi M, Vaz Sousa R, Zacchini B, Centofanti A, Ferrante F, Poggi C, Carillo C, Pecoraro Y, Amore D, Diso D, et al. Lung Cancer Surgery in Octogenarians: Implications and Advantages of Artificial Intelligence in the Preoperative Assessment. Healthcare. 2024; 12(7):803. https://doi.org/10.3390/healthcare12070803
Chicago/Turabian StyleBassi, Massimiliano, Rita Vaz Sousa, Beatrice Zacchini, Anastasia Centofanti, Francesco Ferrante, Camilla Poggi, Carolina Carillo, Ylenia Pecoraro, Davide Amore, Daniele Diso, and et al. 2024. "Lung Cancer Surgery in Octogenarians: Implications and Advantages of Artificial Intelligence in the Preoperative Assessment" Healthcare 12, no. 7: 803. https://doi.org/10.3390/healthcare12070803
APA StyleBassi, M., Vaz Sousa, R., Zacchini, B., Centofanti, A., Ferrante, F., Poggi, C., Carillo, C., Pecoraro, Y., Amore, D., Diso, D., Anile, M., De Giacomo, T., Venuta, F., & Vannucci, J. (2024). Lung Cancer Surgery in Octogenarians: Implications and Advantages of Artificial Intelligence in the Preoperative Assessment. Healthcare, 12(7), 803. https://doi.org/10.3390/healthcare12070803