
The Role of Diet and Physical Activity in Shaping COVID-19 Severity: Design, Validation, and Application of a Retrospective Questionnaire
 , ,
, ,  , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Questionnaire Design
2.2. Questionnaire Validation
2.3. Questionnaire Application
2.4. Participants
2.5. Measuring Lifetime Physical Activity and Sedentary Patterns
2.6. Ethical Considerations
2.7. Statistical Analysis
3. Results
3.1. Questionnaire Validation
3.2. Description of the Study Sample
Social and Demographic Characteristics
3.3. Significant Correlations among Study Participants
Social and Demographic Characteristics
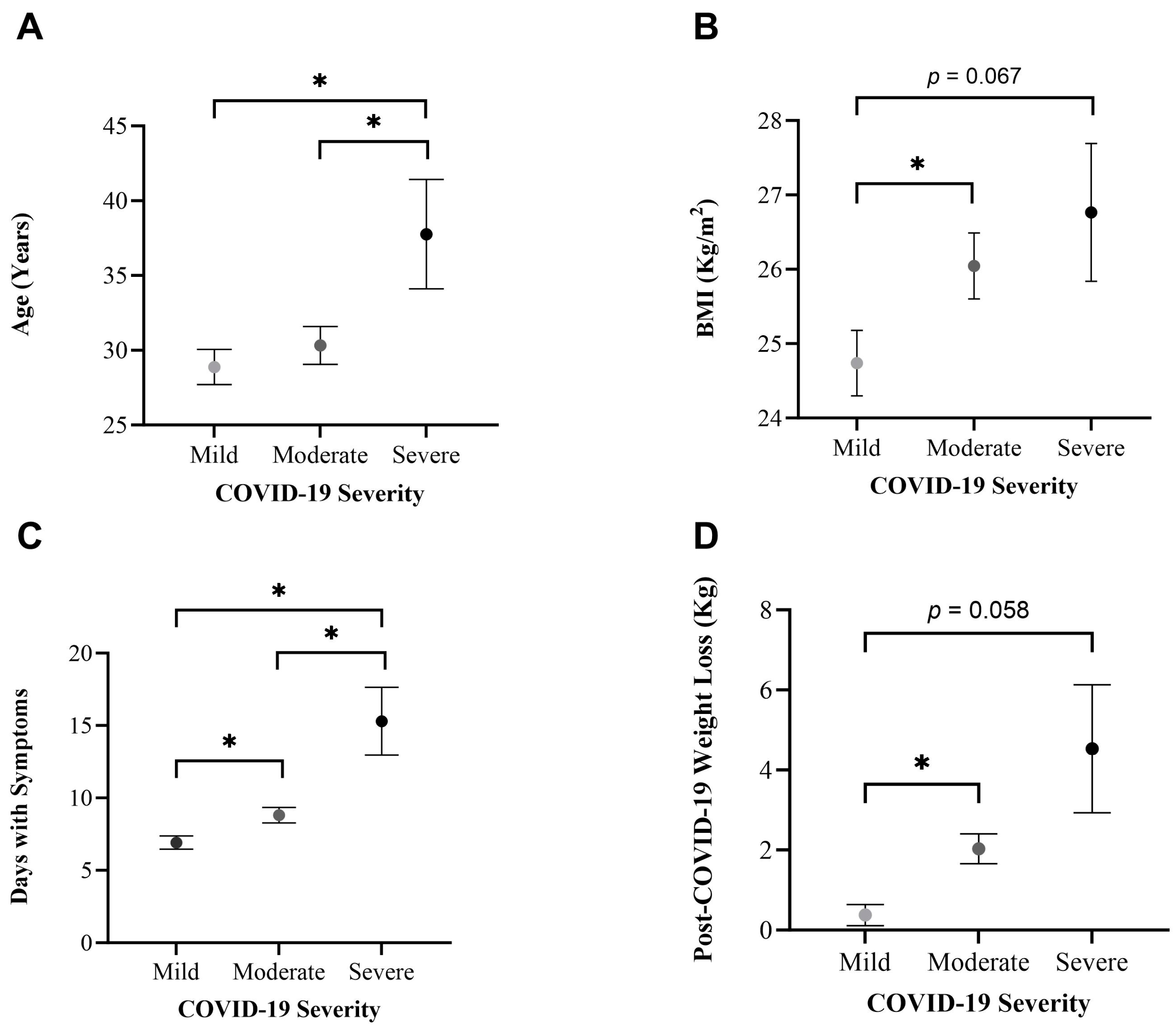
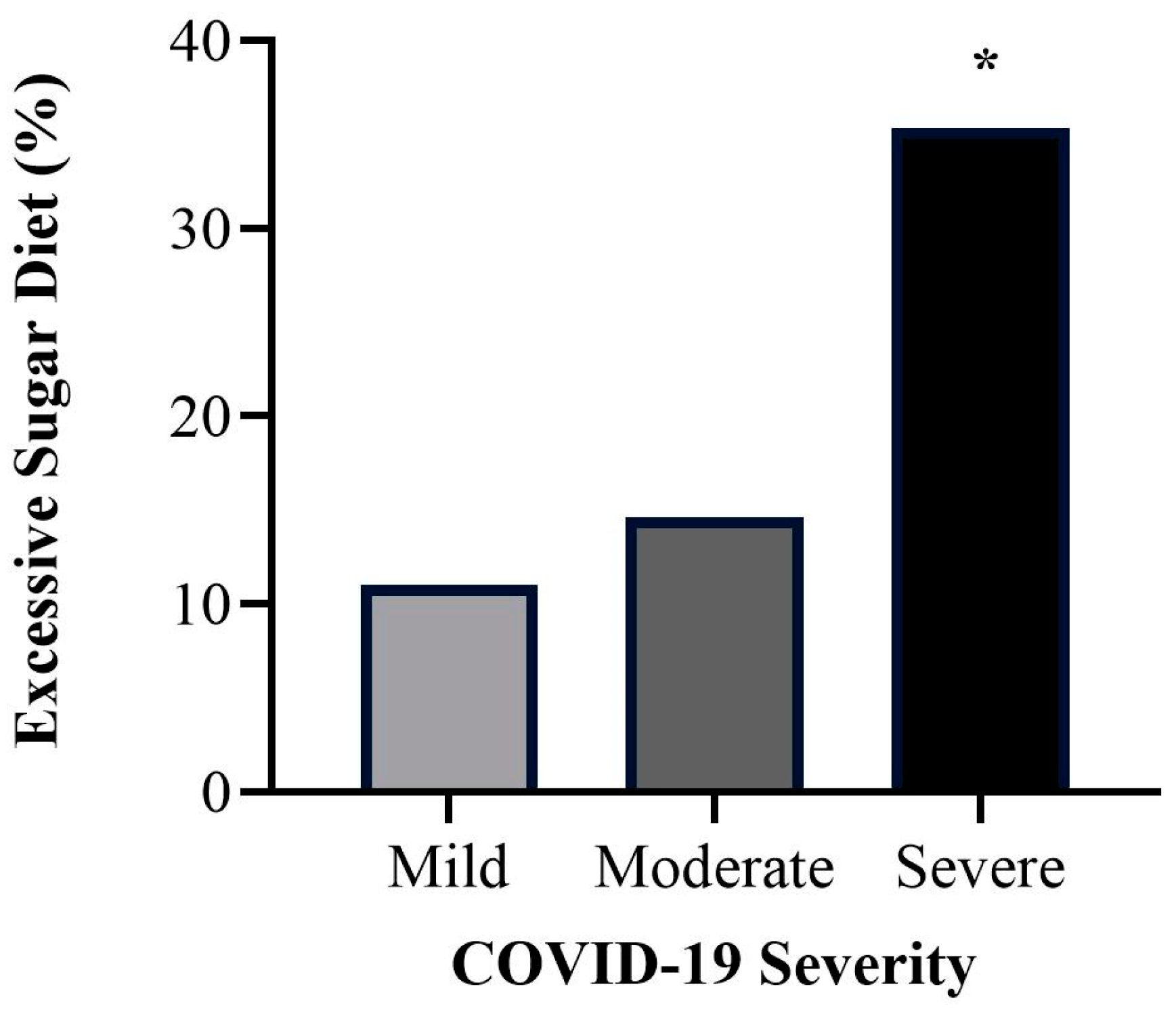
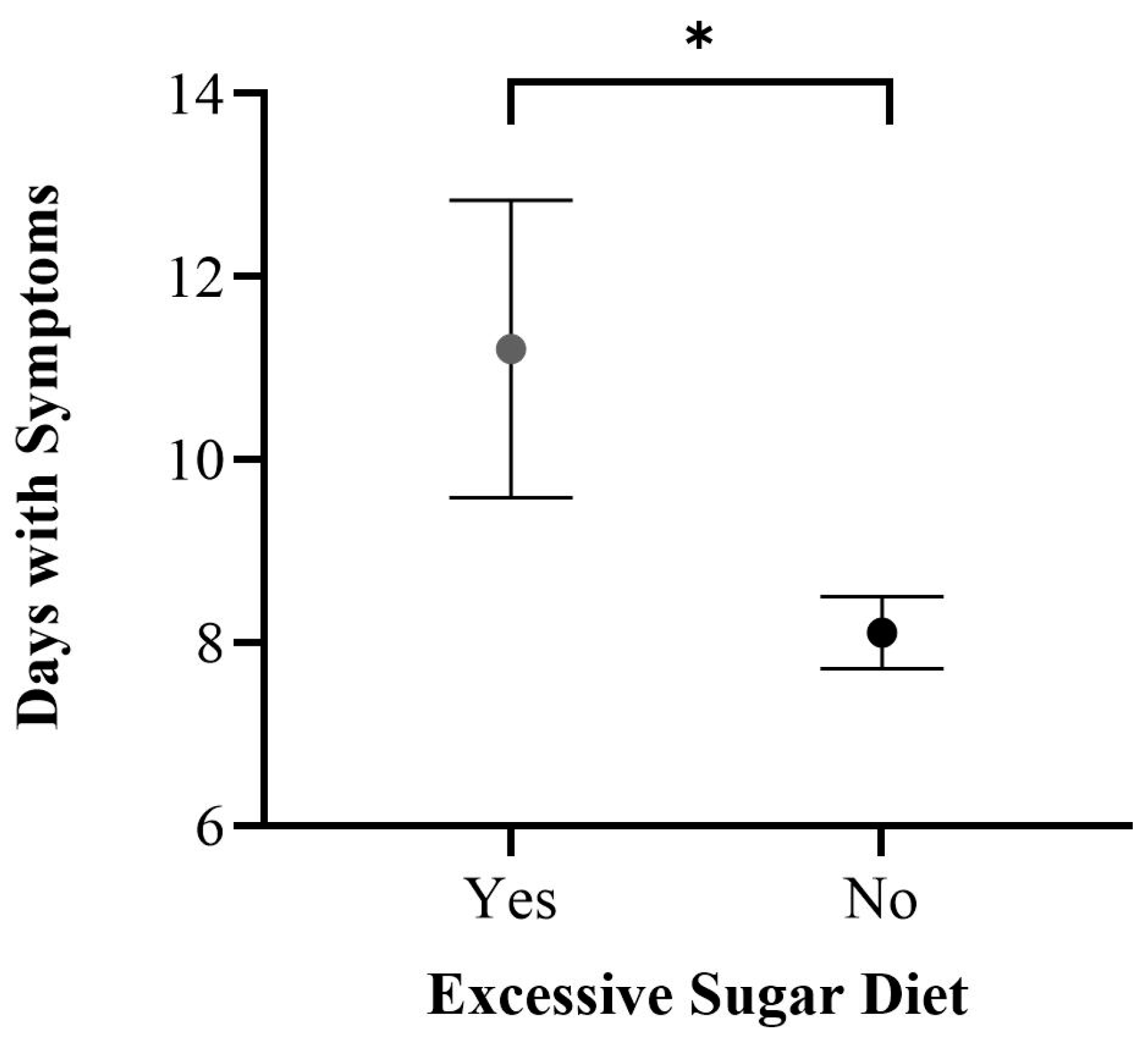
3.4. Differences per COVID-19 Severity
3.4.1. Dietary Patterns
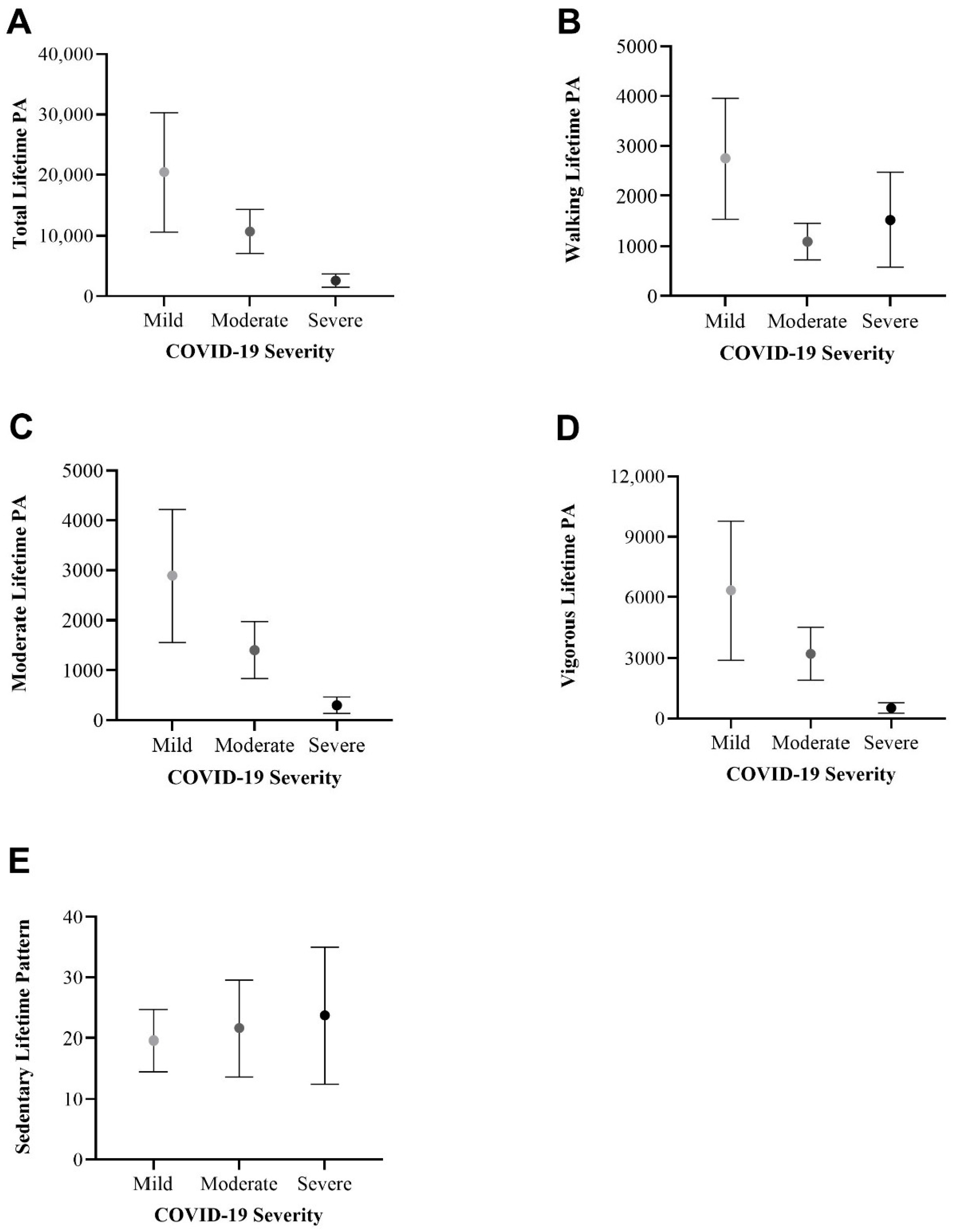
3.4.2. Physical Activity Patterns
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- WHO Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int (accessed on 28 February 2024).
- Woods, J.A.; Hutchinson, N.T.; Powers, S.K.; Roberts, W.O.; Gomez-Cabrera, M.C.; Radak, Z.; Berkes, I.; Boros, A.; Boldogh, I.; Leeuwenburgh, C.; et al. The COVID-19 Pandemic and Physical Activity. Sports Med. Health Sci. 2020, 2, 55–64. [Google Scholar] [CrossRef] [PubMed]
- CDC. COVID-19. Centers for Disease Control and Prevention. Available online: https://www.cdc.gov/coronavirus/2019-ncov/hcp/clinical-care/underlyingconditions.html (accessed on 28 January 2024).
- Steenkamp, L.; Saggers, R.T.; Bandini, R.; Stranges, S.; Choi, Y.-H.; Thornton, J.S.; Hendrie, S.; Patel, D.; Rabinowitz, S.; Patricios, J. Small Steps, Strong Shield: Directly Measured, Moderate Physical Activity in 65,361 Adults Is Associated with Significant Protective Effects from Severe COVID-19 Outcomes. Br. J. Sports Med. 2022, 56, 568–577. [Google Scholar] [CrossRef]
- Sallis, R.; Young, D.R.; Tartof, S.Y.; Sallis, J.F.; Sall, J.; Li, Q.; Smith, G.N.; Cohen, D.A. Physical Inactivity Is Associated with a Higher Risk for Severe COVID-19 Outcomes: A Study in 48,440 Adult Patients. Br. J. Sports Med. 2021, 55, 1099–1105. [Google Scholar] [CrossRef]
- U.S. Department of Health and Human Services. Physical Activity Guidelines for Americans, 2nd Edition. 2018. Available online: https://health.gov/sites/default/files/2019-09/Physical_Activity_Guidelines_2nd_edition.pdf (accessed on 12 January 2024).
- Bennett, D.A.; Du, H.; Clarke, R.; Guo, Y.; Yang, L.; Bian, Z.; Chen, Y.; Millwood, I.; Yu, C.; He, P.; et al. Association of Physical Activity with Risk of Major Cardiovascular Diseases in Chinese Men and Women. JAMA Cardiol. 2017, 2, 1349. [Google Scholar] [CrossRef] [PubMed]
- Uusitupa, M.; Khan, T.A.; Viguiliouk, E.; Kahleova, H.; Rivellese, A.A.; Hermansen, K.; Pfeiffer, A.; Thanopoulou, A.; Salas-Salvadó, J.; Schwab, U.; et al. Prevention of Type 2 Diabetes by Lifestyle Changes: A Systematic Review and Meta-Analysis. Nutrients 2019, 11, 2611. [Google Scholar] [CrossRef]
- Merino, J.; Joshi, A.D.; Nguyen, L.H.; Leeming, E.R.; Mazidi, M.; Drew, D.A.; Gibson, R.; Graham, M.S.; Lo, C.-H.; Capdevila, J.; et al. Diet Quality and Risk and Severity of COVID-19: A Prospective Cohort Study. Gut 2021, 70, 2096–2104. [Google Scholar] [CrossRef]
- Gomide, E.B.G.; Abdalla, P.P.; Pisa, M.F.; Schneider, G.; Vieira, L.G.; Mazzonetto, L.F.; De Sousa Oliveira, A.; Sebastião, E.; Dos Santos, A.P. The Role of Physical Activity in the Clinical Outcomes of People Diagnosed with COVID-19: A Systematic Review. JSAMS Plus 2022, 1, 100007. [Google Scholar] [CrossRef] [PubMed]
- Rahmati, M.; Shamsi, M.M.; Khoramipour, K.; Malakoutinia, F.; Woo, W.; Park, S.; Yon, D.K.; Lee, S.W.; Shin, J.I.; Smith, L. Baseline Physical Activity Is Associated with Reduced Mortality and Disease Outcomes in COVID-19: A Systematic Review and Meta-analysis. Rev. Med. Virol. 2022, 32, e2349. [Google Scholar] [CrossRef]
- Ezzatvar, Y.; Ramírez-Vélez, R.; Izquierdo, M.; Garcia-Hermoso, A. Physical Activity and Risk of Infection, Severity and Mortality of COVID-19: A Systematic Review and Non-Linear Dose–Response Meta-Analysis of Data from 1,853,610 Adults. Br. J. Sports Med. 2022, 56, 1188–1193. [Google Scholar] [CrossRef]
- Hamer, M.; Kivimäki, M.; Gale, C.R.; Batty, G.D. Lifestyle Risk Factors, Inflammatory Mechanisms, and COVID-19 Hospitalization: A Community-Based Cohort Study of 387,109 Adults in UK. Brain Behav. Immun. 2020, 87, 184–187. [Google Scholar] [CrossRef]
- Brandenburg, J.P.; Lesser, I.A.; Thomson, C.J.; Giles, L.V. Does Higher Self-Reported Cardiorespiratory Fitness Reduce the Odds of Hospitalization from COVID-19? J. Phys. Act. Health 2021, 18, 782–788. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.W.; Lee, J.; Moon, S.Y.; Jin, H.Y.; Yang, J.M.; Ogino, S.; Song, M.; Hong, S.H.; Ghayda, R.A.; Kronbichler, A.; et al. Physical Activity and the Risk of SARS-CoV-2 Infection, Severe COVID-19 Illness and COVID-19 Related Mortality in South Korea: A Nationwide Cohort Study. Br. J. Sports Med. 2022, 56, 901–912. [Google Scholar] [CrossRef] [PubMed]
- Craig, C.L.; Marshall, A.L.; Sjöström, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.; et al. International Physical Activity Questionnaire: 12-Country Reliability and Validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef] [PubMed]
- Hernadnez-Nieto, R.A. Contributions to Statistical Analysis; Universidad de Los Andes: Bogotá, Colombia, 1992. [Google Scholar]
- Arámburo-Gálvez, J.; Carvalho Gomes, I.; André, T.; Beltrán-Cárdenas, C.; Macêdo-Callou, M.; Braga Rocha, É.; Mye-Takamatu-Watanabe, E.; Rahmeier-Fietz, V.; Figueroa-Salcido, O.; Cárdenas-Torres, F.; et al. Translation, Cultural Adaptation, and Evaluation of a Brazilian Portuguese Questionnaire to Estimate the Self-Reported Prevalence of Gluten-Related Disorders and Adherence to Gluten-Free Diet. Medicina 2019, 55, 593. [Google Scholar] [CrossRef] [PubMed]
- Szigriszt-Pazos, F. Sistemas Predictivos de Legilibilidad Del Mensaje Escrito: Fórmula de Perspicuidad. Ph.D. Thesis, Universidad Complutense, Madrid, Spain, 2001. [Google Scholar]
- Barrio-Cantalejo, I.M.; Simón-Lorda, P.; Melguizo, M.; Escalona, I.; Marijuán, M.I.; Hernando, P. Validation of the INFLESZ Scale to Evaluate Readability of Texts Aimed at the Patient. An. Sist. Sanit. Navar. 2008, 31, 132–152. [Google Scholar]
- Wu, Z.; McGoogan, J.M. Characteristics of and Important Lessons from the Coronavirus Disease 2019 (COVID-19) Outbreak in China: Summary of a Report of 72,314 Cases from the Chinese Center for Disease Control and Prevention. JAMA 2020, 323, 1239. [Google Scholar] [CrossRef] [PubMed]
- Ashok, P.; Kharche, J.; Raju, R.; Godbole, G. Metabolic Equivalent Task Assessment for Physical Activity in Medical Students. Natl. J. Physiol. Pharm. Pharmacol. 2017, 7, 236. [Google Scholar] [CrossRef]
- Herrmann, S.D.; Willis, E.A.; Ainsworth, B.E.; Barreira, T.V.; Hastert, M.; Kracht, C.L.; Schuna, J.M.; Cai, Z.; Quan, M.; Tudor-Locke, C.; et al. 2024 Adult Compendium of Physical Activities: A Third Update of the Energy Costs of Human Activities. J. Sport Health Sci. 2024, 13, 6–12. [Google Scholar] [CrossRef]
- Chesnut, W.M.; MacDonald, S.; Wambier, C.G. Could Diet and Exercise Reduce Risk of COVID-19 Syndemic? Med. Hypotheses 2021, 148, 110502. [Google Scholar] [CrossRef]
- O’Connor, L.; Imamura, F.; Brage, S.; Griffin, S.J.; Wareham, N.J.; Forouhi, N.G. Intakes and Sources of Dietary Sugars and Their Association with Metabolic and Inflammatory Markers. Clin. Nutr. 2018, 37, 1313–1322. [Google Scholar] [CrossRef]
- Furman, D.; Campisi, J.; Verdin, E.; Carrera-Bastos, P.; Targ, S.; Franceschi, C.; Ferrucci, L.; Gilroy, D.W.; Fasano, A.; Miller, G.W.; et al. Chronic Inflammation in the Etiology of Disease across the Life Span. Nat. Med. 2019, 25, 1822–1832. [Google Scholar] [CrossRef] [PubMed]
- Chastin, S.F.M.; Abaraogu, U.; Bourgois, J.G.; Dall, P.M.; Darnborough, J.; Duncan, E.; Dumortier, J.; Pavón, D.J.; McParland, J.; Roberts, N.J.; et al. Effects of Regular Physical Activity on the Immune System, Vaccination and Risk of Community-Acquired Infectious Disease in the General Population: Systematic Review and Meta-Analysis. Sports Med. 2021, 51, 1673–1686. [Google Scholar] [CrossRef] [PubMed]
- Campbell, J.P.; Turner, J.E. Debunking the Myth of Exercise-Induced Immune Suppression: Redefining the Impact of Exercise on Immunological Health Across the Lifespan. Front. Immunol. 2018, 9, 648. [Google Scholar] [CrossRef] [PubMed]
- Nieman, D. Exercise, Infection, and Immunity. Int. J. Sports Med. 1994, 15 (Suppl. S3), S131–S141. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Number of Experts | Relevance Mean ± SD | Clarity Mean ± SD | Writing and Terminology Mean ± SD | Format Mean ± SD | CVCt |
|---|---|---|---|---|---|
| 11 | 4.53 ± 0.67 | 4.47 ± 0.77 | 4.44 ± 0.78 | 4.45 ± 0.82 | 0.90 |
| Variable | |
|---|---|
| Age (mean ± SD) | 30.30 ± 12.05 |
| Sex n (%) | |
| Female | 130 (66.0) |
| Male | 67 (34.0) |
| BMI kg/m2 (mean ± SD) | 25.50 ± 4.21 |
| Ethnicity n (%) | |
| Mexican Mestizo | 197 (100) |
| Marital Status n (%) | |
| Single | 123 (62.4) |
| Married | 63 (32.0) |
| Consensual union | 7 (3.6) |
| Other | 4 (2.0) |
| Education n (%) | |
| Postsecondary education | 137 (69.5) |
| Elementary and secondary education | 60 (30.5) |
| Occupation n (%) | |
| Student | 75 (38.1) |
| Employee | 64 (32.5) |
| Self-employed | 43 (21.8) |
| Unemployed | 5 (2.5) |
| Other | 10 (5.1) |
| Variable | Variable | ||
|---|---|---|---|
| Diagnostic Tool n (%) | Days with Symptoms (mean ± SD) | 8.57 ± 5.72 | |
| PCR | 76 (38.6) | Hospitalized n (%) | |
| Antigen test | 59 (29.9) | No | 185 (98.4) |
| Antibody test | 22 (11.2) | Yes | 3 (1.6) |
| Antigen test + clinical | 4 (2.0) | ICU | 1 (33.3) |
| Antibody test + clinical | 7 (3.6) | Oxygen Need n (%) | |
| Clinical | 29 (14.7) | No | 181 (96.3) |
| Year of Diagnosis n (%) | Yes | 7 (3.7) | |
| 2022 | 56 (28.6) | Severity n (%) | |
| 2021 | 81 (41.3) | Mild | 91 (46.2) |
| 2020 | 55 (28.1) | Moderate | 89 (45.2) |
| 2019 | 4 (2.0) | Severe | 17 (8.6) |
| Symptoms n (%) | Post-COVID-19 Weight Loss (Kg) (mean ± SD) | 1.48 ± 3.67 | |
| Present | 188 (95.4) | Comorbidities n (%) | |
| Headache | 149 (75.6) | No | 162 (82.2) |
| Fatigue | 137 (69.5) | Yes | 35 (17.8) |
| Fever | 119 (60.4) | Vaccination n (%) | |
| Sore throat | 111 (56.3) | Yes | 187 (96.4) |
| Anosmia | 107 (54.3) | No | 7 (3.6) |
| Cough | 91 (46.2) | Initial vaccine type | |
| Joint pain | 89 (45.2) | AstraZeneca | 70 (37.4) |
| Eye pain | 73 (37.1) | Sinovac | 69 (37.0) |
| Nasal congestion | 69 (35.0) | Pfizer | 23 (12.3) |
| Runny nose | 66 (33.5) | CanSino | 15 (8.0) |
| Shortness of breath | 60 (30.5) | Other | 10 (5.3) |
| Diarrhea | 26 (13.2) | COVID-19 Post Vaccine n (%) | |
| Vomit | 11 (5.6) | Yes | 62 (35.0) |
| Absent | 9 (4.6) | No | 115 (65.0) |
| Variable | 1 | 2 | 3 | 4 |
|---|---|---|---|---|
| 1. Age | 1.00 | 0.45 ** | 0.22 ** | 0.17 * |
| 2. BMI (Pre-COVID-19) | 1.00 | 0.15 * | 0.77 * | |
| 3. Days with Symptoms | 1.00 | 0.17 * | ||
| 4. Post-COVID-19 Weight Loss | 1.00 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vásquez-Aguilar, F.; Vergara-Jiménez, M.d.J.; Figueroa-Salcido, O.G.; Arámburo-Gálvez, J.G.; Cárdenas-Torres, F.I.; Ontiveros, N.; Martínez-López, E.; Barrón-Cabrera, E. The Role of Diet and Physical Activity in Shaping COVID-19 Severity: Design, Validation, and Application of a Retrospective Questionnaire. Healthcare 2024, 12, 813. https://doi.org/10.3390/healthcare12080813
Vásquez-Aguilar F, Vergara-Jiménez MdJ, Figueroa-Salcido OG, Arámburo-Gálvez JG, Cárdenas-Torres FI, Ontiveros N, Martínez-López E, Barrón-Cabrera E. The Role of Diet and Physical Activity in Shaping COVID-19 Severity: Design, Validation, and Application of a Retrospective Questionnaire. Healthcare. 2024; 12(8):813. https://doi.org/10.3390/healthcare12080813
Chicago/Turabian StyleVásquez-Aguilar, Francisco, Marcela de Jesús Vergara-Jiménez, Oscar G. Figueroa-Salcido, Jesús Gilberto Arámburo-Gálvez, Feliznando Isidro Cárdenas-Torres, Noé Ontiveros, Erika Martínez-López, and Elisa Barrón-Cabrera. 2024. "The Role of Diet and Physical Activity in Shaping COVID-19 Severity: Design, Validation, and Application of a Retrospective Questionnaire" Healthcare 12, no. 8: 813. https://doi.org/10.3390/healthcare12080813