
Knee Arthrodesis for Periprosthetic Knee Infection: Fusion Rate, Complications, and Limb Salvage—A Systematic Review

 ,
,  , ,
, ,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
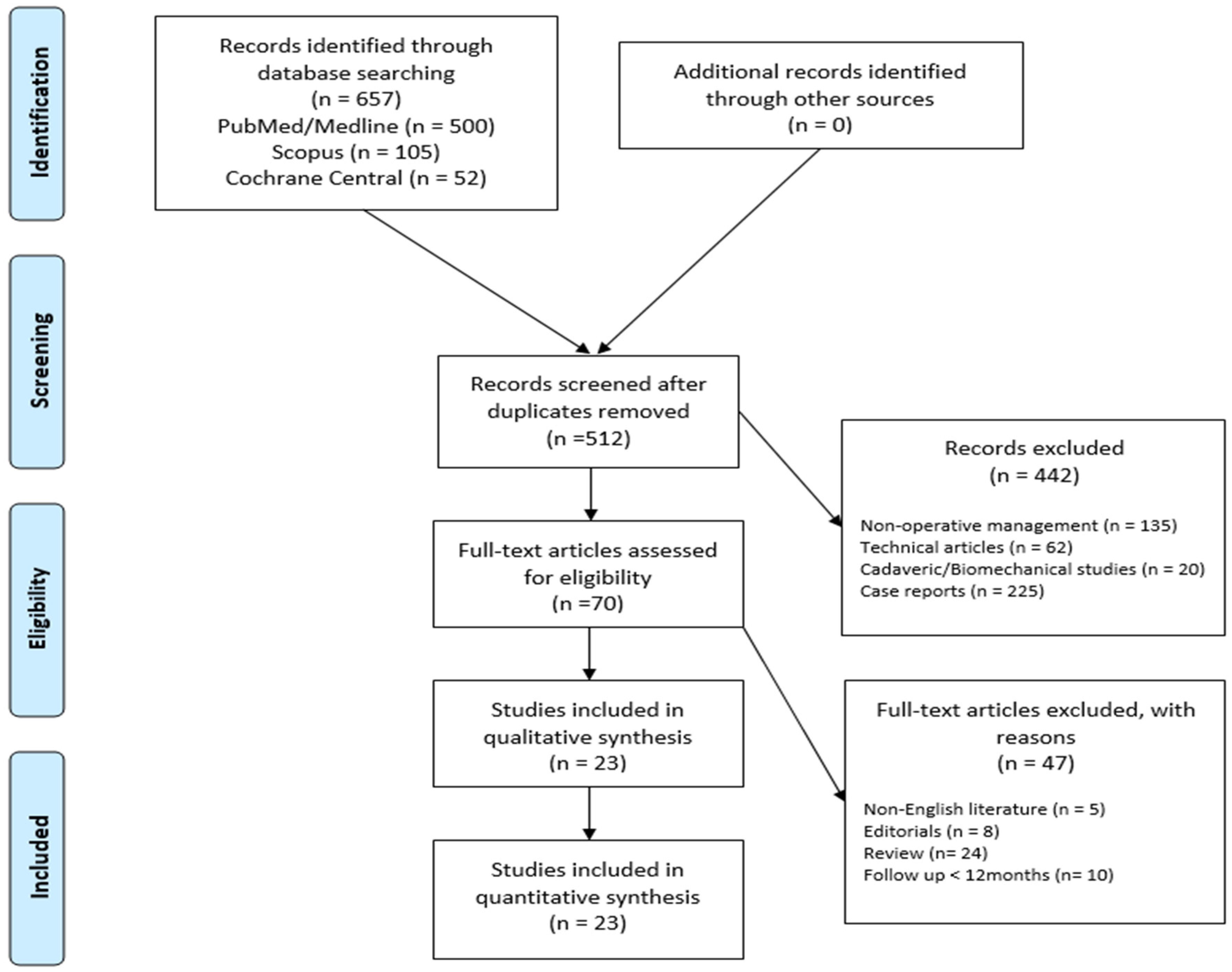
2.1. Search Strategy
2.2. Inclusion Criteria and Study Selection
2.3. Data Extraction and Quality Assessment
2.4. Statistical Analysis
3. Results

{kind=link}
| Author | Journal | Year of Publication | Years of Study | Type of Surgery | Patient Demographics | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Number of Patients (N) | Sex (N) | Age (years) | Time between TKA and Treatment (months) | FU (months) | ||||||||||||
| M | F | Mean | SD | Range | Mean | SD | Range | Mean | SD | Range | ||||||
| Aparicio et al. [31] | Indian Journal of Orthopaedics | 2020 | 2001–2019 | IMN | 45 | 13 | 32 | 72 | 8.3 | 57–90 | 55 | 57 | 12–240 | 102 | 45.5 | 24–206 |
| Balci et al. [14] | Journal of Knee Surgery | 2015 | 1999–2012 | EF | 17 | 14 | 3 | 67 | 16.6 | 29–93 | 6.8 | 2.4 | 5.6–8 | 62.96 | 34 | 24–160 |
| Brown et al. [33] | Journal of the American Academy of Orthopaedic Surgeons | 2020 | 2004–2013 | IMN | 17 | 7 | 11 | 65 | 12.8 | 32–83 | NA | NA | NA | 50 | 37 | 2–150 |
| Corona et al. [16] | European Journal of Orthopaedic Surgery & Traumatology | 2020 | 2014–2018 | EF | 29 | 13 | 16 | 77.96 | 7.7 | 39–88 | NA | NA | NA | 47.1 | 17 | 12–82.8 |
| Faure et al. [17] | Orthopaedic & Traumatology: Surgery & Research | 2021 | 2005–2005 | IMN | 31 | 12 | 19 | 67 | 12 | 48–80 | NA | NA | NA | 158 | 6.3 | 138–163 |
| Friedrich et al. [4] | The Knee | 2017 | 2008–2014 | IMN | 32 | NA | NA | 70.2 | 11.5 | 43–89 | NA | NA | NA | 31 | 15.5 | 12–74 |
| Galluser et al. [32] | European Journal of Orthopaedic Surgery & Traumatology | 2015 | 2004–2012 | IMN | 12 | NA | NA | 67 | 11.3 | 42–87 | 2 | 1.2 | 0.5–5.3 | 33 | 31.5 | 6–132 |
| Gathen et al. [3] | Archives of Orthopaedic and Trauma Surgery | 2018 | 2008–2014 | IMN | 36 | 16 | 20 | 69.9 | 10.4 | NA | NA | NA | NA | 34.6 | 17.7 | NA |
| Gramlich et al. [18] | Archives of Orthopaedic and Trauma Surgery | 2021 | 2010–2017 | IMN | 52 | 23 | 29 | 73.9 | 1.6 | 49–97 | NA | NA | NA | 81.6 | 46.5 | 6–192 |
| Hawi et al. [19] | The Bone & Joint Journal | 2015 | 2002–2012 | IMN | 27 | 17 | 10 | 68.8 | 8.8 | 52–87 | NA | NA | NA | 67.1 | 29.8 | 24–143 |
| Iacono et al. [20] | HSS Journal | 2013 | 2001–2009 | IMN | 22 | 15 | 19 | 69.3 | 8 | 53–85 | NA | NA | NA | 34.4 | 1 | 13–17 |
| EF | 12 | 68.5 | 7.3 | 55–84 | NA | NA | NA | 93.2 | 7.3 | 82–111 | ||||||
| Putman et al. [21] | Orthopaedic & Traumatology: Surgery & Research | 2013 | 2005–2008 | IMN | 31 | NA | NA | 67 | 12 | 78–80 | NA | NA | NA | 50 | 22 | 28–90 |
| Razii et al. [8] | European Journal of Orthopaedic Surgery & Traumatology | 2016 | 2003–2014 | IMN | 12 | 9 | 3 | 67 | 13.3 | 35–88 | NA | NA | NA | 48.5 | 27.8 | 9–120 |
| Robinson et al. [22] | Journal of the American Academy of Orthopaedic Surgeons | 2018 | 2002–2014 | IMN/EF | 21 | 9 | 14 | 63.7 | NA | NA | 18.2 | NA | NA | 4.4 | 126 | 12–138 |
| Rohner et al. [23] | The Journal of Bone and Joint Surgery | 2015 | 1997–2013 | IMN | 26 | 8 | 18 | 68 | 10 | 48–88 | NA | NA | NA | NA | NA | NA |
| Stavrakis et al. [15] | Arthroplasty Today | 2022 | 1998–2019 | IMN | 81 | 39 | 42 | 67 | 7.9 | 45–84 | 25 | NA | NA | 52 | NA | NA |
| Suda et al. [24] | International Orthopaedics | 2021 | 2014–2018 | IMN/EF/CP | 152 | 81 | 78 | 63.6 | 19.5 | 12–90 | NA | NA | NA | 36 | 9.25 | 12–49 |
| Troulliez et al. [25] | Orthopaedic & Traumatology: Surgery & Research | 2021 | 2003–2019 | IMN | 23 | 7 | 16 | 68 | 11.1 | 53–81 | 48 | 6.3 | 24–87 | 116.34 | 56.8 | 13.2–171.96 |
| Vivacqua et al. [13] | Revista brasilera de Ortopedia | 2021 | 2010–2016 | EF | 18 | 9 | 9 | NA | NA | NA | NA | NA | NA | 44.4 | NA | NA |
| Watanabe et al. [26] | Modern Rheumatology | 2014 | 2005–2007 | EF | 8 | 1 | 7 | 72.9 | 4.3 | 63–80 | 23.3 | 16.25 | 5–70 | 39 | 2.25 | 36–45 |
| Wilding et al. [27] | The Journal of Arthroplasty | 2016 | 2008–2014 | IMN | 8 | 2 | 6 | 73.8 | 3.9 | 67–82.5 | 78 | 36 | 6–150 | 16 | 7.5 | 5–35 |
| Yeung et al. [28] | The Journal of Arthroplasty | 2020 | 2000–2016 | IMN/EF/CP | 51 | 23 | 28 | 65 | 4.5 | 55–73 | NA | NA | NA | 78 | 99 | 43–142 |
| Zajonz et al. [29] | Der Orthopäde | 2021 | 2010–2016 | IMN | 18 | NA | NA | 76.6 | 5 | 60.6–80.5 | NA | NA | NA | 51 | 18 | 10–82 |
| CP | 7 | NA | NA | 60.6 | 6.3 | 55–80.5 | NA | NA | NA | 28 | 10.5 | 2–44 | ||||
| Comorbidities | N. of Studies | N. of Patients | Prevalence |
|---|---|---|---|
| Diabetes | 11 | 138 | 30% |
| Hypertension | 7 | 209 | 63% |
| Cardiac Disease | 6 | 44 | 13.8% |
| Rheumatoid Arthritis | 9 | 45 | 16.9% |
| Smoke Habits | 3 | 105 | 57.1% |
3.1. Microbiology
3.2. Complications
3.3. Fusion, Reoperation and Amputation Rates
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mercurio, M.; Gasparini, G.; Sanzo, V.; Familiari, F.; Castioni, D.; Galasso, O. Cemented Total Knee Arthroplasty Shows Less Blood Loss but a Higher Rate of Aseptic Loosening Compared With Cementless Fixation: An Updated Meta-Analysis of Comparative Studies. J. Arthroplast. 2022, 37, 1879–1887.e4. [Google Scholar] [CrossRef]
- Mercurio, M.; Gasparini, G.; Galasso, O.; Familiari, F.; Cofano, E.; Sanzo, V.; Ciolli, G.; Corona, K.; Cerciello, S. Lateral versus Medial Approach for Total Knee Arthroplasty for Valgus Knee Deformity Shows Comparable Functional Outcomes, Hip–Knee–Ankle Angle Values, and Complication Rates: A Meta-Analysis of Comparative Studies. Arch. Orthop. Trauma Surg. 2023, 144, 869–878. [Google Scholar] [CrossRef]
- Gathen, M.; Wimmer, M.D.; Ploeger, M.M.; Weinhold, L.; Schmid, M.; Wirtz, D.C.; Gravius, S.; Friedrich, M.J. Comparison of Two-Stage Revision Arthroplasty and Intramedullary Arthrodesis in Patients with Failed Infected Knee Arthroplasty. Arch. Orthop. Trauma Surg. 2018, 138, 1443–1452. [Google Scholar] [CrossRef]
- Friedrich, M.J.; Schmolders, J.; Wimmer, M.D.; Strauss, A.C.; Ploeger, M.M.; Wirtz, D.C.; Gravius, S.; Randau, T.M. Two-Stage Knee Arthrodesis with a Modular Intramedullary Nail Due to Septic Failure of Revision Total Knee Arthroplasty with Extensor Mechanism Deficiency. Knee 2017, 24, 1240–1246. [Google Scholar] [CrossRef] [PubMed]
- Vasso, M.; Schiavone Panni, A.; De Martino, I.; Gasparini, G. Prosthetic Knee Infection by Resistant Bacteria: The Worst-Case Scenario. Knee Surg. Sports Traumatol. Arthrosc. 2016, 24, 3140–3146. [Google Scholar] [CrossRef]
- Makhdom, A.M.; Fragomen, A.; Rozbruch, S.R. Knee Arthrodesis After Failed Total Knee Arthroplasty. J. Bone Jt. Surg. 2019, 101, 650–660. [Google Scholar] [CrossRef]
- White, C.J.; Palmer, A.J.R.; Rodriguez-Merchan, E.C. External Fixation vs. Intramedullary Nailing for Knee Arthrodesis After Failed Infected Total Knee Arthroplasty: A Systematic Review and Meta-Analysis. J. Arthroplast. 2018, 33, 1288–1295. [Google Scholar] [CrossRef]
- Razii, N.; Abbas, A.M.I.; Kakar, R.; Agarwal, S.; Morgan-Jones, R. Knee Arthrodesis with a Long Intramedullary Nail as Limb Salvage for Complex Periprosthetic Infections. Eur. J. Orthop. Surg. Traumatol. 2016, 26, 907–914. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred Reporting Items for Systematic Reviews and Meta-analyses: The PRISMA Statement. Ann. Intern. Med. 2009, 151, 264–269. [Google Scholar] [CrossRef]
- Schardt, C.; Adams, M.B.; Owens, T.; Keitz, S.; Fontelo, P. Utilization of the PICO Framework to Improve Searching PubMed for Clinical Questions. BMC Med. Inform. Decis. Mak. 2007, 7, 16. [Google Scholar] [CrossRef]
- Mercurio, M.; Castioni, D.; Cosentino, O.; Familiari, F.; Iannò, B.; Gasparini, G.; Galasso, O. Revision Surgery for Periprosthetic Elbow Infection: Eradication Rate, Complications, and Functional Outcomes-a Systematic Review. Arch. Orthop. Trauma Surg. 2023, 143, 1117–1131. [Google Scholar] [CrossRef] [PubMed]
- Ottawa Hospital Research Institute. Available online: https://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 22 February 2024).
- Vivacqua, T.; Moraes, R.; Barretto, J.; Cavanelas, N.; Albuquerque, R.; Mozella, A. Resultado Funcional Dos Pacientes Submetidos a Artrodese de Joelho Após Artroplastia Total Infectada. Rev. Bras. Ortop. 2021, 56, 320–325. [Google Scholar] [CrossRef]
- Balci, H.; Saglam, Y.; Pehlivanoglu, T.; Sen, C.; Eralp, L.; Kocaoglu, M. Knee Arthrodesis in Persistently Infected Total Knee Arthroplasty. J. Knee Surg. 2015, 29, 580–588. [Google Scholar] [CrossRef]
- Stavrakis, A.I.; Mayer, E.N.; Devana, S.K.; Chowdhry, M.; Dipane, M.V.; McPherson, E.J. Outcomes of Modular Knee Arthrodesis for Challenging Periprosthetic Joint Infections. Arthroplast. Today 2022, 13, 199–204. [Google Scholar] [CrossRef]
- Corona, P.S.; Jurado, M.; Scott-Tennent, A.; Fraile, R.; Carrera, L.; Vicente, M. Uniplanar versus Biplanar Monolateral External Fixator Knee Arthrodesis after End-Stage Failed Infected Total Knee Arthroplasty: A Comparative Study. Eur. J. Orthop. Surg. Traumatol. 2020, 30, 815–825. [Google Scholar] [CrossRef]
- Faure, P.-A.; Putman, S.; Senneville, E.; Beltrand, E.; Behal, H.; Migaud, H. Knee Arthrodesis Using a Custom Modular Intramedullary Nail in Failed, Infected Knee Arthroplasties: A Concise Follow-up Note of 31 Cases at a Median of 13 Years Post-Arthrodesis. Orthop. Traumatol. Surg. Res. 2021, 107, 102898. [Google Scholar] [CrossRef]
- Gramlich, Y.; Steinkohl, D.; Kremer, M.; Kemmerer, M.; Hoffmann, R.; Klug, A. Modular Knee Arthrodesis Secures Limb, Mobility, Improves Quality of Life, and Leads to High Infection Control in Periprosthetic Knee Infection, When Revision Knee Arthroplasty Is Not an Option. Arch. Orthop. Trauma Surg. 2021, 141, 1349–1360. [Google Scholar] [CrossRef]
- Hawi, N.; Kendoff, D.; Citak, M.; Gehrke, T.; Haasper, C. Septic Single-Stage Knee Arthrodesis after Failed Total Knee Arthroplasty Using a Cemented Coupled Nail. Bone Jt. J. 2015, 97, 649–653. [Google Scholar] [CrossRef]
- Iacono, F.; Raspugli, G.F.; Bruni, D.; Lo Presti, M.; Sharma, B.; Akkawi, I.; Marcacci, M. Arthrodesis After Infected Revision TKA: Retrospective Comparison of Intramedullary Nailing and External Fixation. HSS J. 2013, 9, 229–235. [Google Scholar] [CrossRef]
- Putman, S.; Kern, G.; Senneville, E.; Beltrand, E.; Migaud, H. Knee Arthrodesis Using a Customised Modular Intramedullary Nail in Failed Infected Total Knee Arthroplasty. Orthop. Traumatol. Surg. Res. 2013, 99, 391–398. [Google Scholar] [CrossRef]
- Robinson, M.; Piponov, H.I.; Ormseth, A.; Helder, C.W.; Schwartz, B.; Gonzalez, M.H. Knee Arthrodesis Outcomes After Infected Total Knee Arthroplasty and Failure of Two-Stage Revision With an Antibiotic Cement Spacer. JAAOS Glob. Res. Rev. 2018, 2, e077. [Google Scholar] [CrossRef]
- Röhner, E.; Windisch, C.; Nuetzmann, K.; Rau, M.; Arnhold, M.; Matziolis, G. Unsatisfactory outcome of arthrodesis performed after septic failure of revision total knee arthroplasty. J. Bone Jt. Surg. Am. 2015, 97, 298–301. [Google Scholar] [CrossRef]
- Suda, A.J.; Brachtendorf, X.; Tinelli, M.; Wagokh, R.; Abou-Nouar, G.; Bischel, O.E. Low Complication Rate and Better Results for Intramedullary Nail—Arthrodesis for Infected Knee Joints Compared to External Fixator—A Series of One Hundred Fifty Two Patients. Int. Orthop. 2021, 45, 1735–1744. [Google Scholar] [CrossRef]
- Trouillez, T.; Faure, P.A.; Martinot, P.; Migaud, H.; Senneville, E.; Pasquier, G.; Dartus, J.; Putman, S. Above–the–Knee Amputation versus Knee Arthrodesis for Revision of Infected Total Knee Arthroplasty: Recurrent Infection Rates and Functional Outcomes of 43 Patients at a Mean Follow-up of 6.7 Years. Orthop. Traumatol. Surg. Res. 2021, 107, 102914. [Google Scholar] [CrossRef]
- Watanabe, K.; Minowa, T.; Takeda, S.; Otsubo, H.; Kobayashi, T.; Kura, H.; Yamashita, T. Outcomes of Knee Arthrodesis Following Infected Total Knee Arthroplasty: A Retrospective Analysis of 8 Cases. Mod. Rheumatol. 2014, 24, 243–249. [Google Scholar] [CrossRef]
- Wilding, C.P.; Cooper, G.A.; Freeman, A.K.; Parry, M.C.; Jeys, L. Can a Silver-Coated Arthrodesis Implant Provide a Viable Alternative to Above Knee Amputation in the Unsalvageable, Infected Total Knee Arthroplasty? J. Arthroplast. 2016, 31, 2542–2547. [Google Scholar] [CrossRef]
- Yeung, C.M.; Lichstein, P.M.; Varady, N.H.; Maguire, J.H.; Chen, A.F.; Estok, D.M. Knee Arthrodesis Is a Durable Option for the Salvage of Infected Total Knee Arthroplasty. J. Arthroplast. 2020, 35, 3261–3268. [Google Scholar] [CrossRef]
- Zajonz, D.; Zimmerlich, B.; Möbius, R.; Edel, M.; Przybyl, J.; Höch, A.; Fakler, J.K.M.; Roth, A.; Ghanem, M. Knee Arthrodesis as Last Resort for Persistent Knee Joint Infections: Comparison of Extramedullary and Intramedullary Treatment. Orthopäde 2021, 50, 207–213. [Google Scholar] [CrossRef]
- Mercurio, M.; Castioni, D.; Porco, E.; Familiari, F.; Gasparini, G.; Galasso, O. Periprosthetic Ankle Infection: Eradication Rate, Complications, and Limb Salvage. A Systematic Review. Foot Ankle Surg. 2022, 28, 550–556. [Google Scholar] [CrossRef]
- Aparicio, G.; Otero, J.; Bru, S. High Rate of Fusion but High Complication Rate After Knee Arthrodesis for Infected Revision Total Knee Replacement. Indian J. Orthop. 2020, 54, 616–623. [Google Scholar] [CrossRef]
- Gallusser, N.; Goetti, P.; Luyet, A.; Borens, O. Knee Arthrodesis with Modular Nail after Failed TKA Due to Infection. Eur. J. Orthop. Surg. Traumatol. 2015, 25, 1307–1312. [Google Scholar] [CrossRef]
- Brown, T.S. Intra-Articular Injections Should Be Avoided in the 3 Months Prior to Total Knee Arthroplasty: Commentary on an Article by Shawn S. Richardson, MD; et al.: “Comparison of Infection Risk with Corticosteroid or Hyaluronic Acid Injection Prior to Total Knee Arthroplasty”. J. Bone Jt. Surg. 2019, 101, e8. [Google Scholar] [CrossRef]
- Senneville, E.; Joulie, D.; Legout, L.; Valette, M.; Dezèque, H.; Beltrand, E.; Roselé, B.; d’Escrivan, T.; Loïez, C.; Caillaux, M.; et al. Outcome and Predictors of Treatment Failure in Total Hip/Knee Prosthetic Joint Infections Due to Staphylococcus Aureus. Clin. Infect. Dis. 2011, 53, 334–340. [Google Scholar] [CrossRef]
- Aggarwal, V.K.; Bakhshi, H.; Ecker, N.U.; Parvizi, J.; Gehrke, T.; Kendoff, D. Organism profile in periprosthetic joint infection: Pathogens differ at two arthroplasty infection referral centers in Europe and in the United States. J. Knee Surg. 2014, 27, 399–406. [Google Scholar] [CrossRef]
- Balato, G.; Roscetto, E.; Vollaro, A.; Galasso, O.; Gasparini, G.; Ascione, T.; Catania, M.R.; Mariconda, M. Bacterial Biofilm Formation Is Variably Inhibited by Different Formulations of Antibiotic-Loaded Bone Cement in Vitro. Knee Surg. Sports Traumatol. Arthrosc. 2019, 27, 1943–1952. [Google Scholar] [CrossRef]
- Gasparini, G.; Castioni, D.; Spina, G.; Familiari, F.; Galasso, O.; Mercurio, M. The Use of a Surgical Helmet System with a High-Efficiency Particulate Air Filter as Possible Protection Equipment during the Coronavirus Disease 2019 Pandemic: A Double-Blinded Randomized Control Study. Int. Orthop. 2022, 46, 1233–1240. [Google Scholar] [CrossRef]
- Quirino, A.; Marascio, N.; Scarlata, G.G.M.; Cicino, C.; Pavia, G.; Pantanella, M.; Carlisi, G.; Mercurio, M.; Familiari, F.; Rotundo, S.; et al. Orthopedic Device-Related Infections Due to Emerging Pathogens Diagnosed by a Combination of Microbiological Approaches: Case Series and Literature Review. Diagnostics 2022, 12, 3224. [Google Scholar] [CrossRef]
- Prié, H.; Meyssonnier, V.; Kerroumi, Y.; Heym, B.; Lidove, O.; Marmor, S.; Zeller, V. Pseudomonas Aeruginosa Prosthetic Joint-Infection Outcomes: Prospective, Observational Study on 43 Patients. Front. Med. 2022, 9, 1039596. [Google Scholar] [CrossRef]
- Kuchinad, R.; Fourman, M.S.; Fragomen, A.T.; Rozbruch, S.R. Knee Arthrodesis as Limb Salvage for Complex Failures of Total Knee Arthroplasty. J. Arthroplast. 2014, 29, 2150–2155. [Google Scholar] [CrossRef] [PubMed]
- Conway, J.D.; Mont, M.A.; Bezwada, H.P. Arthrodesis of the Knee. J. Bone Jt. Surg. 2004, 86, 835–848. [Google Scholar] [CrossRef]
- Birch, J.G.; Samchukov, M.L. Use of the Ilizarov Method to Correct Lower Limb Deformities in Children and Adolescents. J. Am. Acad. Orthop. Surg. 2004, 12, 144–154. [Google Scholar] [CrossRef]
- Oostenbroek, H.J.; van Roermund, P.M. Arthrodesis of the knee after an infected arthroplasty using the Ilizarov method. J. Bone Jt. Surg. 2001, 83, 50–54. [Google Scholar] [CrossRef]
- Kim, K.; Snir, N.; Schwarzkopf, R. Modern Techniques in Knee Arthrodesis. Int. J. Orthop. 2016, 3, 487–496. [Google Scholar] [CrossRef]

| Study Author (year) | Criteria | Total | Quality | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | |||
| Aparicio et al. (2020) [13] | 1 | 0 | 1 | 1 | 2 | 1 | 1 | 1 | 8 | High |
| Balci et al. (2015) [14] | 1 | 0 | 1 | 1 | 2 | 1 | 1 | 1 | 8 | High |
| Brown et al. (2020) [15] | 1 | 0 | 1 | 1 | 2 | 1 | 1 | 1 | 8 | High |
| Corona et al. (2020) [16] | 1 | 1 | 1 | 1 | 2 | 1 | 1 | 1 | 9 | High |
| Faure et al. (2021) [17] | 1 | 0 | 1 | 1 | 2 | 1 | 1 | 1 | 8 | High |
| Friedrich et al. (2017) [4] | 1 | 0 | 1 | 1 | 2 | 1 | 1 | 1 | 8 | High |
| Galluser et al. (2015) [14] | 1 | 0 | 1 | 1 | 2 | 1 | 1 | 1 | 8 | High |
| Gathen et al. (2018) [3] | 1 | 1 | 1 | 1 | 2 | 1 | 1 | 1 | 9 | High |
| Gramlich et al. (2021) [18] | 1 | 1 | 1 | 1 | 2 | 1 | 1 | 1 | 9 | High |
| Hawi et al. (2015) [19] | 1 | 0 | 1 | 1 | 2 | 1 | 1 | 1 | 8 | High |
| Iacono et al. (2013) [20] | 1 | 1 | 1 | 1 | 2 | 1 | 1 | 1 | 9 | High |
| Putman et al. (2013) [21] | 1 | 0 | 1 | 1 | 2 | 1 | 1 | 1 | 8 | High |
| Razii et al. (2016) [8] | 1 | 0 | 1 | 1 | 2 | 1 | 1 | 1 | 8 | High |
| Robinson et al. (2018) [22] | 1 | 0 | 1 | 1 | 2 | 1 | 1 | 1 | 8 | High |
| Rohner et al. (2015) [23] | 1 | 1 | 1 | 1 | 2 | 1 | 1 | 1 | 9 | High |
| Stavrakis et al. (2022) [15] | 1 | 0 | 1 | 1 | 2 | 1 | 1 | 1 | 8 | High |
| Suda et al. (2021) [24] | 1 | 1 | 1 | 1 | 2 | 1 | 1 | 1 | 9 | High |
| Trouillez et al. (2021) [25] | 1 | 1 | 1 | 1 | 2 | 1 | 1 | 1 | 9 | High |
| Vivacqua et al. (2021) [13] | 1 | 0 | 1 | 1 | 2 | 1 | 1 | 1 | 8 | High |
| Watanabe et al. (2014) [26] | 1 | 0 | 1 | 1 | 2 | 1 | 1 | 1 | 8 | High |
| Wilding et al. (2016) [27] | 1 | 0 | 1 | 1 | 2 | 1 | 0 | 1 | 7 | High |
| Yeung et al. (2020) [28] | 1 | 0 | 1 | 1 | 2 | 1 | 1 | 1 | 8 | High |
| Zajonz et al. (2021) [29] | 1 | 1 | 1 | 1 | 2 | 1 | 1 | 1 | 9 | High |
| Microorganism | No. | % |
|---|---|---|
| Not specified | 390 | 45.5 |
| Negative cultures/no bacterial growth | 65 | 7.6 |
| Coagulase-negative Staphylococcus | 60 | 7 |
| Staphylococcus Epidermidis | 52 | 6.1 |
| Methicillin-Resistant Staphylococcus aureus | 50 | 5.8 |
| Methicillin-Sensitive Staphylococcus aureus | 45 | 5.2 |
| Staphylococcus Aureus non specified | 35 | 4 |
| Pseudomonas Aeruginosa | 23 | 2.7 |
| Enterococcus faecalis | 23 | 2.2 |
| Streptococcus spp. | 18 | 2.1 |
| Polymicrobial not otherwise specified | 16 | 1.9 |
| Escherichia Coli | 15 | 1.7 |
| Enterobacter Cloacae | 6 | 0.7 |
| Candida | 5 | 0.6 |
| Vancomycin-Resistant Enterococcus | 4 | 0.5 |
| Enterococcus spp. | 4 | 0.5 |
| Proteus Mirabilis | 4 | 0.5 |
| Propionibacterium Acnes | 3 | 0.3 |
| Streptococcus Agalactiae | 3 | 0.3 |
| Fusobacterium spp. | 3 | 0.3 |
| Staphylococcus Capitis | 3 | 0.3 |
| Serratia marcescens | 3 | 0.3 |
| Methicillin-Resistant Staphylococcus epidermidis | 2 | 0.2 |
| Clostridium | 2 | 0.2 |
| Corynebacterium non specified | 2 | 0.2 |
| Klebsiella Pneumoniae | 2 | 0.2 |
| Prevotella bivia | 2 | 0.2 |
| Stafilococcus Warneri | 2 | 0.2 |
| Streptococco Dysagalactie | 2 | 0.2 |
| Enterococcus Faecium | 2 | 0.2 |
| Streptococcus Viridans | 2 | 0.2 |
| Methicillin-Sensitive Staphylococcus epidermidis | 1 | 0.1 |
| Enterobacter spp. | 1 | 0.1 |
| Corynebacterium Amicolatum | 1 | 0.1 |
| Staphylococcus Haemoliticus | 1 | 0.1 |
| Staphylococcus Hominis | 1 | 0.1 |
| Mycobacterium | 1 | 0.1 |
| Klebsiella | 1 | 0.1 |
| Acinetobacter Baumanii | 1 | 0.1 |
| Morganelli Morgana | 1 | 0.1 |
| Total | 857 |
| Complications | IMN vs. CP | IMN vs. EF | EF vs. CP |
|---|---|---|---|
| Wound dehiscence | p = 1 | p < 0.001 | p = 0.3 |
| Fractures | p = 0.4 | p = 0.07 | p = 1 |
| Transient nerve injury | p = 1 | p = 1 | p = 1 |
| Permanent nerve injury | p = 1 | p = 0.07 | p = 1 |
| Aseptic loosening | p = 1 | p = 0.59 | p = 1 |
| Long-term suppressive antibiotics treatment | p = 1 | p = 0.03 | p = 1 |
| Reinfection | p = 1 | p = 0.9 | p = 1 |
| Reoperation | p = 0.24 | p = 0.56 | p = 0.37 |
| Conversion to amputation | p = 0.053 | p = 0.65 | p = 0.03 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mercurio, M.; Gasparini, G.; Cofano, E.; Zappia, A.; Familiari, F.; Galasso, O. Knee Arthrodesis for Periprosthetic Knee Infection: Fusion Rate, Complications, and Limb Salvage—A Systematic Review. Healthcare 2024, 12, 804. https://doi.org/10.3390/healthcare12070804
Mercurio M, Gasparini G, Cofano E, Zappia A, Familiari F, Galasso O. Knee Arthrodesis for Periprosthetic Knee Infection: Fusion Rate, Complications, and Limb Salvage—A Systematic Review. Healthcare. 2024; 12(7):804. https://doi.org/10.3390/healthcare12070804
Chicago/Turabian StyleMercurio, Michele, Giorgio Gasparini, Erminia Cofano, Andrea Zappia, Filippo Familiari, and Olimpio Galasso. 2024. "Knee Arthrodesis for Periprosthetic Knee Infection: Fusion Rate, Complications, and Limb Salvage—A Systematic Review" Healthcare 12, no. 7: 804. https://doi.org/10.3390/healthcare12070804
APA StyleMercurio, M., Gasparini, G., Cofano, E., Zappia, A., Familiari, F., & Galasso, O. (2024). Knee Arthrodesis for Periprosthetic Knee Infection: Fusion Rate, Complications, and Limb Salvage—A Systematic Review. Healthcare, 12(7), 804. https://doi.org/10.3390/healthcare12070804