
Drivers of COVID-19 Outcomes in Long-Term Care Facilities Using Multi-Level Analysis: A Systematic Review


Abstract
1. Introduction
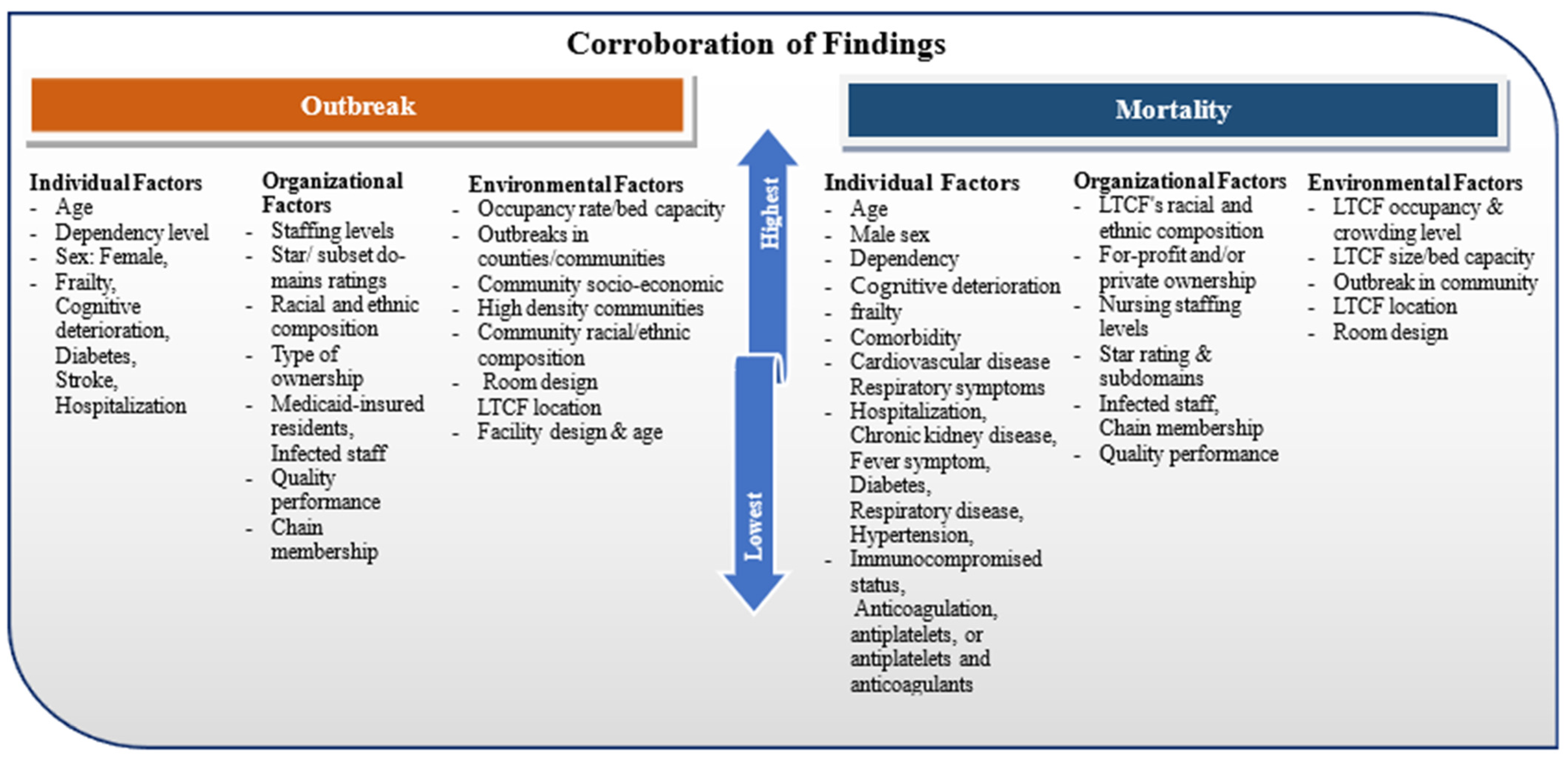
- What individual factors or characteristics, such as Frailty Index and age, impacted COVID-19 outcomes within LTCFs?
- What organizational characteristics and practices (e.g., staffing level, ownership status) within LTCFs affected the spread and mortality-related outcomes?
- Did environmental factors, such as facility/room design and facility age, influence COVID-19 outbreak and death?
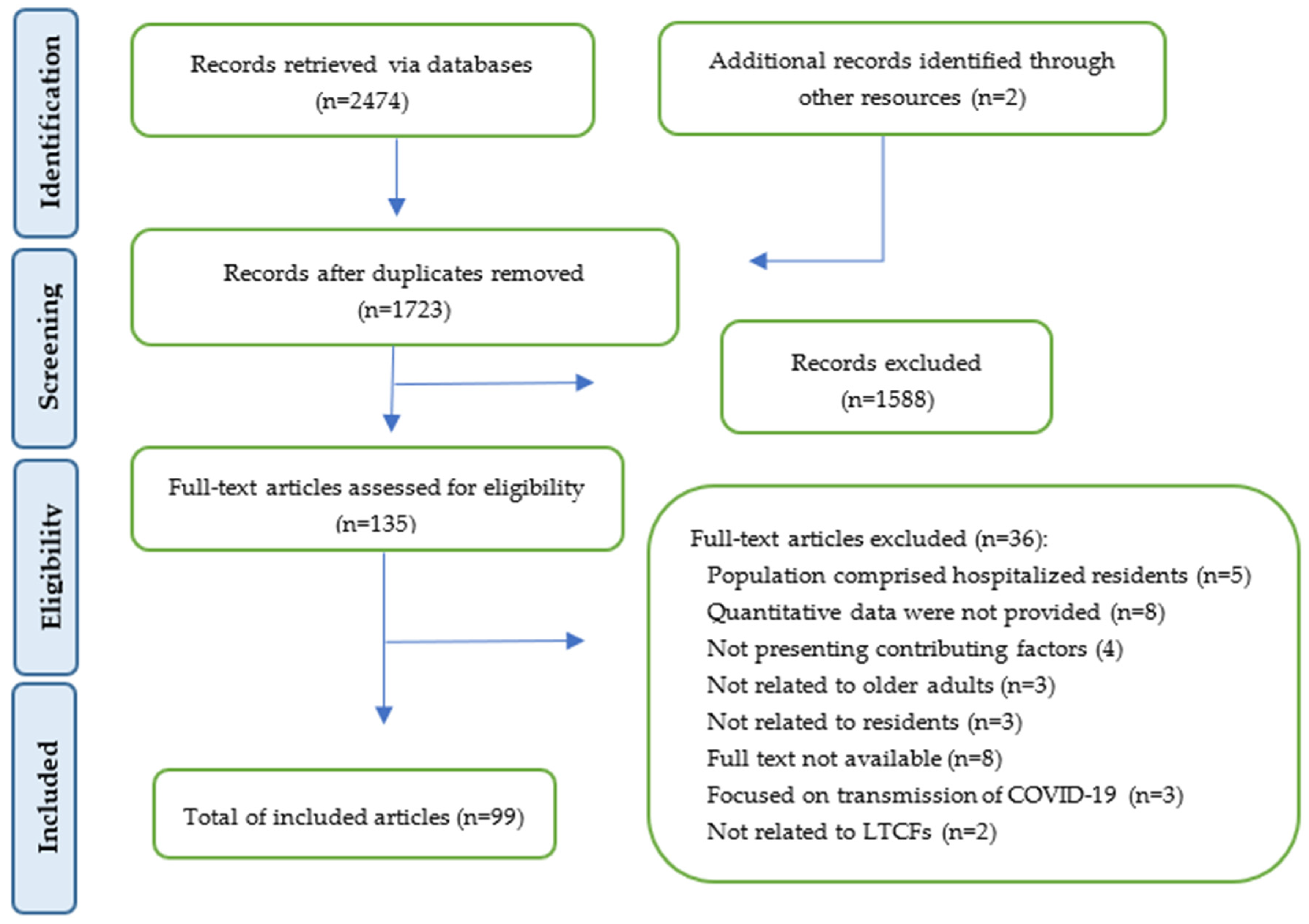
2. Materials and Methods
2.1. Search Strategy and Data Sources
2.2. Eligibility Criteria
2.3. Data Extraction
2.4. Data Analysis
3. Results
3.1. Individual Factors
3.1.1. Individual Factors Related to Outbreaks
3.1.2. Individual Factors Related to COVID-19-Related Deaths
3.2. Organizational Factors
3.2.1. Organizational Factors Related to Infection Outbreaks
3.2.2. Organizational Factors Related to COVID-Related Deaths
3.3. Environmental Factors
3.3.1. Environmental Factors Related to COVID Outbreaks
3.3.2. Environmental Factors Related to COVID-Related Deaths
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- McMichael, T.M.; Currie, D.W.; Clark, S.; Pogosjans, S.; Kay, M.; Schwartz, N.G.; Lewis, J.; Baer, A.; Kawakami, V.; Lukoff, M.D.; et al. Epidemiology of COVID-19 in a long-term care facility in king county, Washington. N. Engl. J. Med. 2020, 382, 2005–2011. [Google Scholar] [CrossRef]
- Unruh, M.A.; Yun, H.; Zhang, Y.; Braun, R.T.; Jung, H.-Y. Nursing home characteristics associated with COVID-19 deaths in connecticut, New Jersey, and New York. J. Am. Med. Dir. Assoc. 2020, 21, 1001–1003. [Google Scholar] [CrossRef] [PubMed]
- Hashan, M.R.; Smoll, N.; King, C.; Ockenden-Muldoon, H.; Walker, J.; Wattiaux, A.; Graham, J.; Booy, R.; Khandaker, G. Epidemiology and clinical features of COVID-19 outbreaks in aged care facilities: A systematic review and meta-analysis. Eclinicalmedicine 2021, 33, 100771. [Google Scholar] [CrossRef]
- Aalto, U.L.; Pitkälä, K.H.; Andersen-Ranberg, K.; Bonin-Guillaume, S.; Cruz-Jentoft, A.J.; Eriksdotter, M.; Gordon, A.L.; Gosch, M.; Holmerova, I.; Kautiainen, H.; et al. COVID-19 pandemic and mortality in nursing homes across USA and Europe up to October 2021. Eur. Geriatr. Med. 2022, 13, 705–709. [Google Scholar] [CrossRef] [PubMed]
- Moolla, I.; Hiilamo, H. Health system characteristics and COVID-19 performance in high-income countries. BMC Health Serv. Res. 2023, 23, 244. [Google Scholar] [CrossRef]
- Bagchi, S.; Mak, J.; Li, Q.; Sheriff, E.; Mungai, E.; Anttila, A.; Soe, M.M.; Edwards, J.R.; Benin, A.L.; Pollock, D.A.; et al. Rates of COVID-19 among residents and staff members in nursing homes—United States, May 25–November 22, 2020. Morb. Mortal. Wkly. Rep. 2021, 70, 52. [Google Scholar] [CrossRef]
- Giri, S.; Chenn, L.M.; Romero-Ortuno, R. Nursing homes during the COVID-19 pandemic: A scoping review of challenges and responses. Eur. Geriatr. Med. 2021, 12, 1127–1136. [Google Scholar] [CrossRef]
- Lin, H.-M.; Liu, S.T.H.; Levin, M.A.; Williamson, J.; Bouvier, N.M.; Aberg, J.A.; Reich, D.; Egorova, N. Informative censoring-a cause of bias in estimating COVID-19 mortality using hospital data. Life 2023, 13, 210. [Google Scholar] [CrossRef] [PubMed]
- COVID-19′s Impact on Long-Term Care [Internet]. 2022. Available online: https://www.cihi.ca/en/COVID-19-resources/impact-of-COVID-19-on-canadas-health-care-systems/long-term-care (accessed on 1 December 2022).
- Konetzka, R.T.; White, E.M.; Pralea, A.; Grabowski, D.C.; Mor, V. A systematic review of long-term care facility characteristics associated with COVID-19 outcomes. J. Am. Geriatr. Soc. 2021, 69, 2766–2777. [Google Scholar] [CrossRef]
- Frazer, K.; Mitchell, L.; Stokes, D.; Lacey, E.; Crowley, E.; Kelleher, C.C. A rapid systematic review of measures to protect older people in long-term care facilities from COVID-19. BMJ Open 2021, 11, e047012. [Google Scholar] [CrossRef]
- Dykgraaf, S.H.; Matenge, S.; Desborough, J.; Sturgiss, E.; Dut, G.; Roberts, L.; McMillan, A.; Kidd, M. Protecting nursing homes and long-term care facilities from COVID-19: A rapid review of international evidence. J. Am. Med. Dir. Assoc. 2021, 22, 1969–1988. [Google Scholar] [CrossRef]
- Rethlefsen, M.L.; Kirtley, S.; Waffenschmidt, S.; Ayala, A.P.; Moher, D.; Page, M.J.; Koffel, J.B. Prisma-s: An extension to the prisma statement for reporting literature searches in systematic reviews. Syst. Rev. 2021, 10, 39. [Google Scholar] [CrossRef] [PubMed]
- Methley, A.M.; Campbell, S.; Chew-Graham, C.; McNally, R.; Cheraghi-Sohi, S. Pico, picos and spider: A comparison study of specificity and sensitivity in three search tools for qualitative systematic reviews. BMC Health Serv. Res. 2014, 14, 579. [Google Scholar] [CrossRef] [PubMed]
- Spilsbury, K.; Hewitt, C.; Stirk, L.; Bowman, C. The relationship between nurse staffing and quality of care in nursing homes: A systematic review. Int. J. Nurs. Stud. 2011, 48, 732–750. [Google Scholar] [CrossRef] [PubMed]
- Kohl, R.; Schwinger, A.; Jürchott, K.; Hering, C.; Gangnus, A.; Steinhagen-Thiessen, E.; Kuhlmey, A.; Gellert, P. Mortality among hospitalized nursing home residents with COVID-19. Dtsch. Arztebl. Int. 2022, 119, 293–294. [Google Scholar] [CrossRef] [PubMed]
- Joanna Briggs Institute. Critical Appraisal Tool 2020. Available online: https://jbi.global/critical-appraisal-tools (accessed on 25 May 2023).
- Taplin, S.H.; Price, R.A.; Edwards, H.M.; Foster, M.K.; Breslau, E.S.; Chollette, V.; Das, I.P.; Clauser, S.B.; Fennell, M.L.; Zapka, J. Introduction: Understanding and influencing multilevel factors across the cancer care continuum. J. Natl. Cancer Inst. Monogr. 2012, 2012, 2–10. [Google Scholar] [CrossRef] [PubMed]
- Lawrence, B.S. Levels of analysis and the qualitative study of quantitative data. In Multi-Level Issues in Organization Behavior and Processes; Francis, J., Yammarino, F.D., Eds.; Elsevier Science: Oxford, UK, 2004; pp. 231–250. [Google Scholar]
- Heras, E.; Garibaldi, P.; Boix, M.; Valero, O.; Castillo, J.; Curbelo, Y.; Gonzalez, E.; Mendoza, O.; Anglada, M.; Miralles, J.C.; et al. COVID-19 mortality risk factors in older people in a long-term care center. Eur. Geriatr. Med. 2021, 12, 601–607. [Google Scholar] [CrossRef] [PubMed]
- Ibrahim, J.E.; Li, Y.; McKee, G.; Eren, H.; Brown, C.; Aitken, G.; Pham, T. Characteristics of nursing homes associated with COVID-19 outbreaks and mortality among residents in Victoria, Australia. Australas. J. Ageing 2021, 40, 283–292. [Google Scholar] [CrossRef] [PubMed]
- Peckeu-Abboud, L.; Van Kleef, E.; Smekens, T.; Latour, K.; Dequeker, S.; Int Panis, L.; Laga, M. Factors influencing SARS-CoV-2 infection rate in Belgian nursing home residents during the first wave of COVID-19 pandemic. Epidemiol. Infect. 2022, 150, e72. [Google Scholar] [CrossRef]
- Frigotto, M.F.; Rodrigues, R.; Rabello, R.; Pietta-Dias, C. COVID-19 in older adult residents in nursing homes: Factors associated with mortality and impact on functional capacity. Sport Sci. Health 2023, 19, 527–535. [Google Scholar] [CrossRef]
- Akhtar-Danesh, N.; Baumann, A.; Crea-Arsenio, M.; Antonipillai, V. COVID-19 excess mortality among long-term care residents in Ontario, Canada. PLoS ONE 2022, 17, e0262807. [Google Scholar] [CrossRef] [PubMed]
- Brown, K.A.; Jones, A.; Daneman, N.; Chan, A.K.; Schwartz, K.L.; Garber, G.E.; Costa, A.P.; Stall, N.M. Association between nursing home crowding and COVID-19 infection and mortality in Ontario, Canada. JAMA Intern. Med. 2021, 181, 229–236. [Google Scholar] [CrossRef] [PubMed]
- Cox, M.B.; McGregor, M.J.; Poss, J.; Harrington, C. The association of facility ownership with COVID-19 outbreaks in long-term care homes in British Columbia, Canada: A retrospective cohort study. CMAJ Open 2023, 11, E267–E273. [Google Scholar] [CrossRef]
- Fisman, D.N.; Tuite, A.R.; Bogoch, I.; Lapointe-Shaw, L.; McCready, J. Risk factors associated with mortality among residents with coronavirus disease 2019 (COVID-19) in long-term care facilities in Ontario, Canada. JAMA Netw. Open 2020, 3, e2015957. [Google Scholar] [CrossRef] [PubMed]
- Kain, D.; Stall, N.; Brown, K.; McCreight, L.; Rea, E.; Kamal, M.; Brenner, J.; Verge, M.; Davies, R.; Johnstone, J. A longitudinal, clinical, and spatial epidemiologic analysis of a large COVID-19 long-term care home outbreak. J. Am. Med. Dir. Assoc. 2021, 22, 2003–2008.e2. [Google Scholar] [CrossRef]
- Lee, D.S.; Ma, S.; Chu, A.; Wang, C.X.; Wang, X.; Austin, P.C.; McAlister, F.A.; Kalmady, S.V.; Kapral, M.K.; Kaul, P.; et al. Predictors of mortality among long-term care residents with SARS-CoV-2 infection. J. Am. Geriatr. Soc. 2021, 69, 3377–3388. [Google Scholar] [CrossRef] [PubMed]
- Stall, N.M.; Jones, A.; Brown, K.A.; Rochon, P.A.; Costa, A.P. For-profit long-term care homes and the risk of COVID-19 outbreaks and resident deaths. Can. Med Assoc. J. 2020, 192, E1662–E1672. [Google Scholar] [CrossRef] [PubMed]
- Vijh, R.; Bharmal, A.; Ng, C.H.; Shirmaleki, M. Factors associated with transmission of COVID-19 in long-term care facility outbreaks. J. Hosp. Infect. 2022, 119, 118–125. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.S.; Charland, K.; Quach, C.; Nguyen, Q.D.; Zinszer, K. Institutional, therapeutic, and individual factors associated with 30-day mortality after COVID-19 diagnosis in Canadian long-term care facilities. J. Am. Geriatr. Soc. 2022, 70, 3210–3220. [Google Scholar] [CrossRef]
- Morciano, M.; Stokes, J.; Turner, A.J.; Kontopantelis, E.; Hall, I. Excess mortality for care home residents during the first 23 weeks of the COVID-19 pandemic in England: A national cohort study. BMC Med. 2021, 19, 71. [Google Scholar] [CrossRef]
- Shallcross, L.; Burke, D.; Abbott, O.; Donaldson, A.; Hallatt, G.; Hayward, A.; Hopkins, S.; Krutikov, M.; Sharp, K.; Wardman, L.; et al. Factors associated with SARS-CoV-2 infection and outbreaks in long-term care facilities in England: A national cross-sectional survey. Lancet Healthy Longev. 2021, 2, e129–e142. [Google Scholar] [CrossRef] [PubMed]
- Corvol, A.; Charras, K.; Prud’Homm, J.; Lemoine, F.; Ory, F.; Viel, J.F.; Somme, D. Structural and managerial risk factors for COVID-19 occurrence in French nursing homes. Int. J. Health Policy Manag. 2022, 11, 2630. [Google Scholar] [CrossRef] [PubMed]
- Piet, E.; Maillard, A.; Mallaval, F.O.; Dusseau, J.Y.; Galas-Haddad, M.; Ducki, S.; Creton, H.; Lallemant, M.; Forestier, E.; Gavazzi, G.; et al. Outbreaks of COVID-19 in nursing homes: A cross-sectional survey of 74 nursing homes in a French area. J. Clin. Med. 2021, 10, 4280. [Google Scholar] [CrossRef] [PubMed]
- Rabilloud, M.; Elsensohn, M.-H.; Riche, B.; Voirin, N.; Bénet, T.; Porcu, C.; Iwaz, J.; Étard, J.-F.; Vanhems, P.; Écochard, R. Stronger impact of COVID-19 in nursing homes of a french region during the second pandemic wave. J. Am. Med. Dir. Assoc. 2023, 24, 885–891.e3. [Google Scholar] [CrossRef] [PubMed]
- Rabilloud, M.; Riche, B.; Etard, J.F.; Elsensohn, M.-H.; Voirin, N.; Bénet, T.; Iwaz, J.; Ecochard, R.; Vanhems, P. COVID-19 outbreaks in nursing homes: A strong link with the coronavirus spread in the surrounding population, France, March to July 2020. PLoS ONE 2022, 17, e0261756. [Google Scholar] [CrossRef] [PubMed]
- Sacco, G.; Foucault, G.; Briere, O.; Annweiler, C. COVID-19 in seniors: Findings and lessons from mass screening in a nursing home. Maturitas 2020, 141, 46–52. [Google Scholar] [CrossRef]
- Tarteret, P.; Strazzulla, A.; Rouyer, M.; Gore, C.; Bardin, G.; Noel, C.; Benguerdi, Z.-E.; Berthaud, J.; Hommel, M.; Aufaure, S.; et al. Clinical features and medical care factors associated with mortality in French nursing homes during the COVID-19 outbreak. Int. J. Infect. Dis. 2021, 104, 125–131. [Google Scholar] [CrossRef] [PubMed]
- Preuß, B.; Fischer, L.; Schmidt, A.; Seibert, K.; Hoel, V.; Domhoff, D.; Heinze, F.; Brannath, W.; Wolf-Ostermann, K.; Rothgang, H. COVID-19 in German nursing homes: The impact of facilities’ structures on the morbidity and mortality of residents-an analysis of two cross-sectional surveys. Int. J. Environ. Res. Public Health 2023, 20, 610. [Google Scholar] [CrossRef] [PubMed]
- Kennelly, S.P.; Dyer, A.H.; Noonan, C.; Martin, R.; Kennelly, S.M.; Martin, A.; O’Neill, D.; Fallon, A. Asymptomatic carriage rates and case fatality of SARS-CoV-2 infection in residents and staff in irish nursing homes. Age Ageing 2021, 50, 49–54. [Google Scholar] [CrossRef]
- Cazzoletti, L.; Zanolin, M.E.; Tocco Tussardi, I.; Alemayohu, M.A.; Zanetel, E.; Visentin, D.; Fabbri, L.; Giordani, M.; Ruscitti, G.; Benetollo, P.P.; et al. Risk factors associated with nursing home COVID-19 outbreaks: A retrospective cohort study. Int. J. Environ. Res. Public Health 2021, 18, 8434. [Google Scholar] [CrossRef]
- Veronese, N.; Koyanagi, A.; Stangherlin, V.; Mantoan, P.; Chiavalin, M.; Tudor, F.; Pozzobon, G.; Tessarin, M.; Pilotto, A. Mortality attributable to COVID-19 in nursing home residents: A retrospective study. Aging Clin. Exp. Res. 2021, 33, 1745–1751. [Google Scholar] [CrossRef] [PubMed]
- Arienti, C.; Brambilla, L.; Campagnini, S.; Fanciullacci, C.; Giunco, F.; Mannini, A.; Patrini, M.; Tartarone, F.; Carrozza, M.C. Mortality and characteristics of older people dying with COVID-19 in lombardy nursing homes, Italy: An observational cohort study. J. Res. Med. Sci. 2021, 26, 40. [Google Scholar] [CrossRef] [PubMed]
- Cangiano, B.; Fatti, L.M.; Danesi, L.; Gazzano, G.; Croci, M.; Vitale, G.; Gilardini, L.; Bonadonna, S.; Chiodini, I.; Caparello, C.F.; et al. Mortality in an Italian nursing home during COVID-19 pandemic: Correlation with gender, age, adl, vitamin d supplementation, and limitations of the diagnostic tests. Aging 2020, 12, 24522. [Google Scholar] [CrossRef] [PubMed]
- Orlando, S.; Mazhari, T.; Abbondanzieri, A.; Cerone, G.; Ciccacci, F.; Liotta, G.; Mancinelli, S.; Marazzi, M.C.; Palombi, L. Characteristics of nursing homes and early preventive measures associated with risk of infection from COVID-19 in lazio region, italy: A retrospective case-control study. BMJ Open 2022, 12, e061784. [Google Scholar] [CrossRef]
- Lee, J.; Shin, J.H.; Lee, K.H.; Harrington, C.A.; Jung, S.O. Staffing levels and COVID-19 infections and deaths in Korean nursing homes. Policy Polit. Nurs. Pract. 2022, 23, 15–25. [Google Scholar] [CrossRef] [PubMed]
- Booij, J.A.; van de Haterd, J.C.; Huttjes, S.N.; van Deijck, R.H.; Koopmans, R.T. Short-and long-term mortality and mortality risk factors among nursing home patients after COVID-19 infection. J. Am. Med. Dir. Assoc. 2022, 23, 1274–1278. [Google Scholar] [CrossRef]
- Houben, F.; den Heijer, C.D.; Dukers-Muijrers, N.H.; Daamen, A.M.; Groeneveld, N.S.; Vijgen, G.C.; Martens, M.J.; Heijnen, R.W.; Hoebe, C.J. Facility- and ward-level factors associated with SARS-CoV-2 outbreaks among residents in long-term care facilities: A retrospective cohort study. Int. J. Infect. Dis. 2023, 130, 166–175. [Google Scholar] [CrossRef] [PubMed]
- Rutten, J.J.S.; van Loon, A.M.; van Kooten, J.; van Buul, L.W.; Joling, K.J.; Smalbrugge, M.; Hertogh, C.M.P.M. Clinical suspicion of COVID-19 in nursing home residents: Symptoms and mortality risk factors. J. Am. Med. Dir. Assoc. 2020, 21, 1791–1797.e1. [Google Scholar] [CrossRef] [PubMed]
- Visser, A.G.R.; Winkens, B.; Schols, J.M.G.A.; Janknegt, R.; Spaetgens, B. The impact of polypharmacy on 30-day covid-related mortality in nursing home residents: A multicenter retrospective cohort study. Eur. Geriatr. Med. 2022, 14, 51–57. [Google Scholar] [CrossRef]
- Arendse, T.; Cowper, B.; Cohen, C.; Masha, M.; Tempia, S.; Legodu, C.; Singh, S.; Ratau, T.; Geffen, L.; Heymans, A.; et al. SARS-CoV-2 cases reported from long-term residential facilities (care homes) in South Africa: A retrospective cohort study. BMC Public Health 2022, 22, 1035. [Google Scholar] [CrossRef]
- Agoües, A.B.; Gallego, M.S.; Resa, R.H.; Llorente, B.J.; Arabi, M.L.; Rodriguez, J.O.; Acebal, H.P.; Hernández, M.C.; Ayala, I.C.; Calero, P.P.; et al. Risk factors for COVID-19 morbidity and mortality in institutionalised elderly people. Int. J. Environ. Res. Public Health 2021, 18, 10221. [Google Scholar] [CrossRef] [PubMed]
- Aguilar-Palacio, I.; Maldonado, L.; Marcos-Campos, I.; Castel-Feced, S.; Malo, S.; Aibar, C.; Rabanaque, M.J. Understanding the COVID-19 pandemic in nursing homes (Aragon, Spain): Sociodemographic and clinical factors associated with hospitalization and mortality. Front. Public Health 2022, 10, 928174. [Google Scholar] [PubMed]
- Arnedo-Pena, A.; Romeu-Garcia, M.A.; Gascó-Laborda, J.C.; Meseguer-Ferrer, N.; Safont-Adsuara, L.; Prades-Vila, L.; Flores-Medina, M.; Rusen, V.; Tirado-Balaguer, M.D.; Sabater-Vidal, S.; et al. Incidence, mortality, and risk factors of COVID-19 in nursing homes. Epidemiologia 2022, 3, 179–190. [Google Scholar] [CrossRef] [PubMed]
- Escribà-Salvans, A.; Rierola-Fochs, S.; Farrés-Godayol, P.; Molas-Tuneu, M.; de Souza, D.L.B.; Skelton, D.A.; Goutan-Roura, E.; Minobes-Molina, E.; Jerez-Roig, J. Risk factors for developing symptomatic COVID-19 in older residents of nursing homes: A hypothesis-generating observational study. J. Frailty Sarcopenia Falls 2023, 8, 74–82. [Google Scholar] [CrossRef] [PubMed]
- Romero, M.M.; Céspedes, A.A.; Sahuquillo, M.T.T.; Zamora, E.B.C.; Ballesteros, C.G.; Alfaro, V.S.-F.; Bru, R.L.; Utiel, M.L.; Cifuentes, S.C.; Longobardo, L.M.P.; et al. COVID-19 outbreak in long-term care facilities from Spain. Many lessons to learn. PLoS ONE 2020, 15, e0241030. [Google Scholar]
- Meis-Pinheiro, U.; Lopez-Segui, F.; Walsh, S.; Ussi, A.; Santaeugenia, S.; Garcia-Navarro, J.A.; San-Jose, A.; Andreu, A.L.; Campins, M.; Almirante, B. Clinical characteristics of COVID-19 in older adults. A retrospective study in long-term nursing homes in Catalonia. PLoS ONE 2021, 16, e0255141. [Google Scholar] [CrossRef] [PubMed]
- Soldevila, L.; Prat, N.; Mas, M.À.; Massot, M.; Miralles, R.; Bonet-Simó, J.M.; Isnard, M.; Expósito-Izquierdo, M.; Garcia-Sanchez, I.; Rodoreda-Noguerola, S.; et al. The interplay between infection risk factors of SARS-CoV-2 and mortality: A cross-sectional study from a cohort of long-term care nursing home residents. BMC Geriatr. 2022, 22, 123. [Google Scholar] [CrossRef] [PubMed]
- San Román, J.; Candel, F.J.; del Mar Carretero, M.; Sanz, J.C.; Pérez-Abeledo, M.; Barreiro, P.; Viñuela-Prieto, J.M.; Ramos, B.; Canora, J.; Barba, R.; et al. Cross-sectional analysis of risk factors for outbreak of COVID-19 in nursing homes for older adults in the community of Madrid. Gerontology 2023, 69, 163–171. [Google Scholar] [CrossRef]
- Suñer, C.; Ouchi, D.; Mas, M.À.; Lopez Alarcon, R.; Massot Mesquida, M.; Prat, N.; Bonet-Simó, J.M.; Expósito Izquierdo, M.; Garcia Sánchez, I.; Rodoreda Noguerola, S.; et al. A retrospective cohort study of risk factors for mortality among nursing homes exposed to COVID-19 in Spain. Nat. Aging 2021, 1, 579–584. [Google Scholar] [CrossRef] [PubMed]
- Cooper, C. United States Nursing Homes and Health Equity during the COVID-19 Pandemic; Georgia Southern University: Statesboro, GA, USA, 2021. [Google Scholar]
- Torres, M.L.; Díaz, D.P.; Oliver-Parra, A.; Millet, J.-P.; Cosialls, D.; Guillaumes, M.; Rius, C.; Vásquez-Vera, H. Inequities in the incidence and mortality due to COVID-19 in nursing homes in Barcelona by characteristics of the nursing homes. PLoS ONE 2022, 17, e0269639. [Google Scholar] [CrossRef]
- Zunzunegui, M.V.; Beland, F.; Rico, M.; Lopez, F.J.G. Long-term care home size association with COVID-19 infection and mortality in Catalonia in March and April 2020. Epidemiologia 2022, 3, 369–390. [Google Scholar] [CrossRef] [PubMed]
- Scanferla, G.; Héquet, D.; Graf, N.; Münzer, T.; Kessler, S.; Kohler, P.; Nussbaumer, A.; Petignat, C.; Schlegel, M.; Flury, D. COVID-19 burden and influencing factors in swiss long-term-care facilities: A cross-sectional analysis of a multicentre observational cohort. Swiss Med. Wkly. 2023, 153, 40052. [Google Scholar] [CrossRef] [PubMed]
- Abrams, H.R.; Loomer, L.; Gandhi, A.; Grabowski, D.C. Characteristics of US nursing homes with COVID-19 cases. J. Am. Geriatr. Soc. 2020, 68, 1653–1656. [Google Scholar] [CrossRef] [PubMed]
- Adler, L.; Lipton, C.; Watson, C.C.; Lawrence, S.; Richie, A.; Spain, C.; Heltemes, K. Mortality reduction associated with coexistent antithrombotic use in nursing home residents with COVID-19. J. Am. Med. Dir. Assoc. 2022, 23, 440–441. [Google Scholar] [CrossRef] [PubMed]
- Bui, D.P.; See, I.; Hesse, E.M.; Varela, K.; Harvey, R.R.; August, E.M.; Winquist, A.; Mullins, S.; McBee, S.; Thomasson, E.; et al. Association between cms quality ratings and COVID-19 outbreaks in nursing homes—West Virginia, March 17–June 11, 2020. MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 1300–1304. [Google Scholar] [CrossRef]
- Cai, S.; Yan, D.; Intrator, O. COVID-19 cases and death in nursing homes: The role of racial and ethnic composition of facilities and their communities. J. Am. Med. Dir. Assoc. 2021, 22, 1345–1351. [Google Scholar] [CrossRef] [PubMed]
- Chatterjee, P.; Kelly, S.; Qi, M.; Werner, R.M. Characteristics and quality of US nursing homes reporting cases of coronavirus disease 2019 (COVID-19). JAMA Netw. Open 2020, 3, e2016930. [Google Scholar] [CrossRef] [PubMed]
- Chen, A.T.; Ryskina, K.L.; Yun, H.; Jung, H.Y. Nursing home characteristics associated with resident COVID-19 morbidity in communities with high infection rates. JAMA Netw. Open 2021, 4, e211555. [Google Scholar] [CrossRef]
- Chen, M.K.; Chevalier, J.A.; Long, E.F. Nursing home staff networks and COVID-19. Proc. Natl. Acad. Sci. USA 2020, 118, e2015455118. [Google Scholar] [CrossRef]
- Cronin, C.J.; Evans, W.N. Nursing home quality, COVID-19 deaths, and excess mortality. J. Health Econ. 2022, 82, 102592. [Google Scholar] [CrossRef]
- Dean, A.; Venkataramani, A.; Kimmel, S. Mortality rates from COVID-19 are lower in unionized nursing homes. Health Aff. 2020, 39, 1993–2001. [Google Scholar] [CrossRef] [PubMed]
- Figueroa, J.F.; Wadhera, R.K.; Papanicolas, I.; Riley, K.; Zheng, J.; Orav, E.J.; Jha, A.K. Association of nursing home ratings on health inspections, quality of care, and nurse staffing with COVID-19 cases. JAMA 2020, 324, 1103–1105. [Google Scholar] [CrossRef] [PubMed]
- Engeda, J.C.; Karmarkar, E.N.; Mitsunaga, T.M.; Raymond, K.L.; Oh, P.; Epson, E. Resident racial and ethnic composition, neighborhood-level socioeconomic status, and COVID-19 infections in California snfs. J. Am. Geriatr. Soc. 2023, 71, 157–166. [Google Scholar] [CrossRef] [PubMed]
- Gilman, M.; Bassett, M.T. Trends in COVID-19 death rates by racial composition of nursing homes. J. Am. Geriatr. Soc. 2021, 69, 2442–2444. [Google Scholar] [CrossRef] [PubMed]
- Gopal, R.; Han, X.; Yaraghi, N. Compress the curve: A cross-sectional study of variations in COVID-19 infections across California nursing homes. BMJ Open 2021, 11, e042804. [Google Scholar] [CrossRef] [PubMed]
- Gorges, R.J.; Konetzka, R.T. Staffing levels and COVID-19 cases and outbreaks in U.S. Nursing homes. J. Am. Geriatr. Soc. 2020, 68, 2462–2466. [Google Scholar] [CrossRef] [PubMed]
- Gorges, R.J.; Konetzka, R.T. Factors associated with racial differences in deaths among nursing home residents with COVID-19 infection in the us. JAMA Netw. Open 2021, 4, e2037431. [Google Scholar] [CrossRef] [PubMed]
- Harrington, C.; Ross, L.; Chapman, S.; Halifax, E.; Spurlock, B.; Bakerjian, D. Nurse staffing and coronavirus infections in California nursing homes. Policy Politics Nurs. Pract. 2020, 21, 174–186. [Google Scholar] [CrossRef] [PubMed]
- He, M.; Fang, F.; Li, Y. Is there a link between nursing home reported quality and COVID-19 cases? Evidence from California skilled nursing facilities. J. Am. Med. Dir. Assoc. 2020, 21, 905–908. [Google Scholar] [CrossRef] [PubMed]
- Hege, A.; Lane, S.; Spaulding, T.; Sugg, M.; Iyer, L.S. County-level social determinants of health and COVID-19 in nursing homes, United States, June 1, 2020–January 31, 2021. Public Health Rep. 2022, 137, 137–148. [Google Scholar] [CrossRef]
- Hill, T.E.; Farrell, D.J. COVID-19 across the landscape of long-term care in alameda county: Heterogeneity and disparities. Gerontol. Geriatr. Med. 2022, 8, 23337214211073419. [Google Scholar] [CrossRef]
- Hua, C.L.; Cornell, P.Y.; Zimmerman, S.; Carder, P.; Thomas, K.S. Excess mortality among assisted living residents with dementia during the COVID-19 pandemic. J. Am. Med. Dir. Assoc. 2022, 23, 1743–1749.e6. [Google Scholar] [CrossRef] [PubMed]
- Iyanda, A.E.; Boakye, K.A. A 2-year pandemic period analysis of facility and county-level characteristics of nursing home coronavirus deaths in the United States, January 1, 2020-December 18, 2021. Geriatr. Nurs. 2022, 44, 237–244. [Google Scholar] [CrossRef]
- Khairat, S.; Zalla, L.C.; Adler-Milstein, J.; Kistler, C.E. US nursing home quality ratings associated with COVID-19 cases and deaths. J. Am. Med. Dir. Assoc. 2021, 22, 2021–2025.e1. [Google Scholar] [PubMed]
- Kim, S.J.; Hollender, M.; DeMott, A.; Oh, H.; Bhatia, I.; Eisenberg, Y.; Gelder, M.; Hughes, S. COVID-19 cases and deaths in skilled nursing facilities in cook county, Illinois. Public Health Rep. 2022, 137, 564–572. [Google Scholar] [CrossRef] [PubMed]
- Kumar, A.; Baldwin, J.A.; Roy, I.; Karmarkar, A.M.; Erler, K.S.; Rudolph, J.L.; Rivera-Hernandez, M. Shifting US patterns of COVID-19 mortality by race and ethnicity from June–December 2020. J. Am. Med. Dir. Assoc. 2021, 22, 966–970.e3. [Google Scholar] [CrossRef] [PubMed]
- Lane, S.J.; Sugg, M.; Spaulding, T.J.; Hege, A.; Iyer, L. Southeastern United States predictors of COVID-19 in nursing homes. J. Appl. Gerontol. 2022, 41, 1641–1650. [Google Scholar] [CrossRef]
- Levy-Storms, L.; Mueller-Williams, A. Certified nursing aides’ training hours and covid case and mortality rates across states in the U.S.: Implications for infection prevention and control and relationships with nursing home residents. Front. Public Health 2022, 10, 798779. [Google Scholar] [CrossRef]
- Longo, B.A.; Barrett, S.C.; Schmaltz, S.P.; Williams, S.C. A multistate comparison study of COVID-19 cases among accredited and nonaccredited nursing homes. Policy Polit. Nurs. Pract. 2022, 23, 26–31. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Temkin-Greener, H.; Shan, G.; Cai, X. COVID-19 infections and deaths among connecticut nursing home residents: Facility correlates. J. Am. Geriatr. Soc. 2020, 68, 1899–1906. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Temkin-Greener, H.; Cen, X.; Cai, X. Racial and ethnic disparities in COVID-19 infections and deaths across U.S. Nursing homes. J. Am. Geriatr. Soc. 2020, 68, 2454–2461. [Google Scholar] [CrossRef]
- Li, Y.; Cai, X.Y.; Mao, Y.J.; Cheng, Z.J.; Temkin-Greener, H. Trends in racial and ethnic disparities in coronavirus disease 2019 (COVID-19) outcomes among nursing home residents. Infect. Control. Hosp. Epidemiol. 2022, 43, 997–1003. [Google Scholar] [CrossRef] [PubMed]
- Lord, J.; Davlyatov, G.; Ghiasi, A.; Weech-Maldonado, R. Nursing homes located in socially deprived communities have been disproportionately affected by COVID-19. J. Health Care Financ. 2021, 48, 1–12. [Google Scholar]
- Lu, Y.; Jiao, Y.; Graham, D.J.; Wu, Y.; Wang, J.; Menis, M.; Chillarige, Y.; Wernecke, M.; Kelman, J.; Forshee, R.A.; et al. Risk factors for COVID-19 deaths among elderly nursing home medicare beneficiaries in the prevaccine period. J. Infect. Dis. 2022, 225, 567–577. [Google Scholar] [CrossRef] [PubMed]
- Mattingly, T.J.; Trinkoff, A.; Lydecker, A.D.; Kim, J.J.; Yoon, J.M.; Roghmann, M.C. Short-stay admissions associated with large COVID-19 outbreaks in Maryland nursing homes. Gerontol. Geriatr. Med. 2021, 7, 23337214211063103. [Google Scholar] [CrossRef]
- McGarry, B.E.; Gandhi, A.D.; Grabowski, D.C.; Barnett, M.L. Larger nursing home staff size linked to higher number of COVID-19 cases in 2020. Health Aff. 2021, 40, 1261–1269. [Google Scholar] [CrossRef] [PubMed]
- Mehta, H.B.; Li, S.; Goodwin, J.S. Risk factors associated with SARS-CoV-2 infections, hospitalization, and mortality among US nursing home residents. JAMA Netw. Open 2021, 4, e216315. [Google Scholar] [CrossRef] [PubMed]
- Olson, A.; Rajgopal, S.; Bai, G. Comparison of resident COVID-19 mortality between unionized and nonunionized private nursing homes. PLoS ONE 2022, 17, e0276301. [Google Scholar] [CrossRef] [PubMed]
- Panagiotou, O.A.; Kosar, C.M.; White, E.M.; Bantis, L.E.; Yang, X.; Santostefano, C.M.; Feifer, R.A.; Blackman, C.; Rudolph, J.L.; Gravenstein, S.; et al. Risk factors associated with all-cause 30-day mortality in nursing home residents with COVID-19. JAMA Intern. Med. 2021, 181, 439–448. [Google Scholar] [CrossRef] [PubMed]
- Shen, K. Relationship between nursing home COVID-19 outbreaks and staff neighborhood characteristics. PLoS ONE 2022, 17, e0267377. [Google Scholar] [CrossRef]
- Shi, S.M.; Travison, T.G.; Berry, S.D.; Bakaev, I.; Chen, H. Risk factors, presentation, and course of coronavirus disease 2019 in a large, academic long-term care facility. J. Am. Med. Dir. Assoc. 2020, 21, 1378–1383.e1. [Google Scholar] [CrossRef]
- Sugg, M.M.; Spaulding, T.J.; Lane, S.J.; Runkle, J.D.; Harden, S.R.; Hege, A.; Iyer, L.S. Mapping community-level determinants of COVID-19 transmission in nursing homes: A multi-scale approach. Sci. Total Environ. 2021, 752, 141946. [Google Scholar] [CrossRef] [PubMed]
- Tang, O.; Bigelow, B.F.; Sheikh, F.; Peters, M.; Zenilman, J.M.; Bennett, R.; Katz, M.J. Outcomes of nursing home COVID-19 patients by initial symptoms and comorbidity: Results of universal testing of 1970 residents. J. Am. Med. Dir. Assoc. 2020, 21, 1767–1773.e1. [Google Scholar] [CrossRef] [PubMed]
- Thorsness, R.; Raines, N.H.; White, E.M.; Santostefano, C.M.; Parikh, S.M.; Riester, M.R.; Feifer, R.A.; Mor, V.; Zullo, A.R. Association of kidney function with 30-day mortality following SARS-CoV-2 infection in nursing home residents: A retrospective cohort study. Am. J. Kidney Dis. 2022, 79, 305–307. [Google Scholar] [CrossRef]
- Travers, J.L.; Wu, B.; Agarwal, M.; Estrada, L.V.; Stone, P.W.; Dick, A.W.; Gracner, T. Assessment of coronavirus disease 2019 infection and mortality rates among nursing homes with different proportions of black residents. J. Am. Med. Dir. Assoc. 2021, 22, 893–898.e2. [Google Scholar] [CrossRef] [PubMed]
- Weech-Maldonado, R.; Orewa, G.; Lord, J.; Davlyatov, G.; Ghiasi, A. High-minority nursing homes disproportionately affected by COVID-19 deaths. Front. Public Health 2021, 9, 606364. [Google Scholar] [CrossRef] [PubMed]
- Williams, C.S.; Zheng, Q.; White, A.J.; Bengtsson, A.I.; Shulman, E.T.; Herzer, K.R.; Fleisher, L.A. The association of nursing home quality ratings and spread of COVID-19. J. Am. Geriatr. Soc. 2021, 69, 2070–2078. [Google Scholar] [CrossRef] [PubMed]
- Young, Y.; Shayya, A.; O’Grady, T.; Chen, Y.M. COVID-19 case and mortality rates lower in green houses compared to traditional nursing homes in New York state. Geriatr. Nurs. 2023, 50, 132–137. [Google Scholar] [CrossRef] [PubMed]
- Zhu, X.; Lee, H.; Yang, H.; Lee, C.; Sang, H.; Muller, J.; Ory, M. Nursing home design and COVID-19: Implications for guidelines and regulation. J. Am. Med. Dir. Assoc. 2022, 23, 272–279.e1. [Google Scholar] [CrossRef] [PubMed]
- Zimmerman, S.; Tandan, M.; Wretman, C.J.; Preisser, J.S.; Dumond-Stryker, C.; Howell, A.; Ryan, S. Nontraditional small house nursing homes have fewer COVID-19 cases and deaths. J. Am. Med. Dir. Assoc. 2021, 22, 489–493. [Google Scholar] [CrossRef]
- Emmerson, C.; Hollinghurst, J.; North, L.; Fry, R.; Akbari, A.; Humphreys, C.; Gravenor, M.B.; Lyons, R.A. The impact of dementia, frailty and care home characteristics on SARS-CoV-2 incidence in a national cohort of welsh care home residents during a period of high community prevalence. Age Ageing 2022, 51, afac250. [Google Scholar] [CrossRef]
- Beobide Telleria, I.; Ferro Uriguen, A.; Laso Lucas, E.; Sannino Menicucci, C.; Enriquez Barroso, M.; Lopez de Munain Arregui, A. Risk factors associated with COVID-19 infection and mortality in nursing homes. Aten. Primaria 2022, 54, 102463. [Google Scholar] [CrossRef]
- Ouslander, J.G.; Grabowski, D.C. COVID-19 in nursing homes: Calming the perfect storm. J. Am. Geriatr. Soc. 2020, 68, 2153–2162. [Google Scholar] [CrossRef] [PubMed]
- Gibson, D.M.; Greene, J. State actions and shortages of personal protective equipment and staff in US nursing homes. J. Am. Geriatr. Soc. 2020, 68, 2721–2726. [Google Scholar] [CrossRef]
- Naughton, S.X.; Raval, U.; Pasinetti, G.M. Potential novel role of COVID-19 in Alzheimer’s disease and preventative mitigation strategies. J. Alzheimer’s Dis. 2020, 76, 21–25. [Google Scholar] [CrossRef]
- Saragih, I.D.; Batubara, S.O.; Lin, C.J.; Saragih, I.S. Dementia as a mortality predictor among older adults with COVID-19: A systematic review and meta-analysis of observational study. Geriatr. Nurs. 2021, 42, 1230–1239. [Google Scholar] [CrossRef]
- Broms, R.; Dahlstrom, C.; Nistotskaya, M. Provider ownership and indicators of service quality: Evidence from swedish residential care homes. J. Public Adm. Res. Theory 2023, 34, 150–163. [Google Scholar] [CrossRef]
- Fosdick, B.K.; Bayham, J.; Dilliott, J.; Ebel, G.D.; Ehrhart, N. Model-based evaluation of policy impacts and the continued COVID-19 risk at long term care facilities. Infect. Dis. Model. 2022, 7, 463–472. [Google Scholar] [CrossRef]
- Patterson, P.B.; Weinberg, T.; McRae, S.; Pollack, C.; Dutton, D. Long-term care staffing policies pre-COVID-19 and pandemic responses: A case comparison of Ontario and British Columbia. Can. Public Policy-Anal. De Polit. 2023, 49, 94–113. [Google Scholar] [CrossRef]
- Bach-Mortensen, A.M.; Verboom, B.; Movsisyan, A.; Degli Esposti, M. A systematic review of the associations between care home ownership and COVID-19 outbreaks, infections and mortality. Nat. Aging 2021, 1, 948–961. [Google Scholar] [CrossRef]
- Kruse, F.M.; Mah, J.C.; Metsemakers, S.J.; Andrew, M.K.; Sinha, S.K.; Jeurissen, P.P. Relationship between the ownership status of nursing homes and their outcomes during the COVID-19 pandemic: A rapid literature review. J. Long-Term Care, 2021; 207–220. [Google Scholar] [CrossRef]
- Solmi, M.; Cobey, K.D.; Moher, D.; Ebrahimzadeh, S.; Dragioti, E.; Shin, J.I.; Radua, J.; Cortese, S.; Shea, B.; Veronese, N.; et al. Development of a reporting guideline for umbrella reviews on epidemiological associations using cross-sectional, case-control, and cohort studies: The preferred reporting items for umbrella reviews of cross-sectional, case-control, and cohort studies (priur-ccc). medRxiv 2022. medRxiv:28.22283572. [Google Scholar]
- Mitjà, O.; Reis, G.; Boulware, D.R.; Spivak, A.M.; Sarwar, A.; Johnston, C.; Webb, B.; Hill, M.D.; Smith, D.; Kremsner, P.; et al. Hydroxychloroquine for treatment of non-hospitalized adults with COVID-19: A meta-analysis of individual participant data of randomized trials. Clin. Transl. Sci. 2023, 16, 524–535. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| First Author | Year | Time Frame Data Collection | Country/ Region | Outcome Type | Objectives | LTCF # | Study Design | Factors’ Level | AA/EA |
|---|---|---|---|---|---|---|---|---|---|
| Heras [20] | 2021 | 15 March 2020 to 5 June 2020 | Andorra | M | Identification of the COVID-19 mortality risk factors in older people from a long-term care center | - | Cross-sectional | Indiv | + |
| Ibrahim [21] | 2021 | 7 July to 13 November 2020 | Australia/Victoria | O and M | Investigation of the LTCFs characteristics, including organizational and facility structures, location, and access to acute health care, associated with the COVID-19 outbreak | 766 | Cross-sectional | Org, Envi | - |
| Peckeu-Abboud [22] | 2022 | 8 April 2022, to 15 May 2020 | Belgium | O | Identification of the factors influencing SARS-CoV-2 infection rate in Belgian LTCFs residents during the first wave of the COVID-19 pandemic | 695 | Cross-sectional | Indiv, Org | + |
| Frigotto [23] | 2023 | 5 November to 31 December 2020 | Brazil | O | Investigation of whether the functional capacity prior to COVID-19 infection was different between survivor and non-survivor older adults | 2 | Cross-sectional | Indiv | - |
| Akhtar -Danesh [24] | 2022 | January 2019 to December 2020 | Canada/Ontario | O and M | Determination of the scale of pandemic-related deaths of long-term care residents in the province of Ontario, Canada, and to estimate excess mortality due to a positive COVID-19 test adjusted for demographics and regional variations | 626 | Cohort | Indiv, Org, Envi | + |
| Brown [25] | 2021 | 29 March 2020 to 20 May 2020 | Canada/Ontario | O and M | Determination of whether crowding was associated with COVID-19 cases and mortality in the first months of the COVID-19 epidemic | 618 | Cross-sectional | Indiv, Org, Envi | + |
| Cox [26] | 2023 | 1 March 2020, to 31 January 2021 | Canada/British Columbia | O and M | Assessment of whether facility ownership was associated with COVID-19 outbreaks among LTCFs | 293 | Cross-sectional | Org, Envi | + |
| Fisman [27] | 2020 | March 2020 to April 2020 | Canada/Ontario | O and M | Identification of the trends and risk factors associated with COVID-19 death in LTCFs in Ontario, Canada | 627 | Cohort | Org, Envi | + |
| Kain [28] | 2021 | 1 March to 21 May 2020 | Canada/Ontario | O | Understanding of the way in which the virus spreads within these homes is critical to preventing further outbreaks. | 1 | Cross-sectional | Indiv, Org, Envi | - |
| Lee [29] | 2021 | 1 January to 31 August 2020 | Canada/Ontario | M | Understanding of the contributions to mortality among SARS-CoV-2-infected residents in LTC homes | - | Cross-sectional | Indiv | + |
| Stall [30] | 2020 | 29 March to 20 May 2020 | Canada/Ontario | O and M | Examination of the association between for-profit status and the risk of COVID-19 outbreaks and death during the peak of the epidemic in Ontario’s LTC homes | 623 | Cross-sectional | Org, Envi | + |
| Vijh [31] | 2021 | 1 March 2020, to 10 January 2021 | Canada/British Columbia | O | Identification of the risk factors associated with outbreak severity to inform current outbreak management and future pandemic preparedness planning efforts | 48 | Cross-sectional | Indiv, Org, Envi | + |
| Zhang [32] | 2022 | 23 February to 11 July 2020 | Canada/Montreal | M | Identification of the individual, therapeutic, and institutional factors associated with death in LTCFs | 17 | Cross-sectional | Indiv, Org | + |
| Morciano [33] | 2021 | 1 January 2017, to 7 August 2020 | England | M | Investigation of the excess mortality for care home residents during the COVID-19 pandemic in England, exploring associations with care home characteristics | 4428 | Cohort | Indiv, Org, Envi | + |
| Shallcross [34] | 2021 | 26 May to 19 June 2020 | England | O | Identification of the factors associated with SARS-CoV-2 infection and outbreaks among staff and residents in LTCFs | 5126 | Cross-sectional | Indiv, Org, Envi | + |
| Corvol [35] | 2022 | 1 March to 31 May 2020 | France/Brittany | O | Identification of the structural and managerial factors associated with COVID-19 outbreaks in LTCFs | 231 | Cross-sectional | Indiv, Org, Envi | + |
| Piet [36] | 2021 | 1 March to 31 May 2020 | France/French Alps | O and M | Identification of the relationship between the occurrence of an outbreak of COVID-19 among residents and staff members | 225 | Cross-Sectional | Indiv, Org, Envi | + |
| Rabilloud [37] | 2023 | 1 March to 31 July 2020, and 1 August to 31 December 2020 | France/Auvergne-Rhône-Alpes | O and M | Quantification of the effects of characteristics of LTCFs and their surroundings on the spread of COVID-19 outbreaks and assessment of the changes in resident protection between the first 2 waves | 937 | Cross-sectional | Org, Envi | + |
| Rabilloud [38] | 2022 | 1 March to 31 July 2020 | France/Auvergne-Rhône-Alpes | O | Identification of the role SARS-CoV-2 virus spread in nearby population plays in introducing the disease in LTCFs | 943 | Cross-sectional | Indiv | - |
| Sacco [39] | 2020 | Prior to 17 March 2020 | France/Maine-et-Loire | O | Comprehensive description of the symptoms and chronological aspects of the diffusion of the SARS-CoV-2 virus in an LTCF, among both residents and caregivers | 1 | Cross-sectional | Indiv | + |
| Tarteret [40] | 2021 | 18 March to 10 April 2020 | France/Ile-de-France | M | Identification of the demographic, clinical, and medical care factors associated with mortality in LTCF residents | 3 | Cross-sectional | Indiv, Org | + |
| Preuß [41] | 2023 | 28 April to 12 May 2020 and 12 January to 7 February 2021 | Germany | O and M | Identification of the impact of Facilities’ Structures on the Morbidity and Mortality of Residents | 824 and 385 during 1st and 2nd waves, respectively | Cross-Sectional | Org, Envi | + |
| Kennelly [42] | 2021 | 29 February to 22 May 2020 | Ireland | O and M | Examination of characteristics of LTCFs across three Irish Community Health Organisations, proportions with COVID-19 outbreaks, staff and resident infection rates, symptom profile and resident case fatality | 45 | Cross-Sectional | Indiv, Org, Envi | - |
| Cazzoletti [43] | 2021 | March to May 2020 | Italy/Trento | O | Examination of the association between certain measurable factors (structural, organizational, and practice-related) and the cumulative incidence of COVID-19 among LTCF residents in the Autonomous Province of Trento, Italy, during the peak of the COVID-19 outbreak | 57 | Cross-sectional | Indiv, Org, Envi | + |
| Veronese [44] | 2021 | 1 March to 31 December 2020. | Italy/Venice | M | Examination of whether COVID-19 was associated with a higher mortality rate in LTCF residents, considering frailty status assessed with the Multidimensional Prognostic Index | 31 | Cross-sectional | Indiv | + |
| Arienti [45] | 2021 | 1 March to 7 May 2020 | Italy/Lombardy | O and M | Description of the epidemiological characteristics of LTCF residents infected by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection and to compute the related case-fatality rate | 6 | Cross-sectional | Indiv | - |
| Cangiano [46] | 2020 | March to April 2020 | Italy | Quantification of the impact of SARS-CoV-2 on mortality in LTCFs and to point out the factors related to its severity as well as the limitations of diagnostic tests used to manage the spread of this infective disease | 1 | Prospective | Indiv | - | |
| Orlando [47] | 2022 | March to December 2020 | Italy/Lazio | O | Understanding of which organizational–structural characteristics of LTCFs associated with the risk of a COVID-19 outbreak | 100 | Case–control | Org, Envi | + |
| Lee [48] | 2022 | 20 January to 20 October 2020 | Korea | O and M | Examination of the organizational factors and characteristics of NH related to the COVD-19 outbreak and mortality during the COVID-19 pandemic’s peak | 3389 | Cross-sectional | Org | + |
| Booij [49] | 2022 | March to November 2020 | Netherlands | O and M | Investigation of short- and long-term mortality and risk factors in LTCFs patients with COVID-19 | 2 | Cross-sectional | Indiv | + |
| Houben [50] | 2023 | September 2020 to June 2021 | Netherlands/South Limburg | O | Identification of the facility- and ward-level factors associated with SARS-CoV-2 outbreaks among LTCF residents | 60 | Cross-sectional | Org, Envi | + |
| Rutten [51] | 2020 | 18 March to 13 May 2020. | Netherlands | O and M | Description of the symptomatology, mortality, and risk factors for mortality in a large group of Dutch LTCF residents with clinically suspected COVID-19 who were tested with a reverse transcription–polymerase chain reaction (RT–PCR) test | NI | Prospective | Indiv | + |
| Visser [52] | 2023 | March 2020 to December 2021 | Netherland | M | Identification of the impact of polypharmacy on 30-day COVID-related mortality after adjustment for age, sex, CCI, BMI, and vaccination status | 15 | Cross-sectional | Indiv | + |
| Arendse [53] | 2022 | 5 March 2020 to 31 July 2022 | South Africa | M | Description of the temporal trends as well as the characteristics and risk factors for mortality | 45 | Cross-sectional | Indiv | + |
| Agoües [54] | 2021 | 15 March to 15 May 2020 | Spain/Sant Cugat del Vallès | O and M | Identification of the factors related to morbidity and mortality of COVID-19 | 12 | Cross-sectional | Indiv, Envi | + |
| Aguilar-Palacio [55] | 2022 | 9 March 2020 to 14 March 2021 | Spain/Aragón | O and M | Description of the profile of institutionalized patients with a confirmed COVID-19 infection and the socioeconomic and morbidity factors associated with hospitalization and death | 1 | Cross-sectional | Indiv | + |
| Arnedo-Pena [56] | 2022 | March 2020 to January 2021 | Spain/Castellon | O and M | Investigation of the incidence and mortality of COVID-19 in LTCFs, and their associated risk factors, before starting the vaccination against the disease | 27 | Cross-sectional | Indiv, Org, Envi | + |
| Escribà-Salvan [57] | 2022 | December 2019 to March 2021 | Spain/Central Catalonia | O | Identification of the risk factors associated with developing COVID-19 infection with symptoms in institutionalized older people | 5 | Longitudinal | Indiv, Org | + |
| Romero [58] | 2020 | March 2020 to 5 April 2020 | Spain/Albacete | O and M | Investigation of the mortality, costs, residents, and personnel characteristics in six long-term care facilities (LTCFs) during the outbreak of COVID-19 in Spain | 6 | Cross-sectional | Indiv | - |
| Meis-Pinheiro [59] | 2021 | 1 March to 31 May 2020 | Spain/Catalonia | O | Identification of the clinical characteristics of COVID-19 in older adults in LTCFs | 80 | Cross-sectional | Indiv | + |
| Soldevila [60] | 2021 | 1 March to 30 June 2020 | Spain/Barcelona in Catalonia | O and M | Identification of the interplay between infection risk factors of SARS-CoV-2 and prognosis | 168 | Cross-Sectional | Indiv, Envi | + |
| San Román [61] | 2023 | July to December 2020 | Spain/Madrid | O | Identification of the factors that facilitate COVID-19 outbreaks in LTCFs | 369 | Cross-sectional | Indiv, Org | + |
| Suñer [62] | 2021 | March to 1 June 2020, | Spain/Catalonia | M | Investigation of the determinants of mortality in LTC facilities during the COVID-19 outbreak | 167 | Cross-sectional | Indiv, Org, Envi | + |
| Telleria [63] | 2022 | March to December 2020 | Spain/Guipúzcoa | O and M | Identification of the association of demographic, clinical, and pharmacological risk factors with the COVID-19 infection, and related death | 4 | Case–control | Indiv | + |
| Torres [64] | 2022 | March to June 2020 | Spain/Barcelona | O and M | Identification of the inequalities in the cumulative incidences (CIs) and in the mortality rates (MRs) due to COVID-19 | 232 | Longitudinal | Org, Envi | + |
| Zunzunegui [65] | 2022 | March to April 2020 | Spain/Catalonia | O and M | Understanding how COVID-19 infection and mortality varied according to facility size | 965 | Cross-Sectional | Org, Envi | + |
| Scanferla [66] | 2023 | February 2020 to 31 May 2021 | Swiss | O and M | Identification of the influencing factors for a higher COVID-19 burden | 59 | Cross-sectional | Indiv, Org, Envi | + |
| Abrams [67] | 2020 | By 11 May 2020 | USA | O | Examination of the characteristics of LTCFs with documented COVID-19 cases in 30 states reporting individual facilities affected | 9395 | Cross-Sectional | Indiv, Org, Envi | + |
| Adler [68] | 2022 | 1 March 2020, and 31 May 2020 | USA | M | Evaluation of the impact of the underlying use of antithrombotic on the 30-day mortality of individuals with COVID-19 and to assess the relationship between age and sex with 30-day all-cause mortality in patients with COVID-19 | NI | Cross-sectional | Indiv | + |
| Bagchi [6] | 2021 | 25 May to 22 November 2020 | USA | O | Identification of the rates of COVID-19 among residents and staff members in LTCFs | 15,342 | Cross-sectional | Org, Envi | - |
| Bui [69] | 2020 | 17 March to 11 June 2020 | USA/West Virginia | O | Identification of the relationship of the quality of LTCFs (using star ratings) and COVID-19 outbreak | 123 | Cross-Sectional | Org, Envi | + |
| Cai [70] | 2021 | 7 June 2020 to 23 August 2020 | USA | O and M | Examination of the racial and ethnic composition of LTCFs and communities with relation to the COVID-19 cases and death in LTCFs | 13,123 | Cross-sectional | Indiv, Org, Envi | + |
| Chatterjee [71] | 2020 | 22 April to 29 April 2020 | USA/23 states and the District of Columbia | O | Description of the characteristics and quality of LTCFs with COVID-19 cases in states where public health departments have begun to publicly report their statuses | 8943 | Cross-sectional | Org, Envi | - |
| Chen [72] | 2021 | By 11 October 2020 | USA | O | Identification of association between LTCF characteristics and resident COVID-19 morbidity in communities with high infection rates | 2017 | Cross-sectional | Indiv, Org, Envi | + |
| Chen [73] | 2020 | 13 April to 23 August 2020 | USA | O | Investigation of LTCF staff networks and COVID-19 | 13,165 | Cross-sectional | Indiv, Org, Envi | + |
| Cooper [63] | 2021 | June 2020 to January 2021 | USA | O and M | Determination of whether LTCFs COVID-19 patient outcomes varied from one nursing facility to another based on location and resident characteristics, and the availability of COVID-19-specific medical equipment in the LTCFs impacts morbidity and mortality outcomes. | 14,405 | Cross-sectional | Indiv, Org, Envi | + |
| Cronin [74] | 2022 | May 2020 to September 2021 | USA | O and M | Investigation of whether high-quality LTCFs measured by the CMS five-star ratings did a better job of preventing deaths from COVID-19 | 14,905 | Cohort | Org, Envi | + |
| Dean [75] | 2020 | 1 March to 31 May 2020 | USA/New York | O and M | Identification of the association between the presence of healthcare worker unions and additional facility-level factors and COVID-19 mortality rates | 355 | Cross-sectional | Indiv, Org, Envi | + |
| Figueroa [76] | 2020 | 1 January to 30 June 2020 | USA/8 states | O | Evaluation of whether LTCFs, rated highly by the Centers for Medicare & Medicaid Services (CMS) across 3 unique domains—health inspections, quality measures, and nurse staffing—had lower COVID-19 cases than facilities with lower ratings | 4254 | Cross-sectional | Org, Envi | + |
| Engeda [77] | 2023 | 25 May to 16 August 2020 | USA/California | O | Identification of the association between LTCFs COVID-19 infections and level of racial and ethnic compositions and facility- and neighborhood-level (census tract- and county-level) indicators of socioeconomic status | 971 | Cross-sectional | Indiv, Envi | + |
| Gilman [78] | 2021 | 25 May 2020, to 18 April 2021 | USA | M | Identification of the trends in COVID-19 death rates by the racial composition of LTCFs through mid-April 2021 | 13,820 | Cross-sectional | Indiv | - |
| Gopal [79] | 2021 | 1 May 2020 | USA/California | O | Understanding of why some LTCFs are more susceptible to larger COVID-19 outbreaks. | 713 | Cross-sectional | Org, Envi | + |
| Gorges [80] | 2020 | 25 June 2020 | USA | O and M | Understanding of whether baseline nurse staffing is associated with the presence of COVID-19 in LTCFs and whether staffing impacts outbreak severity | 13,167 | Cross-sectional | Indiv, Org, Envi | + |
| Gorges [81] | 2021 | 1 January 2020, to 13 September 2020 | USA | M | Description of differences in the number of COVID-19 deaths by LTCFs racial composition and examine the factors associated with these differences | 13,312 | Cross-sectional | Indiv, Org, Envi | + |
| Harrington [82] | 2020 | March to 4 May 2020 | USA/California | O | Examination of the relationship of nurse staffing in California LTCFs and compare homes with and without COVID-19 residents | 1091 | Cross-sectional | Org, Envi | + |
| He [83] | 2020 | 2 June 2020 | USA/California | O and M | Determination of whether COVID-19 cases and deaths are related to the LTCFs reported quality | 1223 | Cross-sectional | Indiv, Org, Envi | + |
| Hege [84] | 2021 | 1 June 2020, to 31 January 2021 | USA | O | Investigation of the relationship between US LTCF-associated COVID-19 infection rates and county-level and LTCFs attributes | 9990 | Cohort | Indiv, Org, Envi | + |
| Hill [85] | 2022 | March 2020 to March 2021 | USA/Alameda | M | Identification of the differential impacts across settings as well as racial and economic disparities among long-term care residents with relation to COVID-19-related death | 592 | Cross-sectional | Indiv | - |
| Hua [86] | 2022 | 12 March to 31 December 2020 and 1 January 2019, to 11 March 2020 | USA | M | Comparison of the weekly rate of excess all-cause mortality during the first several months of the COVID-19 pandemic among residents with ADRD in assisted living to those without ADRD and among residents with ADRD in memory care assisted living or in general assisted living | NI | Cross-sectional | Indiv | + |
| Iyanda [87] | 2022 | 1 January 2020 to 18 December 2021 | USA | M | Examination of the determinants of COVID-19 deaths in LTCFs in the first 2-year pandemic period | 13,350 | Cross-sectional | Org, Envi | + |
| Khairat [88] | 2021 | 25 May to 20 December 2020 | USA | O and M | Identification of the relationship between LTCFs’ quality and the spread and severity of COVID-19 in LTCFs | 15,390 | Cross-sectional | Org, Envi | + |
| Kim [89] | 2022 | 1 January to 30 September 2021 | USA/Illinois | O and M | Examination of the pathways through which community and facility factors may have affected COVID-19 cases and deaths | 177 | Cross-sectional | Indiv, Org, Envi | + |
| Kumar [90] | 2021 | 1 June to 27 December 2020 | USA | O and M | Examination of the impact of a high proportion of minority residents in LTCFs on COVID-19-related mortality rates over a 30-week period. | 11,718 | Longitudinal | Indiv, Org, Envi | + |
| Lane [91] | 2022 | May to September 2020, September to December 2020, and December to February 2021 | USA-Southern | O | Identification of the LTCFs and county-level predictors of COVID-19 outbreaks in LTCFs in the southeastern region of the United States across three time periods. | 2951 | Longitudinal | Indiv, Org, Envi | + |
| Levy-Storms [92] | 2022 | 1 January 2020 to 2 July 2021 | USA | O and M | Determination of the role of Certified Nursing Aides (CNAs) in the care of residents living in LTCFs | - | Cross-sectional | Org | - |
| Longo [93] | 2022 | June 2020 to January 2021 | USA/Illinois, Florida, and Massachusetts | O | To compare COVID-19 cases among accredited and nonaccredited LTCFs | Cross-sectional | Envi | + | |
| Li [94] | 2020 | By 16 April 2020 | USA | O and M | Determination of the associations of LTCFs registered nurse (RN) staffing, overall quality of care, and concentration of Medicaid or racial and ethnic minority residents with 2019 coronavirus disease (COVID-19) confirmed cases and deaths | 215 | Cross-sectional | Indiv, Org, Envi | + |
| Li [95] | 2020 | 25 May to 31 May 2020 | USA | O and M | Determination of the racial/ethnic disparities in weekly counts of new COVID-19 cases and deaths among LTCFs residents or staff | 12,576 | Cross-sectional | Indiv, Org, Envi | + |
| Li [96] | 2022 | 13 April to 19 June 2020 | USA | O and M | Evaluation of the trends in racial and ethnic disparities in weekly cumulative rates of coronavirus disease 2019 (COVID-19) cases and deaths | 211 | Longitudinal | Indiv | + |
| Lord [97] | 2021 | 1 January 2020 to 11 July 2021 | USA | O | Examination of the relationship between community resource scarcity, as conceptualized by the Social Deprivation Index (SD), and COVID-19 incidence rates in LTCFs. | 13,772 | Cross-sectional | Indiv, Org, Envi | + |
| Lu [98] | 2021 | 1 April 2020 to 22 December 2020 | USA | M | Evaluation of risk factors for COVID-19 deaths and hospitalizations among LTCFs Medicare beneficiaries in the prevaccine pandemic period. | - | Cross-sectional | Indiv, Org, Envi | + |
| Mattingly [99] | 2021 | 1 January to 1 July 2020 | USA/Maryland | O | Identification of the characteristics associated with large outbreaks | 216 | Cross-sectional | Indiv, Org, Envi | + |
| McGarry [100] | 2021 | By 30 September 2020 | USA | O and M | Examination of how the number of unique staff members might influence the likelihood of COVID-19 cases and deaths in LTCFs | 15,071 | Cross-sectional | Indiv, Org, Envi | + |
| Mehta [101] | 2021 | 1 April to 30 September 2020 | USA | O and M | Identification of the risk factors for SARS-CoV-2 incidence, hospitalization, and mortality among LTCF residents in the US | 482, 323 | Cross-sectional | Indiv | + |
| Olson [102] | 2022 | 24 April 2022 | USA | O and M | Understanding of the association between LTCFs unionization and resident COVID-19 mortality percentage | 14,380 | Cross-sectional | Indiv, Org, Envi | + |
| Panagiotou [103] | 2021 | 16 March to 15 September 2020 | USA | M | Identification of the risk factors for 30-day all-cause mortality among US LTCF residents with COVID-19. | 5256 | Cross-sectional | Indiv | + |
| Shen [104] | 2022 | 5 July–10 July 2020 | USA/18 states | M | Examination of the relationship between LTCFs COVID-19 outbreaks and differences in the characteristics of the residential neighbourhoods | 6132 | Cross-sectional | Indiv, Org, Envi | + |
| Shi [105] | 2020 | 16 March to 8 May 2020 | USA/Boston, MA | O and M | Description of the clinical characteristics and risk factors associated with coronavirus disease 2019 (COVID-19) in long-stay LTCF residents | 1 | Cross-sectional | Indiv | + |
| Sugg [106] | 2021 | By 30 June 2020 | USA | O and M | Determination of the association between LTCF-level metrics and county-level, place-based variables with COVID-19 confirmed cases in LTCFs across the United States | 13,709 | Cross-sectional | Org, Envi | + |
| Tang [107] | 2020 | 1 March to 12 June 2020 | USA/Maryland | M | Identification of the association of symptom status and medical comorbidities on mortality and hospitalization risk associated with COVID-19 | 15 | Cross-sectional | Indiv | + |
| Thorsness [108] | 2022 | 1 March to 31 December 2020 | USA | M | Identification of the association of kidney function with 30-day mortality following COVID-19 infection | 176 | Cross-sectional | Indiv | + |
| Travers [109] | 2021 | 20 January to 19 July 2020 | USA | O and M | Examination of the associations between the proportion of Black residents in LTCFs and COVID-19 infections and deaths, accounting for structural bias (operationalized as county-level factors) and stratifying by urbanicity/rurality | 11,587 | Cross-sectional | Indiv, Org, Envi | + |
| Unruh [2] | 2020 | 20 January–30 April 2020 | USA/Connecticut, New Jersey, and New York | M | Evaluation of the characteristics of LTCFs with COVID-19 deaths compared to other LTCFs using data from Connecticut, New Jersey, and New York | 1162 | Cross-sectional | Indiv, Org, Envi | + |
| Weech-Maldonado [110] | 2021 | 1 January to 25 October 2020 | USA | M | Examination of the relationship between LTCFs racial/ethnic mix and COVID-19 resident mortality | 12,914 | Cross-sectional | Indiv, Org, Envi | + |
| Williams [111] | 2021 | 10 January 2021 | USA | O and M | Understanding of the relationship of LTCFs quality ratings and measures of COVID-19 outbreak severity and persistence | 14,693 | Cross-sectional | Indiv, Org, Envi | + |
| Young [112] | 2023 | 31 May 2020 to 27 March 2022 | USA/New York | O and M | Evaluation of the COVID-19 case and mortality rates in green houses compared to traditional LTCFs in New York state | 608 | Cross-sectional | Org | - |
| Zhu [113] | 2022 | 7 June to 20 December 2020 | USA | O and M | Examination of the associations of LTCFs design with COVID-19 cases, deaths, and transmissibility and provide relevant design recommendations | 7785 | Cross-sectional | Indiv, Org, Envi | + |
| Zimmerman [114] | 2021 | 20 January to 31 July 2020 | USA | O and M | Comparison of the rates of COVID-19 infections, COVID-19 admissions/readmissions, and COVID-19 mortality, among Green House/small LTCFs with rates in other LTCFs | 43 | Cross-sectional | Org | - |
| Emmerson [115] | 2022 | 1 September to 31 December 2020 | Wales | O | Identification of the impact of dementia, frailty, and care home characteristics on SARS-CoV-2 incidence in a national cohort of Welsh care home residents during a period of high community prevalence | 673 | Cross-sectional | Indiv, Org, Envi | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Karimi-Dehkordi, M.; Hanson, H.M.; Silvius, J.; Wagg, A. Drivers of COVID-19 Outcomes in Long-Term Care Facilities Using Multi-Level Analysis: A Systematic Review. Healthcare 2024, 12, 807. https://doi.org/10.3390/healthcare12070807
Karimi-Dehkordi M, Hanson HM, Silvius J, Wagg A. Drivers of COVID-19 Outcomes in Long-Term Care Facilities Using Multi-Level Analysis: A Systematic Review. Healthcare. 2024; 12(7):807. https://doi.org/10.3390/healthcare12070807
Chicago/Turabian StyleKarimi-Dehkordi, Mehri, Heather M. Hanson, James Silvius, and Adrian Wagg. 2024. "Drivers of COVID-19 Outcomes in Long-Term Care Facilities Using Multi-Level Analysis: A Systematic Review" Healthcare 12, no. 7: 807. https://doi.org/10.3390/healthcare12070807
APA StyleKarimi-Dehkordi, M., Hanson, H. M., Silvius, J., & Wagg, A. (2024). Drivers of COVID-19 Outcomes in Long-Term Care Facilities Using Multi-Level Analysis: A Systematic Review. Healthcare, 12(7), 807. https://doi.org/10.3390/healthcare12070807