
Exploring Adverse Drug Reactions in Psychotropic Medications: A Retrospective Analysis of Portuguese Pharmacovigilance Data

Abstract
:1. Introduction
2. Materials and Methods
3. Results
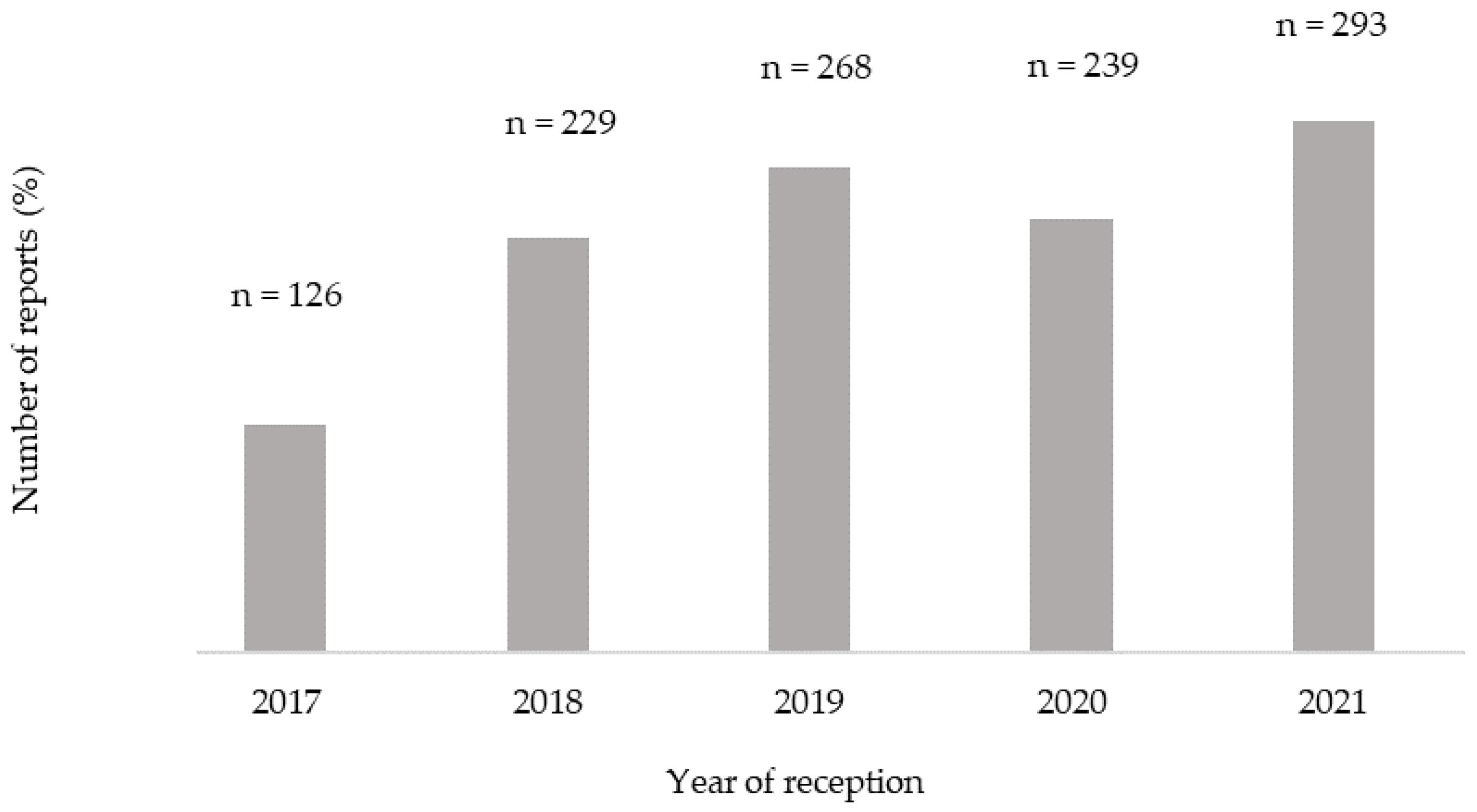
3.1. Characterization of Individual Case Safety Reports (ICSRs)
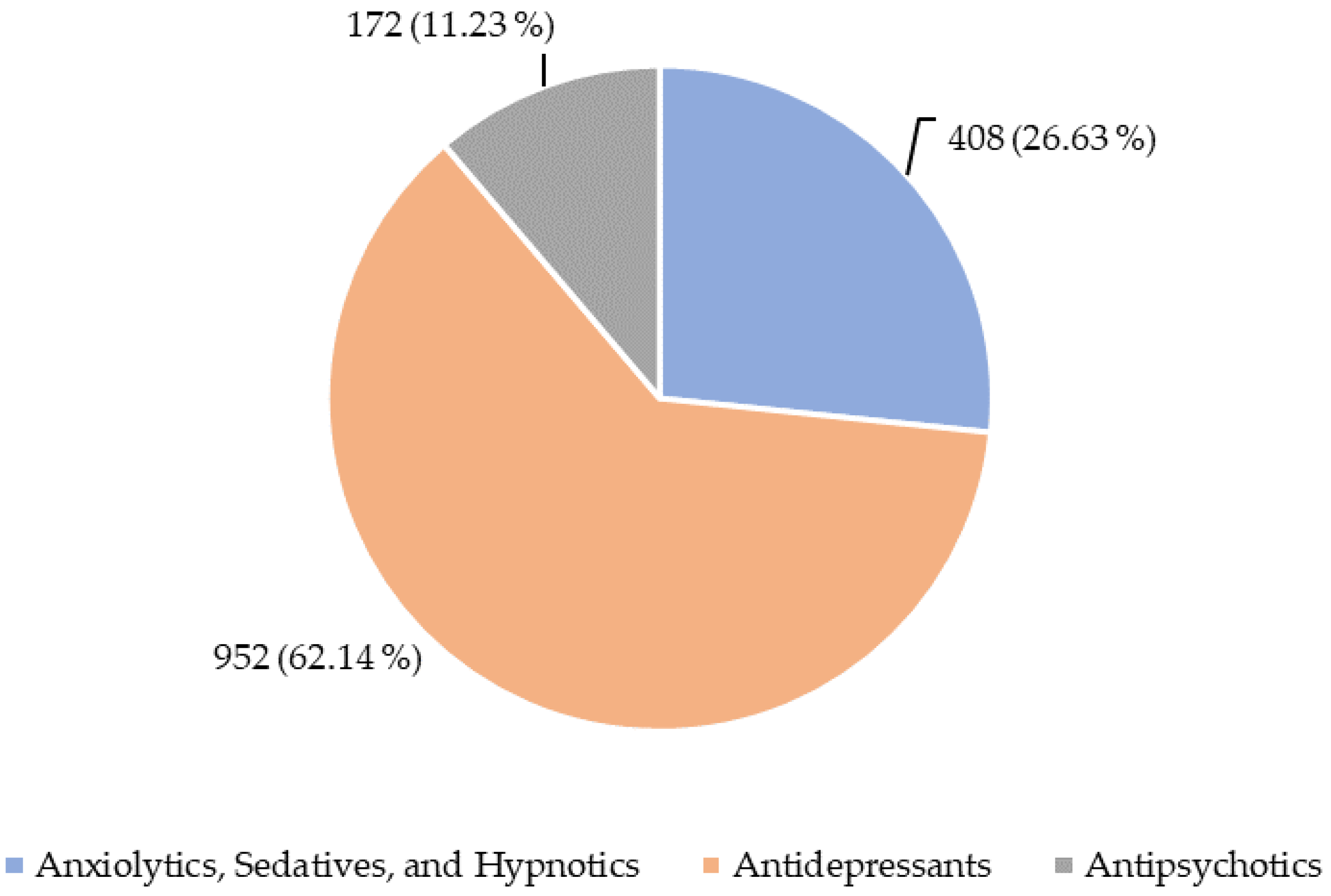
3.2. Characterization of Psychotropic Drugs Involved in the ICSRs
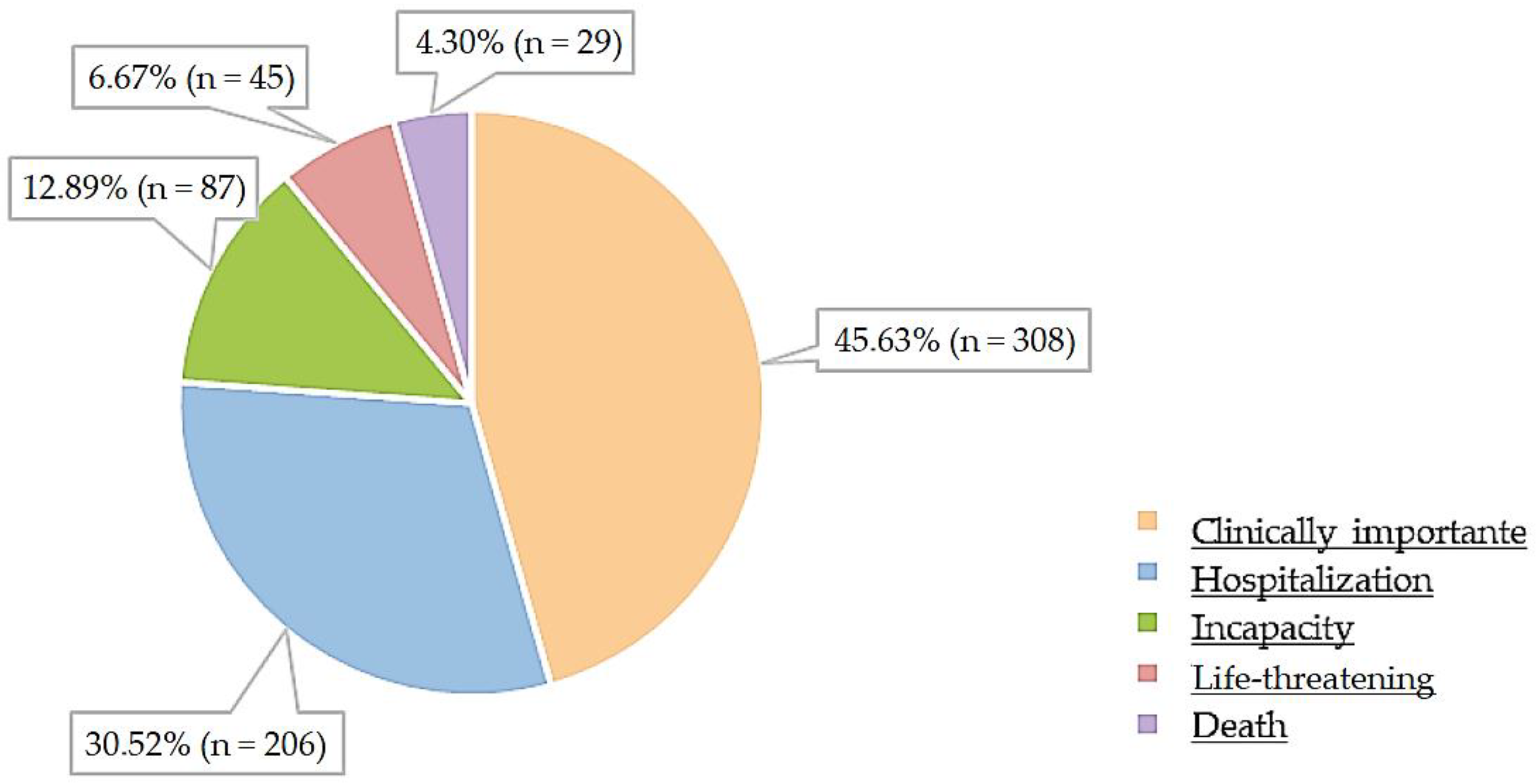
3.3. Characterization of Adverse Drug Reactions (ADRs)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hollingworth, H.L.; Barnes, F.M. Mental Disorders. J. Philos. 2022, 21, 165. [Google Scholar] [CrossRef]
- De Almeida, J.M.C.; Xavier, M.; Cardoso, G.; Pereira, M.G.; Gusmão, R.; Corrêa, B.; Gago, J.; Talina, M.; Silva, J. Estudo Epidemiológico Nacional de Saúde Mental—1° Relatório; Universidade Nova de Lisboa: Lisboa, Portugal, 2013. [Google Scholar]
- Observatório Nacional Luta Contra a Pobreza. Boletim #7—A Saúde Mental Em Portugal: Um Breve Retrato Epidemiológico; Observatório Nacional Luta Contra a Pobreza: Porto, Portugal, 2021. [Google Scholar]
- Direção-Geral da Saúde. Saúde Mental Em Números—2014; Direção-Geral da Saúde: Lisbon, Portugal, 2014. [Google Scholar]
- Instituto Nacional de Estatística. Estatísticas Da Saúde—2020; Instituto Nacional de Estatística: Lisbon, Portugal, 2020. [Google Scholar]
- INFARMED—National Authority of Medicines and Health Products, I.P. Medicine and Healthcare Products Statistics; INFARMED—National Authority of Medicines and Health Products, I.P.: Lisbon, Portugal, 2014; pp. 1–95. [Google Scholar]
- INFARMED—National Authority of Medicines and Health Products, I.P. Estatística Do Medicamento e Produtos de Saúde 2022. Available online: https://www.infarmed.pt/web/infarmed/entidades/medicamentos-uso-humano/monitorizacao-mercado/estatistica-anual/relatorios-anuais (accessed on 13 March 2024).
- Mottram, P.G.; Wilson, K.; Strobl, J.J. Antidepressants for Depressed Elderly. Cochrane Database Syst. Rev. 2006, 2006, CD003491. [Google Scholar] [CrossRef]
- Alonso-Pedrero, L.; Bes-Rastrollo, M.; Marti, A. Effects of Antidepressant and Antipsychotic Use on Weight Gain: A Systematic Review. Obes. Rev. 2019, 20, 1680–1690. [Google Scholar] [CrossRef] [PubMed]
- Whalen, K.; Finkel, R.; Panavelil, T.A. Farmacologia Ilustrada; Artmed—Grupo A: Lisbon, Portugal, 2016; ISBN 8565852695. [Google Scholar]
- European Comission. Strengthening Pharmacovigilance to Reduce Adverse Effects of Medicines. Available online: https://ec.europa.eu/commission/presscorner/detail/en/MEMO_08_782 (accessed on 13 September 2022).
- European Medicines Agency. Annex I—Definitions (Rev 4). In Guideline on Good Pharmacovigilance Practices (GVP); European Medicines Agency: Amsterdam, The Nederlands, 2012. [Google Scholar]
- European Medicines Agency. Module I—Pharmacovigilance Systems and Their Quality Systems. In Guideline on Good Pharmacovigilance Practices (GVP); European Medicines Agency: Amsterdam, The Nederlands, 2012. [Google Scholar]
- INFARMED—National Authority of Medicines and Health Products, I.P. Sistema Nacional de Farmacovigilância (SNF). Available online: https://www.infarmed.pt/web/infarmed/entidades/medicamentos-uso-humano/farmacovigilancia/sistema-de-farmacovigilancia (accessed on 13 March 2024).
- World Health Organization. WHOCC—ATC/DDD Index. Available online: https://www.whocc.no/atc_ddd_index/ (accessed on 6 November 2023).
- INFARMED—National Authority of Medicines and Health Products, I.P. Monitorização Do Consumo de Medicamentos Ambulatório. 2022. Available online: https://www.infarmed.pt/documents/15786/6353588/dezembro/caa03065-ec69-d2a7-95f0-1b1c2227e13b?version=1.0 (accessed on 13 March 2024).
- INFARMED—National Authority of Medicines and Health Products, I.P. Sistema Nacional de Farmacovigilancia (SNF): Relatório de Atividade 2021. Available online: https://www.infarmed.pt/documents/15786/2099374/Relat%C3%B3rio+Anual+de+Atividades+2021/f88db1bd-40a7-7207-54a4-003b48fc6b10 (accessed on 13 March 2024).
- Pego, A.; Pereira, A.; Figueirdo, A.; Araújo, A.; Severiano, A.; Macedo, A. Farmacovigilância Em Portugal: 25 Anos. Available online: http://app10.infarmed.pt/e_book_farmacovigilancia25/index.html (accessed on 10 September 2022).
- Direção-Geral da Saúde. Health Literacy Action Plan 2019–2021; Direção-Geral da Saúde: Lisbon, Portugal, 2019. [Google Scholar]
- Arriaga, M.; Francisco, R.; Nogueira, P.; Oliveira, J.; Silva, C.; Câmara, G.; Sørensen, K.; Dietscher, C.; Costa, A. Health Literacy in Portugal: Results of the Health Literacy Population Survey Project 2019–2021. Int. J. Environ. Res. Public Health 2022, 19, 4225. [Google Scholar] [CrossRef] [PubMed]
- Ashida, S.; Goodman, M.; Pandya, C.; Koehly, L.M.; Lachance, C.; Stafford, J.; Kaphingst, K.A. Age Differences in Genetic Knowledge, Health Literacy and Causal Beliefs for Health Conditions. Public. Health Genom. 2011, 14, 307–316. [Google Scholar] [CrossRef] [PubMed]
- Instituto Nacional Estatística. População Residente (N.º) por Local de Residência à Data dos Censos [2021]. Available online: https://www.ine.pt/xportal/xmain?xpid=INE&xpgid=ine_indicadores&contecto=pi&indOcorrCod=0011628&selTab=tab0 (accessed on 3 January 2023).
- Da Silva, J.C.; Soares, M.; Martins, S. Reações Adversas a Medicamentos-Análise Da Base de Dados Do Sistema Nacional de Farmacovigilância (SVIG); INFARMED—National Authority of Medicines and Health Products, I.P.: Lisbon, Portugal, 2012; pp. 6–9. [Google Scholar]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-5)-Criteria Updates, 5th ed.; American Psychiatric Association: Washington, DC, USA, 2018. [Google Scholar]
- Caramona, M.; Vitória, I.; Teixeira, M.; Alcobia, A.; Almeida, P.; Horta, R.; Reis, L. Normas de Orientação Terapêutica; Ordem dos Farmacêuticos: Lisbon, Portugal, 2011; ISBN 9789729655593. [Google Scholar]
- INFARMED—National Authority of Medicines and Health Products, I.P. Desempenho Do SNF. Available online: https://www.infarmed.pt/web/infarmed/entidades/medicamentos-uso-humano/farmacovigilancia/desempenho-do-snf?fbclid=IwAR2newrgP1U44sihYWC4a-PgqmI35xNuIDGv7dHdLqTo4WKV9vzqL0t4Pag (accessed on 26 December 2023).
- Varallo, F.R.; Guimarães, S.d.O.P.; Abjaude, S.A.R.; Mastroianni, P.d.C. Causes for the Underreporting of Adverse Drug Events by Health Professionals: A Systematic Review. Rev. Esc. Enferm. 2014, 48, 739–747. [Google Scholar] [CrossRef] [PubMed]
- Simões, J.A. A Consulta Em Medicina Geral e Familiar. Rev. Port. Clínica Geral 2009, 25, 197–198. [Google Scholar] [CrossRef]
- Allen, J.; Gay, B.; Crebolder, H.; Heyrman, J.; Svab, I.; Ram, P. A Definição Europeia de Medicina Geral e Familiar (Clínica Geral/Medicina Familiar) Versão Reduzida. EURACT, 2005. Rev. Port. Clin. Geral. 2005, 21, 511–516. [Google Scholar]
- Ferreira-Da-Silva, R.; Ribeiro-Vaz, I.; Silva, A.M.; Marques, J.; Polónia, J.J. Looking Back on 20 Years of Work at the Porto Pharmacovigilance Centre, Portugal. Cad. Saúde Pública 2021, 37, e00304420. [Google Scholar] [CrossRef]
- Sienkiewicz, K.; Burzyńska, M.; Rydlewska-Liszkowska, I.; Sienkiewicz, J.; Gaszyńska, E. The Importance of Direct Patient Reporting of Adverse Drug Reactions in the Safety Monitoring Process. Int. J. Environ. Res. Public. Health 2022, 19, 413. [Google Scholar] [CrossRef] [PubMed]
- Weigmann, K. Consumer Reporting of Adverse Drug Reactions. Embo Rep. 2016, 17, 949–952. [Google Scholar] [CrossRef] [PubMed]
- Direção-Geral da Saúde. Programa Nacional Para a Saúde Mental—2017; Direção-Geral da Saúde: Lisbon, Portugal, 2017. [Google Scholar]
- INFARMED—National Authority of Medicines and Health Products, I.P. Meio Ambulatório—Monitorização Do Consumo de Medicamentos; INFARMED—National Authority of Medicines and Health Products, I.P.: Lisbon, Portugal, 2021. [Google Scholar]
- Pordata. SNS: Consultas, Internamentos e Urgências Nos Hospitais—Continente. Available online: https://www.pordata.pt/portugal/sns+consultas++internamentos+e+urgencias+nos+hospitais+por+mil+habitantes+++continente-3409 (accessed on 13 March 2024).
- Caldas, A.C.; Torre, C.; Castelão, J.; Monteiro, M.d.P.L.; Lopes, P.; Baptista, T. Sem Mais Tempo a Perder—Relatório CNS Saúde Mental Em Portugal: Um Desafio Para a Próxima Década; Conselho Nacional de Saúde: Lisbon, Portugal, 2019; pp. 1–130. [Google Scholar]
- Pady, S.M. Evolução Do Consumo Em Portugal Continental (2000–2012). Ann. Bot. 1935, os-49, 71–93. [Google Scholar] [CrossRef]
- World Health Organization. Depression and Other Common Mental Disorders. Obstet. Gynecol. 2017, 48, 56–60. [Google Scholar]
- Institute for Health Metrics and Evaluation VizHub—GBD Results. Available online: https://vizhub.healthdata.org/gbd-results/?params=gbd-api-2019-permalink/d780dffbe8a381b25e1416884959e88b (accessed on 14 June 2022).
- Nogueira, J.; Santos, M. Análise Do Consumo de Antidepressivos e Seus Encargos Em Portugal Continental. RevSALUS 2018, 8, 73261. [Google Scholar]
- Rosales, A.T. Frecuencia de Sospechas de Reacciones Adversas de Medicamentos (SRAM) Con Psicofármacos En Pacientes Con Polifarmacia; Universidad Autónoma Metropolitana: Mexico City, Mexico, 2022; pp. 1–38. Available online: https://repositorio.xoc.uam.mx/jspui/handle/123456789/26443 (accessed on 14 January 2024).
- INFARMED—National Authority of Medicines and Health Products, I.P. Psicofármacos: Evolução Do Consumo Em Portugal Continental (2000–2012); National Authority of Medicines and Health Products, I.P.: Lisbon, Portugal, 2013. [Google Scholar]
- Khalil, H.; Kirschbaum, M. Adverse Drug Reactions in Primary Care: A Scoping Review Protocol. JBI Database Syst. Rev. Implement. Rep. 2018, 16, 615–621. [Google Scholar] [CrossRef] [PubMed]
- Ramos, A.R. Perfil de Segurança Dos Inibidores Da Bomba de Protões: Reações Adversas Notificadas de 2007 a 2017. Master’s Thesis, Universidade da Beira Interior, Covilhã, Portugal, 2019. Available online: https://ubibliorum.ubi.pt/handle/10400.6/8905 (accessed on 13 March 2024).
- Mota, D.M. Evolução E Resultados Do Sistema De Farmacovigilância Do Brasil. 2017. Available online: https://bibliotecadigital.anvisa.gov.br/jspui/handle/anvisa/350 (accessed on 16 February 2024).
- Mota, D.M.; Vigo, Á.; De Souza Kuchenbecker, R. Adverse Drug Reactions Reported to the Brazilian Pharmacovigilance System from 2008 to 2013: Descriptive Study. Cad. Saúde Pública 2019, 35, e00148818. [Google Scholar] [CrossRef]
- Aronson, J.K.; Ferner, R.E. Unlicensed and off-Label Uses of Medicines: Definitions and Clarification of Terminology. Br. J. Clin. Pharmacol. 2017, 83, 2615–2625. [Google Scholar] [CrossRef]
- Roberts, R.J.; Lohano, K.K.; El-Mallakh, R.S. Antipsychotics as Antidepressants. Asia-Pac. Psychiatry 2016, 8, 179–188. [Google Scholar] [CrossRef] [PubMed]
- Pochiero, I.; Gorini, M.; Comandini, A.; Calisti, F.; Di Loreto, G.; Cattaneo, A.; Knight, T.; Anastassopoulos, K.P.; Patel, R.; Baik, R.; et al. Real-World Characteristics and Treatment Patterns of Patients with Insomnia Prescribed Trazodone in the United States. Clin. Ther. 2022, 44, 1093–1105. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Patient’s Age | % (n) |
| 0–1 month | 0.31 (3) |
| 2 months–2 years | 0.10 (1) |
| 3–11 years | 0.31 (3) |
| 12–17 years | 1.94 (19) |
| 18–64 years | 63.71 (625) |
| More than 65 years | 33.64 (330) |
| Unknown | 15.06 (174) |
| Total | 100.00 (981) |
| Geographic Origin (region according to NUTS II) | % (n) |
| North | 32.19 (178) |
| Centre | 20.98 (116) |
| Lisbon Metropolitan Area * West and Tagus Valley * Setúbal Peninsula * | 33.82 (187) |
| Alentejo | 5.79 (32) |
| Algarve | 5.97 (33) |
| Autonomous Region of the Azores | 0.72 (4) |
| Autonomous Region of Madeira | 0.54 (3) |
| Unknown | 52.12 (602) |
| Total | 100.0 (1155) |
| Reporters Professional Group | % (n) |
| Pharmaceutical Industry | 62.16 (718) |
| Pharmacist | 12.55 (145) |
| Physician | 12.21 (141) |
| Nurse | 0.52 (6) |
| Other health professional (HP) | 0.69 (8) |
| User or other non-HP | 11.86 (137) |
| Total | 100.00 (1155) |
| Suspected Psychotropic Drug | ATC | % (n) | |
|---|---|---|---|
| Alprazolam | N05B | Anxiolytics | 16.67 (68) |
| Bromazepam | 9.80 (40) | ||
| Clobazam | 1.47 (6) | ||
| Chlordiazepoxide dipotassium | 0.25 (1) | ||
| Cloxazolam | 2.94 (12) | ||
| Diazepam | 19.36 (79) | ||
| Ethyl loflazepate | 4.66 (19) | ||
| Lorazepam | 12.50 (51) | ||
| Oxazepam | 2.45 (10) | ||
| Buspirone | 0.98 (4) | ||
| Hydroxyzine | 4.90 (20) | ||
| Total | 75.98 (310) | ||
| Brotizolam | N05C | Hypnotics and Sedatives | 0.25 (1) |
| Estazolam | 0.49 (2) | ||
| Flurazepam | 1.23 (5) | ||
| Midazolam | 11.03 (45) | ||
| Temazepam | 0.25 (1) | ||
| Triazolam | 0.25 (1) | ||
| Valerian | 0.98 (4) | ||
| Dexmedetomidine | 1.72 (7) | ||
| Melatonin | 0.25 (1) | ||
| Zolpidem | 5.64 (23) | ||
| Total | 22.06 (90) | ||
| Doxylamine | R06AA | Antihistaminic for systemic use | 1.96 (8) |
| Total | 1.96 (8) | ||
| Total | 100.00 (408) | ||
| Suspected Psychotropic Drug | ATC Classification (5th Level) | ATC Classification (3rd Level) | % (n) |
|---|---|---|---|
| Imipramine | N06AA02 | Non-selective monoamine reuptake inhibitors | 0.11 (1) |
| Clomipramine | N06AA04 | 1.37 (13) | |
| Amitriptyline | N06AA09 | 3.68 (35) | |
| Nortriptyline | N06AA10 | 0.32 (3) | |
| Total | 5.48 (52) | ||
| Fluoxetine | N06AB03 | Selective serotonin reuptake inhibitors | 7.25 (69) |
| Citalopram | N06AB04 | 0.42 (4) | |
| Paroxetine | N06AB05 | 4.10 (39) | |
| Sertraline | N06AB06 | 18.59 (177) | |
| Fluvoxamine | N06AB08 | 1.26 (12) | |
| Escitalopram | N06AB10 | 9.87 (94) | |
| Total | 41.49 (395) | ||
| Moclobemide | N06AG02 | Monoamine oxidase A inhibitors | 0.11 (1) |
| Total | 0.11 (1) | ||
| Pirlindole | N06AX | Other antidepressants | 0.11 (1) |
| Mianserin | N06AX03 | 0.53 (5) | |
| Trazodone | N06AX05 | 16.81 (160) | |
| Mirtazapine | N06AX11 | 7.88 (75) | |
| Bupropion | N06AX12 | 5.57 (53) | |
| Tianeptine | N06AX14 | 0.53 (5) | |
| Venlafaxine | N06AX16 | 9.03 (86) | |
| Milnacipran | N06AX17 | 0.11 (1) | |
| Duloxetine | N06AX21 | 5.36 (51) | |
| Agomelatine | N06AX22 | 3.05 (29) | |
| Vortioxetine | N06AX26 | 3.89 (37) | |
| Esketamine | N06AX27 | 0.11 (1) | |
| Total | 52.08 (504) | ||
| Total | 100.0 (952) | ||
| Suspected Psychotropic Drug | ATC (Fifth Level) | ATC (Third Level) | % (n) |
|---|---|---|---|
| Cyamemazine | N05AA01 | Phenothiazines with aliphatic sidechain | 7.56 (13) |
| Chlorpromazine | N05AA01 | 2.33 (4) | |
| Levomepromazine | N05AA02 | 3.49 (6) | |
| Haloperidol | N05AD01 | Butyrophenone derivatives | 11.05 (19) |
| Zuclopenthixol | N05AF05 | Thioxanthene derivative | 0.58 (1) |
| Pimozide | N05AG02 | Diphenylbutylpiperidine derivatives | 1.16 (2) |
| Clozapine | N05AH02 | Diazepines, oxazepines, thiazepines, and oxepines | 4.07 (7) |
| Olanzapine | N05AH03 | 15.12 (26) | |
| Quetiapine | N05AH04 | 26.16 (45) | |
| Tiapride | N05AL03 | Benzamides | 1.74 (3) |
| Amisulpride | N05AL05 | 1.74 (3) | |
| Risperidone | N05AX08 | Other antipsychotics | 13.95 (24) |
| Zotepine | N05AX11 | 1.16 (2) | |
| Paliperidone | N05AX13 | 4.07 (7) | |
| Aripiprazole | N05AX12 | 5.81 (10) | |
| Total | 100.0 (172) | ||
| ADR Evolution | % (n) |
|---|---|
| Cure | 43.84 (1840) |
| Unknown | 35.60 (1494) |
| Recovery | 8.98 (377) |
| Persists without recovery | 8.53 (358) |
| Death | 2.12 (89) |
| Cure with sequelae | 0.93 (39) |
| Total | 100.0 (4197) |
| SOC Classification | % (n) |
|---|---|
| Nervous system disorders | 22.23 (769) |
| Psychiatric disorders | 16.53 (572) |
| General disorders and administration site conditions | 14.45 (500) |
| Gastrointestinal disorders | 14.42 (499) |
| Injury, poisoning, and procedural complications | 9.16 (317) |
| Skin and subcutaneous tissue disorders | 6.13 (212) |
| Metabolism and nutrition disorders | 4.57 (158) |
| Musculoskeletal and connective tissue disorders | 4.57 (158) |
| Investigations | 4.51 (156) |
| Respiratory, thoracic, and mediastinal disorders | 3.44 (119) |
| Total | 100.00 (3460) |
| LLT Classification | % (n) |
|---|---|
| Nausea | 14.84 (88) |
| Dizziness | 14.50 (86) |
| Off-label use | 14.00 (83) |
| Headache | 11.47 (68) |
| Vomiting | 9.11 (54) |
| Diarrhea | 8.60 (51) |
| Serotonin syndrome | 7.08 (42) |
| Drug ineffective | 6.91 (41) |
| Insomnia | 6.91 (41) |
| Drug interaction | 6.58 (39) |
| Total | 100.00 (593) |
| Causality Assessment | % (n) |
|---|---|
| Definitive | 4.96 (49) |
| Probable | 42.25 (417) |
| Possible | 45.49 (449) |
| Unlikely | 4.56 (45) |
| Conditional | 0.51 (5) |
| Unclassifiable | 1.32 (13) |
| Not related | 0.71 (7) |
| Unknown | 0.10 (1) |
| Not applicable | 0.10 (1) |
| Total | 100.00 (987) |
| Psychotropic Drug | ADR According to MedDRA LLT Classification | % (n) |
|---|---|---|
| Duloxetine | Tightness of jaw muscles; vomiting; swelling of tongue; nausea; blood pressure increased; malaise; numbness of limbs | 20.41 (10) |
| Escitalopram | Tremor; tachycardia; agitation; anxiety; confusion; insomnia; hypotension; intentional overdose; somnolence; altered state of consciousness | 20.41 (10) |
| Sertraline | Chapped lips; tremor; sexual dysfunction; diarrhea; dry mouth; malaise; raw gums | 14.29 (7) |
| Lorazepam | Prostration; drowsiness; hypotension; intentional overdose; somnolence; altered state of consciousness | 12.24 (6) |
| Diazepam | Hallucination; hypotension; incoherent; bradycardia | 8.16 (4) |
| Hydroxyzine | Angioedema; hallucination; maculo-papular rash; altered state of consciousness | 8.16 (4) |
| Fluoxetine | Anorgasmia; libido decreased | 4.08 (2) |
| Agomelatine | Pimple-like rash | 2.04 (1) |
| Alprazolam | Panic attack | 2.04 (1) |
| Mirtazapine | Agitation | 2.04 (1) |
| Paroxetine | Urticaria localized | 2.04 (1) |
| Trazodone | Urinary tract obstruction | 2.04 (1) |
| Venlafaxine | Medication in stool | 2.04 (1) |
| Total | 100.00 (49) | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bandarra, A.; Costa, C.; Angelova, K.; Leonardo, L.; Espírito-Santo, M. Exploring Adverse Drug Reactions in Psychotropic Medications: A Retrospective Analysis of Portuguese Pharmacovigilance Data. Healthcare 2024, 12, 808. https://doi.org/10.3390/healthcare12080808
Bandarra A, Costa C, Angelova K, Leonardo L, Espírito-Santo M. Exploring Adverse Drug Reactions in Psychotropic Medications: A Retrospective Analysis of Portuguese Pharmacovigilance Data. Healthcare. 2024; 12(8):808. https://doi.org/10.3390/healthcare12080808
Chicago/Turabian StyleBandarra, Ana, César Costa, Kristina Angelova, Lília Leonardo, and Margarida Espírito-Santo. 2024. "Exploring Adverse Drug Reactions in Psychotropic Medications: A Retrospective Analysis of Portuguese Pharmacovigilance Data" Healthcare 12, no. 8: 808. https://doi.org/10.3390/healthcare12080808